Refugee Status as a Possible Risk Factor for Childhood Enuresis


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Austin, P.F.; Bauer, S.B.; Bower, W.; Chase, J.; Franco, I.; Hoebeke, P.; Rittig, S.; Walle, J.V.; Von Gontard, A.; Wright, A.; et al. The standardization of terminology of lower urinary tract function in children and adolescents: Update report from the Standardization Committee of the International Children’s Continence Society. J. Urol. 2014, 191, 1863–1865. [Google Scholar] [CrossRef] [PubMed]
- Nevéus, T. Pathogenesis of enuresis: Towards a new understanding. Int. J. Urol. 2017, 24, 174–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, R.J. Annotation: Night wetting in children: Psychological aspects. J. Child Psychol. Psychiatry 1998, 39, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Longstaffe, S.; Moffatt, M.E.; Whalen, J.C. Behavioral and self-concept changes after six months of enuresis treatment: A randomized, controlled trial. Pediatrics 2000, 105, 935–940. [Google Scholar] [PubMed]
- Moffatt, M.E. Nocturnal enuresis: Psychologic implications of treatment and nontreatment. J. Pediatr. 1989, 114, 697–704. [Google Scholar] [CrossRef]
- Joinson, C.; Sullivan, S.; von Gontard, A.; Heron, J. Early childhood psychological factors and risk for bedwetting at school age in a UK cohort. Eur. Child. Adolesc. Psychiatry 2016, 25, 519–528. [Google Scholar] [CrossRef]
- Bähr, V.; Franzen, N.; Oelkers, W.; Pfeiffer, A.F.; Diederich, S. Effect of exogenous glucocorticoid on osmotically stimulated antidiuretic hormone secretion and on water reabsorption in man. Eur. J. Endocrinol. 2006, 155, 845–848. [Google Scholar] [CrossRef]
- Joinson, C.; Sullivan, S.; von Gontard, A.; Heron, J. Stressful Events in Early Childhood and Developmental Trajectories of Bedwetting at School Age. J. Pediatr. Psychol. 2016, 41, 1002–1010. [Google Scholar] [CrossRef] [Green Version]
- Ceri, V.; Özlü-Erkilic, Z.; Özer, Ü.; Yalcin, M.; Popow, C.; Akkaya-Kalayci, T. Psychiatric symptoms and disorders among Yazidi children and adolescents immediately after forced migration following ISIS attacks. Neuropsychiatrie 2016, 30, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Nasıroğlu, S.; Çeri, V.; Erkorkmaz, Ü.; Semerci, B. Determinants of psychiatric disorders in children refugees in Turkey’s Yazidi refugee camp. Psychiatry Clin. Psychopharmacol. 2018, 28, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Çeri, V.; Nasıroğlu, S.; Ceri, M.; Çetin, F.Ç. Psychiatric Morbidity Among a School Sample of Syrian Refugee Children in Turkey: A Cross-Sectional, Semistructured, Standardized Interview-Based Study. J. Am. Acad. Child. Adolesc. Psychiatry 2018, 57, 696–698. [Google Scholar] [CrossRef] [PubMed]
