Association between Diabetes and Cognitive Function among People over 45 Years Old in China: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
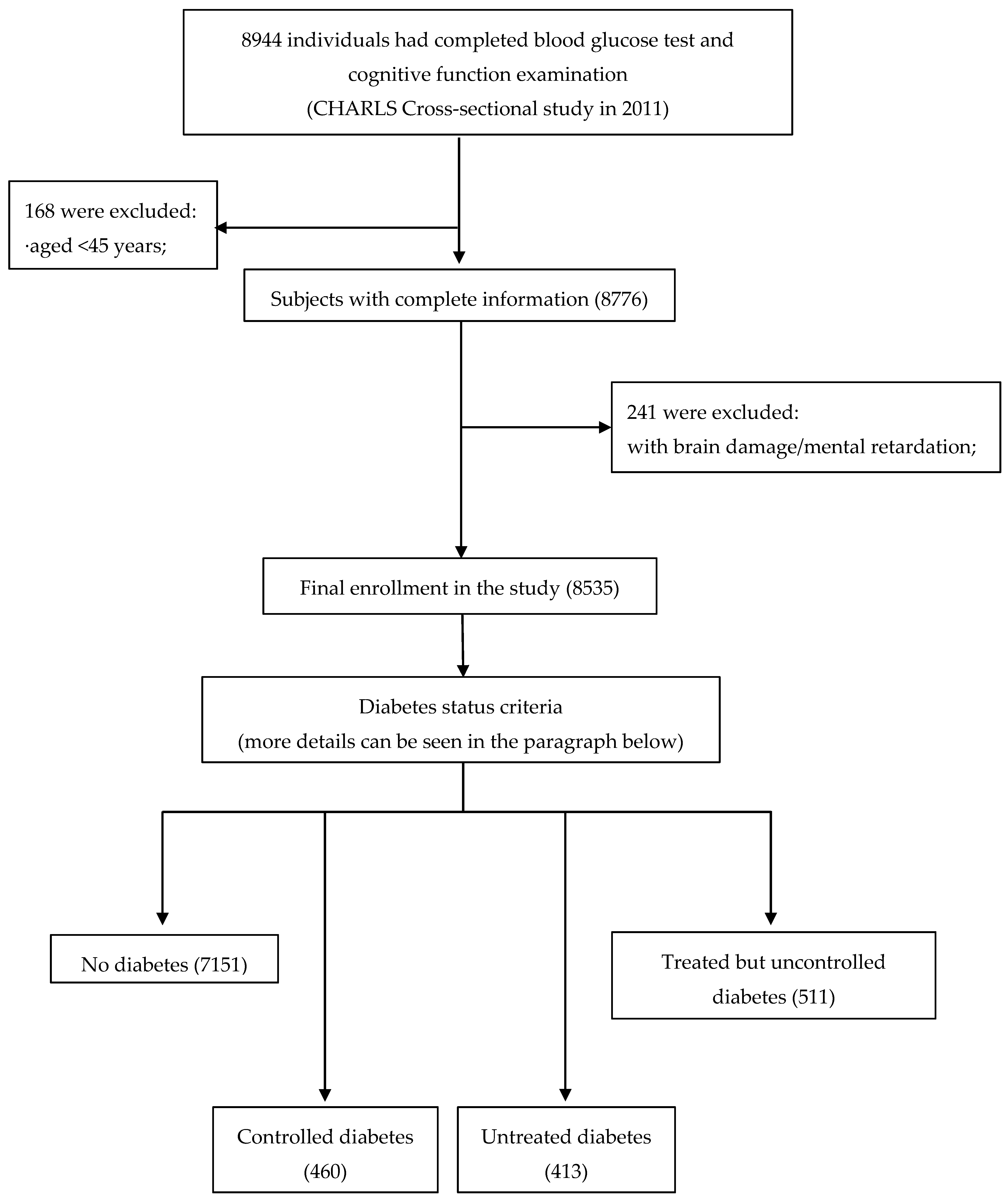
2.1. Study Population
2.2. Measurement of Cognitive Function in CHARLS
2.3. Definition of Diabetes Status
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Subjects Characteristics
3.2. Reliability of Cognition Scales
3.3. Association between Covariates and Cognition
3.4. Association between Diabetes Status and Cognition
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Friedrich, M.J. New Figures on Global Dementia Cases. JAMA 2015, 314, 1553. [Google Scholar] [CrossRef]
- Liu, J.; Wang, L.N.; Tan, J.P.; Shubhakaran, K.P.; Khichar, R.J. Dementia in China: current status. Neurology 2013, 81, 1077–1078. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Gao, P.; Zhang, M.; Huang, Z.; Zhang, D.; Deng, Q.; Li, Y.; Zhao, Z.; Qin, X.; Jin, D.; et al. Prevalence and Ethnic Pattern of Diabetes and Prediabetes in China in 2013. JAMA 2017, 317, 2515–2523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Liu, S.W.; Wang, L.J.; Bai, Y.M.; Zeng, X.Y.; Guo, H.B.; Liu, Y.N.; Jiang, Y.Y.; Dong, W.L.; He, G.X.; et al. Burden of diabetes, hyperglycaemia in China from to 2016: Findings from the 1990 to 2016, global burden of disease study. Diabetes Metab. 2018. [Google Scholar] [CrossRef] [PubMed]
- Biessels, G.J.; Staekenborg, S.; Brunner, E.; Brayne, C.; Scheltens, P. Risk of dementia in diabetes mellitus: A systematic review. Lancet Neurol. 2006, 5, 64–74. [Google Scholar] [CrossRef]
- Cukierman, T.; Gerstein, H.C.; Williamson, J.D. Cognitive decline and dementia in diabetes—systematic overview of prospective observational studies. Diabetologia 2005, 48, 2460–2469. [Google Scholar] [CrossRef] [Green Version]
- Strachan, M.W.J.; Reynolds, R.M.; Marioni, R.E.; Price, J.F. Cognitive function, dementia and type 2 diabetes mellitus in the elderly. Nat. Rev. Endocrinol. 2011, 7, 108–114. [Google Scholar] [CrossRef]
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF Diabetes Atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: a Delphi consensus study. Tijdschrift Voor Verpleeghuisgeneeskunde 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef]
- Li, J.; Cesari, M.; Liu, F.; Dong, B.; Vellas, B. Effects of Diabetes Mellitus on Cognitive Decline in Patients with Alzheimer Disease: A Systematic Review. Can. J. Diabetes 2017, 41, 114–119. [Google Scholar] [CrossRef]
