Trends and Inequalities in the Health Care and Hypertension Outcomes in China, 2011 to 2015

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Indicators
2.3. Statistical Analysis
3. Results
3.1. Trends in Hypertension Prevalence and Healthcare in China
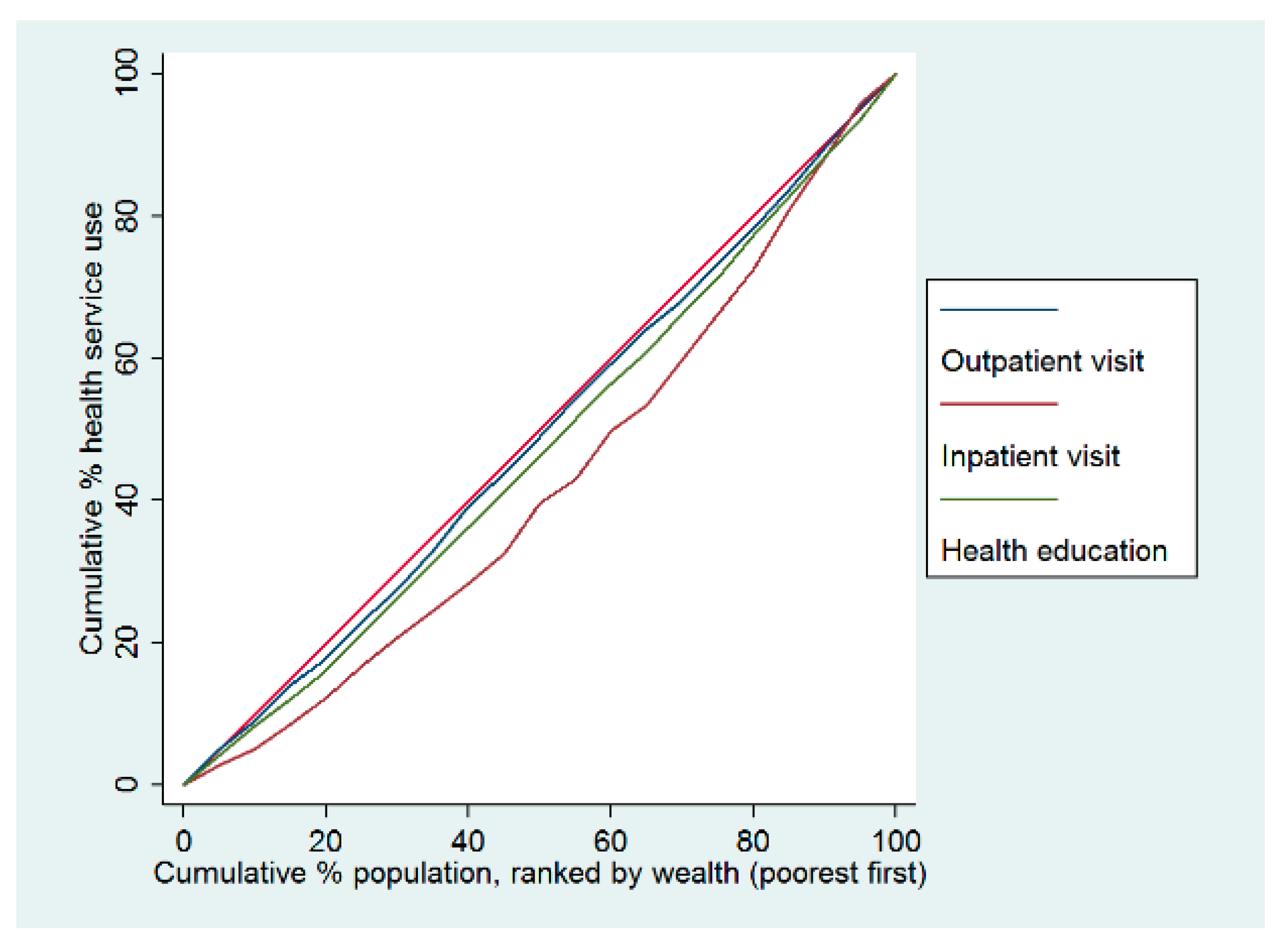
3.2. Socioeconomic Inequalities in Healthcare and Outcomes
3.3. Results of Multivariate Regression Analysis
4. Discussion
4.1. Trends in Hypertension Prevalence and Treatment in China
4.2. Health Service Use among Chinese Adults with Hypertension
4.3. Low Level of Control for Hypertension in China
4.4. Socioeconomic Inequalities in Hypertenison Care
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization and International Bank for Reconstruction and Development/The World Bank, Tracking Universal Health Coverage: 2017 Global Monitoring Report; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization and International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017.