- Mežnarić, S.; Zlatković Winter, J. Forced Migration and Refugee Flows in Croatia, Slovenia and Bosnia-Herzegovina. Refuge 1993, 7, 3–6. [Google Scholar]
- Fazel, M.; Stein, A. The mental health of refugee children. Arch. Dis. Child. 2002, 87, 366–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronstein, I.; Montgomery, P. Psychological distress in refugee children: A systematic review. Clin. Child. Fam. Psychol. Rev. 2011, 14, 44–56. [Google Scholar] [CrossRef]
- Šikić, N.; Javornik, N.; Stracenski, M.; Bunjevac, T.; Buljan-Flander, G. Psychopathological differences among three groups of school children affected by the war in Croatia. Acta Med. Croat. 1997, 51, 143–149. [Google Scholar]
- Ajduković, M.; Ajduković, D. Psychological well-being of refugee children. Child Abuse Negl. 1993, 17, 843–854. [Google Scholar] [CrossRef]
- Elez, P.; Živić, D. Vukovarsko-srijemska županija u procesu stvaranja i obrane hrvatske države. In Vukovarsko-Srijemska Županija- Prostor, ljudi, Identitet; Institut društvenih znanosti Ivo Pilar: Zagreb, Croatia, 2012; pp. 181–202. [Google Scholar]
- Jones, L.; Rustemi, A.; Shahini, M.; Uka, A. Mental health services for war-affected children: Report of a survey in Kosovo. Br. J. Psychiatry 2003, 183, 540–546. [Google Scholar] [CrossRef]
- Nasıroğlu, S.; Çeri, V. Posttraumatic stress and depression in Yazidi refugees. Neuropsychiatr. Dis. Treat. 2016, 12, 2941–2948. [Google Scholar] [CrossRef] [Green Version]
- Tai, H.L.; Chang, Y.J.; Chang, S.C.; Chen, G.D.; Chang, C.P.; Chou, M.C. The epidemiology and factors associated with nocturnal enuresis and its severity in primary school children in Taiwan. Acta Paediatr. 2007, 96, 242–245. [Google Scholar] [CrossRef]
- Mejias, S.G.; Ramphul, K. Nocturnal enuresis in children from Santo Domingo, Dominican Republic: A questionnaire study of prevalence and risk factors. BMJ Paediatr. Open 2018, 2, e000311. [Google Scholar] [CrossRef]