- Takeda, S.; Sato, N.; Rakugi, H.; Morishita, R. Molecular mechanisms linking diabetes mellitus and Alzheimer disease: beta-amyloid peptide, insulin signaling, and neuronal function. Mol. Biosyst. 2011, 7, 1822–1827. [Google Scholar] [CrossRef]
- Sheen, Y.J.; Sheu, W.H. Association between hypoglycemia and dementia in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2016, 116, 279–287. [Google Scholar] [CrossRef]
- Nie, H.; Xu, Y.; Liu, B.; Zhang, Y.; Lei, T.; Hui, X.; Zhang, L.; Wu, Y. The prevalence of mild cognitive impairment about elderly population in China: a meta-analysis. Int. J. Geriatr. Psychiatry 2011, 26, 558–563. [Google Scholar] [CrossRef]
- Seo, E.H.; Lee, D.Y.; Kim, S.G.; Kim, K.W.; Kim, D.H.; Kim, B.J.; Kim, M.D.; Kim, S.Y.; Kim, Y.H.; Kim, J.L.; et al. Validity of the telephone interview for cognitive status (TICS) and modified TICS (TICSm) for mild cognitive imparment (MCI) and dementia screening. Arch. Gerontol. Geriatr. 2011, 52, 26–30. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort Profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef]
- Guerreroberroa, E.; Ravonaspringer, R.; Schmeidler, J.; Silverman, J.M.; Sano, M.; Koifmann, K.; Preiss, R.; Hoffman, H.; Heymann, A.; Schnaiderbeeri, M. Age, gender, and education are associated with cognitive performance in an older Israeli sample with type 2 diabetes. Int. J. Geriatr. Psychiatry 2013, 9, 299–309. [Google Scholar]
- Liu, H.; Xu, X.; Hall, J.J.; Wu, X.; Zhang, M. Differences in depression between unknown diabetes and known diabetes: results from China health and retirement longitudinal study. Int. Psychogeriatr. 2016, 28, 1191–1199. [Google Scholar] [CrossRef]
- Cheng, H.G.; Chen, S.; Mcbride, O.; Phillips, M.R. Prospective relationship of depressive symptoms, drinking, and tobacco smoking among middle-aged and elderly community-dwelling adults: Results from the China Health and Retirement Longitudinal Study (CHARLS). J. Affect. Disord. 2016, 195, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Dybjer, E.; Nilsson, P.M.; Engström, G.; Helmer, C.; Nägga, K. Pre-diabetes and diabetes are independently associated with adverse cognitive test results: a cross-sectional, population-based study. BMC Endocr. Disord. 2018, 18, 91–100. [Google Scholar] [CrossRef]
- Pugazhenthi, S.; Qin, L.; Reddy, P.H. Common neurodegenerative pathways in obesity, diabetes, and Alzheimer’s disease. Biochim. Biophys. Acta 2017, 1863, 1037–1045. [Google Scholar] [CrossRef]
- Lee, Y.; Smofsky, A.; Nykoliation, P.; Allain, S.J.; Lewis-Daly, L.; Schwartz, J.; Pollack, J.H.; Tarride, J.E.; Mclntyre, R.S. Cognitive Impairment Mediates Workplace Impairment in Persons with Type 2 Diabetes Mellitus: Results From the Motivaction Study. Can. J. Diabetes 2017, 42, 289–295. [Google Scholar] [CrossRef]
