Factors Affecting Discharge to Home of Medical Patients Treated in an Intensive Care Unit



Abstract
:1. Introduction
2. Materials and Methods
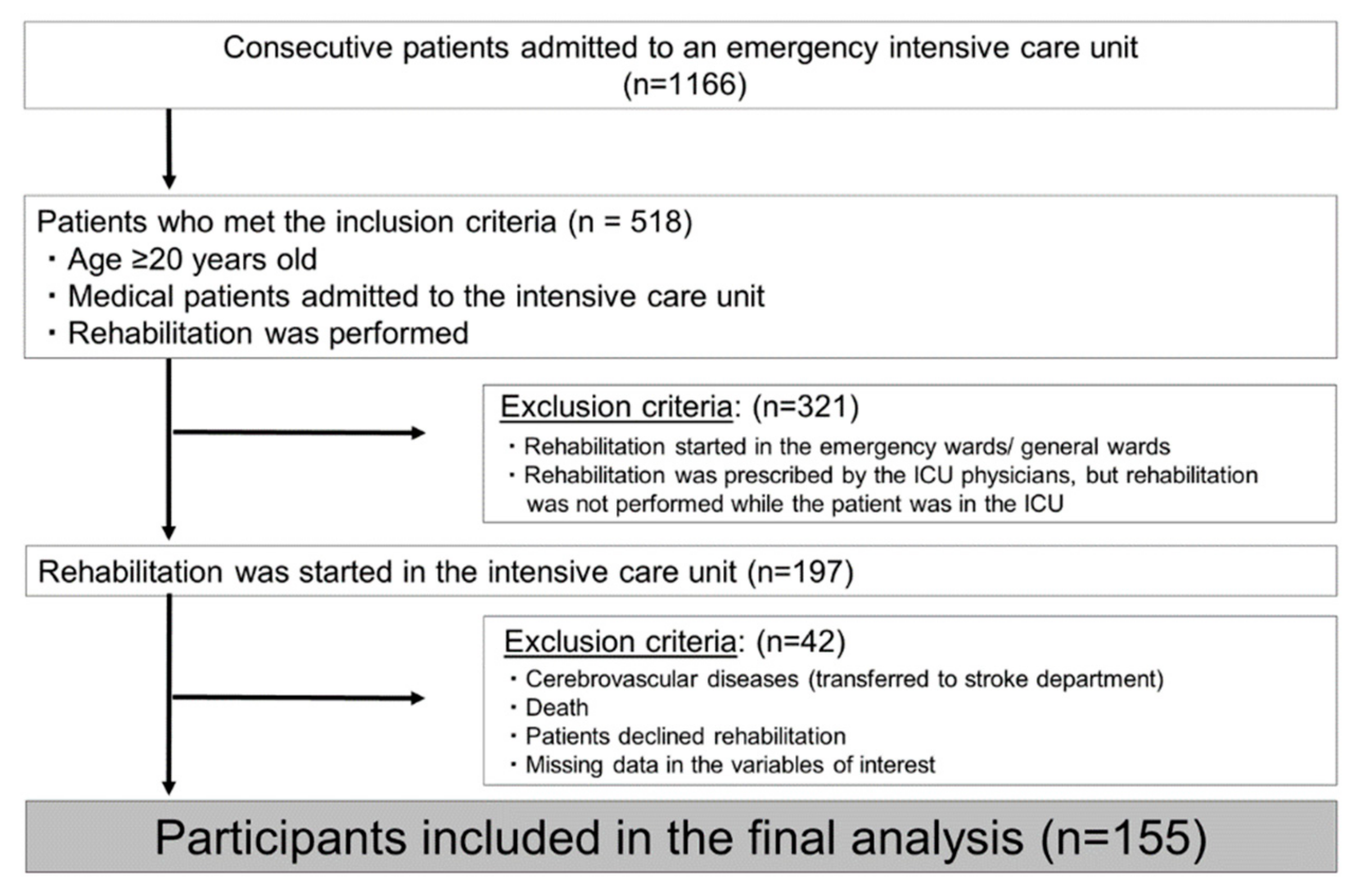
2.1. Study Design and Patients
2.2. Study Procedures
2.3. Criteria for Evaluation of ADL Before Admission
2.4. Assessment of Muscle Strength
2.5. Assessment of Disability
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
4. Discussion
4.1. Independence at Home Before Admission
4.2. Starting Date of Standing
4.3. Factors Affecting Discharge to Home
4.4. Implications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaukonen, K.M.; Bailey, M.; Suzuki, S.; Pilcher, D.; Bellomo, R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA 2014, 311, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Iwashyna, T.J.; Cooke, C.R.; Wunsch, H.; Kahn, J.M. Population burden of long-term survivorship after severe sepsis in older Americans. J. Am. Geriatr. Soc. 2012, 60, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Reineck, L.A.; Pike, F.; Le, T.Q.; Cicero, B.D.; Iwashyna, T.J.; Kahn, J.M. Hospital factors associated with discharge bias in ICU performance measurement. Crit. Care Med. 2014, 42, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Creditor, M.C. Hazards of hospitalization of the elderly. Ann. Intern. Med. 1993, 118, 219–223. [Google Scholar] [CrossRef]
- Basmaji, J.; Lau, V.; Lam, J.; Priestap, F.; Ball, I.M. Lessons learned and new directions regarding Discharge Direct from Adult Intensive Care Units Sent Home (DISH): A narrative review. J. Intensive Care Soc. 2019, 20, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Lau, V.I.; Priestap, F.A.; Lam, J.N.H.; Ball, I.M. Factors Associated with the Increasing Rates of Discharges Directly Home from Intensive Care Units-A Direct from ICU Sent Home Study. J. Intensive Care Med. 2018, 33, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Gehlbach, B.K.; Salamanca, V.R.; Levitt, J.E.; Sachs, G.A.; Sweeney, M.K.; Pohlman, A.S.; Charbeneau, J.; Krishnan, J.A.; Hall, J.B. Patient-related factors associated with hospital discharge to a care facility after critical illness. Am. J. Crit. Care 2011, 20, 378–386. [Google Scholar] [CrossRef]
- Chawla, S.; D’Agostino, R.L.; Pastores, S.M.; Thirumala, R.; Kostelecky, N.; Chou, J.F.; Thaler, H.T.; Halpern, N.A. Homeward bound: An analysis of patients discharged home from an oncologic intensive care unit. J. Crit. Care 2012, 27, 681–687. [Google Scholar] [CrossRef]
- Harrison, J.K.; Walesby, K.E.; Hamilton, L.; Armstrong, C.; Starr, J.M.; Reynish, E.L.; MacLullich, A.M.J.; Quinn, T.J.; Shenkin, S.D. Predicting discharge to institutional long-term care following acute hospitalisation: A systematic review and meta-analysis. Age Ageing 2017, 46, 547–558. [Google Scholar] [CrossRef]
- Centre for Clinical Practice at NICE. National Institute for Health and Clinical Excellence: Guidance. In Rehabilitation after Critical Illness; National Institute for Health and Clinical Excellence (UK): London, UK, 2009. [Google Scholar]
