Trajectories of Outpatient Service Utilisation of Hypertensive Patients in Tertiary Hospitals in China

 , ,
, ,
Abstract
:1. Introduction
2. Method
2.1. Study Design and Population
2.2. Statistical Analysis
3. Results
3.1. Basic Characteristics of Hypertensive Patients
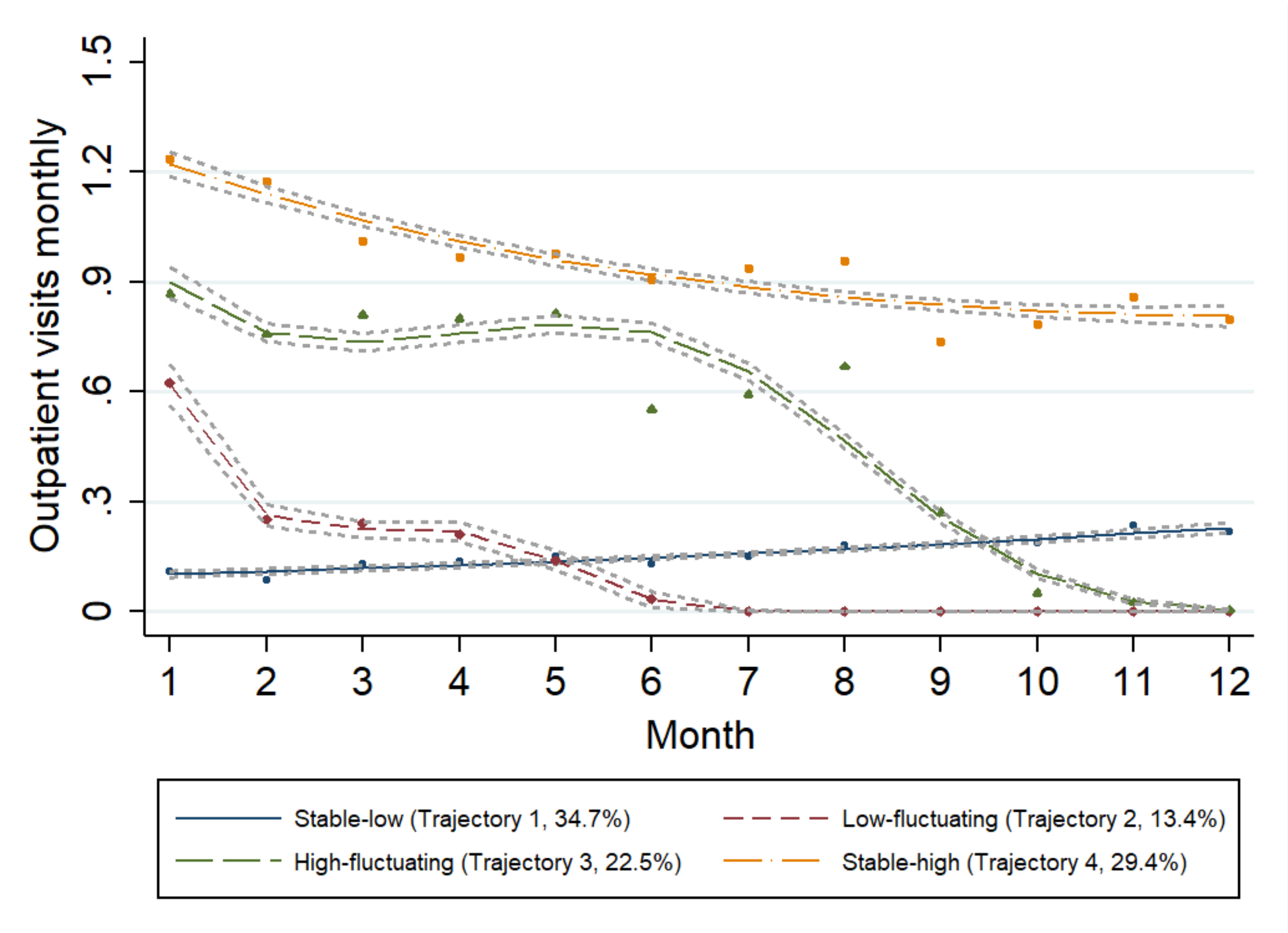
3.2. Trajectories of Outpatient Service Utilisation among Hypertensive Patients
3.3. Differences of the Demographic Characteristics and Medical Service Utilisation-Related Variables Among Different Trajectory Groups
3.4. Determinants of Outpatient Service Utilisation Trajectories
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Chockalingam, A.; Campbell, N.R.; Fodor, J.G. Worldwide epidemic of hypertension. Can. J. Cardiol. 2006, 22, 553–555. [Google Scholar] [CrossRef] [Green Version]
- Bromfield, S.; Muntner, P. High Blood Pressure: The Leading Global Burden of Disease Risk Factor and the Need for Worldwide Prevention Programs. Curr. Hypertens Rep. 2013, 15, 134–136. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Hajjar, I.; Kotchen, T.A. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988–2000. JAMA J. Am. Med. Assoc. 2003, 290, 199–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, S.S.; Fryar, C.; Carroll, M.D. Hypertension Prevalence and Control Among Adults: United States, 2011–2014. Available online: https://www.cdc.gov/nchs/data/databriefs/db220.pdf. (accessed on 25 November 2019).
- Neuhauser, H.K.; Adler, C.; Rosario, A.S.; Diederichs, C.; Ellert, U. Hypertension prevalence, awareness, treatment and control in Germany 1998 and 2008-11. J. Hum. Hypertens. 2015, 29, 247–253. [Google Scholar] [CrossRef]
- Lewington, S.; Lacey, B.; Clarke, R.; Guo, Y.; Kong, X.L.; Yang, L.; Chen, Y.; Bian, Z.; Chen, J.; Meng, J.; et al. The Burden of Hypertension and Associated Risk for Cardiovascular Mortality in China. JAMA Intern. Med. 2016, 176, 524–532. [Google Scholar] [CrossRef]
- Lu, J.; Lu, Y.; Wang, X.; Li, X.; Linderman, G.C.; Wu, C.; Cheng, X.; Mu, L.; Zhang, H.; Liu, J.; et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1.7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet 2017, 390, 2549–2558. [Google Scholar] [CrossRef]
- Wu, Y.; Huxley, R.; Li, L.; Anna, V.; Xie, G.; Yao, C.; Woodward, M.; Li, X.; Chalmers, J.; Gao, R.; et al. Prevalence, awareness, treatment, and control of hypertension in China: Data from the China National Nutrition and Health Survey 2002. Circulation 2008, 118, 2679–2686. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Chen, Z.; Zhang, L.; Wang, X.; Hao, G.; Zhang, Z.; Shao, L.; Tian, Y.; Dong, Y.; Zheng, C.; et al. Status of Hypertension in China: Results From the China Hypertension Survey, 2012–2015. Circulation 2018, 137, 2344–2356. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Li, H.; Liu, F.; Xi, B. Control of hypertension in China: Challenging. Int. J. Cardiol. 2014, 174, 797. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Hu, S.; Li, Y.; Yan, B.; Shen, G.; Wang, L. Systematic review of hypertension clinical practice guidelines based on the burden of disease: A global perspective. J. Evid. Based. Med. 2014, 7, 52–59. [Google Scholar] [CrossRef]
