Increased Heart Rate during Walk Test Predicts Chronic-Phase Worsening of Renal Function in Patients with Acute Myocardial Infarction and Normal Kidney Function


 ,
,
Abstract
:1. Introduction
2. Methods
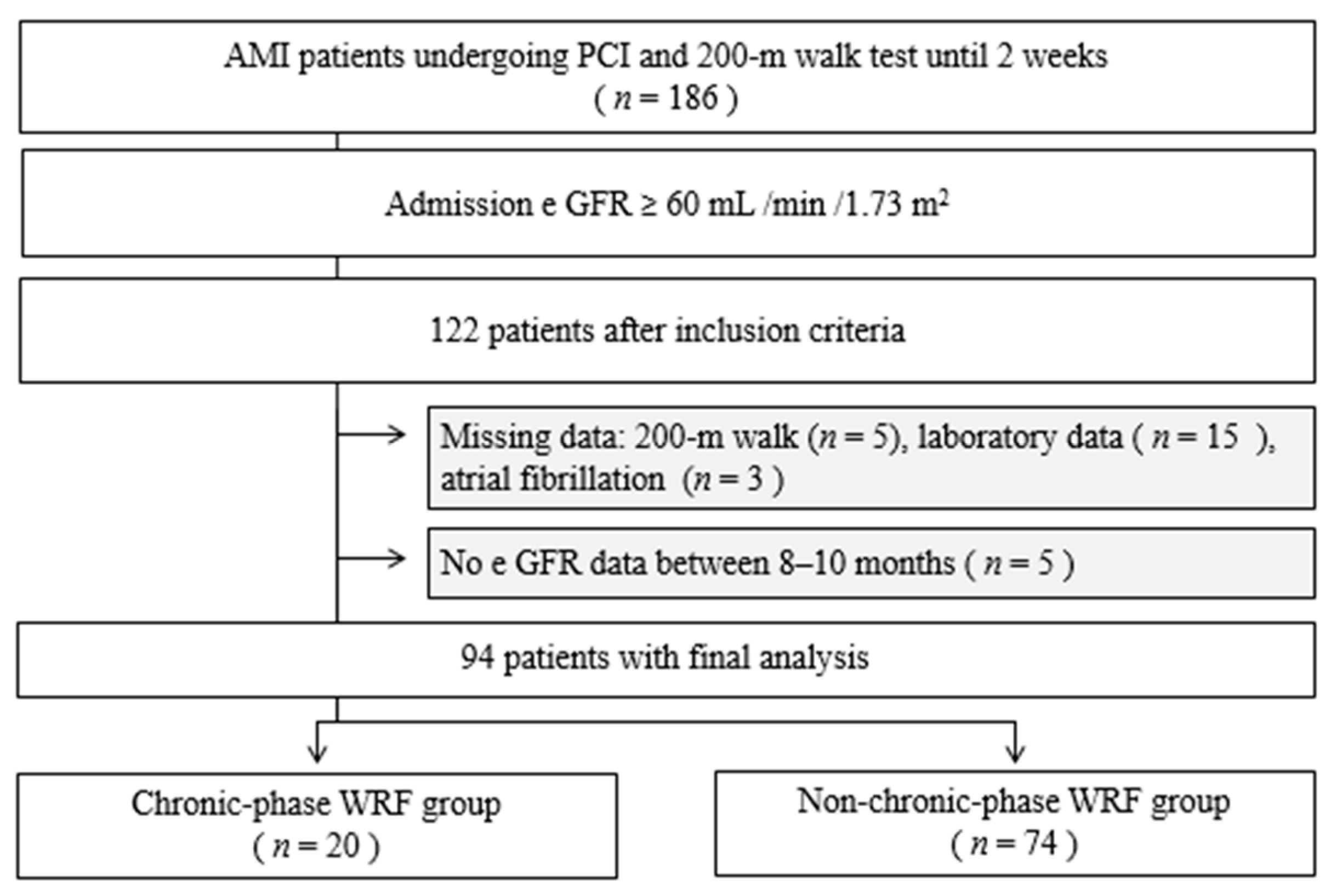
2.1. Study Design and Patients
2.2. Definitions
2.2.1. AMI
2.2.2. Renal Function
2.2.3. Chronic-Phase WRF
2.2.4. Walk Test
2.3. Statistics
3. Results
4. Discussion
4.1. Risk Factors for Chronic-Phase WRF
4.2. Association between ΔHR and Chronic-Phase WRF
4.3. Sympathetic Hyperactivity and Chronic-Phase WRF
4.4. Sympathetic Hyperactivity and Other Parameters of the 200-m Walk Test
4.5. Usefulness of the 200-m Walk Test
4.6. Clinical Implication and Future Research
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morici, N.; Savonitto, V.; Ponticelli, C.; Schrieks, I.C.; Nozza, A.; Cosentino, F.; Stähli, B.E.; Perrone Filardi, P.; Schwartz, G.G.; Mellbin, L.; et al. Post-discharge worsening renal function in patients with type 2 diabetes and recent acute coronary syndrome. Am. J. Med. 2017, 130, 1068–1075. [Google Scholar] [CrossRef]
- Nemoto, N.; Iwasaki, M.; Nakanishi, M.; Araki, T.; Utsunomiya, M.; Hori, M.; Ikeda, N.; Makino, K.; Itaya, H.; Iijima, R.; et al. Impact of continuous deterioration of kidney function 6 to 8 months after percutaneous coronary intervention for acute coronary syndrome. Am. J. Cardiol. 2014, 113, 1647–1651. [Google Scholar] [CrossRef]
- Murata, N.; Kaneko, H.; Yajima, J.; Oikawa, Y.; Oshima, T.; Tanaka, S.; Kano, H.; Matsuno, S.; Suzuki, S.; Kato, Y.; et al. The prognostic impact of worsening renal function in Japanese patients undergoing percutaneous coronary intervention with acute coronary syndrome. J. Cardiol. 2015, 66, 326–332. [Google Scholar] [CrossRef]
- Choe, J.C.; Cha, K.S.; Ahn, J.; Park, J.S.; Lee, H.W.; Oh, J.H.; Kim, J.S.; Choi, J.H.; Park, Y.H.; Lee, H.C.; et al. Persistent renal dysfunction after percutaneous coronary intervention in patients with acute myocardial infarction. Angiology 2017, 68, 159–167. [Google Scholar] [CrossRef]
- Ogita, M.; Sakakura, K.; Nakamura, T.; Funayama, H.; Wada, H.; Naito, R.; Sugawara, Y.; Kubo, N.; Ako, J.; Momomura, S. Association between deteriorated renal function and long-term clinical outcomes after percutaneous coronary intervention. Heart Vessels 2012, 27, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Hernando, L.; Canovas, E.; Freites, A.; de la Rosa, A.; Alonso, J.; del Castillo, R.; Salinas, P.; Montalvo, G.B.; Huelmos, A.I.; Botas, J. Prevalence and prognosis of percutaneous coronary intervention-associated nephropathy in patients with acute coronary syndrome and normal kidney function. Rev. Esp. Cardiol. 2015, 68, 310–316. [Google Scholar] [CrossRef] [PubMed]
