Level of Stigma among Spanish Nursing Students toward Mental Illness and Associated Factors: A Mixed-Methods Study

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Selection of Study Subjects
2.2. Methodology of the Quantitative Phase
2.2.1. Study Design and Scope
2.2.2. Information Sources
2.2.3. Calculation of the Sample Size
2.2.4. Statistical Analysis Used
2.2.5. Ethical Approval
2.3. Methodology of the Qualitative Phase
3. Results
3.1. Results of the Quantitative Phase
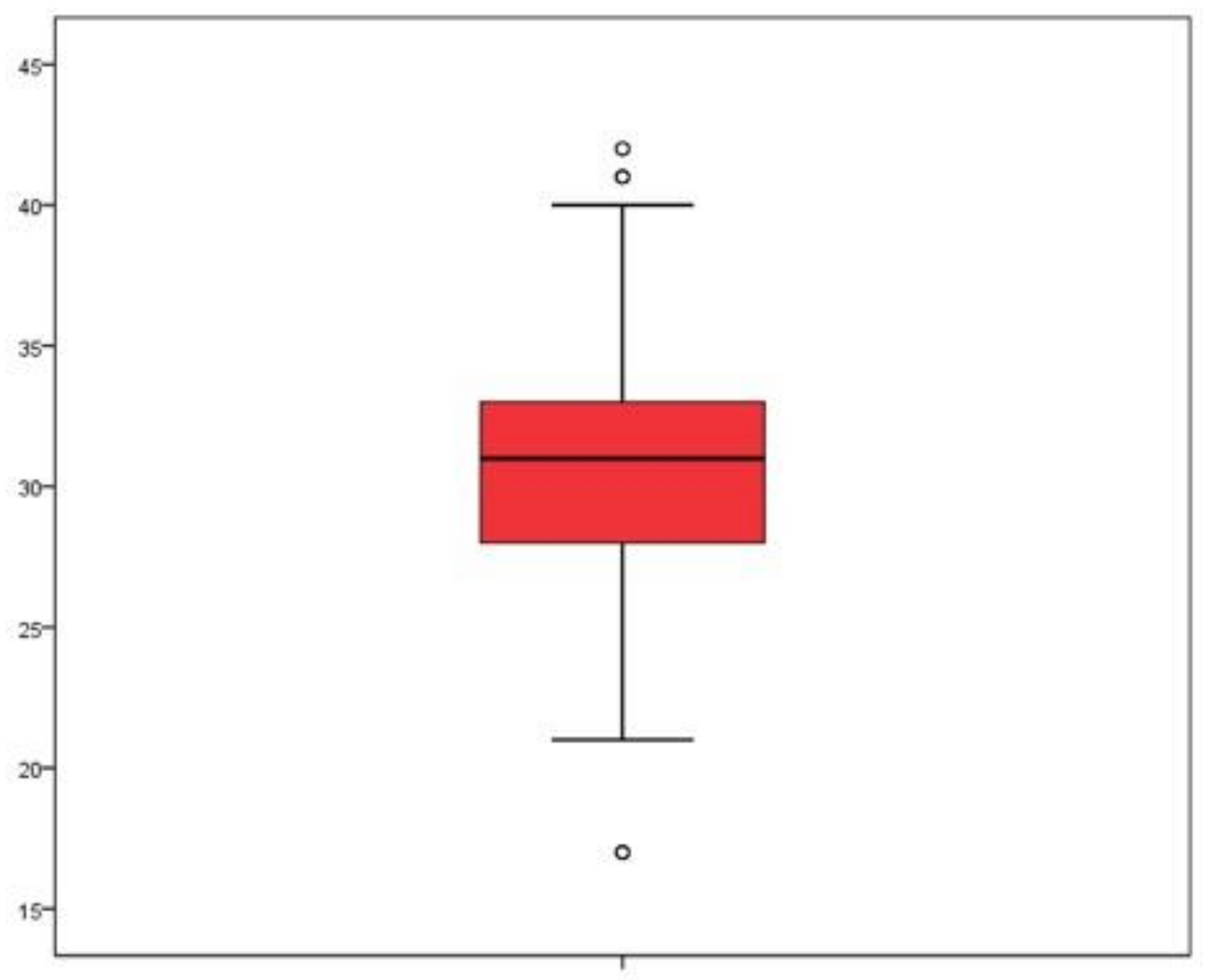
3.1.1. Students’ Level of Stigma toward Patients with Mental Health Problems
3.1.2. Factors Associated with Stigma toward Mental Health Problems and Mental Health Patients
3.2. Results of the Qualitative Phase
3.2.1. Participants
3.2.2. Fear and Lack of Knowledge
3.2.3. Breaking the Silence
3.2.4. Integration into Society
4. Discussion
Relevance for Clinical Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Mental Health Stigma Scale (MHSS)
- Someone who is recovering from a mental health problem can look after their children alone.