- Ezzati, M.; Vander Hoorn, S.; Lawes, C.M.; Leach, R.; James, W.P.; Lopez, A.D.; Rodgers, A.; Murray, C.J. Rethinking the “diseases of affluence” paradigm: Global patterns of nutritional risks in relation to economic development. PLoS Med. 2005, 2, e133. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Weaver, C.G.; Clement, F.M.; Campbell, N.R.; James, M.T.; Klarenbach, S.W.; Hemmelgarn, B.R.; Tonelli, M.; McBrien, K.A. Healthcare Costs Attributable to Hypertension: Canadian Population-Based Cohort Study. Hypertension 2015, 66, 502–508. [Google Scholar] [CrossRef]
- Mennini, F.S.; Marcellusi, A.; von der Schulenburg, J.M.; Gray, A.; Levy, P.; Sciattella, P.; Soro, M.; Staffiero, G.; Zeidler, J.; Maggioni, A.; et al. Cost of poor adherence to anti-hypertensive therapy in five European countries. Eur. J. Health Econ. 2015, 16, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Gheorghe, A.; Griffiths, U.; Murphy, A.; Legido-Quigley, H.; Lamptey, P.; Perel, P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health 2018, 18, 975. [Google Scholar] [CrossRef] [Green Version]
- Stavreski, B.; Young-soo, S.; Zhao, M.; Hasegawa, T.; Cowie, M.; Garg, R.; Earle, N. The Cost of Silence: Cardiovascular Disease in Asia; The Economist Intelligence Unit: London, UK, 2018. [Google Scholar]
- Li, H. Hypertension Management in Primary Care in China: Still a Long Way to Proceed. J. Gen. Pract. 2016, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Jiang, B.; Li, Y.C.; Zhang, M.; Huang, Z.J.; Liu, Y.; Wang, L.M. Expenditure in outpatient department and pharmacy on patients with hypertension and the influence from community health management program. Zhonghua Liu Xing Bing Xue Za Zhi 2016, 37, 248–253. [Google Scholar] [CrossRef]
- Wang, L.; Kong, L.; Wu, F.; Bai, Y.; Burton, R. Preventing chronic diseases in China. Lancet 2005, 366, 1821–1824. [Google Scholar] [CrossRef]
- Shin, J.; Choi, Y.; Lee, S.G.; Kim, T.H.; Park, E.C. Higher cost sharing for visiting general hospitals and the changing trend in the first-visited healthcare organization among newly diagnosed hypertension patients. Medicine 2016, 95, e4880. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, Y.; Huang, S.; Xie, X. General Situation and Analysis on the Distribution of Outpatient Service Organization and Cost in Patients with Cardio-cerebrovascular Diseases Covered by Fujian Provincial Health Insurance from 2005 to 2014. Chin. Gen. Pract. 2017, 20, 3008–3014. [Google Scholar] [CrossRef]