- Morris, P.E.; Goad, A.; Thompson, C.; Taylor, K.; Harry, B.; Passmore, L.; Ross, A.; Anderson, L.; Baker, S.; Sanchez, M.; et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit. Care Med. 2008, 36, 2238–2243. [Google Scholar] [CrossRef]
- Kayambu, G.; Boots, R.; Paratz, J. Physical therapy for the critically ill in the ICU: A systematic review and meta-analysis. Crit. Care Med. 2013, 41, 1543–1554. [Google Scholar] [CrossRef] [PubMed]
- Ota, H.; Kawai, H.; Sato, M.; Ito, K.; Fujishima, S.; Suzuki, H. Effect of early mobilization on discharge disposition of mechanically ventilated patients. J. Phys. Ther. Sci. 2015, 27, 859–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, B.B.; Laughlin, J.A.; Fiedler, R.C.; Granger, C.V. Interrater reliability of the 7-level functional independence measure (FIM). Scand. J. Rehabil. Med. 1994, 26, 115–119. [Google Scholar]
- An Official Decument of Ministry Secretariat of Health and Welfare for the Elderly Bureau. Criteria for Evaluating the Degree of Independence (Degree of “Bedriddenness”) of Disabled Elderly Persons in Performing Activities of Daily Living; Rohken publication, 1991. (In Japanese)
- Uza, M.; Tome, K.; Imai, M.; Danboku, K.; Suzuki, M. A study of case finding of the latent bedridden elderly using criteria of activity of daily living. Jpn. J. Health Hum. Ecol. 1997, 63, 79–89. [Google Scholar] [CrossRef]
- Tsuga, K.; Yoshikawa, M.; Oue, H.; Okazaki, Y.; Tsuchioka, H.; Maruyama, M.; Yoshida, M.; Akagawa, Y.J.G. Maximal voluntary tongue pressure is decreased in Japanese frail elderly persons. Gerodontology 2012, 29, e1078–e1085. [Google Scholar] [CrossRef]
- Kleyweg, R.P.; van der Meche, F.G.; Schmitz, P.I. Interobserver agreement in the assessment of muscle strength and functional abilities in Guillain-Barre syndrome. Muscle Nerve 1991, 14, 1103–1109. [Google Scholar] [CrossRef]
- Hoffer, M.M. Basic considerations and classifications of cerebral palsy. Am. Acad. Orthop. Surg. Instr. Course Lect. 1976, 25, 37. [Google Scholar]
- Hodgson, C.L.; Berney, S.; Harrold, M.; Saxena, M.; Bellomo, R. Clinical review: Early patient mobilization in the ICU. Crit. Care 2013, 17, 207. [Google Scholar] [CrossRef]
- Cameron, S.; Ball, I.; Cepinskas, G.; Choong, K.; Doherty, T.J.; Ellis, C.G.; Martin, C.M.; Mele, T.S.; Sharpe, M.; Shoemaker, J.K.; et al. Early mobilization in the critical care unit: A review of adult and pediatric literature. J. Crit. Care 2015, 30, 664–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covinsky, K.E.; Justice, A.C.; Rosenthal, G.E.; Palmer, R.M.; Landefeld, C.S. Measuring prognosis and case mix in hospitalized elders: The importance of functional status. J. Gen. Intern. Med. 1997, 12, 203–208. [Google Scholar]
- Nierman, D.M.; Schechter, C.B.; Cannon, L.M.; Meier, D.E. Outcome prediction model for very elderly critically ill patients. Crit. Care Med. 2001, 29, 1853–1859. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, L.E.; Pisani, M.A.; Murphy, T.E.; Gahbauer, E.A.; Leo-Summers, L.S.; Gill, T.M. The Association of Frailty with Post-ICU Disability, Nursing Home Admission, and Mortality: A Longitudinal Study. Chest 2018, 153, 1378–1386. [Google Scholar] [CrossRef] [PubMed]