- Someone who is recovering from a mental health problem should remain in hospital or in supported housing.
- Someone who is recovering from a mental health problem can live alone.
- People with mental health problems have the right to adopt children.
- Discipline/education at home can prevent the majority of mental health problems in children.
- People with a lack of drive tend to have mental health problems.
- Someone with a lack of discipline/education is more likely to have a mental health problem.
- People with mental health problems are more likely to be violent.
- I would be worried if a mental health hospital was opened near to where I live.
- It would be difficult for me to establish a friendship with someone with a mental health problem.
- For me, being admitted to a mental health hospital would be a sign of having failed in life.
- It would be difficult for me if a friend found out that one of my family members had a mental health problem.
References
- World Health Organization. Mental Health Evidence and Research Team. In Mental Health Atlas 2011; World Health Organization: Geneva, Switzerland, 2011; 82p. [Google Scholar]
- Pescosolido, B.A. The Public Stigma of Mental Illness. J. Health Soc. Behav. 2013, 54, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.-C.; Lin, C.-Y.; Gronholm, P.C.; Wu, T.-H. Cross-Validation of Two Commonly Used Self-Stigma Measures, Taiwan Versions of the Internalized Stigma Mental Illness Scale and Self-Stigma Scale–Short, for People With Mental Illness. Assessment 2018, 25, 777–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.-C.; Su, J.-A.; Chang, K.-C.; Lin, C.-Y.; Koschorke, M.; Thornicroft, G. Perceived stigma of caregivers: Psychometric evaluation for Devaluation of Consumer Families Scale. Int. J. Clin. Health Psychol. 2018, 18, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.-Y.; Chen, S.-P.; Pakpour, A.H.; Lin, C.-Y. The Mediation Role of Self-Esteem for Self-Stigma on Quality of Life for People with Schizophrenia: A Retrospectively Longitudinal Study. J. Pacific Rim. Psychol. 2018, 12, e10. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.-C.; Su, J.-A.; Chang, K.-C.; Lin, C.-Y.; Koschorke, M.; Rüsch, N.; Thornicroft, G. Development of the Family Stigma Stress Scale (FSSS) for Detecting Stigma Stress in Caregivers of People with Mental Illness. Eval. Health Prof. 2019, 42, 148–168. [Google Scholar] [CrossRef]
- Chang, C.-C.; Yen, C.-F.; Jang, F.-L.; Su, J.-A.; Lin, C.-Y. Comparing Affiliate Stigma between Family Caregivers of People with Different Severe Mental Illness in Taiwan. J. Nerv. Ment. Dis. 2017, 205, 542–549. [Google Scholar] [CrossRef]
- Chang, C.-C.; Wu, T.-H.; Chen, C.-Y.; Lin, C.-Y. Comparing Self-stigma Between People with Different Mental Disorders in Taiwan. J. Nerv. Ment. Dis. 2016, 204, 547–553. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Chang, C.-C.; Wu, T.-H.; Wang, J.-D. Dynamic changes of self-stigma, quality of life, somatic complaints, and depression among people with schizophrenia: A pilot study applying kernel smoothers. Stigma Health 2016, 1, 29–43. [Google Scholar] [CrossRef]
- Chang, C.-C.; Su, J.-A.; Tsai, C.-S.; Yen, C.-F.; Liu, J.-H.; Lin, C.-Y. Rasch analysis suggested three unidimensional domains for Affiliate Stigma Scale: Additional psychometric evaluation. J. Clin. Epidemiol. 2015, 68, 674–683. [Google Scholar] [CrossRef]
