The Impact of Opium Abuse on Lipid Profile in Patients with Diabetes: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
1.1. Why is the Review Important?
1.2. Aim
2. Method
2.1. Types of Studies
2.2. Types of Participants
2.3. Types of Interventions
2.4. Outcome Measures
2.5. Data Sources and Search Strategy
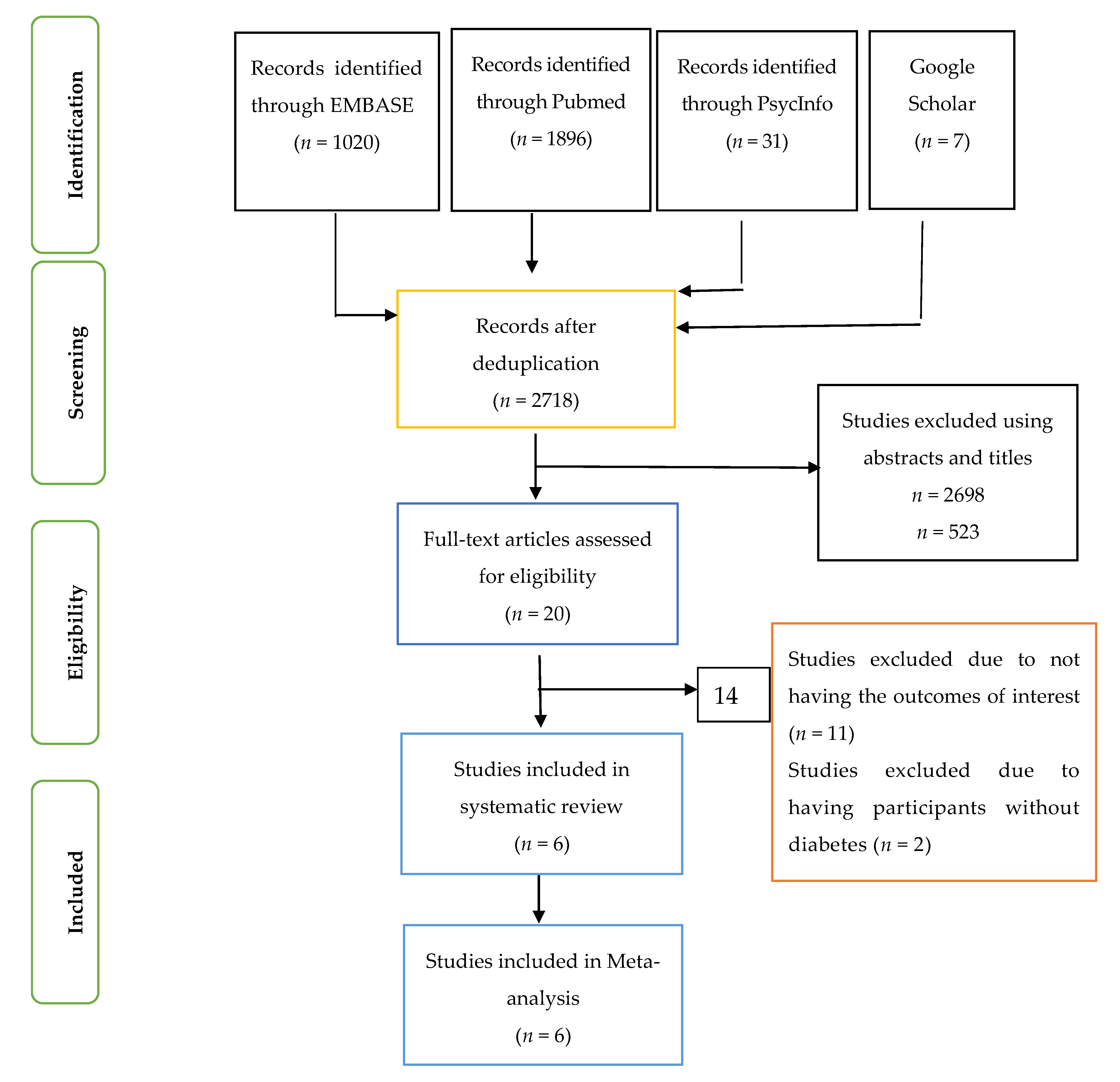
2.6. Study Selection
2.7. Inclusion and Exclusion Criteria
2.8. Rationale for the Studies Selected
2.9. Data Extraction
2.10. Quality Evaluation
2.11. Statistical Analysis