- Doganer, Y.C.; Aydogan, U.; Ongel, K.; Sari, O.; Koc, B.; Saglam, K. The Prevalence and Sociodemographic Risk Factors of Enuresis Nocturna among Elementary School-age Children. J. Fam. Med. Prim. Care 2015, 4, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Miskulin, M.; Miskulin, I.; Mujkic, A.; Dumic, A.; Puntaric, D.; Buljan, V.; Bilic-Kirin, V.; Juretic-Kovac, D. Enuresis in school children from eastern Croatia. Turk. J. Pediatr. 2010, 52, 393–399. [Google Scholar]
- Theunis, M.; Van Hoecke, E.; Paesbrugge, S.; Hoebeke, P.; Vande Walle, J. Self-image and performance in children with nocturnal enuresis. Eur. Urol. 2002, 41, 660–667. [Google Scholar] [CrossRef]
- Chiozza, M.L.; Bernardinelli, L.; Caione, P.; Del Gado, R.; Ferrara, P.; Giorgi, P.L.; Montomoli, C.; Rottoli, A.; Vertucci, P. An Italian epidemiological multicentre study of nocturnal enuresis. Br. J. Urol. 1998, 81, 86–89. [Google Scholar] [CrossRef] [Green Version]
- Wen, J.G.; Wang, Q.W.; Chen, Y.; Wen, J.J.; Liu, K. An epidemiological study of primary nocturnal enuresis in Chinese children and adolescents. Eur. Urol. 2006, 49, 1107–1113. [Google Scholar] [CrossRef]
- Eapen, V.; Mabrouk, A.M. Prevalence and correlates of nocturnal enuresis in the United Arab Emirates. Saudi Med. J. 2003, 24, 49–51. [Google Scholar]
- Ozkan, K.U.; Garipardic, M.; Toktamis, A.; Karabiber, H.; Sahinkanat, T. Enuresis prevalence and accompanying factors in schoolchildren: A questionnaire study from southeast Anatolia. Urol. Int. 2004, 73, 149–155. [Google Scholar] [CrossRef]
- Aloni, M.N.; Ekila, M.B.; Ekulu, P.M.; Aloni, M.L.; Magoga, K. Nocturnal enuresis in children in Kinshasa, Democratic Republic of Congo. Acta Paediatr. 2012, 101, e475–e478. [Google Scholar] [CrossRef]
- Gümüş, B.; Vurgun, N.; Lekili, M.; Işcan, A.; Müezzinoğlu, T.; Büyuksu, C. Prevalence of nocturnal enuresis and accompanying factors in children aged 7–11 years in Turkey. Acta Paediatr. 1999, 88, 1369–1372. [Google Scholar] [CrossRef]
- Hansakunachai, T.; Ruangdaraganon, N.; Udomsubpayakul, U.; Sombuntham, T.; Kotchabhakdi, N. Epidemiology of enuresis among school-age children in Thailand. J. Dev. Behav. Pediatr. 2005, 26, 356–360. [Google Scholar] [CrossRef]
- von Gontard, A.; Heron, J.; Joinson, C. Family history of nocturnal enuresis and urinary incontinence: Results from a large epidemiological study. J. Urol. 2011, 185, 2303–2306. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
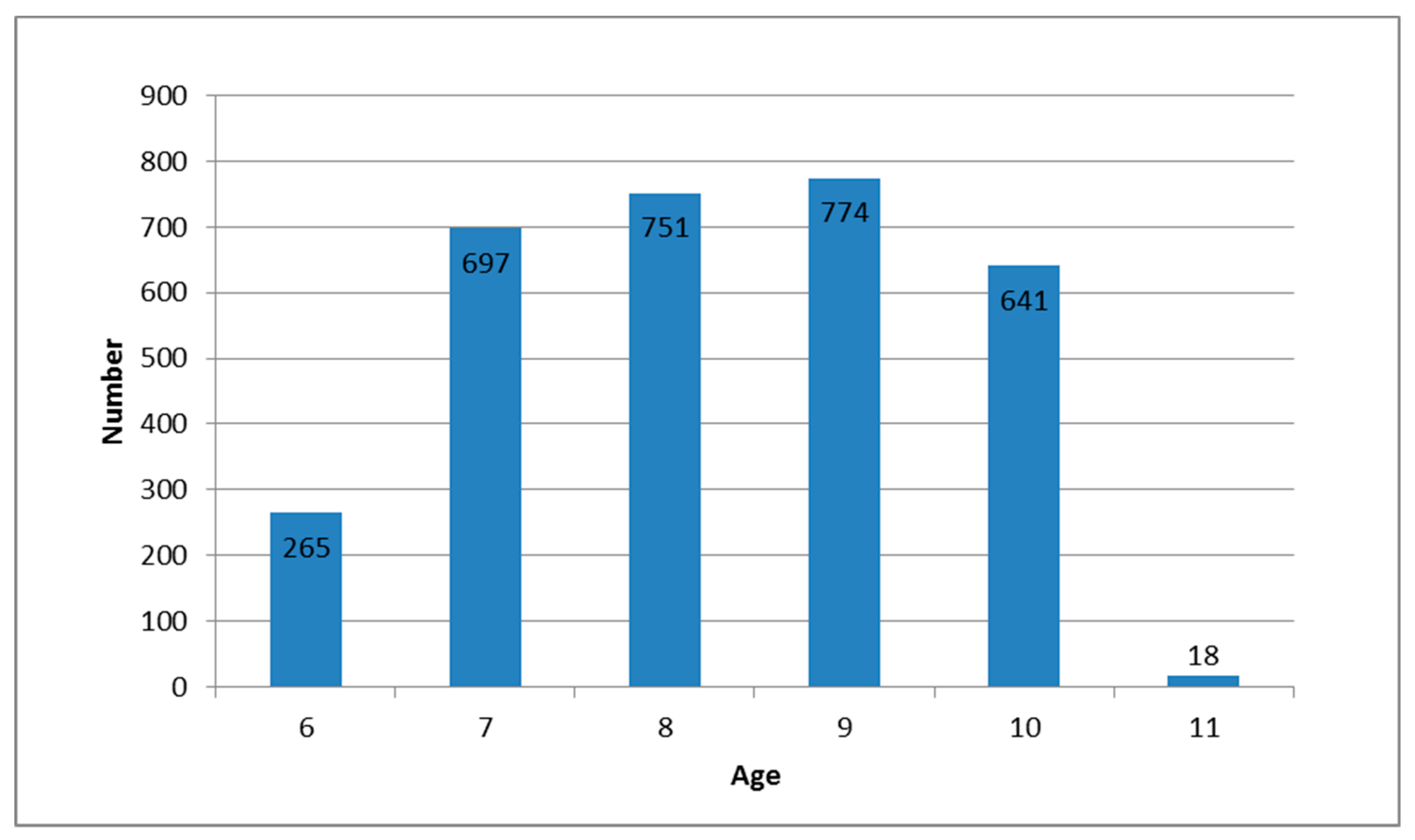