- Meneilly, G.S.; Tessier, D.M. Diabetes, Dementia and Hypoglycemia. Can. J. Diabetes 2016, 40, 73–76. [Google Scholar] [CrossRef]
- Gao, Y.; Xiao, Y.; Miao, R.; Zhao, J.; Cui, M.; Huang, G.; Fei, M. The prevalence of mild cognitive impairment with type 2 diabetes mellitus among elderly people in China: A cross-sectional study. Arch. Gerontol. Geriatr. 2016, 62, 138–142. [Google Scholar] [CrossRef]
- Nooyens, A.C.; Baan, C.A.; Spijkerman, A.M.; Verschuren, W.M. Type 2 diabetes and cognitive decline in middle-aged men and women: the Doetinchem Cohort Study. Diabetes Care 2010, 33, 1964–1969. [Google Scholar] [CrossRef]
- Velayudhan, L.; Poppe, M.; Archer, N.; Proitsi, P.; Brown, R.G.; Lovestone, S. Risk of developing dementia in people with diabetes and mild cognitive impairment. Br. J. Psychiatry 2010, 196, 36–40. [Google Scholar] [CrossRef] [Green Version]
- Pappas, C.; Andel, R.; Infurna, F.J.; Seetharaman, S. Glycated haemoglobin (HbA1c), diabetes and trajectories of change in episodic memory performance. J. Epidemiol. Community Health 2017, 71, 115–120. [Google Scholar] [CrossRef]
- Okereke, O.I.; Kang, J.H.; Cook, N.R.; Gaziano, J.M.; Manson, J.E.; Buring, J.E.; Grodstein, F. Type 2 Diabetes Mellitus and Cognitive Decline in Two Large Cohorts of Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2008, 56, 1028–1036. [Google Scholar] [CrossRef]
- Ebady, S.; Arami, M.; Shafigh, M.H. Investigation on the relationship between diabetes mellitus type 2 and cognitive impairment. Diabetes Res. Clin. Pract. 2008, 82, 305–309. [Google Scholar] [CrossRef]
- Degen, C.; Toro, P.; Schönknecht, P.; Sattler, C.; Schröder, J. Diabetes mellitus Type II and cognitive capacity in healthy aging, mild cognitive impairment and Alzheimer’s disease. Psychiatry Res. 2016, 240, 42–46. [Google Scholar] [CrossRef]
- Koekkoek, P.S.; Kappelle, L.J.; van den Berg, E.; Rutten, G.E.; Biessels, G.J. Cognitive function in patients with diabetes mellitus: guidance for daily care. Lancet Neurol. 2015, 14, 329–340. [Google Scholar] [CrossRef]
- Stein, Z.; Susser, M.; Saenger, G.; Marolla, F. Nutrition and Mental Performance: Prenatal exposure to the Dutch famine of 1944–1945 seems not related to mental performance at age 19. Science 1972, 178, 708–713. [Google Scholar] [CrossRef]
- De Rooij, S.R.; Wouters, H.; Yonker, J.E.; Painter, R.C.; Roseboom, T.J. Prenatal undernutrition and cognitive function in late adulthood. Proc. Natl. Acad. Sci. USA 2010, 107, 16881–16886. [Google Scholar] [CrossRef] [Green Version]