- Mendis, S.; Johnston, S.C.; Fan, W.; Oladapo, O.; Cameron, A.; Faramawi, M.F. Cardiovascular risk management and its impact on hypertension control in primary care in low-resource settings: a cluster-randomized trial. Bull. World Health Organ. 2010, 88, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.Y.; Jian, W.Y.; Fang, H. Analysis of substitutional effect of outpatient expenditure on inpatient expenditure in hypertensive patients with rural new cooperative medical scheme. Beijing Da Xue Xue Bao Yi Xue Ban 2016, 48, 472–477. [Google Scholar] [PubMed]
- Sui, H.; Wang, W.; Cheng, H.Y.; Cheng, Y.F.; Liu, L.S.; Zhange, W. Characterization, risk stratification and the hypertension control rate at hospital-based clinics: a survey of 25,336 hypertensives in Beijing, Shanghai and Guangzhou. Intern. Med. 2013, 52, 1863–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shechang, L. Control of Hypertension, Medication Adherence and Their Correlates in Chinese Hypertensive Outpatients in Tertiary Hospitals. Master’s Thesis, Fudan University, Shanghai, China, 2012. [Google Scholar]
- Shi, L.; Lee, D.C.; Liang, H.; Zhang, L.; Makinen, M.; Blanchet, N.; Kidane, R.; Lindelow, M.; Wang, H.; Wu, S. Community health centers and primary care access and quality for chronically-ill patients - a case-comparison study of urban Guangdong Province, China. Int. J. Equity Health 2015, 14, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, D.Y.; Liu, L.S.; Yu, J.M.; Yao, C.H.; China, S.S.G. National survey of blood pressure control rate in Chinese hypertensive outpatients-China STATUS. Zhonghua Xin Xue Guan Bing Za Zhi 2010, 38, 230–238. [Google Scholar]
- Shima, A.; Tatsumi, Y.; Ishizaki, T.; Godai, K.; Kawatsu, Y.; Okamura, T.; Nishikawa, T.; Morimoto, A.; Morino, A.; Miyamatsu, N. Relationship between outpatient visit frequency and hypertension control: a 9-year occupational cohort study. Hypertens Res. 2016, 39, 376–381. [Google Scholar] [CrossRef]
- Guthmann, R.; Davis, N.; Brown, M.; Elizondo, J. Visit frequency and hypertension. J. Clin. Hypertens (Greenwich) 2005, 7, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Berlin, K.S.; Parra, G.R.; Williams, N.A. An introduction to latent variable mixture modeling (part 2): longitudinal latent class growth analysis and growth mixture models. J. Pediatr. Psychol. 2014, 39, 188–203. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D.S. A Note on a Stata Plugin for Estimating Group-based Trajectory Models. Sociol Method Res. 2013, 42, 608–613. [Google Scholar] [CrossRef]
- Rhebergen, D.; Huisman, A.; Bouckaert, F.; Kho, K.; Kok, R.; Sienaert, P.; Spaans, H.P.; Stek, M. Older Age Is Associated with Rapid Remission of Depression After Electroconvulsive Therapy: A Latent Class Growth Analysis. Am. J. Geriat. Psychiat. 