Neighborhood Walkability in Relation to Knee and Low Back Pain in Older People: A Multilevel Cross-Sectional Study from the JAGES

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Methods
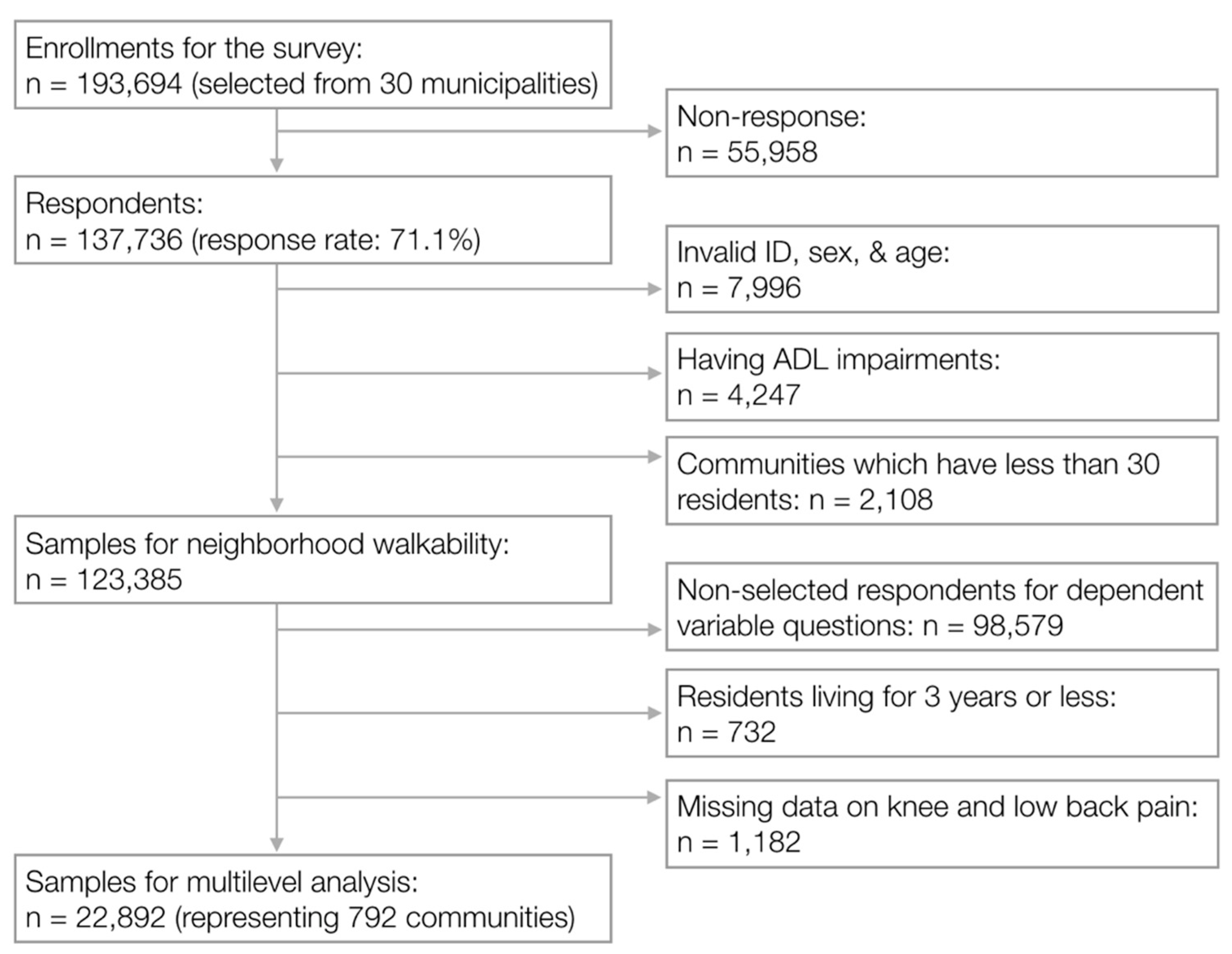
2.1. Study Design and Participants
2.2. Outcome Variables
2.3. Neighborhood Walkability
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Access to Parks and Sidewalks | Access to Fresh Food Stores | Easy Walking without Slopes or Stairs | Population Density | ||
|---|---|---|---|---|---|
| PR (95% CI) | PR (95% CI) | PR (95% CI) | PR (95% CI) | ||
| Sex | Male | ref | ref | ref | ref |
| Female | 1.51 (1.42–1.60) | 1.51 (1.43–1.60) | 1.51 (1.43–1.61) | 1.50 (1.42–1.59) | |
| Age, years | 65–69 | ref | ref | ref | ref |
| 70–74 | 1.21 (1.12–1.30) | 1.20 (1.12–1.30) | 1.20 (1.12–1.30) | 1.21 (1.12–1.30) | |
| 75–79 | 1.45 (1.34–1.56) | 1.45 (1.34–1.56) | 1.45 (1.34–1.56) | 1.45 (1.35–1.57) | |
| 80–84 | 1.68 (1.54–1.83) | 1.68 (1.54–1.83) | 1.68 (1.54–1.83) | 1.68 (1.54–1.83) | |
| 85+ | 1.74 (1.57–1.94) | 1.75 (1.57–1.94) | 1.75 (1.57–1.95) | 1.74 (1.56–1.94) | |
| Educational background, years | 13+ | ref | ref | ref | ref |
| 10–12 | 1.06 (0.98–1.15) | 1.07 (0.98–1.15) | 1.07 (0.99–1.16) | 1.06 (0.98–1.15) | |
| <10 | 1.16 (1.07–1.25) | 1.17 (1.08–1.26) | 1.18 (1.09–1.28) | 1.15 (1.06–1.25) | |
| Missing | 1.17 (0.95–1.42) | 1.17 (0.96–1.42) | 1.19 (0.97–1.45) | 1.15 (0.95–1.41) | |
| Equivalent annual income, yen | 4.0+ million | ref | ref | ref | ref |
| 2.0–3.9 million | 1.22 (1.10–1.35) | 1.22 (1.10–1.35) | 1.22 (1.10–1.36) | 1.21 (1.09–1.35) | |
| <2.0 million | 1.02 (0.92–1.14) | 1.03 (0.92–1.14) | 1.03 (0.92–1.14) | 1.02 (0.92–1.14) | |
| Missing | 1.09 (0.97–1.22) | 1.10 (0.98–1.23) | 1.10 (0.98–1.23) | 1.09 (0.97–1.22) | |
| Past occupation | White-collar worker | ref | ref | ref | ref |
| Blue-collar worker | 1.08 (1.01–1.15) | 1.08 (1.01–1.15) | 1.08 (1.01–1.15) | 1.07 (1.01–1.14) | |
| Primary industry worker | 1.56 (1.41–1.73) | 1.56 (1.45–1.72) | 1.60 (1.45–1.77) | 1.53 (1.37–1.69) | |
| Never worked | 1.13 (1.01–1.26) | 1.13 (1.01–1.26) | 1.13 (1.01–1.26) | 1.12 (1.01–1.25) | |
| Missing | 1.16 (1.06–1.27) | 1.16 (1.07–1.27) | 1.16 (1.07–1.27) | 1.15 (1.05–1.26) | |
| Walking time, min | 60+ | ref | ref | ref | ref |
| 30–59 | 1.20 (1.13–1.29) | 1.21 (1.13–1.29) | 1.21 (1.13–1.29) | 1.20 (1.13–1.29) | |
| <30 | 1.11 (1.05–1.18) | 1.11 (1.05–1.18) | 1.11 (1.04–1.18) | 1.11 (1.05–1.19) | |
| Missing | 1.10 (0.93–1.30) | 1.10 (0.93–1.30) | 1.11 (0.94–1.32) | 1.09 (0.92–1.29) | |
| Physical activity | Daily | ref | ref | ref | ref |