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015; pp. 16–17. [Google Scholar]
- Chen, J.; Zhao, W. Diet, Nutrition and Chronic Disease in Mainland China. J. Food Drug Anal. 2012, 20, 222–225. [Google Scholar]
- Limwattananon, S.; Tangcharoensathien, V.; Tisayathicom, K.; Boonyapaisarncharoen, T.; Prakongsai, P. Why has the universal coverage scheme in Thailand achieved a pro-poor public subsidy for health care? BMC Public Health 2012, 12 (Suppl. 1), S6. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Oldenburg, B.; Zhao, S.; Haregu, T.N.; Zhang, L. Temporal trends and geographic disparity in hypertension care in China. J. Epidemiol. 2019, 30. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lee, D.C.; Liang, H.; Zhang, L.; Makinen, M.; Blanchet, N.; Kidane, R.; Lindelow, M.; Wang, H.; Wu, S. Community health centers and primary care access and quality for chronically-ill patients—A case-comparison study of urban Guangdong Province, China. Int. J. Equity Health 2015, 14, 90. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, Z.; Zhang, L.; Wang, X.; Hao, G.; Zhang, Z.; Shao, L.; Tian, Y.; Dong, Y.; Zheng, D.; et al. Status of hypertension in China: Results from the China Hypertension Survey, 2012–2015. Circulation 2018, 137, 2344–2356. [Google Scholar] [CrossRef] [PubMed]
- Xi, B.; Liang, Y.; Reilly, K.H.; Wang, Q.; Hu, Y.; Tang, W. Trends in prevalence, awareness, treatment, and control of hypertension among Chinese adults 1991–2009. Int. J. Cardiol. 2012, 158, 326–329. [Google Scholar] [CrossRef]
- Nrc, C.; Zhang, X.H. Hypertension in China: Time to Transition From Knowing the Problem to Implementing the Solution. Circulation 2018, 137, 2357. [Google Scholar]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press. 2013, 22, 193–278. [Google Scholar] [CrossRef]
- Chobanian, A.-V. National heart, lung, and blood institute joint national committee on prevention, detection, evaluation, and treatment of high blood pressure; national high blood pressure education program coordinating committee: The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. Jama 2003, 289, 2560–2572. [Google Scholar]
- Ibrahim, M.M.; Damasceno, A. Hypertension in developing countries. Lancet 2012, 380, 611–619. [Google Scholar] [CrossRef]
- O’Donnell, O.; Van Doorslaer, E.; Wagstaff, A.; Lindelow, M. Analyzing Health Equity Using Household Survey Data:A Guide to Techniques and Their Implementation; World Bank Publications: Washington, DC, USA, 2008; pp. 83–93. [Google Scholar]
- Chen, Z. Launch of the health-care reform plan in China. Lancet 2009, 373, 1322–1324. [Google Scholar] [CrossRef]
- Yip, W.C.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Feng, X.L.; Pang, M.; Beard, J. Health system strengthening and hypertension awareness, treatment and control:data from the China Health and Retirement Longitudinal Study. Bull. World Health Organ. 2014, 92, 29–41. [Google Scholar] [CrossRef]
- Xiao, N.; Long, Q.; Tang, X.; Tang, S. A community-based approach to non-communicable chronic disease management within a context of advancing universal health coverage in China: Progress and challenges. BMC Public Health 2014, 14 (Suppl. 2), S2. [Google Scholar] [CrossRef]