- JCS Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ. J. 2014, 78, 2022–2093. [Google Scholar] [CrossRef] [PubMed]
- Shacham, Y.; Leshem-Rubinow, E.; Gal-Oz, A.; Arbel, Y.; Keren, G.; Roth, A.; Steinvil, A. Acute cardio-renal syndrome as a cause for renal deterioration among myocardial infarction patients treated with primary percutaneous intervention. Can. J. Cardiol. 2015, 31, 1240–1244. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equation for estimated GFR from serum creatinine in Japan. Am. J. Kidney. Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart. J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Asif, M.; Jameel, A.; Sahito, N.; Hwang, J.; Hussain, A.; Manzoor, F. Can leadership enhance patient satisfaction? Assessing the role of administrative and medical quality. Int. J. Environ. Res. Public Health 2019, 16, 3212. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, K.; Shimada, K.; Katayama, H.; Nakamura, H.; Ishikawa, H.; Takeda, H.; Fujimoto, K.; Kasayuki, N.; Yoshiyama, M. Prognostic significance of renal dysfunction and its change pattern on outcomes in patients with acute coronary syndrome treated with emergent percutaneous coronary intervention. Heart Vessels 2019, 34, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, M.K.; Kannankeril, P.J.; Goldberger, J.J. Assessment of autonomic function in cardiovascular disease: physiological basis and prognostic implications. Am. Coll. Cardiol. 2008, 51, 1725–1733. [Google Scholar] [CrossRef]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s Guide to cardiopulmonary exercise testing in adults. a scientific statement from the American Heart Association. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef]
- Graham, L.N.; Smith, P.A.; Stoker, J.B.; Mackintosh, A.F.; Mary, D.A. Time course of sympathetic neural hyperactivity after uncomplicated acute myocardial infarction. Circulation 2002, 106, 793–797. [Google Scholar] [CrossRef]
- Diniz, L.S.; Neves, V.R.; Starke, A.C.; Barbosa, M.P.T.; Britto, R.R.; Ribeiro, A.L.P. Safety of early performance of the six-minute walk test following acute myocardial infarction: a cross-sectional study. Braz. J. Phys. Ther. 2017, 21, 167–174. [Google Scholar] [CrossRef]
- Omiya, K.; Itoh, H.; Osada, N.; Kato, M.; Koike, A.; Sagara, K.; Aoki, K.; Fu, L.T.; Watanabe, H.; Kato, K.; et al. Impaired heart rate response during incremental exercise in patients with acute myocardial infarction and after coronary artery bypass grafting. Jpn. Circ. J. 2000, 64, 851–855. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Hughson, R.L.; Peterson, J.C. Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J. Appl. Physiol. 1991, 71, 1136–1142. [Google Scholar] [CrossRef]