- De Groot, R.H.; Stein, A.D.; Jolles, J.; van Boxtel, M.P.; Blauw, G.J.; van de Bor, M.; Lumey, L. Prenatal famine exposure and cognition at age 59 years. Int. J. Epidemiol. 2011, 40, 327–337. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Zhang, Z.; Li, L.; Liu, J. Early life exposure to China’s 1959-61 famine and midlife cognition. Int. J. Epidemiol. 2017, 47, 109–120. [Google Scholar] [CrossRef]
- Biessels, G.J.; Strachan, M.W.J.; Visseren, F.L.; Kappelle, L.J.; Whitmer, R.A. Dementia and cognitive decline in type 2 diabetes and prediabetic stages: towards targeted interventions. Lancet Diabetes Endocrinol. 2014, 2, 246–255. [Google Scholar] [CrossRef]
- Sörensen, B.M.; Houben, A.J.; Berendschot, T.T.; Schouten, J.S.; Kroon, A.A.; van der Kallen, C.J.; Henry, R.M.; Koster, A.; Sep, S.J.; Dagnelie, P.C.; et al. Prediabetes and Type 2 Diabetes Are Associated With Generalized Microvascular Dysfunction: The Maastricht Study. Circulation 2016, 134, 1339–1352. [Google Scholar] [CrossRef]
- Stehouwer, C.D.A. Microvascular Dysfunction and Hyperglycemia: A Vicious Cycle with Widespread Consequences. Diabetes 2018, 67, 1729–1741. [Google Scholar] [CrossRef]
- Seetharaman, S.; Andel, R.; Mcevoy, C.; Dahl Aslan, A.K.; Finkel, D.; Pedersen, N.L. Blood Glucose, Diet-Based Glycemic Load and Cognitive Aging Among Dementia-Free Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 471–479. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Diabetes Status | p | |||
|---|---|---|---|---|---|
| A (n = 7151) | B (n = 460) | C (n = 413) | D (n = 511) | ||
| Age (years, mean ± SD) | 59.5 ± 9.5 | 60.8 ± 9.5 | 61.7 ± 9.7 | 60.4 ± 8.5 | <0.001 |
| Age groups (n, %) | <0.001 | ||||
| 46–59 | 3880 (54.3) | 232 (50.4) | 185 (44.8) | 241 (47.2) | |
| 60–74 | 2703 (37.8) | 181 (39.4) | 182 (44.1) | 238 (46.6) | |
| ≥75 | 568 (7.9) | 47 (10.2) | 46 (11.14) | 32 (6.3) | |
| Educational levels (n, %) | 0.843 | ||||
| primary school or below | 4993 (69.82) | 323 (70.22) | 303(73.4) | 353 (69.1) | |
| middle school | 1428 (20.0) | 89 (19.4) | 72 (17.4) | 106 (20.7) | |
| high school or above | 730 (10.2) | 48 (10.4) | 38 (9.2) | 52 (10.2) | |
| BMI (kg/m2, n, %) | <0.001 | ||||
| <18.5 | 3870 (54.1) | 188 (40.9) | 183 (44.3) | 207 (40.5) | |
| 18.5–23.9 | 527 (7.4) | 20 (4.4) | 25 (6.1) | 13 (2.5) | |
| 24.0–27.9 | 2016 (28.2) | 154 (33.5) | 142 (34.4) | 192 (37.6) | |
| ≥28.0 | 738 (10.3) | 98 (21.3) | 63 (15.3) | 99 (19.4) | |
| Depression (n, %) | 0.049 | ||||
| Yes | 1566 (21.9) | 112 (24.4) | 103 (24.9) | 134 (26.2) | |
| No | 5585 (78.1) | 348 (75.6) | 310 (75.1) | 377 (73.8) | |