| Weekly | 1.06 (0.98–1.14) | 1.06 (0.98–1.14) | 1.05 (0.98–1.13) | 1.06 (0.99–1.14) | |
| Annually | 1.10 (1.00–1.20) | 1.10 (1.00–1.20) | 1.09 (1.00–1.19) | 1.10 (1.01–1.20) | |
| None | 1.22 (1.13–1.32) | 1.22 (1.13–1.32) | 1.21 (1.13–1.31) | 1.23 (1.14–1.32) | |
| Missing | 1.15 (1.04–1.27) | 1.15 (1.04–1.27) | 1.15 (1.04–1.26) | 1.15 (1.04–1.27) | |
| Driving status | No | ref | ref | ref | ref |
| Yes | 1.02 (0.94–1.08) | 1.04 (0.96–1.08) | 1.04 (0.98–1.10) | 1.01 (0.95–1.07) | |
| Body mass index, kg/m2 | 18.5–24.9 | ref | ref | ref | ref |
| <18.5 | 0.77 (0.69–0.87) | 0.78 (0.70–0.87) | 0.78 (0.69–0.87) | 0.77 (0.69–0.87) | |
| 25+ | 1.38 (1.31–1.46) | 1.38 (1.31–1.46) | 1.39 (1.32–1.47) | 1.38 (1.31–1.46) | |
| Missing | 1.00 (0.60–1.67) | 1.01 (0.61–1.67) | 1.01 (0.61–1.68) | 1.02 (0.62–1.70) | |
| Depression | None (GDS < 5) | ref | ref | ref | ref |
| Mild (GDS of 5–9) | 1.52 (1.42–1.62) | 1.52 (1.43–1.63) | 1.52 (1.43–1.63) | 1.52 (1.43–1.63) | |
| Severe (GDS ≥ 10) | 1.79 (1.62–1.96) | 1.79 (1.62–1.96) | 1.79 (1.63–1.97) | 1.78 (1.62–1.96) | |
| Missing | 1.20 (1.12–1.29) | 1.20 (1.12–1.29) | 1.20 (1.12–1.29) | 1.20 (1.12–1.29) |
| Access to Parks and Sidewalks | Access to Fresh Food Stores | Easy Walking without Slopes or Stairs | Population Density | ||
|---|---|---|---|---|---|
| PR (95% CI) | PR (95% CI) | PR (95% CI) | PR (95% CI) | ||
| Sex | Male | ref | ref | ref | ref |
| Female | 1.17 (1.11–1.23) | 1.17 (1.11–1.23) | 1.17 (1.11–1.23) | 1.17 (1.11–1.23) | |
| Age, years | 65–69 | ref | ref | ref | ref |
| 70–74 | 1.03 (0.96–1.10) | 1.03 (0.97–1.11) | 1.03 (0.96–1.10) | 1.03 (0.97–1.10) | |
| 75–79 | 1.18 (1.10–1.27) | 1.18 (1.10–1.27) | 1.18 (1.10–1.27) | 1.18 (1.10–1.27) | |
| 80–84 | 1.28 (1.18–1.39) | 1.28 (1.18–1.39) | 1.28 (1.18–1.39) | 1.28 (1.18–1.39) | |
| 85+ | 1.41 (1.28–1.56) | 1.41 (1.27–1.56) | 1.41 (1.28–1.56) | 1.41 (1.27–1.55) | |
| Educational background, years | 13+ | ref | ref | ref | ref |
| 10–12 | 1.02 (0.95–1.09) | 1.02 (0.95–1.09) | 1.02 (0.95–1.11) | 1.02 (0.95–1.09) | |
| <10 | 1.07 0.99–1.15) | 1.06 0.99–1.14) | 1.07 1.00–1.15) | 1.05 0.98–1.13) | |
| Missing | 1.01 (0.82–1.24) | 1.01 (0.82–1.23) | 1.01 (0.83–1.25) | 1.00 (0.81–1.22) | |
| Equivalent annual income, yen | 4.0+ million | ref | ref | ref | ref |
| 2.0–3.9 million | 1.25 (1.13–1.37) | 1.24 (1.13–1.37) | 1.25 (1.13–1.38) | 1.24 (1.13–1.37) | |
| <2.0 million | 1.11 (1.01–1.23) | 1.11 (1.01–1.23) | 1.11 (1.01–1.23) | 1.11 (1.00–1.23) | |
| Missing | 1.14 (1.02–1.27) | 1.14 (1.02–1.27) | 1.14 (1.03–1.28) | 1.14 (1.02–1.27) | |