- Huang, K.; Song, Y.T.; He, Y.H.; Feng, X.L. Health system strengthening and hypertension management in China. Glob. Health Res. Policy 2016, 1, 13. [Google Scholar] [CrossRef]
- Gu, D.; He, J.; Coxson, P.G.; Rasmussen, P.W.; Huang, C.; Thanataveerat, A.; Tzong, K.Y.; Xiong, J.; Wang, M.; Zhao, D.; et al. The cost-effectiveness of low-cost essential antihypertensive medicines for hypertension control in China: A modelling study. PLoS Med. 2015, 12, e1001860. [Google Scholar] [CrossRef]
- Li, Y.; Ying, C.; Sufang, G.; Brant, P.; Bin, L.; Hipgrave, D. Evaluation, in three provinces, of the introduction and impact of China’s National Essential Medicines Scheme. Bull. World Health Organ. 2013, 91, 184–194. [Google Scholar] [CrossRef]
- Gordon, G.L.; Samantha, A.; Vortherms, X.H. China’s Health Reform Update. Annu. Rev. Public Health 2017, 38, 431–448. [Google Scholar]
- Meng, Q.; Fang, H.; Liu, X.; Yuan, B.; Xu, J. Consolidating the social health insurance schemes in China: Towards an equitable and efficient health system. Lancet 2015, 386, 1484–1492. [Google Scholar] [CrossRef]
- Bleich, S.N.; Cutler, D.M.; Adams, A.S.; Lozano, R.; Murray, C.J. Impact of insurance and supply of health professionals on coverage of treatment for hypertension in Mexico:population based study. BMJ 2007, 335, 875. [Google Scholar] [CrossRef] [PubMed]
- Duru, O.K.; Vargas, R.B.; Kermah, D.; Pan, D.; Norris, K.C. Health insurance status and hypertension monitoring and control in the United States. Am. J. Hypertens. 2007, 20, 348–353. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Whelton, P.K. Elevated systolic blood pressure and risk of cardiovascular and renal disease:overview of evidence from observational epidemiologic studies and randomized controlled trials. Am. Heart J. 1999, 138, 211–219. [Google Scholar] [CrossRef]
- Huttin, C.; Moeller, J.E.; Stafford, R.S. Patterns and costs for hypertension treatment in the United States:clinical, lifestyle and socioeconomic predictors from the 1987 National Medical Expenditures Survey. Clin. Drug Investig. 2000, 20, 181–195. [Google Scholar] [CrossRef]
- Peacock, E.; Krousel-Wood, M. Adherence to antihypertensive therapy. Med. Clin. N. Am. 2017, 101, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Moy, E.; Bartman, B.A.; Weir, M.R. Access to hypertensive care. Effects of income, insurance, and source of care. Arch. Intern. Med. 1995, 155, 1497–1502. [Google Scholar] [CrossRef]
- Shea, S.; Misra, D.; Ehrlich, M.H.; Field, L.; Francis, C.K. Predisposing factors for severe, uncontrolled hypertension in an inner-city minority population. N. Engl. J. Med. 1992, 327, 776–781. [Google Scholar] [CrossRef]
- Liao, Y.; Gilmour, S.; Shibuya, K. Health Insurance Coverage and Hypertension Control in China:Results from the China Health and Nutrition Survey. PLoS ONE 2016, 11, e0152091. [Google Scholar] [CrossRef]
- Wagstaff, A.; Lindelow, M.; Jun, G.; Ling, X.; Juncheng, Q. Extending health insurance to the rural population:an impact evaluation of China’s new cooperative medical scheme. J. Health Econ. 2009, 28, 1–19. [Google Scholar] [CrossRef]