- Schweickert, W.D.; Kress, J.P. Implementing early mobilization interventions in mechanically ventilated patients in the ICU. Chest 2011, 140, 1612–1617. [Google Scholar] [CrossRef]
- Adler, J.; Malone, D. Early mobilization in the intensive care unit: A systematic review. Cardiopulm. Phys. Ther. J. 2012, 23, 5–13. [Google Scholar] [CrossRef]
- Sommers, J.; Engelbert, R.H.; Dettling-Ihnenfeldt, D.; Gosselink, R.; Spronk, P.E.; Nollet, F.; van der Schaaf, M. Physiotherapy in the intensive care unit: An evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin. Rehabil. 2015, 29, 1051–1063. [Google Scholar] [CrossRef]
- Parry, S.M.; Denehy, L.; Beach, L.J.; Berney, S.; Williamson, H.C.; Granger, C.L. Functional outcomes in ICU—What should we be using?—An observational study. Crit. Care 2015, 19, 127. [Google Scholar] [CrossRef]
- Baldwin, M.R.; Narain, W.R.; Wunsch, H.; Schluger, N.W.; Cooke, J.T.; Maurer, M.S.; Rowe, J.W.; Lederer, D.J.; Bach, P.B. A Prognostic Model for 6-Month Mortality in Elderly Survivors of Critical Illness. Chest 2013, 143, 910–919. [Google Scholar] [CrossRef] [Green Version]
- De Rooij, S.E.; Govers, A.C.; Korevaar, J.C.; Giesbers, A.W.; Levi, M.; de Jonge, E. Cognitive, functional, and quality-of-life outcomes of patients aged 80 and older who survived at least 1 year after planned or unplanned surgery or medical intensive care treatment. J. Am. Geriatr. Soc. 2008, 56, 816–822. [Google Scholar] [CrossRef]


{kind=link}
| Major Classification | n | Minor Classification |
|---|---|---|
| I. Certain infectious and parasitic diseases | 46 | Sepsis 46 |
| X. Diseases of the respiratory system | 37 | Chronic obstructive pulmonary disease (COPD)—acute exacerbation 4, interstitial pulmonary diseases 5, asthma 3, hemorrhage from other sites in respiratory passages 1, bacterial pneumonia 14, pneumonitis due to food and vomiting 1, drug-induced interstitial lung disorders, unspecified 2, drowning and nonfatal submersion 2, bronchus or lung, unspecified 1, acute respiratory failure 3, other and unspecified abnormalities of breathing (CO2 narcosis) 1 |
| XI. Diseases of the digestive system | 21 | Gastrointestinal hemorrhage 12, acute pancreatitis 5, esophageal varices 2, gastric ulcer 1, peritonitis 1 |
| XIX. Injury, poisoning and certain other consequences of external causes | 18 | Other and unspecified drugs/medicaments and biological substance (acute drug addiction) 13, hypothermia 2, injury of muscles and tendons of unspecified body region 1, injury of intercostal blood vessels 1, toxic effect of carbon monoxide 1 |
| IV. Endocrine, nutritional and metabolic diseases | 15 | Elevated blood glucose level 3, hypoglycemia, unspecified 2, diabetes mellitus with ketoacidosis 4, other disorders of electrolyte and fluid balance, not elsewhere classified 4, hypothyroidism, unspecified 1, acidosis (due to alcohol) 1 |
| VI. Diseases of the nervous system | 7 | Encephalitis, myelitis and encephalomyelitis 3, epilepsy 2, disorder of autonomic nervous system 1, myasthenia gravis 1 |
| XVIII. Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified | 3 | Coma, unspecified 1, unspecified adverse effect of drug or medicament (serotonin syndrome) 1, Hemoptysis 1 |