| Past occupation | White-collar worker | ref | ref | ref | ref |
| Blue-collar worker | 1.01 (0.96–1.08) | 1.01 (0.96–1.07) | 1.01 (0.96–1.08) | 1.01 (0.95–1.07) | |
| Primary industry worker | 1.46 (1.33–1.61) | 1.44 (1.31–1.59) | 1.46 (1.34–1.63) | 1.41 (1.28–1.56) | |
| Never worked | 1.09 (0.98–1.22) | 1.09 (0.98–1.21) | 1.09 (0.98–1.22) | 1.09 (0.98–1.21) | |
| Missing | 1.09 (1.00–1.19) | 1.09 (0.99–1.18) | 1.09 (1.00–1.19) | 1.08 (0.99–1.18) | |
| Walking time, min | 60+ | ref | ref | ref | ref |
| 30–59 | 1.28 (1.20–1.36) | 1.28 (1.20–1.36) | 1.28 (1.20–1.36) | 1.28 (1.20–1.36) | |
| <30 | 1.11 (1.05–1.18) | 1.11 (1.05–1.18) | 1.11 (1.05–1.18) | 1.11 (1.05–1.18) | |
| Missing | 1.13 (0.95–1.33) | 1.13 (0.95–1.32) | 1.13 (0.96–1.34) | 1.13 (0.95–1.32) | |
| Physical activity | Daily | ref | ref | ref | ref |
| Weekly | 1.09 (1.02–1.17) | 1.09 (1.02–1.17) | 1.09 (1.02–1.17) | 1.09 (1.02–1.17) | |
| Annually | 1.06 (0.98–1.15) | 1.06 (0.98–1.15) | 1.06 (0.97–1.15) | 1.06 (0.98–1.15) | |
| None | 1.19 (1.11–1.28) | 1.19 (1.11–1.28) | 1.19 (1.11–1.27) | 1.19 (1.11–1.28) | |
| Missing | 1.20 (1.09–1.32) | 1.20 (1.10–1.32) | 1.20 (1.09–1.32) | 1.21 (1.10–1.33) | |
| Driving status | No | ref | ref | ref | ref |
| Yes | 1.08 (1.02–1.14) | 1.08 (1.02–1.14) | 1.09 (1.03–1.15) | 1.08 (1.01–1.13) | |
| Body mass index, kg/m2 | 18.5–24.9 | ref | ref | ref | ref |
| <18.5 | 0.96 (0.87–1.05) | 0.96 (0.87–1.05) | 0.96 (0.87–1.05) | 0.96 (0.87–1.05) | |
| 25+ | 1.18 (1.12–1.25) | 1.18 (1.12–1.25) | 1.18 (1.12–1.25) | 1.18 (1.12–1.25) | |
| Missing | 1.12 (0.72–1.73) | 1.12 (0.72–1.73) | 1.12 (0.72–1.73) | 1.14 (0.73–1.76) | |
| Depression | None (GDS < 5) | ref | ref | ref | ref |
| Mild (GDS of 5–9) | 1.53 (1.44–1.63) | 1.53 (1.44–1.63) | 1.53 (1.44–1.63) | 1.53 (1.44–1.63) | |
| Severe (GDS ≥ 10) | 1.81 (1.65–1.98) | 1.81 (1.65–1.98) | 1.81 (1.65–1.98) | 1.80 (1.64–1.97) | |
| Missing | 1.31 (1.23–1.44) | 1.31 (1.23–1.40) | 1.31 (1.23–1.40) | 1.31 (1.22–1.40) |
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sanchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Arden, N.K. Strategies for the prevention of knee osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.; Maher, C.G.; Pereira, L.S.; Stevens, M.L.; Oliveira, V.C.; Chapple, M.; Teixeira-Salmela, L.F.; Hancock, M.J. Prevention of Low Back Pain: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2016, 176, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Silverwood, V.; Blagojevic-Bucknall, M.; Jinks, C.; Jordan, J.L.; Protheroe, J.; Jordan, K.P. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Japan Sports Agency. Opinion Survey about the Implementation Situation of Sports; Ministry of Health, Labour, and Welfare: Tokyo, Japan, 2019.