- Madoz-Gúrpide, A.; Ballesteros Martín, J.C.; Leira Sanmartín, M.; García Yagüe, E. Enfoque en la atención integral a los pacientes con trastorno mental grave treinta años después de la reforma psiquiátrica. Rev. Esp. Salud Pública 2017, 91. [Google Scholar]
- World Health Organization. The World Health Report 2001-Mental Health: New Understanding, New Hope; WHO: Geneve, Switzerland, 2013. [Google Scholar]
- Link, B.G.; Phelan, J.C. Stigma and its public health implications. Lancet 2006, 367, 528–529. [Google Scholar] [CrossRef]
- Horsfall, J.; Cleary, M.; Hunt, G.E. Stigma in Mental Health: Clients and Professionals. Issues Ment. Health Nurs. 2010, 31, 450–455. [Google Scholar] [CrossRef]
- Mårtensson, G.; Jacobsson, J.W.; Engström, M. Mental health nursing staff’s attitudes towards mental illness: An analysis of related factors. J. Psychiatry Ment. Health Nurs. 2014, 21, 782–788. [Google Scholar] [CrossRef] [Green Version]
- Chin, S.H.; Balon, R. Attitudes and perceptions toward depression and schizophrenia among residents in different medical specialties. Acad. Psychiatry 2006, 30, 262–263. [Google Scholar] [CrossRef] [PubMed]
- Lmudena, A. La lucha contra el estigma y la discriminación en salud mental. Una estrategia compleja basada en la información disponible. Rev. Asoc. Esp. Neuropsiq. 2008, 28, 43–83. [Google Scholar]
- Cook, T.M.; Wang, J. Descriptive epidemiology of stigma against depression in a general population sample in Alberta. BMC Psychiatry 2010, 10, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pescosolido, B.A.; Martin, J.K.; Long, J.S.; Medina, T.R.; Phelan, J.C.; Link, B.G. “A Disease Like Any Other”? A Decade of Change in Public Reactions to Schizophrenia, Depression, and Alcohol Dependence. Am. J. Psychiatry 2010, 167, 1321–1330. [Google Scholar] [CrossRef] [Green Version]
- Boyd, J.E.; Katz, E.P.; Link, B.G.; Phelan, J.C. The relationship of multiple aspects of stigma and personal contact with someone hospitalized for mental illness, in a nationally representative sample. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Makowski, A.C.; von dem Knesebeck, O. Depression stigma and migration–results of a survey from Germany. BMC Psychiatry 2017, 17, 381. [Google Scholar] [CrossRef]
- Ruiz, M.Á.; Montes, J.M.; Correas Lauffer, J.; Álvarez, C.; Mauriño, J.; De Dios Perrino, C. Opinions and beliefs of the Spanish population on serious mental illnesses (schizophrenia and bipolar disorder). Rev. Psiquiatr. Salud. Ment. 2012, 5, 98–106. [Google Scholar] [CrossRef]
- Granados-Gámez, G.; Lopez Rodriguez, M.D.M.; Corral Granados, A.; Márquez-Hernández, V.V. Attitudes and Beliefs of Nursing Students toward Mental Disorder: The Significance of Direct Experience with Patients. Perspect. Psychiatr. Care 2017, 53, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Poreddi, V.; Thimmaiah, R.; Math, S.B. Attitudes toward people with mental illness among medical students. J. Neurosci. Rural Pract. 2015, 6, 349–354. [Google Scholar] [PubMed]