2015, 23, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Ye, T.; Zhang, P.; Ouyang, Z.L.; Yang, J.J.; Xu, C.Z.; Pan, Z.J.; Wu, Z.Z.; Zhang, L.; Li, B.Y. Multi-trajectory modeling of home blood pressure telemonitoring utilization among hypertensive patients in China: A latent class growth analysis. Int. J. Med. Inform 2018, 119, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.L.; Mendoza, T.R.; Gunn, G.B.; Wang, X.S.; Rosenthal, D.I.; Cleeland, C.S. Using group-based trajectory modeling to examine heterogeneity of symptom burden in patients with head and neck cancer undergoing aggressive non-surgical therapy. Qual. Life. Res. 2013, 22, 2331–2339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Jiang, S.; He, R.B.; Dong, Y.H.; Pan, Z.J.; Xu, C.Z.; Lu, F.F.; Zhang, P.; Zhang, L. Trajectories of Hospitalization Cost Among Patients of End-Stage Lung Cancer: A Retrospective Study in China. Int. J. Env. Res. Pub. He. 2018, 15, E2877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckman, K.D. How to document and code for hypertensive diseases in ICD-10. Fam. Pract. Manag. 2014, 21, 5–9. [Google Scholar]
- ICD-10-CM Official Guidelines for Coding and Reporting 2012 ICD-10-CM and GEMs: 2012. Available online: https://www.cms.gov/Medicare/Coding/ICD10/Downloads/2019-ICD10-Coding-Guidelines-.pdf (accessed on 25 November 2019).
- Nagin, D.S.; Land, K.C.J.C. Age, criminal careers, and population heterogeneity: Specification and estimation of a nonparametric, mixed Poisson model. Criminology 1993, 31, 327–362. [Google Scholar] [CrossRef]
- Twisk, J.; Hoekstra, T. Classifying developmental trajectories over time should be done with great caution: A comparison between methods. J. Clin. Epidemiol. 2012, 65, 1078–1087. [Google Scholar] [CrossRef]
- Huang, H.C.; Chang, C.H.; Lee, T.H.; Chang, Y.J.; Ryu, S.J.; Chang, T.Y.; Huang, K.L.; Liu, C.H.; Chang, H.J. Differential trajectory of functional recovery and determinants for first time stroke survivors by using a LCGA approach: a hospital based analysis over a 1-year period. Eur. J. Phys. Rehabil. Med. 2013, 49, 463–472. [Google Scholar]
- Jones, B.L.; Nagin, D.S. Advances in group-based trajectory modeling and an SAS procedure for estimating them. Sociol. Method Res. 2007, 35, 542–571. [Google Scholar] [CrossRef] [Green Version]
- Neelon, B.H.; O’Malley, A.J.; Normand, S.L.T. A Bayesian model for repeated measures zero-inflated count data with application to outpatient psychiatric service use. Stat. Model 2010, 10, 421–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nylund, K.L.; Asparouhov, T.; Muthen, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study (vol 14, pg 535, 2007). Struct. Equ. Modeling 2008, 15, 182. [Google Scholar]
- Lin, F.; Jia, G.; Yu, J.-M.; Hu, D. Blood pressure control rate and its influencing factors in Chinese hypertensive outpatients. Chin. J. Hypertens. 2013, 21, 170–174. [Google Scholar]
- Ashfaq, T.; Anjum, Q.; Siddiqui, H.; Shaikh, S.; Vohra, E.A. Awareness of hypertension among patients attending primary health care centre and outpatient department of tertiary care hospital of Karachi. J. Pak. Med. Assoc. 2007, 57, 396–399. [Google Scholar] [PubMed]