- Gillespie, C.D.; Hurvitz, K.A. Prevalence of Hypertension and Controlled Hypertension-United States, 2007–2010. MMWR Surveill. Summ. 2013, 62, 144–148. [Google Scholar]
- Manning, W.G.; Newhouse, J.P.; Duan, N.; Keeler, E.B.; Leibowitz, A.; Marquis, M.S. Health insurance and the demand for medical care:evidence from a randomized experiment. Am. Econ. Rev. 1987, 77, 251–277. [Google Scholar] [PubMed]
- Basu, S.; Millett, C. Social epidemiology of hypertension in middle-income countries:determinants of prevalence, diagnosis, treatment, and control in the WHO SAGE study. Hypertension 2013, 62, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.J.; Liu, J.; Ge, J.P.; Chen, L.; Zhao, Z.-G.; Yang, W.-Y.; China National Diabetes and Metabolic Disorders Study Group. Prevalence of cardiovascular disease risk factor in the Chinese population: The 2007–2008 China National Diabetes and Metabolic Disorders Study. Eur. Heart J. 2012, 33, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Huxley, R.; Li, L.; Anna, V.; Xie, G.; Yao, C.; Woodward, M.; Li, X.; Chalmers, J.; Gao, R.; et al. Prevalence, awareness, treatment, and control of hypertension in China: Data from the China National Nutrition and Health Survey 2002. Circulation 2008, 118, 2679–2686. [Google Scholar] [CrossRef]
- Chinese Centre for Disease Control and Prevention. Report on Chronic Disease Risk Factor Surveillance in China 2010; Military Medical Science Press: Beijing, China, 2012.
- Gu, D.; Reynolds, K.; Wu, X.; Chen, J.; Duan, X.; Muntner, P.; Huang, G.; Reynolds, R.F.; Su, S.; Whelton, P.K.; et al. Prevalence, awareness, treatment, and control of hypertension in China. Hypertension 2002, 40, 920–927. [Google Scholar] [CrossRef]
- Zhao, Y.; Yan, H.; Marshall, R.J.; Dang, S.; Yang, R.; Li, Q.; Qin, X. Trends in population blood pressure and prevalence, awareness, treatment, and control of hypertension among middle-aged and older adults in a rural area of Northwest China from 1982 to 2010. PLoS ONE 2013, 8, e61779. [Google Scholar] [CrossRef]
- Tian, S.; Dong, G.H.; Wang, D.; Liu, M.M.; Lin, Q.; Meng, X.J.; Xu, L.X.; Hou, H.; Ren, Y.F. Factors associated with prevalence, awareness, treatment and control of hypertension in urban adults from 33 communities in China: The CHPSNE Study. Hypertens. Res. 2011, 34, 1087. [Google Scholar] [CrossRef]
- Ma, Y.Q.; Mei, W.H.; Yin, P.; Yang, X.H.; Rastegar, S.K.; Yan, J.D. Prevalence of hypertension in Chinese cities: A meta-analysis of published studies. PLoS ONE 2013, 8, e58302. [Google Scholar] [CrossRef]
- Ma, W.J.; Tang, J.L.; Zhang, Y.H.; Xu, Y.J.; Lin, J.Y.; Li, J.S.; Lao, X.Q.; Tam, W.W.; Wong, M.C.; Yu, I.T. Hypertension prevalence, awareness, treatment, control, and associated factors in adults in southern China. Am. J. Hypertens. 2012, 25, 590–596. [Google Scholar] [CrossRef] [Green Version]
- Junling, G.; Yang, L.; Junming, D.; Pinpin, Z.; Hua, F. Evaluation of group visits for chinese hypertensives based on primary health care center. Asia Pac. J. Public Health 2015, 27, 350–360. [Google Scholar] [CrossRef]