- Patten, S.B.; Remillard, A.; Phillips, L.; Modgill, G.; Szeto, A.C.; Kassam, A.; Gardner, D.M. Effectiveness of contact-based education for reducing mental illness-related stigma in pharmacy students. BMC Med. Educ. 2012, 12, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Martínez, C.; Sánchez-Martínez, V.; Sales-Orts, R.; Dinca, A.; Richart-Martínez, M.; Ramos-Pichardo, J.D. Effectiveness of direct contact intervention with people with mental illness to reduce stigma in nursing students. Int. J. Ment. Health Nurs. 2019, 28, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Thornicroft, G.; Mehta, N.; Clement, S.; Evans-Lacko, S.; Doherty, M.; Rose, D.; Koschorke, M.; Shidhaye, R.; O’Reilly, C.; Henderson, C. Evidence for effective interventions to reduce mental-health-related stigma and discrimination. Lancet 2016, 387, 1123–1132. [Google Scholar] [CrossRef]
- Ay, P.; Save, D.; Fidanoglu, O. Does stigma concerning mental disorders differ through medical education? Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 63–67. [Google Scholar] [CrossRef]
- Sari, S.P.; Yuliastuti, E. Investigation of attitudes toward mental illness among nursing students in Indonesia. Int. J. Nurs. Sci. 2018, 5, 414–418. [Google Scholar] [CrossRef]
- Lawrence, D.; Kisely, S. Inequalities in healthcare provision for people with severe mental illness. J. Psychopharmacol. 2010, 24, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Enarsson, P.; Sandman, P.-O.; Hellzén, O. The Preservation of Order: The Use of Common Approach among Staff toward Clients in Long-Term Psychiatric Care. Qual. Health Res. 2007, 17, 718–729. [Google Scholar] [CrossRef] [Green Version]
- Kameg, K.; Mitchell, A.M.; Clochesy, J.; Howard, V.M.; Suresky, J. Communication and Human Patient Simulation in Psychiatric Nursing. Issues Ment. Health Nurs. 2009, 30, 503–508. [Google Scholar] [CrossRef]
- Samari, E.; Seow, E.; Chua, B.Y.; Ong, H.L.; Abdin, E.; Chong, S.A.; Subramaniam, M. Stigma towards people with mental disorders: Perspectives of nursing students. Arch. Psychiatr. Nurs. 2018, 32, 802–808. [Google Scholar] [CrossRef] [Green Version]
- Foster, K.; Withers, E.; Blanco, T.; Lupson, C.; Steele, M.; Giandinoto, J.A.; Furness, T. Undergraduate nursing students’ stigma and recovery attitudes during mental health clinical placement: A pre/post-test survey study. Int. J. Ment. Health Nurs. 2019, 28, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Ivankova, N.; Kawamura, Y. Emerging trends in the utilization of integration designs in the social, behavioral and health sciences. In The Sage Handbook of Mixed Methods in Social and Behavioral Research, 2nd ed.; Tashakkori, A., Teddlie, C., Eds.; Sage: London, UK, 2010; pp. 581–611. [Google Scholar]
- Plano Clark, V.L. The Adoption and Practice of Mixed Methods: U.S. Trends in Federally Funded Health-Related Research. Qual. Inq. 2010, 16, 428–440. [Google Scholar] [CrossRef]
- Creswell, J.; Plano Clark, V. Designing and Conducting Mixed Methods Research; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Creswell, J. Research Design. In Qualitative, Quantitative, and Mixed Methods Approaches, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Guetterman, T.C.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research through Joint Displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Polanco Frontera, N.; Cajigas Vargas, I.; Rivera Segarra, E.; Varas Díaz, N.; Santos Figueroa, A.; Rosario Hernández, E. Salud y sociedad investigaciones en psicologiía de la salud y psicologiía social. Salud Soc. 2013, 4, 250–263, ISSN-e-0718-7475. [Google Scholar] [CrossRef] [Green Version]