2.12. Data Inclusion Decisions
3. Results
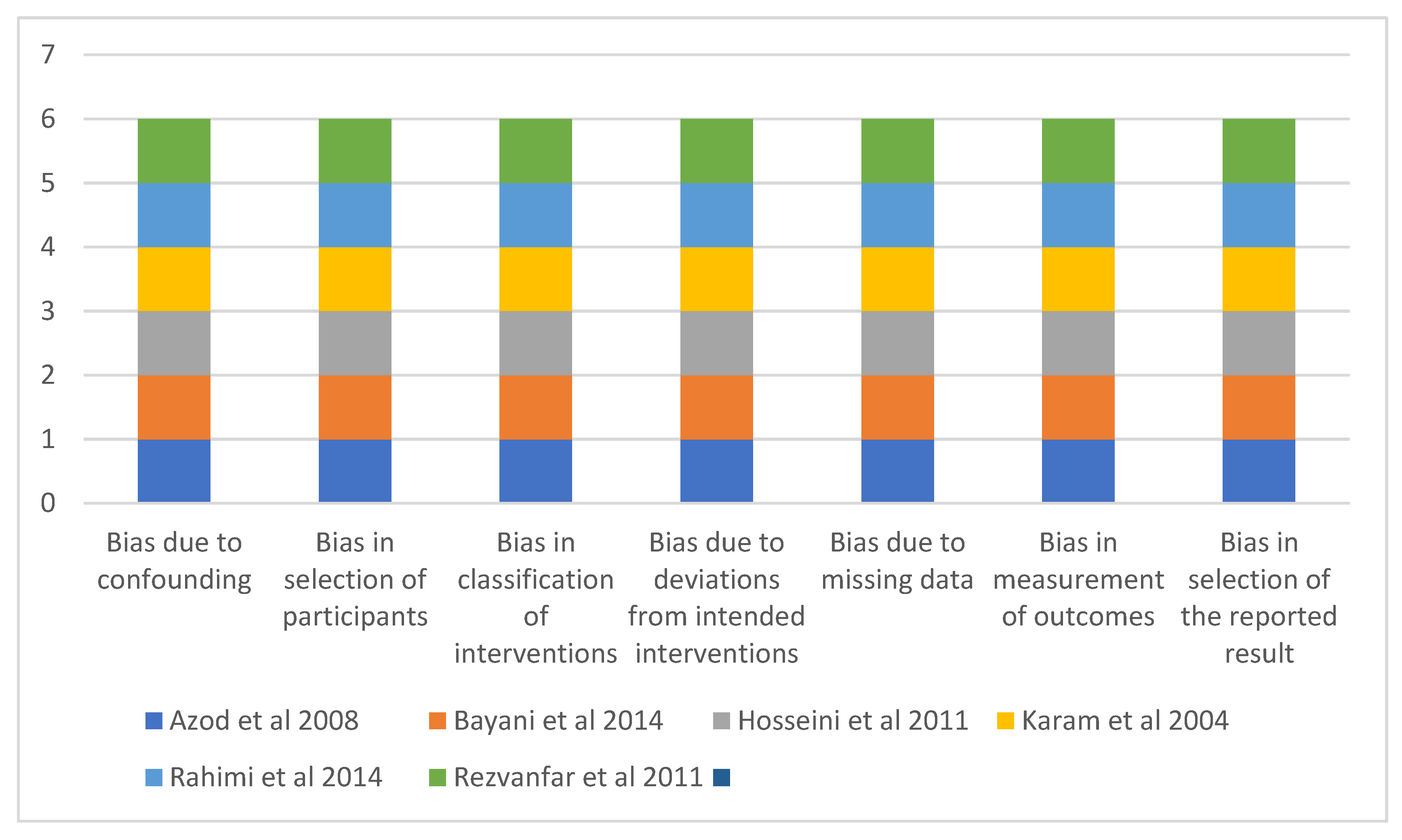
3.1. Assessment of Risk of Bias of Included Studies
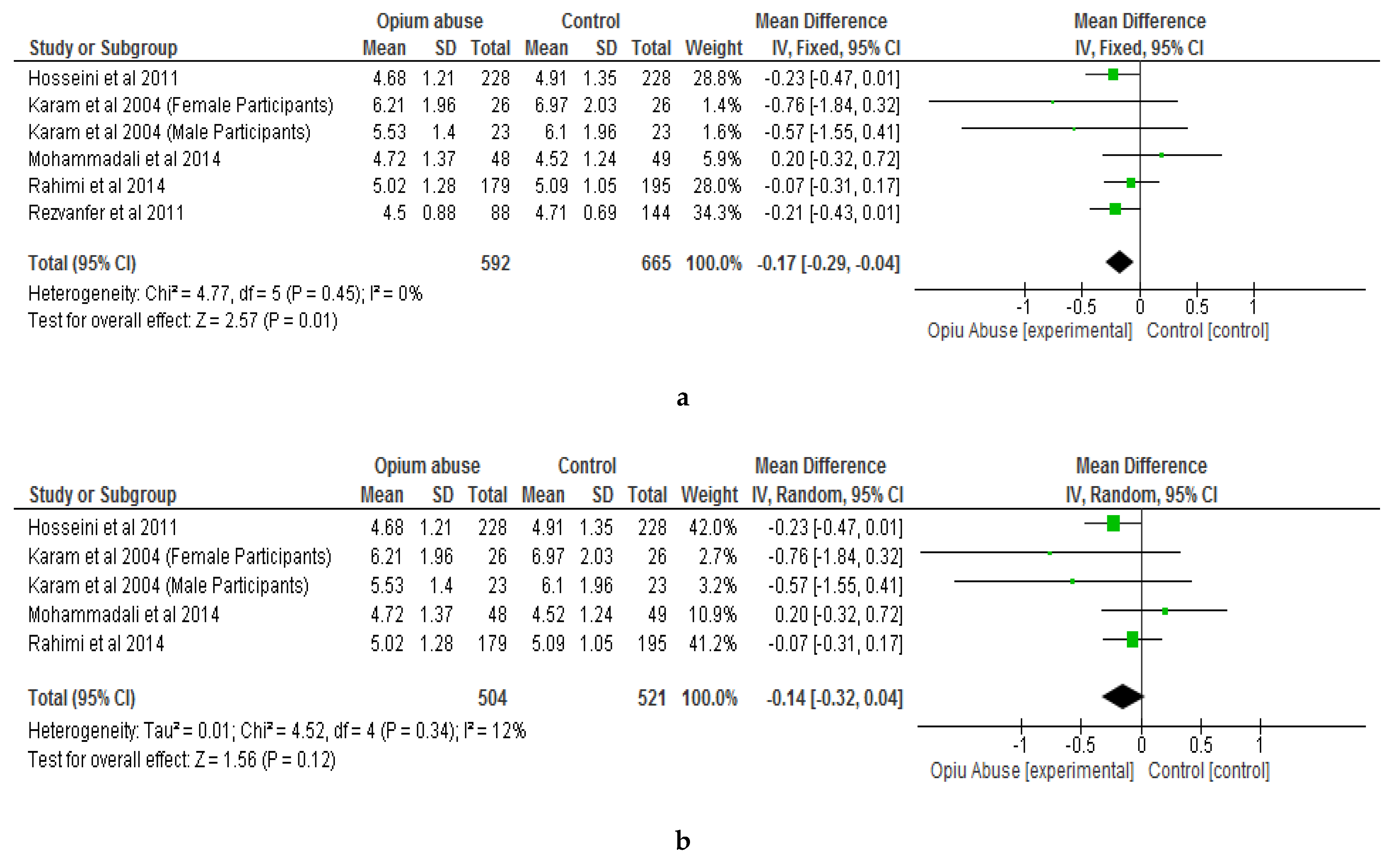
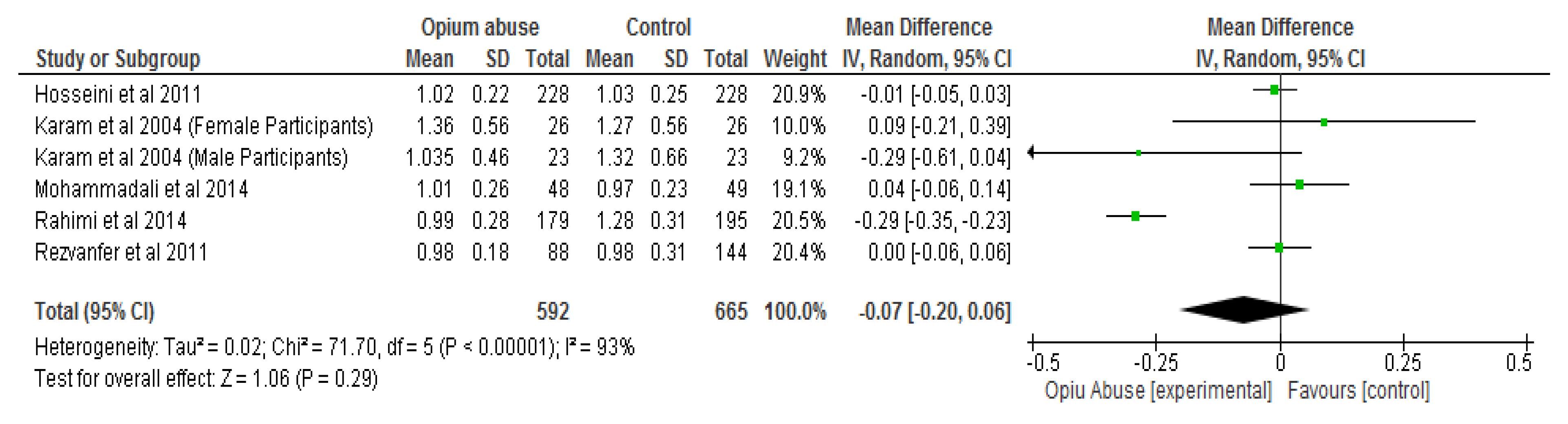
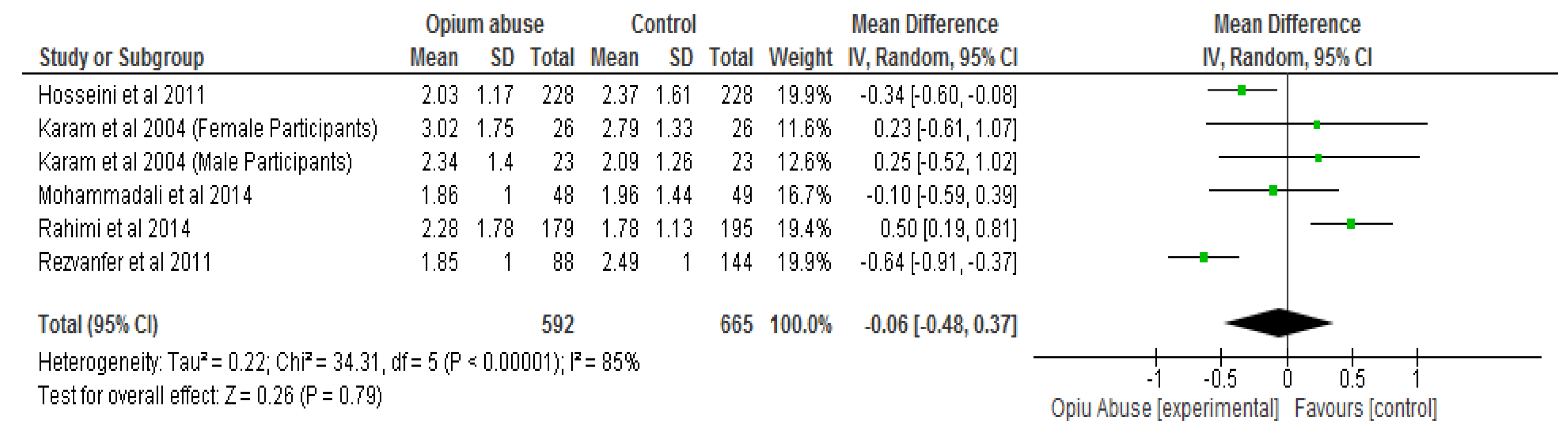
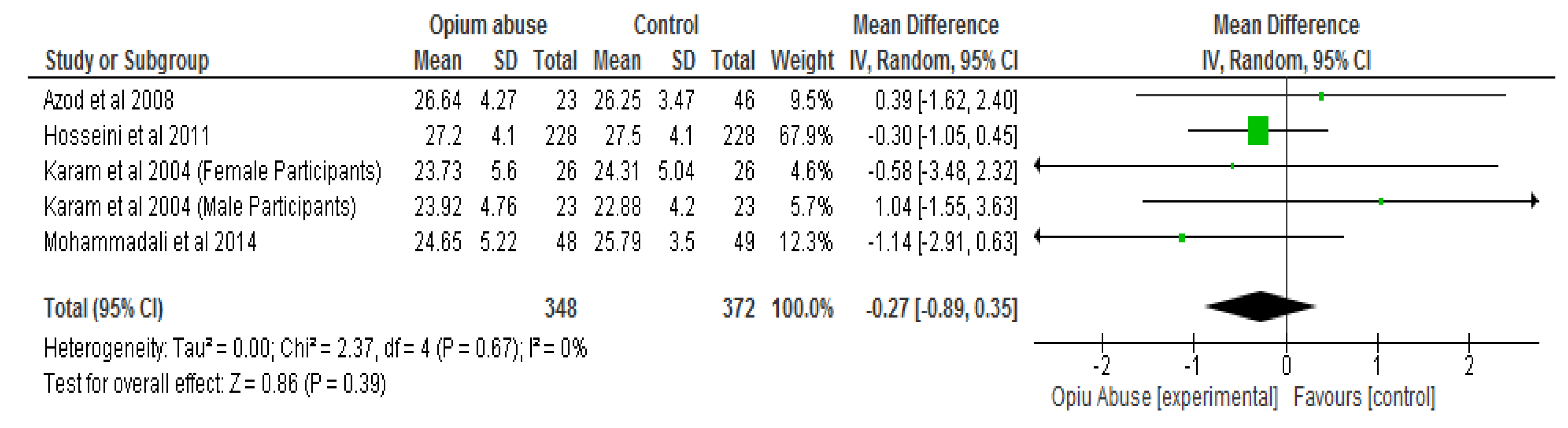
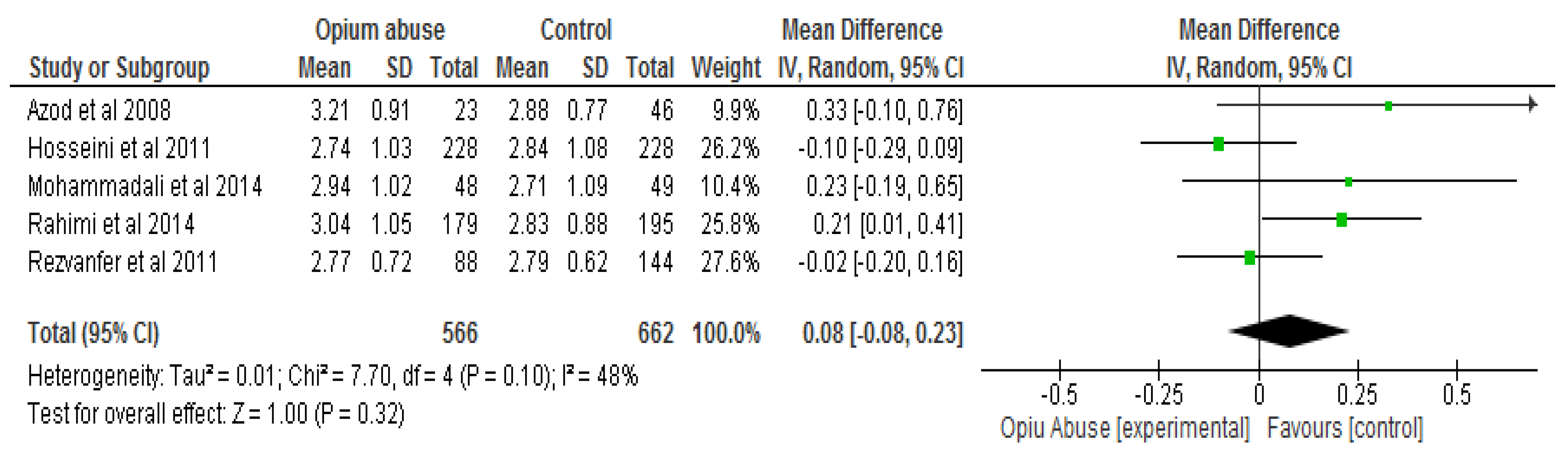
3.2. Meta-Analysis of Data
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organisation (WHO). Diabetes. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 29 March 2019).