- Notara, V.; Panagiotakos, D.B.; Kogias, Y.; Stravopodis, P.; Antonoulas, A.; Zombolos, S.; Mantas, Y.; Pitsavos, C. The Impact of Educational Status on 10-Year (2004–2014) Cardiovascular Disease Prognosis and All-cause Mortality Among Acute Coronary Syndrome Patients in the Greek Acute Coronary Syndrome (GREECS) Longitudinal Study. J. Prev. Med. Public Health 2016, 49, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Y.J.; Wang, H.C.; Li, Y.C.; Zhao, W.H. Hypertension Screening and Follow-up Management by Primary Health Care System among Chinese Population Aged 35 Years and Above. Biomed. Environ. Sci. 2015, 28, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Wang, H.; Wang, Z.; Su, C.; Zhang, J.; Zhang, B.J. Medical cost attributable to hypertension among Chinese middle and old aged residents in 2011. Wei Sheng Yan Jiu 2017, 46, 246–250. [Google Scholar]
- Park, C.; Fang, J.; Hawkins, N.A.; Wang, G. Comorbidity Status and Annual Total Medical Expenditures in U.S. Hypertensive Adults. Am. J. Prev. Med. 2017, 53, S172–S181. [Google Scholar] [CrossRef] [Green Version]
- Bovet, P.; Gervasoni, J.P.; Mkamba, M.; Balampama, M.; Lengeler, C.; Paccaud, F. Low utilization of health care services following screening for hypertension in Dar es Salaam (Tanzania): A prospective population-based study. BMC Public Health 2008, 8, 407. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Shi, L.; Li, S.; Xu, L.; Qin, W.; Wang, H. Urban-rural disparities in hypertension prevalence, detection, and medication use among Chinese Adults from 1993 to 2011. Int. J. Equity Health 2017, 16, 50. [Google Scholar] [CrossRef] [Green Version]
- Xiaohui, H. Urban-rural disparity of overweight, hypertension, undiagnosed hypertension, and untreated hypertension in China. Asia. Pac. J. Public Health 2008, 20, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Su, M.; Fang, P.Q.; Xu, J. Analysis on Medical Expenses of Hypertensive Inpatients in Urban Areas from 2010 to 2013-Evidence from Two Provinces in South of China. Curr. Med. Sci. 2018, 38, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Bundy, J.D.; He, J. Hypertension and Related Cardiovascular Disease Burden in China. Ann. Glob. Health 2016, 82, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Wang, G.; Zhang, P.; Fang, J.; Ayala, C. Medical Expenditures Associated With Hypertension in the U.S., 2000–2013. Am. J. Prev. Med. 2017, 53, S164–S171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.; Gao, J.; Jin, G. Effects and Expense of Blood Pressure Control on Hypertensive Patients Using Different Treatment Methods:A Comparative Study. Chin. Gen. Pract. 2016, 19, 96–99. [Google Scholar]
- Shao, H.; Mohammed, M.U.; Thomas, N.; Babazadeh, S.; Yang, S.; Shi, Q.; Shi, L.Z. Evaluating Excessive Burden of Depression on Health Status and Health Care Utilization Among Patients With Hypertension in a Nationally Representative Sample From the Medial Expenditure Panel Survey (MEPS 2012). J. Nerv. Ment. Dis. 2017, 205, 397–404. [Google Scholar] [CrossRef]