| Age (Years) | Enuretic Children | Total | |
|---|---|---|---|
| n | % | n | |
| 6 | 9 | 3.4 | 256 |
| 7 | 16 | 2.3 | 697 |
| 8 | 18 | 2.4 | 751 |
| 9 | 19 | 2.5 | 774 |
| 10 | 9 | 1.7 | 541 |
| 11 | 0 | 0 | 18 |
| Total | 71 | 2.3 | 3046 |
| Number of Children | Odds Ratios | 95% CI | p * | |||
|---|---|---|---|---|---|---|
| Enuretic | Non-Enuretic | Total | ||||
| Maternal enuresis | ||||||
| Yes | 20 | 153 | 173 | 7.4 | 4.3–12.8 | <0.001 |
| No | 49 | 2781 | 2830 | |||
| Total | 69 | 2934 | 3003 | |||
| Paternal enuresis | ||||||
| Yes | 15 | 89 | 104 | 9.5 | 5.1–17.6 | <0.001 |
| No | 48 | 2698 | 2746 | |||
| Total | 63 | 2787 | 2850 | |||
| Parental Status of Refugee or Displaced Person | p * | |||
|---|---|---|---|---|
| Yes | No | Total | ||
| Maternal enuresis | ||||
| Yes | 127 | 44 | 171 | 0.001 |
| No | 1709 | 1088 | 2797 | |
| Total | 1836 | 1132 | 2968 | |
| Paternal enuresis | ||||
| Yes | 66 | 33 | 99 | 0.04 |
| No | 1447 | 1136 | 2583 | |
| Total | 1513 | 1169 | 2682 | |
| Number of Children | p * | |||
|---|---|---|---|---|
| Enuretic | Non-Enuretic | Total | ||
| Refugee or displaced person (mother or/and father) | ||||
| Yes | 53 | 2066 | 2119 | 0.41 |
| No | 18 | 880 | 898 | |
| Total | 71 | 2946 | 3017 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurković, M.; Tomašković, I.; Tomašković, M.; Smital Zore, B.; Pavić, I.; Roić, A.C. Refugee Status as a Possible Risk Factor for Childhood Enuresis. Int. J. Environ. Res. Public Health 2019, 16, 1293. https://doi.org/10.3390/ijerph16071293
Jurković M, Tomašković I, Tomašković M, Smital Zore B, Pavić I, Roić AC. Refugee Status as a Possible Risk Factor for Childhood Enuresis. International Journal of Environmental Research and Public Health. 2019; 16(7):1293. https://doi.org/10.3390/ijerph16071293
Chicago/Turabian StyleJurković, Marija, Igor Tomašković, Mirna Tomašković, Branka Smital Zore, Ivan Pavić, and Andrea Cvitković Roić. 2019. "Refugee Status as a Possible Risk Factor for Childhood Enuresis" International Journal of Environmental Research and Public Health 16, no. 7: 1293. https://doi.org/10.3390/ijerph16071293
APA StyleJurković, M., Tomašković, I., Tomašković, M., Smital Zore, B., Pavić, I., & Roić, A. C. (2019). Refugee Status as a Possible Risk Factor for Childhood Enuresis. International Journal of Environmental Research and Public Health, 16(7), 1293. https://doi.org/10.3390/ijerph16071293