- Ministry of Health, Labour, and Welfare. Basic Survey on National Life; Ministry of Health; Ministry of Health, Labour, and Welfare: Tokyo, Japan, 2016.
- Bhatnagar, A. Environmental Determinants of Cardiovascular Disease. Circ. Res. 2017, 121, 162–180. [Google Scholar] [CrossRef]
- den Braver, N.R.; Lakerveld, J.; Rutters, F.; Schoonmade, L.J.; Brug, J.; Beulens, J.W.J. Built environmental characteristics and diabetes: A systematic review and meta-analysis. BMC Med. 2018, 16, 26. [Google Scholar] [CrossRef]
- McCormack, G.R.; Cabaj, J.; Orpana, H.; Lukic, R.; Blackstaffe, A.; Goopy, S.; Hagel, B.; Keough, N.; Martinson, R.; Chapman, J.; et al. A scoping review on the relations between urban form and health: A focus on Canadian quantitative evidence. Health Promot. Chronic Dis. Prev. Can. 2019, 39, 187–200. [Google Scholar] [CrossRef]
- WHO. Measuring the Age-Friendliness of Cities: A Guide to Using Core Indicators; WHO Centre for Health Development: Kobe, Japan, 2015. [Google Scholar]
- Cerin, E.; Nathan, A.; van Cauwenberg, J.; Barnett, D.W.; Barnett, A. The neighbourhood physical environment and active travel in older adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 15. [Google Scholar] [CrossRef]
- Wang, Y.; Chau, C.K.; Ng, W.Y.; Leung, T.M. A review on the effects of physical built environment attributes on enhancing walking and cycling activity levels within residential neighborhoods. Cities 2016, 50, 1–15. [Google Scholar] [CrossRef]
- Barnett, D.W.; Barnett, A.; Nathan, A.; Van Cauwenberg, J.; Cerin, E. Built environmental correlates of older adults’ total physical activity and walking: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Cervero, R.A.K.K. Travel Demand and the 3Ds: Density, Diversity, and Design. Transp. Res. Part D Transp. Environ. 1997, 2, 199–219. [Google Scholar] [CrossRef]
- Hajna, S.; Ross, N.A.; Brazeau, A.S.; Belisle, P.; Joseph, L.; Dasgupta, K. Associations between neighbourhood walkability and daily steps in adults: A systematic review and meta-analysis. BMC Public Health 2015, 15, 768. [Google Scholar] [CrossRef]
- Creatore, M.I.; Glazier, R.H.; Moineddin, R.; Fazli, G.S.; Johns, A.; Gozdyra, P.; Matheson, F.I.; Kaufman-Shriqui, V.; Rosella, L.C.; Manuel, D.G.; et al. Association of Neighborhood Walkability with Change in Overweight, Obesity, and Diabetes. JAMA 2016, 315, 2211–2220. [Google Scholar] [CrossRef]