- Kirkland, E.B.; Heincelman, M.; Bishu, K.G.; Schumann, S.O.; Schreiner, A.; Axon, R.N.; Mauldin, P.D.; Moran, W.P. Trends in Healthcare Expenditures Among US Adults With Hypertension: National Estimates, 2003-2014. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Van den Bussche, H.; Schon, G.; Kolonko, T.; Hansen, H.; Wegscheider, K.; Glaeske, G.; Koller, D. Patterns of ambulatory medical care utilization in elderly patients with special reference to chronic diseases and multimorbidity—Results from a claims data based observational study in Germany. BMC Geriatr. 2011, 11. [Google Scholar] [CrossRef] [Green Version]
- Beckett, N.; Peters, R.; Tuomilehto, J.; Swift, C.; Sever, P.; Potter, J.; McCormack, T.; Forette, F.; Gil-Extremera, B.; Dumitrascu, D.; et al. Immediate and late benefits of treating very elderly people with hypertension: results from active treatment extension to Hypertension in the Very Elderly randomised controlled trial. BMJ Br. Med. J. 2012, 344. [Google Scholar] [CrossRef] [Green Version]
- Feldman, P.H.; McDonald, M.V.; Barron, Y.; Gerber, L.M.; Peng, T.R. Home-based interventions for black patients with uncontrolled hypertension: A cluster randomized controlled trial. J. Comp. Eff. Res. 2016, 5, 155–168. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; Zhou, W.; Huang, C.; Huang, S. A cross-sectional survey of self-rated health and its determinants in patients with hypertension. Appl. Nurs. Res. 2015, 28, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Palladino, R.; Lee, J.T.; Ashworth, M.; Triassi, M.; Millett, C. Associations between multimorbidity, healthcare utilisation and health status: Evidence from 16 European countries. Age Ageing 2016, 45, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Fang, J.; Zhao, G.X.; Wang, G.J.; Ayala, C.; Loustalot, F. Insurance Status Among Adults With Hypertension-The Impact of Underinsurance. J. Am. Heart Assoc. 2016, 5, e004313. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Gilmour, S.; Shibuya, K. Health Insurance Coverage and Hypertension Control in China: Results from the China Health and Nutrition Survey. PLoS ONE 2016, 11, e0152091. [Google Scholar] [CrossRef]
- Yu, B.; Zhang, X.; Wang, G. Full coverage for hypertension drugs in rural communities in China. Am. J. Manag. Care 2013, 19, e22–e29. [Google Scholar]
- Gu, D.; He, J.; Coxson, P.G.; Rasmussen, P.W.; Huang, C.; Thanataveerat, A.; Tzong, K.Y.; Xiong, J.; Wang, M.; Zhao, D.; et al. The Cost-Effectiveness of Low-Cost Essential Antihypertensive Medicines for Hypertension Control in China: A Modelling Study. PLoS Med. 2015, 12, e1001860. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Overall (N = 9822) | Trajectory 1 (N = 3330) | Trajectory 2 (N = 1519) | Trajectory 3 (N = 2279) | Trajectory 4 (N = 2694) | χ2/F | p-Value |
|---|---|---|---|---|---|---|---|
| Age | |||||||
| <45 | 778, 7.9% | 388, 11.7% | 233, 15.3% | 79, 3.5% | 78, 2.9% | 446.24 | p < 0.001 |
| 45–64 | 3953, 40.2% | 1380, 41.4% | 669, 44.0% | 911, 40.0% | 993, 36.9% | ||