- Gautam, S.; Franzini, L.; Mikhail, O.I.; Chan, W.; Turner, B.J. Novel measure of opioid dose and costs of care for diabetes mellitus: Opioid dose and health care costs. J. Pain 2016, 17, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Walter, K.N.; Petry, N.M. Patients with diabetes respond well to contingency management treatment targeting alcohol and substance use. Psychol. Health Med. 2015, 20, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Gautam, S.; Franzini, L.; Mikhail, O.I.; Wenyaw, C.; Turner, B.J. Longitudinal analysis of opioid analgesic dose and diabetes quality of care measures. Pain Med. 2015, 16, 2134–2141. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Aguayo, A.; Araneda, J.C.; Fernandez, D.; Gleisner, A.; Perez, V.; Codner, E. Tobacco, alcohol, and illicit drug use in adolescents with diabetes mellitus. Pediatric Diabetes 2007, 8, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Shiri, R.; Hassani, K.F.; Ansari, M. Association between opium abuse and comorbidity in diabetic men. Am. J. Addict. 2006, 15, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.W.; Samet, J.H.; Cheng, D.M.; Bernstein, J.; Wang, N.; German, J.; Saitz, R. The spectrum of unhealthy drug use and quality of care for hypertension and diabetes: A longitudinal cohort study. BMJ Open 2015, 5, e008508. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). Noncommunicable Diseases. 2018. Available online: https://www.who.int/en/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 29 March 2019).
- World Health Organisation (WHO). The Top Ten Causes of Death. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 29 March 2019).