- Casillas, J.M.; Hannequin, A.; Besson, D.; Benaïm, S.; Krawcow, C.; Laurent, Y.; Gremeaux, V. Walking tests during the exercise training: specific use of the cardiac rehabilitation. Ann. Phys. Rehabil. Med. 2013, 56, 561–575. [Google Scholar] [CrossRef]
- Lekawanvijit, S.; Kompa, A.R.; Zhang, Y.; Wang, B.H.; Kelly, D.J.; Krum, H. Myocardial infarction impairs renal function, induces renal interstitial fibrosis, and increases renal KIM-1 expression: implications for cardiorenal syndrome. Am. J. Physiol. Heart. Circ. Physiol. 2012, 302, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.; Hammerman, H.; Petcherski, S.; Zdorovyak, A.; Yalonetsky, S.; Kapeliovich, M.; Agmon, Y.; Markiewicz, W.; Aronson, D. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am. Heart. J. 2005, 150, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Hogarth, A.J.; Graham, L.N.; Mary, D.A.; Greenwood, J.P. Gender differences in sympathetic neural activation following uncomplicated acute myocardial infarction. Eur. Heart. J. 2009, 30, 1764–1770. [Google Scholar] [CrossRef] [PubMed]
- Hall, T.M.; Gordon, C.; Roy, R.; Schwenke, D.O. Delayed coronary reperfusion is ineffective at impeding the dynamic increase in cardiac efferent sympathetic nerve activity following myocardial ischemia. Basic. Res. Cardiol. 2016, 111, 35. [Google Scholar] [CrossRef]
- Billman, G.E.; Kukielka, M. Effects of endurance exercise training on heart rate variability and susceptibility to sudden cardiac death: protection is not due to enhanced cardiac vagal regulation. J. Appl. Physiol. 2006, 100, 896–906. [Google Scholar] [CrossRef]
- Tatsuki, H.; Noma, Y.; Kawahara, T.; Kawabata, M.; Aizawa, T.; Matsuzaki, A.; Hoshiba, Y.; Sugihara, T.; Kawanura, Y.; Ito, D.; et al. Clinical background and hospitalization progress in patients with acute myocardial infarction who experienced cardiac rehabilitation –comparison among age groups–. J. Rural. Med. 2012, 61, 16–26. [Google Scholar]
- Matsuzawa, Y.; Konishi, M.; Akiyama, E.; Suzuki, H.; Nakayama, N.; Kiyokuni, M.; Sumita, S.; Ebina, T.; Kosuge, M.; Hibi, K.; et al. Association between gait speed as a measure of frailty and risk of cardiovascular events after myocardial infarction. J. Am. Coll. Cardiol. 2013, 61, 1964–1972. [Google Scholar] [CrossRef]
- Asgari, M.R.; Jafarpoor, H.; Soleimani, M.; Ghorbani, R.; Askandarian, R.; Jafaripouret, I. Effects of early mobilization program on the heart rate and blood pressure of patients with myocardial infarction hospitalized at the coronary care unit. Middle. East. J. Rehabil. Health. 2015, 2, e24168. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Chronic-Phase WRF n = 20 | Non-Chronic-Phase WRF n = 74 | p Value | |