- Koohsari, M.J.; McCormack, G.R.; Nakaya, T.; Shibata, A.; Ishii, K.; Yasunaga, A.; Hanibuchi, T.; Oka, K. Urban design and Japanese older adults’ depressive symptoms. Cities 2019, 87, 166–173. [Google Scholar] [CrossRef]
- Kondo, K. Progress in Aging Epidemiology in Japan: The JAGES Project. J. Epidemiol. 2016, 26, 331–336. [Google Scholar] [CrossRef]
- Adams, M.A.; Ryan, S.; Kerr, J.; Sallis, J.F.; Patrick, K.; Frank, L.D.; Norman, G.J. Validation of the Neighborhood Environment Walkability Scale (NEWS) items using geographic information systems. J. Phys. Act. Health 2009, 6, S113–S123. [Google Scholar] [CrossRef]
- Frank, L.D.; Sallis, J.F.; Saelens, B.E.; Leary, L.; Cain, K.; Conway, T.L.; Hess, P.M. The development of a walkability index: Application to the Neighborhood Quality of Life Study. Br. J. Sports Med. 2010, 44, 924–933. [Google Scholar] [CrossRef]
- Stark, J.H.; Neckerman, K.; Lovasi, G.S.; Quinn, J.; Weiss, C.C.; Bader, M.D.; Konty, K.; Harris, T.G.; Rundle, A. The impact of neighborhood park access and quality on body mass index among adults in New York City. Prev. Med. 2014, 64, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Tani, Y.; Suzuki, N.; Fujiwara, T.; Hanazato, M.; Kondo, N.; Miyaguni, Y.; Kondo, K. Neighborhood food environment and mortality among older Japanese adults: Results from the JAGES cohort study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 101. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Takamoto, I.; Amemiya, A.; Hanazato, M.; Suzuki, N.; Nagamine, Y.; Sasaki, Y.; Tani, Y.; Yazawa, A.; Inoue, Y.; et al. Is a hilly neighborhood environment associated with diabetes mellitus among older people? Results from the JAGES 2010 study. Soc. Sci. Med. 2017, 182, 45–51. [Google Scholar] [CrossRef]
- Hanibuchi, T.; Nakaya, T.; Yonejima, M.; Honjo, K. Perceived and Objective Measures of Neighborhood Walkability and Physical Activity among Adults in Japan: A Multilevel Analysis of a Nationally Representative Sample. Int. J. Environ. Res. Public Health 2015, 12, 13350–13364. [Google Scholar] [CrossRef] [PubMed]
- Glazier, R.H.; Creatore, M.I.; Weyman, J.T.; Fazli, G.; Matheson, F.I.; Gozdyra, P.; Moineddin, R.; Kaufman-Shriqui, V.; Booth, G.L. Density, destinations or both? A comparison of measures of walkability in relation to transportation behaviors, obesity and diabetes in Toronto, Canada. PLoS ONE 2014, 9, e85295. [Google Scholar] [CrossRef]
- Ministry of Land, Infrastructure, Transport and Tourism. National Land Numerical Information Land Utilization Tertiary Mesh Data; Ministry of Land, Infrastructure, Transport and Tourism: Tokyo, Japan, 2016.