- Wu, L.; Ghitza, U.E.; Zhu, H.; Spratt, S.; Swartz, M.; Mannelli, P. Substance use disorders and medical comorbidities among high-need, high-risk patients with diabetes. Drug Alcohol Depend. 2018, 186, 86–93. [Google Scholar] [CrossRef]
- Sharma, P.; Singh Balhara, Y.P. Opioid use and diabetes: An overview. J. Soc. Health Diabetes 2016, 4, 6–10. [Google Scholar] [CrossRef]
- Najafipour, H.; Beik, A. The impact of opium consumption on blood glucose, serum lipids and blood pressure, and related mechanisms. Front. Physiol. 2016, 7, 436. [Google Scholar] [CrossRef]
- Walter, K.N.; Wagner, J.A.; Cengiz, E.; Tamborlane, W.V.; Petry, N.M. Substance use disorders among patients with type 2 diabetes: A dangerous but understudied combination. Curr. Diabetes Rep. 2017, 17, 2. [Google Scholar] [CrossRef]
- Hamilton, I.; Lloyd, C.; Phillips, A. Substance use and diabetes: Practical solutions. Pract. Nurs. 2012, 23, 148–152. [Google Scholar] [CrossRef]
- Sheldon, B.; Quin, J. Diabetes and illicit drug use. Pract. Diabetes Int. 2005, 22, 222–224. [Google Scholar] [CrossRef]
- Ojo, O.; Wang, X.-H.; Ojo, O.O.; Ibe, J. The effects of substance abuse on blood glucose parameters in patients with diabetes: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2018, 15, 2691. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e100097. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579–596. [Google Scholar] [CrossRef]
- Saunders, S.A.; Democratis, J.; Martin, J.; Macfarlane, I.A. Intravenous drug abuse and Type 1 diabetes: Financial and healthcare implications. Diabet. Med. 2004, 21, 1269–1273. [Google Scholar] [CrossRef]
- Modzelewski, K.L.; Rybin, D.V.; Weinberg, J.M.; Alexanian, S.M.; McDonnell, M.E.; Steenkamp, D.W. Active cocaine use does not increase the likelihood of hyperglycemic crisis. J. Clin. Transl. Endocrinol. 2017, 9, 1–7. [Google Scholar] [CrossRef]
- Lee, P.; Greenfield, J.R.; Gilbert, K.; Campbell, L.V. Recreational drug use in type 1 diabetes: An invisible accomplice to poor glycaemic control? Intern. Med. J. 2012, 42, 198–202. [Google Scholar] [CrossRef]
- Saif-Ali, R.; Al-Qirbi, A.; Al-Geiry, A.; AL-Habori, M. Effect of Catha edulis on plasma glucose and C-peptide in both type 2 diabetics and non-diabetics. J. Ethnopharmacol. 2003, 86, 45–49. [Google Scholar] [CrossRef]
- Isidro, M.L.; Jorge, S. Recreational drug abuse in patients hospitalized for diabetic ketosis or diabetic ketoacidosis. Acta Diabetol. 2013, 50, 183–187. [Google Scholar] [CrossRef]
- Warner, E.A.; Greene, G.S.; Buchsbaum, M.S.; Cooper, D.S.; Robinson, B.E. Diabetic ketoacidosis associated with cocaine use. Arch. Int. Med. 1998, 158, 1799–1802. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ (Clin. Res. Ed.) 2016, 355, i4919. [Google Scholar] [CrossRef]
- The Nordic Cochrane Centre. Review Manager (RevMan) [Computer Program]; Version 5.3.; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2009. [Google Scholar]
- Mohammadali, B.; Sepideh, N.; Mohammadreza Khosoosi, N.; Mirsaeid, R.; Afshin, K. Opium consumption and lipid and glucose parameters in diabetic patients with acute coronary syndrome: A survey in northern Iran. La Tunisie Médicale 2014, 92, 497–500. [Google Scholar]
- Rahimi, N.; Gozashti, M.H.; Najafipour, H.; Shokoohi, M.; Marefati, H. Potential effect of opium consumption on controlling diabetes and some cardiovascular risk factors in diabetic patients. Addict. Health 2014, 6, 1. [Google Scholar]
- Azod, L.; Rashidi, M.; Afkhami-Ardekani, M.; Kiani, G.; Khoshkam, F. Effect of opium addiction on diabetes. Am. J. Drug Alcohol Abus. 2008, 34, 383–388. [Google Scholar] [CrossRef]