|---|---|---|---|
| Age, years | 66.3 ± 11.0 | 62.9 ± 11.0 | 0.225 |
| Female, n (%) | 7 (35) | 7 (9.5) | 0.009 |
| Body mass index, kg/m2 | 22.6 (20.9–23.9) | 23.8 (21.9–25.9) | 0.116 |
| Peak CPK, IU/L | 1822 (920.0–3490.3) | 1917.0 (843.8–3142.0) | 0.989 |
| STEMI, n (%) | 15 (75.0) | 59 (79.7) | 0.759 |
| LVEF, (%) | 53.1 ± 9.4 | 57.3 ± 11.9 | 0.149 |
| Contrast volume, mL | 150 (133.8–190.0) | 140 (115.0–170.0) | 0.425 |
| Pain to balloon time, min | 285 (164.0–497.5) | 179.0 (131.0–296.3) | 0.039 |
| Medical history | |||
| Previous MI, n (%) | 0 (0) | 6 (8.1) | 0.336 |
| Hypertension, n (%) | 13 (65.0) | 45 (60.8) | 0.800 |
| Diabetes mellitus, n (%) | 5 (25.0) | 27 (36.5) | 0.430 |
| 200-m walk test | |||
| Rest HR, bpm | 63.1 ± 10.2 | 64.5 ± 8.7 | 0.522 |
| Peak HR, bpm | 91.8 ± 12.9 | 86.4 ± 10.6 | 0.057 |
| ΔHR (peak-rest), bpm | 28.7 ± 7.3 | 21.8 ± 7.0 | <0.001 |
| Rest SBP, mmHg | 108.5 (100–114.5) | 111.0 (102–119.5) | 0.567 |
| Post SBP, mmHg | 113.5 (101.8–124.5) | 118.0 (107.3–123.0) | 0.563 |
| ΔSBP (post-rest), mmHg | 6.1 ± 11.4 | 5.9 ± 11.3 | 0.953 |
| eGFR, mL/min/1.73 m2 | |||
| Admission | 81.5 (74.5–96.0) | 71.3 (64.7–78.9) | <0.001 |
| 8–10 months | 60.2 ± 13.3 | 69.9 ± 11.6 | 0.002 |
| Δ (admission–8–10 months) | 24.4 (20.1–29.6) | 4.1 (−2.2–8.6) | <0.001 |
| Admission laboratory findings | |||
| BUN/CRE | 21.0 (18.1–27.9) | 19.0 (16.2–21.3) | 0.075 |
| BNP, pg/mL | 65.2 (22.3–116.8) | 20.7 (6.9–43.6) | 0.001 |
| Serum CRP, nmol/L | 0.46 (0.06–2.34) | 0.14 (0.05–0.68) | 0.322 |
| Hemoglobin, g/dL | 14.3 ± 1.8 | 14.9 ± 1.7 | 0.159 |
| HbA1c, % | 5.9 (5.7–6.4) | 6.1 (5.8–6.9) | 0.119 |
| Medications at 200-m walk | |||
| Beta blockers, n (%) | 11 (55.0) | 43 (58.9) | 0.802 |
| Medications at discharge | |||
| Beta blocker, n (%) | 13 (65.0) | 40 (57.1) | 0.612 |
| ACE-I, n (%) | 5 (25.0) | 19 (26.0) | 1 |
| ARB, n (%) | 6 (30.0) | 25 (34.2) | 0.795 |
| CCB, n (%) | 3 (15.0) | 12 (16.4) | 1 |
| Diuretic, n (%) | 6 (30.0) | 8 (11.0) | 0.070 |
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| β | 95% CI | p-Value | β | 95% CI | t | p-Value | |
| Age | 0.063 | −0.180, 0.308 | 0.606 | ||||
| Female | 8.542 | 1.233, 15.852 | 0.023 | 9.631 | 3.190, 16.073 | 2.975 | 0.004 |
| Body mass index | −0.375 | −1.108, 0.359 | 0.313 | ||||
| Peak CPK | <0.001 | −0.001, 0.001 | 0.891 | ||||
| STEMI | −1.485 | −9.787, 6.818 | 0.723 | ||||
| LVEF | −0.109 | −0.348, 0.131 | 0.370 | ||||
| Contrast volume | 0.033 | −0.025, 0.090 | 0.267 | ||||
| Pain to balloon time | 0.020 | 0.007, 0.033 | 0.004 | 0.016 | 0.005, 0.027 | 2.970 | 0.004 |