- Lakke, S.E.; Soer, R.; Takken, T.; Reneman, M.F. Risk and prognostic factors for non-specific musculoskeletal pain: A synthesis of evidence from systematic reviews classified into ICF dimensions. Pain 2009, 147, 153–164. [Google Scholar] [CrossRef]
- Ikeda, T.; Sugiyama, K.; Aida, J.; Tsuboya, T.; Watabiki, N.; Kondo, K.; Osaka, K. Socioeconomic inequalities in low back pain among older people: The JAGES cross-sectional study. Int. J. Equity Health 2019, 18, 15. [Google Scholar] [CrossRef]
- Muraki, S.; Akune, T.; Oka, H.; Mabuchi, A.; En-Yo, Y.; Yoshida, M.; Saika, A.; Nakamura, K.; Kawaguchi, H.; Yoshimura, N. Association of occupational activity with radiographic knee osteoarthritis and lumbar spondylosis in elderly patients of population-based cohorts: A large-scale population-based study. Arthritis Rheum. 2009, 61, 779–786. [Google Scholar] [CrossRef]
- Rautio, N.; Filatova, S.; Lehtiniemi, H.; Miettunen, J. Living environment and its relationship to depressive mood: A systematic review. Int. J. Soc. Psychiatry 2018, 64, 92–103. [Google Scholar] [CrossRef]
- Eriksson, U.; Arvidsson, D.; Gebel, K.; Ohlsson, H.; Sundquist, K. Walkability parameters, active transportation and objective physical activity: Moderating and mediating effects of motor vehicle ownership in a cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 123. [Google Scholar] [CrossRef]
- Hanibuchi, T.; Kawachi, I.; Nakaya, T.; Hirai, H.; Kondo, K. Neighborhood built environment and physical activity of Japanese older adults: Results from the Aichi Gerontological Evaluation Study (AGES). BMC Public Health 2011, 11, 657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuji, T.; Miyaguni, Y.; Kanamori, S.; Hanazato, M.; Kondo, K. Community-level Sports Group Participation and Older Individuals’ Depressive Symptoms. Med. Sci. Sports Exerc. 2018, 50, 1199–1205. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, A.S.; Hayakawa, H.; Morimoto, T.; Kakuma, T. Screening for late life depression: Cut-off scores for the Geriatric Depression Scale and the Cornell Scale for Depression in Dementia among Japanese subjects. Int. J. Geriatr. Psychiatry 2003, 18, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, I.; Kondo, K.; Kondo, N.; Aida, J.; Ichikawa, H.; Kusumi, T.; Sueishi, N.; Imanaka, Y. Are pension types associated with happiness in Japanese older people?: JAGES cross-sectional study. PLoS ONE 2018, 13, e0197423. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Ishine, M.; Sakagami, T.; Okumiya, K.; Fujisawa, M.; Murakami, S.; Otsuka, K.; Yano, S.; Kita, T.; Matsubayashi, K. Depression in Japanese community-dwelling elderly--prevalence and association with ADL and QOL. Arch. Gerontol. Geriatr. 2004, 39, 15–23. [Google Scholar] [CrossRef]
- Yoshimura, N.; Akune, T.; Fujiwara, S.; Shimizu, Y.; Yoshida, H.; Nishiwaki, Y.; Sudo, A.; Omori, G.; Yoshida, M.; Shimokata, H.; et al. Incidence of disability and its associated factors in Japanese men and women: The Longitudinal Cohorts of Motor System Organ (LOCOMO) study. J. Bone Miner. Metab. 2015, 33, 186–191. [Google Scholar] [CrossRef]
- Zhang, T.T.; Liu, Z.; Liu, Y.L.; Zhao, J.J.; Liu, D.W.; Tian, Q.B. Obesity as a Risk Factor for Low Back Pain: A Meta-Analysis. Clin. Spine Surg. 2018, 31, 22–27. [Google Scholar] [CrossRef]
- Yoshimura, N.; Akune, T.; Fujiwara, S.; Shimizu, Y.; Yoshida, H.; Omori, G.; Sudo, A.; Nishiwaki, Y.; Yoshida, M.; Shimokata, H.; et al. Prevalence of knee pain, lumbar pain and its coexistence in Japanese men and women: The Longitudinal Cohorts of Motor System Organ (LOCOMO) study. J. Bone Miner. Metab. 2014, 32, 524–532. [Google Scholar] [CrossRef]
- Althoff, T.; Sosic, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017, 547, 336–339. [Google Scholar] [CrossRef]