| 65–80 | 4109, 41.8% | 1289, 38.7% | 490, 32.3% | 985, 43.2% | 1345, 49.9% | ||
| >80 | 982, 10.0% | 273, 8.2% | 127, 8.4% | 304, 13.3% | 278, 10.3% | ||
| Gender | |||||||
| Male | 5278, 53.7% | 1720, 51.7% | 790, 52.0% | 1170, 51.3% | 1598, 59.3% | 46.67 | p < 0.001 |
| Female | 4544, 46.3% | 1610, 48, 3% | 729, 48.0% | 1109, 48, 7% | 1096, 40.7% | ||
| Marital status | |||||||
| Married | 6983, 71.1% | 2445, 73.4% | 1089, 71.7% | 1311, 57.5% | 2138, 79.4% | 302.85 | p < 0.001 |
| Others | 2839, 28.9% | 885, 26.6% | 430, 28.3% | 968, 42.5% | 556, 20.6% | ||
| Place of residence | |||||||
| Urban | 7379, 75.1% | 2504, 75.2% | 1071, 70.5% | 1508, 66.2% | 2296, 85.2% | 262.27 | p < 0.001 |
| Rural area | 2443, 24.9% | 826, 24.8% | 448, 29.5% | 771, 33.8% | 398, 14.8% | ||
| Education | |||||||
| University | 540, 5.5% | 206, 6.2% | 92, 6.1% | 82, 3.6% | 160, 5.9% | 442.24 | p < 0.001 |
| Senior high school | 2518, 25.6% | 862, 25.9% | 396, 26.1% | 622, 27.3% | 638, 23.7% | ||
| Junior high school | 2264, 23.1% | 793, 23.8% | 332, 21.9% | 324, 14.2% | 815, 30.3% | ||
| Primary school | 2264, 23.1% | 407, 12.2% | 174, 11.5% | 171, 7.5% | 430, 16.0% | ||
| Others | 3318, 33.8% | 1062, 31.9% | 525, 34.6% | 1080, 47.4% | 651, 24.2% | ||
| Follow-up | 206, 2.1% | 103, 3.1% | 50, 3.3% | 25, 1.1% | 28, 1.0% | 52.43 | p < 0.001 |
| Outpatient visit times | 5.59 (4.729) | 1.88 (1.22) | 1.49 (0.79) | 6.53 (1.86) | 11.70 (3.44) | 12508.8 | p < 0.001 |
| Inpatient service utilisation | 3027, 30.8% | 1146, 34.4% | 444, 29.2% | 562, 24.7% | 875, 32.5% | 66.02 | p < 0.001 |
| Outpatient cost | 227.09 (262.12) | 85.64 (163.26) | 60.49 (70.00) | 244.21 (137.99) | 481.39 (305.62) | 2373.74 | p < 0.001 |
| Inpatient cost | 758.85 (2467.85) | 826.73 (2556.89) | 725.84 (2780.33) | 657.79 (2646.32) | 779.05 (1957.79) | 2.265 | 0.079 |
| Medical cost | 985.74 (2497.20) | 912.37 (2574.25) | 786.34 (2783.53) | 902.00 (2663.67) | 1260.44 (2017.52) | 15.98 | p < 0.001 |
| Number of Class | Polynomial Order of Coefficients | BIC | AIC | Log Bayes Factor |
|---|---|---|---|---|
| Hypertension patient outpatient service utilisation trajectory | ||||
| 1 | 1 | −100,803.52 | −100,797.61 | 100,795.61 |
| 2 | 22 | −92,401.84 | −92,376.67 | −92,369.67 |
| 3 | 232 | −91,291.47 | −91,248.32 | −91,236.32 |
| 4 | 1332 | −91,036.24 | −90,978.7 | −90,962.7 |
| Variables | Trajectory 2 | Trajectory 3 | Trajectory 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | OR (95%CI) | p-Value | β | OR(95%CI) | p-Value | β | OR(95%CI) | p-Value | |
| Age | |||||||||
| ≤45 | 0.071 | 1.074 (0.812–1.420) | 0.616 | −0.655 | 0.519 (0.295–0.915) | 0.023 | 0.152 | 1.165 (0.539–2.517) | 0.698 |
| 45–65 | −0.055 | 0.947 (0.745–1.203) | 0.656 | −0.245 | 0.783 (0.541–1.133) | 0.194 | 0.123 | 1.130 (0.709–1.801) | 0.606 |
| 65–80 | −0.206 | 0.814 (0.640–1.036) | 0.094 | −0.459 | 0.632 (0.439–0.909) | 0.013 | −0.240 | 0.786 (0.498–1.241) | 0.302 |