- Lloyd-Sherlock, P.; Beard, J.; Minicuci, N.; Ebrahim, S.; Chatterji, S. Hypertension among older adults in low- and middle-income countries: Prevalence, awareness and control. Int. J. Epidemiol. 2014, 43, 116–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muntner, P.; Gu, D.; Wu, X.; Duan, X.; Wenqi, G.; Whelton, P.K.; He, J. Factors associated with hypertension awareness, treatment, and control in a representative sample of the chinese population. Hypertension 2004, 43, 578–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firmo, J.O.; Barreto, S.M.; Lima-Costa, M.F. The Bambui Health and Aging Study (BHAS): Factors associated with the treatment of hypertension in older adults in the community. Cad Saude Publica 2003, 19, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Bovet, P.; Ross, A.G.; Gervasoni, J.P.; Mkamba, M.; Mtasiwa, D.M.; Lengeler, C.; Whiting, D.; Paccaud, F. Distribution of blood pressure, body mass index and smoking habits in the urban population of Dar es Salaam, Tanzania, and associations with socioeconomic status. Int. J. Epidemiol. 2002, 31, 240–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheraghali, A.M.; Nikfar, S.; Behmanesh, Y.; Rahimi, V.; Habibipour, F.; Tirdad, R.; Asadi, A.; Bahrami, A. Evaluation of availability, accessibility and prescribing pattern of medicines in the Islamic Republic of Iran. East. Mediterr. Health J. 2004, 10, 406–415. [Google Scholar]
- Palafox, B.; McKee, M.; Balabanova, D.; AlHabib, K.F.; Bahonar, A.; Ismail, N.; Chifamba, J.; Chow, C.K.; Corsi, D.J.; Dagenais, G.R.; et al. Wealth and cardiovascular health: A cross-sectional study of wealth-related inequalities in the awareness, treatment and control of hypertension in high-, middle- and low-income countries. Int. J. Equity Health 2016, 15, 199. [Google Scholar] [CrossRef] [Green Version]
- State Council of the People’s Republic of China. Hypertension and Diabetes Patients’ Burdens to be Eased. 2019. Available online: http://english.www.gov.cn/premier/news/201909/14/content_WS5d7c3559c6d0bcf8c4c135ae.html. (accessed on 14 September 2019).



{kind=link}
{kind=link}
| Measures | Definition |
|---|---|
| Prevalence | Systolic blood pressure ≥140 mmHg and/or diastolic blood pressure≥90 mmHg and/or self-reported antihypertensive medication use at the time of the investigation |
| Hypertension care | |
| Awareness | Hypertensive persons who reported the doctor's diagnosis of hypertension previously or current use of antihypertensive medication |
| Treatment | Identified hypertensive adults who reported current use of antihypertensive medication |
| Control | Identified hypertensive adults whose systolic blood pressure was <140 mmHg and whose diastolic blood pressure was <90 mmHg |
| Health service utilisation | |
| Outpatient visit | ‘In the last month have you visited a public hospital, private hospital, public health centre, clinic, or doctor’s practice, or been visited by a doctor for outpatient care?’ |
| Inpatient visit | ‘Have you received inpatient care in the past year?’ |
| Health education | Health education provided by health professionals, which includes weight control, exercise, healthy diet and aspects of smoking control |