- Newton, S.; Braithwaite, D.; Akinyemiju, T.F. Socio-economic status over the life course and obesity: Systematic review and meta-analysis. PLoS ONE 2017, 12, 15. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.T.; Prina, A.M.; Brayne, C. The association between community environment and cognitive function: A systematic review. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 351–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levasseur, M.; Cohen, A.A.; Dubois, M.F.; Genereux, M.; Richard, L.; Therrien, F.H.; Payette, H. Environmental Factors Associated With Social Participation of Older Adults Living in Metropolitan, Urban, and Rural Areas: The NuAge Study. Am. J. Public Health 2015, 105, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Yoshitaka, O.; Mamoru, N.; Yutaka, I. Relationship between diversity of activities in urban parks and interaction in the local community. J. Jpn. Soc. Reveg. Technol. 2018, 44, 111. [Google Scholar] [CrossRef]
- Pereira, G.; Christian, H.; Foster, S.; Boruff, B.J.; Bull, F.; Knuiman, M.; Giles-Corti, B. The association between neighborhood greenness and weight status: An observational study in Perth Western Australia. Environ. Health 2013, 12, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, C.; Gallacher, J.; Webster, C. Built environment configuration and change in body mass index: The Caerphilly Prospective Study (CaPS). Health Place 2013, 19, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.I.; Bath, B.; Boden, C.; Adebayo, O.; Trask, C. The association between awkward working posture and low back disorders in farmers: A systematic review. J. Agromed. 2019, 24, 74–89. [Google Scholar] [CrossRef]
- Cohen, D.; Huynh, T.; Sebold, A.; Harvey, J.; Neudorf, C.; Brown, A. The population health approach: A qualitative study of conceptual and operational definitions for leaders in Canadian healthcare. SAGE Open Med. 2014, 2, 2050312114522618. [Google Scholar] [CrossRef] [Green Version]
- Bonita, R.; Beaglehole, R.; Kjellström, T. Basic Epidemiology; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Cerin, E.; Saelens, B.E.; Sallis, J.F.; Frank, L.D. Neighborhood Environment Walkability Scale: Validity and development of a short form. Med. Sci. Sports Exerc. 2006, 38, 1682–1691. [Google Scholar] [CrossRef] [Green Version]
- Cain, K.L.; Geremia, C.M.; Conway, T.L.; Frank, L.D.; Chapman, J.E.; Fox, E.H.; Timperio, A.; Veitch, J.; Van Dyck, D.; Verhoeven, H.; et al. Development and reliability of a streetscape observation instrument for international use: MAPS-global. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 19. [Google Scholar] [CrossRef]
- Zadro, J.R.; Shirley, D.; Pinheiro, M.B.; Bauman, A.; Duncan, G.E.; Ferreira, P.H. Neighborhood walkability moderates the association between low back pain and physical activity: A co-twin control study. Prev. Med. 2017, 99, 257–263. [Google Scholar] [CrossRef]
- Duncan, R.; Peat, G.; Thomas, E.; Hay, E.; McCall, I.; Croft, P. Symptoms and radiographic osteoarthritis: Not as discordant as they are made out to be? Ann. Rheum. Dis. 2007, 66, 86–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 77. [Google Scholar] [CrossRef] [Green Version]

| Characteristics | n | % | |
|---|---|---|---|
| Sex | |||
| Male | 11,114 | 46.5 | |
| Female | 12,775 | 53.5 | |
| Age, years | |||
| 65–69 | 6690 | 28 | |
| 70–74 | 7231 | 30.3 | |
| 75–79 | 5330 | 22.3 | |
| 80–84 | 3147 | 13.2 | |
| 85+ | 1491 | 6.2 | |
| Educational background, years | |||
| 13+ | 4713 | 19.7 | |
| 10–12 | 8819 | 36.9 | |
| <10 | 9974 | 41.8 | |
| Missing | 383 | 1.6 | |
| Equivalent annual income, yen | |||
| 4.0+ million | 2025 | 8.5 | |
| 2.0–3.9 million | 7140 | 29.9 | |
| <2.0 million | 9875 | 41.3 | |
| Missing | 4849 | 20.3 | |
| Past occupation | |||
| White-collar worker | 8481 | 37.1 | |
| Blue-collar worker | 9494 | 41.5 | |
| Primary industry worker | 1291 | 5.6 | |
| Never worked | 1170 | 5.1 | |
| Missing | 2456 | 10.7 | |
| Walking time, min | |||
| 60+ | 9241 | 38.7 | |
| 30–59 | 8401 | 35.2 | |
| <30 | 5704 | 23.9 | |