- Varas-Díaz, N.; Santos–Figueroa, A.; Polanco-Frontera, N.; Cajigas-Vargas, I.; Díaz, M.R.; Candelas, C.I.L.; Rosario-Hernández, E.; Rivera-Segarra, E. Desarrollo de una Escala para Medir el Estigma Relacionado a Problemas de Salud Mental en Puerto Rico. Rev. Puertorriquena Psicol. 2012, 23, 8. [Google Scholar]
- Polit, D.; Hungler, B. Investigación Cientifica en Ciencias de la Salud, 6th ed.; McGraw-Hill Interamericana: México City, Mexico, 2000. [Google Scholar]
- Jeon, Y.-H. The application of grounded theory and symbolic interactionism. Scand. J. Caring Sci. 2004, 18, 249–256. [Google Scholar] [CrossRef]
- Bryant, A.; Charmaz, K. The SAGE Handbook of Grounded Theory; SAGE Publications Ltd.: London, UK, 2007. [Google Scholar]
- Giorgi, A. The Theory, Practice, and Evaluation of the Phenomenological Method as a Qualitative Research Procedure. J. Phenomenol. Psychol. 1997, 28, 235–260. [Google Scholar] [CrossRef]
- Giorgi, A. The Descriptive Phenomenological Method in Psychology: A Modified Husserlian Approach; Duquesne University Press: Pittsburgh, PA, USA, 2009. [Google Scholar]
- Cornejo Cancino, M.; Salas Guzmán, N. Rigor y calidad metodológicos: Un reto a la investigación social cualitativa. Psicoperspectivas Individuo y Soc. 2011, 10, 12–34. [Google Scholar] [CrossRef]
- Happell, B.; Platania-Phung, C.; Bocking, J.; Scholz, B.; Horgan, A.; Manning, F.; Doody, R.; Hals, E.; Granerud, A.; Lahti, M.; et al. Nursing Students’ Attitudes Towards People Diagnosed with Mental Illness and Mental Health Nursing: An International Project from Europe and Australia. Issues Ment. Health Nurs. 2018, 39, 829–839. [Google Scholar] [CrossRef]
- Happell, B.; Gaskin, C.J.; Byrne, L.; Welch, A.; Gellion, S. Clinical Placements in Mental Health: A Literature Review. Issues Ment. Health Nurs. 2015, 36, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Happell, B.; Platania-Phung, C.; Scholz, B.; Bocking, J.; Horgan, A.; Manning, F.; Doody, R.; Hals, E.; Granerud, A.; Lahti, M.; et al. Changing attitudes: The impact of Expert by Experience involvement in Mental Health Nursing Education: An international survey study. Int. J. Ment. Health Nurs. 2019, 28, 480–491. [Google Scholar] [CrossRef] [PubMed]
- Guimón, J. Prejudice and Realities in Stigma. Int. J. Ment. Health 2010, 39, 20–43. [Google Scholar] [CrossRef]
- İnan, F.Ş.; Günüşen, N.; Duman, Z.Ç.; Ertem, M.Y. The Impact of Mental Health Nursing Module, Clinical Practice and an Anti-Stigma Program on Nursing Students’ Attitudes toward Mental Illness: A Quasi-Experimental Study. J. Prof. Nurs. 2019, 35, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Happell, B.; Gaskin, C.J. The attitudes of undergraduate nursing students towards mental health nursing: A systematic review. J. Clin. Nurs. 2013, 22, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Barrett, P.; Jackson, A. Swimming without the water: A critical perspective on mental health experience for adult nursing students. Nurse Educ. Pract. 2013, 13, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Madigan, R. How Memory Works–and How to make it Work for You. Available online: https://books.google.es/books?id=InT3CQAAQBAJ&pg=PA62&lpg=PA62&dq=How+Memory+Works+and+How+to+MakeIt+Work+for+You&source=bl&ots=flgLgBkRO8&sig=ACfU3U1XgXMHV6JKxemn4fsBNiE5lGaDAg&hl=es&sa=X&ved=2ahUKEwiiyuqsuYXkAhUGTBoKHbkZDJEQ6AEwCHoECAoQAQ#v=onepage&q=How Memory Works and How to MakeIt Work for You&f=false (accessed on 24 November 2019).