- Hosseini, S.K.; Masoudkabir, F.; Vasheghani-Farahani, A.; Alipour-Parsa, S.; Sheikh Fathollahi, M.; Rahimi-Foroushani, A.; Hakki, E.; Goodarzynejad, H.; Eftekhar, H. Opium consumption and coronary atherosclerosis in diabetic patients: A propensity score-matched study. Planta Med. 2011, 77, 1870–1875. [Google Scholar] [CrossRef]
- Karam, G.A.; Reisi, M.; Kaseb, A.A.; Khaksari, M.; Mohammadi, A.; Mahmoodi, M. Effects of opium addiction on some serum factors in addicts with non-insulin-dependent diabetes mellitus. Addict. Biol. 2004, 9, 53–58. [Google Scholar] [CrossRef]
- Rezvanfar, M.R.; Farahany, H.; Rafiee, M.; Kaboli, S. Opium consumption challenge and diabetes mellitus control. Iran. J. Diabetes Obes. 2011, 3, 72–76. [Google Scholar]
- Asgary, S.; Sarrafzadegan, N.; Naderi, G.-A.; Rozbehani, R. Effect of opium addiction on new and traditional cardiovascular riskfactors: Do duration of addiction and route of administration matter? Lipids Health Dis. 2008, 7, 42–46. [Google Scholar] [CrossRef]
- Kouros, D.; Tahereh, H.; Mohammadreza, A.; Minoo, M.Z. Opium and heroin alter biochemical parameters of human’s serum. Am. J. Drug Alcohol Abus. 2010, 36, 135–139. [Google Scholar] [CrossRef]
- Martini, F.H.; Nath, J.L.; Bartholomew, E.F. Fundamentals of Anatomy and Physiology, 9th ed.; Pearson: London, UK, 2011. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient/Population | Intervention | Comparator | Outcomes of Interest | Combining Search Terms |
|---|---|---|---|---|
| Patients with diabetes | Substance Abuse | Lipid Profile and Body Mass Index | ||
| Type 2 diabetes OR type 1 diabetes OR diabetes complications OR diabetes mellitus, type 2 OR diabetes mellitus, type 1 OR diabetes mellitus | Substance-related disorders OR substance* OR marijuana abuse OR amphetamine-related disorders OR cocaine-related disorders OR opioid-related disorders OR opiate* OR opioid* OR heroin dependence | Body mass index OR BMI OR Total cholesterol OR High-density lipoprotein cholesterol OR HDL OR Low-density lipoprotein cholesterol OR LDL OR Triglycerides | Column 1 AND Column 2 AND Column 3 |
| Study Reference | Country | Length of Study | Study Type/Design | Sample Size/Description | Age | Gender | Diabetes Type/Duration of Diabetes (YRS- Mean ± SD) | Type of Substance Abused |
|---|---|---|---|---|---|---|---|---|
| Azod et al. [30] | Iran | Not stated | Cross-sectional study | 23 opium 46 non-opium The two groups were matched in age, BMI, duration of diabetes, cigarette smoking, medication, and education | Mean 60.52 ± 12.25 55.24 ± 10.92 years | All males | Type 2 DM Duration of diabetes recorded during the study, but not reported by authors. | Opium |
| Hosseini et al. [31] | Iran | 2008–2010 | Cross-sectional study | 228 opium 228 non-opium The two groups were matched in age, BMI, sex and smoking status | Mean 58.9 (SD = 9.2 years | 92% male | 91% were type 2 DM Opium: 7.6 ± 7.1 non Opium: 8.2 ± 8.4 | Opium |
| Karam et al. [32] | Iran | Not stated | Case-control study | 23 male and 26 female opium 23 male and 26 female non-opium The two groups were matched in age, BMI, cigarette smoking and medication | 35–65 years | 53% female | Type 2 DM Duration of diabetes was not reported | Opium |
| Mohammadali et al. [28] | Iran | 2006–2007 | Cross-sectional study | 48 opium users 49 non-opium users The two groups were matched in age, BMI, duration of diabetes and medication history | Mean 64 years | >60% female | Type 2 DM Opium: 11.31 ± 6.33 non Opium: 10.39 ± 7.91 | Opium |
| Rahimi et al. [29] | Iran | Not stated | Cross-sectional study | 179 opium users 195 non-opium users The two groups were not matched in age, BMI and cigarette smoking | Mean 53.5–58.2 years | Combined males and females | Type 2 DM Duration of diabetes was not reported | Opium |