| Missing | 543 | 2.3 | |
| Physical activity | |||
| Daily | 6858 | 28.7 | |
| Weekly | 6517 | 27.3 | |
| Annually | 3379 | 14.1 | |
| None | 4999 | 20.9 | |
| Missing | 2136 | 8.9 | |
| Driving status | |||
| No | 10,854 | 45.6 | |
| Yes | 12,967 | 54.4 | |
| Body mass index, kg/m2 | |||
| 18.5–24.9 | 16,006 | 67 | |
| <18.5 | 1665 | 7 | |
| 25+ | 6153 | 25.8 | |
| Missing | 65 | 0.3 | |
| Depression | |||
| None (GDS < 5) | 14,223 | 62.1 | |
| Mild (GDS of 5–9) | 3603 | 15.7 | |
| Severe (GDS ≥ 10) | 1143 | 5 | |
| Missing | 3923 | 17.1 | |
| Knee pain | |||
| Yes | 6314 | 26.2 | |
| Missing | 646 | 2.8 | |
| Low back pain | |||
| Yes | 7050 | 29.3 | |
| Missing | 657 | 2.9 | |
| Mean | SD | Median | Minimum | Maximum | R | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | ||||||
| (i) Access to parks and sidewalks (score) | 2.94 | 0.29 | 2.96 | 1.94 | 3.81 | 1 | |||||
| (ii) Access to fresh food stores (score) | 2.97 | 0.39 | 3.05 | 1.65 | 3.85 | 0.52 * | 1 | ||||
| (iii) Easy walking without slopes or stairs (score) | 2.56 | 0.38 | 2.61 | 1.44 | 3.29 | −0.17 * | 0.08 * | 1 | |||
| (iv) Population density (persons/km2) | 6543 | 4727 | 6719 | 22 | 31,565 | 0.44 * | 0.59 * | 0.24 * | 1 | ||
| (v) Knee pain (%) | 29 | 6.8 | 27.7 | 15.6 | 51.4 | −0.21 * | −0.14 | 0.02 | −0.33 * | 1 | |
| (vi) Low back pain (%) | 32.9 | 6.9 | 32 | 13.6 | 51.4 | −0.14 | −0.14 | −0.03 | −0.17 * | 0.63 * | 1 |
| Crude Model | Model 1 a | Model 2 b | Model 3 c | |
|---|---|---|---|---|
| PR (95% CI) | PR (95% CI) | PR (95% CI) | PR (95% CI) | |
| Access to parks and sidewalks | 0.69 (0.63–0.76) * | 0.84 (0.76–0.93) * | 0.85 (0.77–0.94) * | 0.92 (0.81–1.03) |
| Access to fresh food stores | 0.81 (0.76–0.87) * | 0.90 (0.84–0.96) * | 0.90 (0.84–0.96) * | 0.95 (0.87–1.03) |
| Easy walking without slopes or stairs | 1.02 (0.94–1.10) | 0.96 (0.89–1.04) | 0.95 (0.88–1.02) | 0.91 (0.85–0.99) * |
| Population density | 0.91 (0.89–0.93) * | 0.96 (0.94–0.98) * | 0.95 (0.93–0.98) * | - |
| Crude Model | Model 1 a | Model 2 b | Model 3 c | |
|---|---|---|---|---|
| PR (95% CI) | PR (95% CI) | PR (95% CI) | PR (95% CI) | |
| Access to parks and sidewalks | 0.81 (0.74–0.89) * | 0.94 (0.85–1.03) | 0.96 (0.88–1.06) | 1.08 (0.97–1.20) |
| Access to fresh food stores | 0.85 (0.80–0.90) * | 0.92 (0.86–0.98) * | 0.92 (0.86–0.98) * | 0.98 (0.91–1.06) |
| Easy walking without slopes or stairs | 1.02 (0.95–1.09) | 0.98 (0.91–1.05) | 0.96 (0.89–1.03) | 0.93 (0.87–1.00) |
| Population density | 0.92 (0.91–0.94) * | 0.96 (0.94–0.98) * | 0.96 (0.94–0.98) * | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okabe, D.; Tsuji, T.; Hanazato, M.; Miyaguni, Y.; Asada, N.; Kondo, K. Neighborhood Walkability in Relation to Knee and Low Back Pain in Older People: A Multilevel Cross-Sectional Study from the JAGES. Int. J. Environ. Res. Public Health 2019, 16, 4598. https://doi.org/10.3390/ijerph16234598
Okabe D, Tsuji T, Hanazato M, Miyaguni Y, Asada N, Kondo K. Neighborhood Walkability in Relation to Knee and Low Back Pain in Older People: A Multilevel Cross-Sectional Study from the JAGES. International Journal of Environmental Research and Public Health. 2019; 16(23):4598. https://doi.org/10.3390/ijerph16234598
Chicago/Turabian StyleOkabe, Daichi, Taishi Tsuji, Masamichi Hanazato, Yasuhiro Miyaguni, Nao Asada, and Katsunori Kondo. 2019. "Neighborhood Walkability in Relation to Knee and Low Back Pain in Older People: A Multilevel Cross-Sectional Study from the JAGES" International Journal of Environmental Research and Public Health 16, no. 23: 4598. https://doi.org/10.3390/ijerph16234598
APA StyleOkabe, D., Tsuji, T., Hanazato, M., Miyaguni, Y., Asada, N., & Kondo, K. (2019). Neighborhood Walkability in Relation to Knee and Low Back Pain in Older People: A Multilevel Cross-Sectional Study from the JAGES. International Journal of Environmental Research and Public Health, 16(23), 4598. https://doi.org/10.3390/ijerph16234598