{kind=link}
{kind=link}
| Independent Variables | N = 359 (n/%) | Low Stigma (n = 106) (<29 Points) (n/%) | Moderate‒high Stigma (n = 253) (≥29 points) (n/%) |
|---|---|---|---|
| Gender | |||
| Male | 61 (17.0) | 18 (29.5) | 43 (70.5) |
| Female | 298 (83.0) | 88 (29.5) | 210 (70.5) |
| Year of study | |||
| First year | 91 (25.3) | 19 (20.9) | 72 (79.1) |
| Second year | 96 (26.7) | 29 (30.2) | 67 (69.8) |
| Third year | 84 (23.4) | 28 (33.3) | 56 (66.7) |
| Fourth year | 88 (24.5) | 30 (34.1) | 58 (65.9) |
| Clinical rotation in mental health | |||
| No | 319 (88.9) | 94 (29.5) | 225 (70.5) |
| Yes | 40 (11.1) | 12 (30.0) | 28 (70.0) |
| Having family members with mental health problems | |||
| No | 250 (69.6) | 83 (33.2) | 167 (66.8) |
| Yes | 109 (30.4) | 23 (21.1) | 86 (78.9) |
| Having friends with mental health problems | |||
| No | 282 (78.6) | 87 (30.9) | 195 (69.1) |
| Yes | 77 (21.4) | 19 (27.7) | 758 (75.3) |
| Logistic Regression Probability of High/Moderate Stigma | ||
|---|---|---|
| Variables | P-Value | OR CI95% |
| Gender | 0.518 | |
| Male (Reference cat.) | 1 | |
| Female | 1.23 (0.65–2.33) | |
| Year of study | ||
| First year (Reference cat.) | 1 | |
| Second year | 0.151 | 0.61 (0.31–1.20) |
| Third year | 0.043 | 0.49 (0.24–0.98) |
| Fourth year | 0.015 | 0.41 (0.20–0.84) |
| Clinical rotation in mental health | 0.995 | |
| No (Reference cat.) | 1 | |
| Yes | 1.00 (0.46–2.18) | |
| Having family members with mental health problems | 0.010 | |
| No (Reference cat.) | 1 | |
| Yes | 2.05 (1.19‒3.56) | |
| Having friends with mental health problems | 0.300 | |
| No (Reference cat.) | 1 | |
| Yes | 1.37 (0.76–2.48) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Almagro, J.; Hernández-Martínez, A.; Rodríguez-Almagro, D.; Quiros-García, J.M.; Solano-Ruiz, M.d.C.; Gómez-Salgado, J. Level of Stigma among Spanish Nursing Students toward Mental Illness and Associated Factors: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2019, 16, 4870. https://doi.org/10.3390/ijerph16234870
Rodríguez-Almagro J, Hernández-Martínez A, Rodríguez-Almagro D, Quiros-García JM, Solano-Ruiz MdC, Gómez-Salgado J. Level of Stigma among Spanish Nursing Students toward Mental Illness and Associated Factors: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2019; 16(23):4870. https://doi.org/10.3390/ijerph16234870
Chicago/Turabian StyleRodríguez-Almagro, Julián, Antonio Hernández-Martínez, David Rodríguez-Almagro, José Miguel Quiros-García, María del Carmen Solano-Ruiz, and Juan Gómez-Salgado. 2019. "Level of Stigma among Spanish Nursing Students toward Mental Illness and Associated Factors: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 16, no. 23: 4870. https://doi.org/10.3390/ijerph16234870
APA StyleRodríguez-Almagro, J., Hernández-Martínez, A., Rodríguez-Almagro, D., Quiros-García, J. M., Solano-Ruiz, M. d. C., & Gómez-Salgado, J. (2019). Level of Stigma among Spanish Nursing Students toward Mental Illness and Associated Factors: A Mixed-Methods Study. International Journal of Environmental Research and Public Health, 16(23), 4870. https://doi.org/10.3390/ijerph16234870