| 2011 | 2013 | 2015 | p Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Unweighted (%) | Weighted (%) | N | Unweighted (%) | Weighted (%) | N | Unweighted (%) | Weighted (%) | ||
| Total population | 13,725 | 100.00 | 100.00 | 10,893 | 100.00 | 100.00 | 11,675 | 100.00 | 100.00 | |
| Prevalence | 5285 | 38.51 | 40.78 | 4666 | 42.83 | 43.25 | 4874 | 41.75 | 41.81 | <0.001 |
| Among people with hypertension | ||||||||||
| Awareness | 2976 | 56.31 | 55.87 | 2876 | 61.64 | 60.04 | 3316 | 68.03 | 68.31 | <0.001 |
| Without comorbidity | 755 | 43.07 | 42.19 | 598 | 46.39 | 44.48 | 734 | 54.29 | 55.80 | <0.001 |
| With comorbidity | 2221 | 62.88 | 63.38 | 2278 | 67.46 | 66.77 | 2582 | 73.31 | 73.32 | <0.001 |
| Medication treatment | 2579 | 48.80 | 48.44 | 2485 | 53.26 | 52.57 | 2980 | 61.14 | 61.97 | <0.001 |
| Without comorbidity | 638 | 36.39 | 35.40 | 473 | 36.70 | 36.39 | 645 | 47.71 | 49.59 | <0.001 |
| With comorbidity | 1941 | 54.95 | 55.60 | 2012 | 59.58 | 59.56 | 2335 | 66.30 | 66.93 | <0.001 |
| Blood pressure control | 1072 | 20.28 | 19.34 | 1064 | 22.80 | 22.19 | 1326 | 27.21 | 28.57 | <0.001 |
| Without comorbidity | 250 | 14.26 | 13.24 | 189 | 14.66 | 12.79 | 268 | 19.82 | 22.96 | <0.001 |
| With comorbidity | 822 | 23.27 | 22.69 | 875 | 25.91 | 26.25 | 1058 | 30.04 | 30.81 | <0.001 |
| Health Service Use | 2011 | 2013 | 2015 | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Unweighted (%) | Weighted (%) | N | Unweighted (%) | Weighted (%) | N | Unweighted (%) | Weighted (%) | ||
| Proportion of outpatient visit | 1029 | 19.72 | 21.24 | 1084 | 23.60 | 23.38 | 988 | 20.62 | 20.60% | 0.105 |
| Without comorbidity | 200 | 11.53 | 13.65 | 166 | 12.98 | 13.16 | 179 | 13.44 | 14.21% | 0.692 |
| With comorbidity | 829 | 23.81 | 25.43 | 918 | 27.70 | 27.84 | 809 | 23.39 | 23.18% | 0.226 |
| Proportion of inpatient visit | 577 | 10.93 | 10.68 | 754 | 16.19 | 17.68 | 861 | 17.72 | 17.41% | <0.001 |
| Without comorbidity | 100 | 5.72 | 5.62 | 93 | 7.24 | 14.73 | 154 | 11.44 | 11.82% | <0.001 |
| With comorbidity | 477 | 13.51 | 13.45 | 661 | 19.60 | 18.95 | 707 | 20.12 | 19.66% | <0.001 |
| Proportion of health education | 1717 | 32.49 | 33.67 | 1713 | 36.71 | 36.55 | 1942 | 39.84 | 39.79% | <0.001 |
| Without comorbidity | 388 | 22.13 | 22.87 | 280 | 21.72 | 22.54 | 413 | 30.55 | 30.37% | <0.001 |
| With comorbidity | 1329 | 37.63 | 39.59 | 1433 | 42.43 | 42.60 | 1529 | 43.41 | 43.57% | <0.001 |
| Wealth Group, PCE (Quintiles) | Awareness | Medication Treatment | BP Control | Outpatient Visit | Inpatient Visit | Health Education |
|---|---|---|---|---|---|---|
| 1st (Poorest) | 64.82% | 57.71% | 24.28% | 17.41% | 8.01% | 31.63% |
| 2nd (Poor) | 65.43% | 59.88% | 27.99% | 21.41% | 14.28% | 41.68% |
| 3rd (Middle) | 71.04% | 63.52% | 32.14% | 17.84% | 17.67% | 46.70% |
| 4th (Rich) | 74.42% | 65.07% | 30.86% | 18.86% | 19.08% | 47.20% |
| 5th (Richest) | 71.97% | 66.66% | 34.32% | 25.65% | 23.27% | 42.95% |
| Ratio (Richest/Poorest) | 1.11 | 1.16 | 1.41 | 1.47 | 2.91 | 1.36 |
| CIc | 0.007 | 0.010 | 0.008 | 0.033 | 0.086 *** | −0.004 |
| Variable (Reference) | SBP-Model 1 | SBP-Model 2 | DBP-Model 1 | DBP-Model 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI | |||||