| Marital status (n, %) | 0.108 | ||||
| married | 5947 (83.2) | 380 (82.6) | 329 (79.7) | 438 (85.7) | |
| other status | 1204 (16.8) | 80 (17.4) | 84 (20.3) | 73 (14.3) | |
| Living areas (n, %) | <0.001 | ||||
| rural | 5920 (82.8) | 357 (77.6) | 331 (80.2) | 381 (74.6) | |
| urban | 1231 (17.2) | 103 (22.4) | 82 (19.9) | 130 (25.4) | |
| Hypertension (n, %) | <0.001 | ||||
| Yes | 2751 (38.5) | 261 (56.7) | 205 (49.6) | 281 (55.0) | |
| No | 4400 (61.5) | 199 (43.3) | 208 (50.4) | 230 (45.0) | |
| Glucose (mg/dL, M(Q)) | 100.3 (14.1) | 130.8 (41.1) | 139.5 (41.1) | 151.6 (69.5) | <0.001 |
| HbAlc (%, mean ± SD) | 5.1 ± 0.4 | 5.8 ± 1.2 | 6.0 ± 1.4 | 6.8 ± 1.8 | <0.001 |
| Cognition (mean ± SD) | |||||
| episodic memory | 3.2 ± 1.9 | 3.1 ± 1.7 | 2.9 ± 1.9 | 3.2 ± 1.9 | 0.014 |
| executive function | 7.0 ± 3.2 | 7.0 ± 3.4 | 6.6 ± 3.3 | 7.2 ± 3.2 | 0.098 |
| Characteristics | Episodic Memory β (p) | Executive Functionβ (p) |
|---|---|---|
| Age, y (“45–59” as reference) | ||
| 60–74 | −0.354 (<0.001) | −0.332 (<0.001) |
| ≥75 | −1.323 (<0.001) | −1.847 (<0.001) |
| Gender (“male” as reference) | 0.021 (0.600) | −1.205 (<0.001) |
| Living areas (“rural” as reference) | 0.532 (<0.001) | 1.075 (<0.001) |
| Educational level | ||
| Primary school or below (reference) | ||
| Middle school | 0.779 (<0.001) | 1.772 (<0.001) |
| High school or above | 1.081 (<0.001) | 1.910 (<0.001) |
| Marital status (“married as reference”) | −0.072 (0.175) | −0.296 (<0.001) |
| Hypertension status (“no hypertension” as reference) | −0.107 (0.009) | −0.155 (0.015) |
| BMI level | ||
| Underweight | −0.244 (0.002) | −0.517 (<0.001) |
| Normal weight (reference) | ||
| Overweight | 0.106 (0.018) | 0.396 (<0.001) |
| Obesity | 0.234 (<0.001) | 0.546 (<0.001) |
| Depression status (“no depression” as reference) | −0.544 (<0.001) | −0.987 (<0.001) |
| Full Sample (n = 8535) | Episodic Memory | Executive Function | ||
|---|---|---|---|---|
| Model 1 a β(p) | Model 2 c β(p) | Model 1 b β(p) | Model 2 c β(p) | |
| Diabetes status (“No diabetes” as reference) | ||||
| Controlled diabetes | −0.095 (0.263) | 0.216 (0.840) | −0.031 (0.815) | −0.716 (0.706) |
| Untreated diabetes | −0.192 (0.030) * | −0.235 (0.819) | −0.197 (0.154) | 0.491 (0.789) |
| Treated but uncontrolled diabetes | −0.048 (0.551) | 0.375 (0.730) | 0.114 (0.366) | −0.029 (0.988) |
| Duration of diabetes | 0.072 (0.426) | 0.087 (0.662) | −0.017 (0.905) | −0.231 (0.527) |
| Glucose, mg/dL | −0.0009 (0.076) | −0.0007 (0.725) | −0.001 (0.236) | −0.0001 (0.968) |
| HbA1c, % | −0.04 (0.080) | 0.007 (0.938) | −0.048 (0.179) | 0.016 (0.919) |