| Medical history | |||||||
| Previous MI | −10.042 | −20.800, 0.711 | 0.067 | ||||
| Hypertension | 0.871 | −4.634, 6.375 | 0.754 | ||||
| Diabetes mellitus | −3.522 | −9.125, 2.018 | 0.215 | ||||
| 200-m walk test | |||||||
| Rest HR | −0.065 | −0.363,0.234 | 0.668 | ||||
| Peak HR | 0.252 | 0.019, 0.486 | 0.034 | −0.017 | −0.245, 0.212 | −0.145 | 0.885 |
| ΔHR (peak-rest) | 0.645 | 0.317, 0.973 | <0.001 | 0.427 | 0.076, 0.777 | 2.419 | 0.018 |
| Rest SBP | −0.022 | −0.165, 0.208 | 0.817 | ||||
| Post SBP | 0.049 | −0.111, 0.208 | 0.547 | ||||
| ΔSBP (post-rest) | 0.073 | −0.156, 0.312 | 0.545 | ||||
| Admission laboratory findings | |||||||
| eGFR | 0.507 | 0.351, 0.664 | <0.001 | 0.418 | 0.265, 0.571 | 5.415 | <0.001 |
| BUN/CRE | 0.632 | 0.125, 1.138 | 0.015 | 0.009 | −0.431, 0.449 | 0.042 | 0.967 |
| BNP | 0.005 | −0.019, 0.029 | 0.665 | ||||
| CRP | 1.278 | −0.407, 2.963 | 0.135 | ||||
| Hemoglobin | −1.046 | −2.609, 0.517 | 0.187 | ||||
| HbA1c | −0.831 | −3.508, 1.847 | 0.539 | ||||
| R2 | 0.439 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogura, A.; Izawa, K.P.; Tawa, H.; Kureha, F.; Wada, M.; Kanai, M.; Kubo, I.; Yoshikawa, R.; Matsuda, Y. Increased Heart Rate during Walk Test Predicts Chronic-Phase Worsening of Renal Function in Patients with Acute Myocardial Infarction and Normal Kidney Function. Int. J. Environ. Res. Public Health 2019, 16, 4785. https://doi.org/10.3390/ijerph16234785
Ogura A, Izawa KP, Tawa H, Kureha F, Wada M, Kanai M, Kubo I, Yoshikawa R, Matsuda Y. Increased Heart Rate during Walk Test Predicts Chronic-Phase Worsening of Renal Function in Patients with Acute Myocardial Infarction and Normal Kidney Function. International Journal of Environmental Research and Public Health. 2019; 16(23):4785. https://doi.org/10.3390/ijerph16234785
Chicago/Turabian StyleOgura, Asami, Kazuhiro P. Izawa, Hideto Tawa, Fumie Kureha, Masaaki Wada, Masashi Kanai, Ikko Kubo, Ryohei Yoshikawa, and Yuichi Matsuda. 2019. "Increased Heart Rate during Walk Test Predicts Chronic-Phase Worsening of Renal Function in Patients with Acute Myocardial Infarction and Normal Kidney Function" International Journal of Environmental Research and Public Health 16, no. 23: 4785. https://doi.org/10.3390/ijerph16234785
APA StyleOgura, A., Izawa, K. P., Tawa, H., Kureha, F., Wada, M., Kanai, M., Kubo, I., Yoshikawa, R., & Matsuda, Y. (2019). Increased Heart Rate during Walk Test Predicts Chronic-Phase Worsening of Renal Function in Patients with Acute Myocardial Infarction and Normal Kidney Function. International Journal of Environmental Research and Public Health, 16(23), 4785. https://doi.org/10.3390/ijerph16234785