| Rezvanfar et al. [33] | Iran | 2009–2010 | Case-control study | 88 opium users 144 non-opium users The two groups were matched in age, BMI, duration of diabetes | Mean 55–57 years | All males | Type 2 DM Opium: 9.8 ± 6.4 non Opium: 7.8 ± 5.4 | Opium |
| Study reference | Participants Studied | Body Mass Index (BMI) (kg/m2) | Total Cholesterol | High Density Lipoprotein (HDL) | Low Density Lipoprotein (LDL) | Triglycerides |
|---|---|---|---|---|---|---|
| Azod et al. [30] | Substance abusers Mean ± SD | 26.64 ± 4.27 | No data | 34.98 mg/dL | 123.96 ± 34.96 mg/dL | 31.50 mg/dL |
| Non-substance abusers | 26.25 ± 3.47 P = 0.68 | No data | 35.01 mg/dL P = 0.99 | 111.24 ± 29.57 mg/dL P = 0.11 | 36.75 mg/dL P = 0.30 | |
| Hosseini et al. [31] | Substance abusers Mean ± SD | 27.2 ± 4.1 | 180.96 ± 46.85 mg/dL | 39.67 ± 8.80 mg/dL | 105.82 ± 39.76 mg/dL | 179.68 ± 103.15 mg/dL |
| Non-substance abusers | 27.5 ± 4.1 P = 0.391 | 189.85 ± 52.14 mg/dL P = 0.061 | 40.08 ± 9.70 mg/dL P = 0.640 | 109.63 ± 41.76 mg/dL P = 0.343 | 209.59 ± 142.12 mg/dL P = 0.012 | |
| Karam et al. [32] (for men) | Substance abusers Mean ± SEM | 23.92 ± 0.68 | 5.53 ± 0.2 mmol/L | 1.035 ± 0.066 mmol/L | No data | 2.34 ± 0.2 mmol/L |
| Non-substance abusers | 22.88 ± 0.60 P = 0.2598 | 6.1 ± 0.28 mmol/L P = 0.098 | 1.32 ± 0.094 mmol/L P = 0.0376 | No data | 2.09 ± 0.18 mmol/L P = 0.3481 | |
| Karam et al. [32] (for women) | Substance abusers Mean ± SEM | 23.73 ± 0.80 | 6.21 ± 0.28 mmol/L | 1.36 ± 0.08 mmol/L | No data | 3.02 ± 0.25 mmol/L |
| Non-substance abusers | 24.31 ± 0.72 P = 0.2200 | 6.97 ± 0.29 mmol/L P = 0.0711 | 1.27 ± 0.08 mmol/L P = 0.3483 | No data | 2.79 ± 0.19 mmol/L P = 0.5349 | |
| Mohammadali et al. [28] | Substance abusers Mean ± SD | 24.65 ± 5.22 | 182.27 ± 53.23 mg/dL | 39 ± 10.4 mg/dL | 113.6 ± 39.25 mg/dL | 164.46 ± 84.65 mg/dL |
| Non-substance abusers | 25.79 ± 3.5 P = 0.153 | 174.88 ± 47.89 mg/dL P = 0.307 | 37.47 ± 9.24 mg/dL P = 0.477 | 104.86 ± 42.1 mg/dL P = 0.171 | 173.49 ± 127.61 mg/dL P = 0.751 | |
| Rahimi et al. [29] | Substance abusers Mean ± SD | 26.3 ± 5.6 | 194.1 ± 49.6 mg/dL | 38.6 ± 10.9 mg/dL | 117.6 ± 40.7 mg/dL | 201.5 ± 157.3 mg/dL |
| Non-substance abusers | 27.7 ± 4.4 P = 0.009 | 196.9 ± 40.6 mg/dL P = 0.550 | 49.8 ± 12.2 mg/dL P < 0.001 | 109.4 ± 34.2 mg/dL P = 0.052 | 200.1 ± 99.8 mg/dL P = 0.910 | |
| Rezvanfar et al. [33] | Substance abusers Mean ± SD | No data | 174 ± 34 mg/dL | 38 ± 7 mg/dL | 107 ± 28 mg/dL | 164 ± 88 mg/dL |
| Non-substance abusers | No data | 182 ± 27 mg/dL P = 0.18 | 38 ± 12 mg/dL P = 0.90 | 108 ± 24 mg/dL P = 0.92 | 220 ± 86 mg/dL P = 0.005 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Wang, X.-H.; Ojo, O.O.; Ibe, J. The Impact of Opium Abuse on Lipid Profile in Patients with Diabetes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4795. https://doi.org/10.3390/ijerph16234795
Ojo O, Wang X-H, Ojo OO, Ibe J. The Impact of Opium Abuse on Lipid Profile in Patients with Diabetes: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(23):4795. https://doi.org/10.3390/ijerph16234795
Chicago/Turabian StyleOjo, Omorogieva, Xiao-Hua Wang, Osarhumwese Osaretin Ojo, and Jude Ibe. 2019. "The Impact of Opium Abuse on Lipid Profile in Patients with Diabetes: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 23: 4795. https://doi.org/10.3390/ijerph16234795
APA StyleOjo, O., Wang, X. -H., Ojo, O. O., & Ibe, J. (2019). The Impact of Opium Abuse on Lipid Profile in Patients with Diabetes: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 16(23), 4795. https://doi.org/10.3390/ijerph16234795