| XIV. Diseases of the genitourinary system | 5 | Acute renal failure 5 |
| IX. Diseases of the circulatory system | 1 | Cardiac arrest 1 |
| XII. Diseases of the skin and subcutaneous tissue | 1 | Bullous erythema multiforme (Stevens-Johnson syndrome) 1 |
| XIII. Diseases of the musculoskeletal system and connective tissue | 1 | Other specified disorders of muscle (rhabdomyolysis) 1 |
| Home Discharge | Transfer | P-Value | |
|---|---|---|---|
| n = 95 | n = 60 | ||
| Age | 66.0 (51.0, 74.0)* | 75.5 (65.8, 82.3) * | <0.001 |
| Sex (male/female) | 61/34 | 37/23 | 0.75 |
| SOFA score | 6.0(3.5, 9.0) * | 7.0 (4.8, 9.3) * | 0.049 |
| APACHE II score | 16.0 (11.5, 20.0) * | 21.5 (15.0, 25.0) * | <0.001 |
| Independence at home before admission (%) | 95.8% (91/95) | 76.7% (46/60) | <0.001 |
| Peak CRP (mg/L) | 10.32 (4.16, 17.14) * | 14.88 (5.69, 19.74) * | 0.26 |
| Peak WBC (×103/μL) | 14.20(10.05, 18.90) * | 15.25 (10.00, 21.47) * | 0.39 |
| Admission albumen (g/dL) | 3.00 (2.60, 3.80) * | 2.70 (2.20, 3.40) * | 0.009 |
| Use of cardiotonic drugs (%) | 23.2% (22/95) | 35.0% (21/60) | 0.109 |
| Mechanical ventilation (%) | 74.7% (71/95) | 73.3% (44/60) | 0.85 |
| Delirium (%) | 9.5 (9/95) | 16.7 (10/60) | 0.184 |
| Rehabilitation start date (day) | 1.0 (1.0, 2.0) * | 1.0 (1.0, 2.0) * | 0.59 |
| Initial MRC score | 52 (48, 55) * | 46 (37, 49.5) * | <0.001 |
| Hands-dependent sitter (%) | 89.5 (85/95) | 51.7 (31/60) | <0.001 |
| Standing within 5 days of admission (%) | 84.2 (80/95) | 51.7 (31/60) | <0.001 |
| Motor FIM (start) | 13.0 (13.0, 16.5) * | 13.0 (13.0, 13.0) * | 0.012 |
| Cognitive FIM (start) | 23.0 (10.5, 29.0) * | 5.5 (5.0, 14.3) * | <0.001 |
| Hospital stay (days) | 18.0 (12.0, 29.0) * | 29.5 (19.0, 49.8) * | <0.001 |
| Variable | P-Value | OR | 95% CI |
|---|---|---|---|
| Age | 0.001 | 1.06 | 1.02 – 1.09 |
| APACHE II score | 0.002 | 1.12 | 1.04 – 1.20 |
| Independence at home before admission | 0.008 | 7.10 | 1.65 – 30.44 |
| Standing within 5 days of admission | <0.001 | 6.58 | 2.60 – 16.61 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimogai, T.; P. Izawa, K.; Kawada, M.; Kuriyama, A. Factors Affecting Discharge to Home of Medical Patients Treated in an Intensive Care Unit. Int. J. Environ. Res. Public Health 2019, 16, 4324. https://doi.org/10.3390/ijerph16224324
Shimogai T, P. Izawa K, Kawada M, Kuriyama A. Factors Affecting Discharge to Home of Medical Patients Treated in an Intensive Care Unit. International Journal of Environmental Research and Public Health. 2019; 16(22):4324. https://doi.org/10.3390/ijerph16224324
Chicago/Turabian StyleShimogai, Takayuki, Kazuhiro P. Izawa, Minoru Kawada, and Akira Kuriyama. 2019. "Factors Affecting Discharge to Home of Medical Patients Treated in an Intensive Care Unit" International Journal of Environmental Research and Public Health 16, no. 22: 4324. https://doi.org/10.3390/ijerph16224324
APA StyleShimogai, T., P. Izawa, K., Kawada, M., & Kuriyama, A. (2019). Factors Affecting Discharge to Home of Medical Patients Treated in an Intensive Care Unit. International Journal of Environmental Research and Public Health, 16(22), 4324. https://doi.org/10.3390/ijerph16224324