| Main effects | ||||||||||||
| Treatment (no) | −13.483 | −15.672 | −11.293 | −16.115 | −28.382 | −3.848 | −5.367 | −6.390 | −4.344 | −8.326 | −14.048 | −2.604 |
| Age | −0.386 | −0.674 | −0.097 | −0.388 | −0.677 | −0.100 | −0.121 | −0.255 | 0.013 | −0.121 | −0.255 | 0.013 |
| PCE, Quintile 1st | ||||||||||||
| 2nd | −3.125 | −5.419 | −0.830 | −1.736 | −5.400 | 1.928 | −0.508 | −1.576 | 0.560 | −0.002 | −1.710 | 1.707 |
| 3rd | 0.025 | −2.338 | 2.388 | 2.094 | −1.664 | 5.853 | −0.215 | −1.316 | 0.885 | 0.150 | −1.604 | 1.903 |
| 4th | 0.313 | −2.179 | 2.806 | 2.757 | −1.035 | 6.548 | −0.231 | −1.392 | 0.931 | −0.441 | −2.213 | 1.331 |
| 5th | −2.066 | −4.740 | 0.608 | −0.190 | −4.574 | 4.193 | −0.197 | −1.442 | 1.047 | 0.402 | −1.642 | 2.446 |
| BMI | 0.126 | −0.221 | 0.474 | 0.005 | −0.448 | 0.457 | 0.175 | 0.013 | 0.336 | 0.084 | −0.126 | 0.295 |
| Comorbidity (no) | −1.353 | −4.980 | 2.275 | −1.400 | −5.839 | 3.039 | −1.853 | −3.545 | −0.162 | −1.596 | −3.673 | 0.481 |
| Smoking (no) | 3.492 | −0.586 | 7.569 | 3.327 | −0.759 | 7.413 | 0.130 | −1.773 | 2.032 | 0.133 | −1.773 | 2.040 |
| Drinking (no) | 1.527 | −1.084 | 4.139 | 1.512 | −1.101 | 4.125 | 0.980 | −0.236 | 2.196 | 0.975 | −0.242 | 2.192 |
| Interaction effects | ||||||||||||
| Treatment × PCE | ||||||||||||
| Treatment × 2nd | −2.381 | −7.080 | 2.318 | −0.815 | −3.006 | 1.376 | ||||||
| Treatment × 3rd | −3.459 | −8.169 | 1.251 | −0.629 | −2.824 | 1.566 | ||||||
| Treatment × 4th | −4.090 | −8.879 | 0.698 | 0.353 | −1.882 | 2.587 | ||||||
| Treatment × 5th | −3.078 | −8.323 | 2.167 | −0.885 | −3.329 | 1.559 | ||||||
| Treatment × BMI | 0.204 | −0.262 | 0.670 | 0.146 | −0.072 | 0.363 | ||||||
| Treatment × Comorbidity | 0.134 | −4.080 | 4.348 | −0.423 | −2.396 | 1.550 | ||||||
| Constant | 176.336 | 156.896 | 195.776 | 178.044 | 157.463 | 198.625 | 91.426 | 82.380 | 100.471 | 93.207 | 83.630 | 102.784 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Mahal, A.S.; Haregu, T.N.; Katar, A.; Oldenburg, B.; Zhang, L. Trends and Inequalities in the Health Care and Hypertension Outcomes in China, 2011 to 2015. Int. J. Environ. Res. Public Health 2019, 16, 4578. https://doi.org/10.3390/ijerph16224578
Zhao Y, Mahal AS, Haregu TN, Katar A, Oldenburg B, Zhang L. Trends and Inequalities in the Health Care and Hypertension Outcomes in China, 2011 to 2015. International Journal of Environmental Research and Public Health. 2019; 16(22):4578. https://doi.org/10.3390/ijerph16224578
Chicago/Turabian StyleZhao, Yang, Ajay Singh Mahal, Tilahun Nigatu Haregu, Ameera Katar, Brian Oldenburg, and Luwen Zhang. 2019. "Trends and Inequalities in the Health Care and Hypertension Outcomes in China, 2011 to 2015" International Journal of Environmental Research and Public Health 16, no. 22: 4578. https://doi.org/10.3390/ijerph16224578
APA StyleZhao, Y., Mahal, A. S., Haregu, T. N., Katar, A., Oldenburg, B., & Zhang, L. (2019). Trends and Inequalities in the Health Care and Hypertension Outcomes in China, 2011 to 2015. International Journal of Environmental Research and Public Health, 16(22), 4578. https://doi.org/10.3390/ijerph16224578