| Gender | 0.039 | 1.039 (0.918–1.177) | 0.544 | −0.095 | 0.910 (0.729–1.135) | 0.403 | 0.140 | 1.151 (0.869–1.523) | 0.326 |
| Marital (married) | 0.018 | 1.018 (0.859–1.207) | 0.835 | −0.327 | 0.721 (0.527–0.987) | 0.041 | 0.221 | 1.247 (0.836–1.859) | 0.279 |
| Place of residence (urban area) | −0.189 | 0.828 (0.710–0.965) | 0.016 | −0.244 | 0.784 (0.584–1.051) | 0.103 | 0.098 | 1.103 (0.751–1.619) | 0.617 |
| Education | |||||||||
| University | −0.087 | 0.917 (0.686–1.227) | 0.560 | −0.318 | 0.727 (0.410–1.291) | 0.277 | 0.329 | 1.390 (0.680–2.838) | 0.367 |
| Senior high school | 0.012 | 1.012 (0.836–1.225) | 0.905 | 0.105 | 1.111 (0.788–1.566) | 0.549 | 0.043 | 1.044 (0.674–1.617) | 0.847 |
| Junior high school | −0.121 | 0.886 (0.733–1.070) | 0.209 | −0.474 | 0.622 (0.437–0.887) | 0.009 | 0.398 | 1.489 (0.955–2.321) | 0.079 |
| Primary school | −0.025 | 0.976 (0.777–1.226) | 0.832 | −0.526 | 0.591 (0.389–0.896) | 0.013 | 0.567 | 1.763 (1.044–2.976) | 0.034 |
| Follow-up | 0.060 | 1.062 (0.745–1.513) | 0.739 | −0.034 | 0.967 (0.450–2.076) | 0.931 | 0.259 | 1.295 (0.440–3.810) | 0.639 |
| Outpatient visit times, | −0.335 | 0.715 (0.663–0.772) | <0.001 | 1.652 | 5.219 (4.748–5.737) | <0.001 | 2.460 | 11.700 (10.524–13.007) | <0.001 |
| Inpatient service utilisation | −0.182 | 0.833 (0.717–0.969) | 0.018 | -0.387 | 0.679 (0.525–0.879) | 0.003 | 0.049 | 1.051 (0.748–1.476) | 0.776 |
| Outpatient cost | −0.888 | 0.412 (0.179–0.944) | 0.036 | -1.391 | 0.249 (0.123–0.502) | <0.001 | 0.313 | 1.367 (0.733–2.549) | 0.325 |
| Total cost | 0.009 | 1.009 (0.983–1.036) | 0.492 | 0.021 | 1.021 (0.982–1.062) | <0.001 | 0.026 | 1.026 (0.967–1.090) | 0.393 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, Z.; Xu, W.; Li, Z.; Xu, C.; Lu, F.; Zhang, P.; Zhang, L.; Ye, T. Trajectories of Outpatient Service Utilisation of Hypertensive Patients in Tertiary Hospitals in China. Int. J. Environ. Res. Public Health 2020, 17, 852. https://doi.org/10.3390/ijerph17030852
Pan Z, Xu W, Li Z, Xu C, Lu F, Zhang P, Zhang L, Ye T. Trajectories of Outpatient Service Utilisation of Hypertensive Patients in Tertiary Hospitals in China. International Journal of Environmental Research and Public Health. 2020; 17(3):852. https://doi.org/10.3390/ijerph17030852
Chicago/Turabian StylePan, Zijing, Wanchun Xu, Zhong Li, Chengzhong Xu, Fangfang Lu, Pei Zhang, Liang Zhang, and Ting Ye. 2020. "Trajectories of Outpatient Service Utilisation of Hypertensive Patients in Tertiary Hospitals in China" International Journal of Environmental Research and Public Health 17, no. 3: 852. https://doi.org/10.3390/ijerph17030852
APA StylePan, Z., Xu, W., Li, Z., Xu, C., Lu, F., Zhang, P., Zhang, L., & Ye, T. (2020). Trajectories of Outpatient Service Utilisation of Hypertensive Patients in Tertiary Hospitals in China. International Journal of Environmental Research and Public Health, 17(3), 852. https://doi.org/10.3390/ijerph17030852