| Age Groups | Episodic Memory | Executive Function | ||
|---|---|---|---|---|
| Model 1 a β(p) | Model 2 c β(p) | Model 1 b β(p) | Model 2 c β(p) | |
| Sample in 45–59 years (n = 4538) | ||||
| Diabetes status (“No diabetes” as reference) | ||||
| Controlled diabetes | −0.154 (0.209) | −0.138 (0.953) | 0.044 (0.807) | −2.900 (0.521) |
| Untreated diabetes | −0.471 (0.001) * | −0.005 (0.998) | −0.035 (0.076) | −3.570 (0.427) |
| Treated but uncontrolled diabetes | −0.145 (0.228) | 0.172 (0.938) | 0.208 (0.234) | −1.593 (0.706) |
| Duration of diabetes | 0.025 (0.863) | 0.191 (0.613) | 0.122 (0.580) | −0.111 (0.876) |
| Glucose, mg/dL | −0.001 (0.135) | 0.0001 (0.977) | −0.001 (0.861) | −0.0007 (0.907) |
| HbA1c, % | −0.074 (0.027) * | 0.104 (0.457) | −0.051 (0.296) | −0.007 (0.977) |
| Sample in 60–74 years (n = 3304) | ||||
| Diabetes status (“No diabetes” as reference) | ||||
| Controlled diabetes | 0.007 (0.956) | 0.275 (0.852) | −0.024 (0.914) | −1.124 (0.645) |
| Untreated diabetes | 0.104 (0.421) | −1.14 (0.417) | −0.037 (0.866) | −1.816 (0.438) |
| Treated but uncontrolled diabetes | −0.032 (0.784) | 0.307 (0.845) | −0.118 (0.544) | −1.183 (0.651) |
| Duration of diabetes | 0.054 (0.671) | −0.035 (0.902) | −0.104 (0.615) | −0.124 (0.794) |
| Glucose, mg/dL | −0.001 (0.162) | −0.002 (0.543) | −0.002 (0.122) | 0.002 (0.684) |
| HbA1c, % | −0.037 (0.275) | −0.091 (0.549) | −0.102 (0.072) | −0.062 (0.804) |
| Sample in ≥75 years (n = 693) | ||||
| Diabetes status (“No diabetes” as reference) | ||||
| Controlled diabetes | −0.098 (0.672) | −0.111 (0.633) | −0.250 (0.559) | −1.124 (0.645) |
| Untreated diabetes | −0.249 (0.282) | −0.267 (0.249) | −0.277 (0.514) | −1.816 (0.438) |
| Treated but uncontrolled diabetes | 0.016 (0.954) | 0.008 (0.977) | 0.218 (0.666) | −1.183 (0.651) |
| Duration of diabetes | 0.028 (0.934) | 0.021 (0.948) | 0.283 (0.717) | 0.181 (0.823) |
| Glucose, mg/dL | −0.001 (0.617) | −0.001 (0.624) | −0.003 (0.330) | −0.003 (0.375) |
| HbA1c, % | 0.032 (0.668) | 0.041 (0.584) | −0.042 (0.767) | 0.027 (0.844) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Yang, J.; Liao, Z.; Zhao, X.; Hu, X.; Zhu, W.; Zhang, Z. Association between Diabetes and Cognitive Function among People over 45 Years Old in China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 1294. https://doi.org/10.3390/ijerph16071294
Zhang L, Yang J, Liao Z, Zhao X, Hu X, Zhu W, Zhang Z. Association between Diabetes and Cognitive Function among People over 45 Years Old in China: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(7):1294. https://doi.org/10.3390/ijerph16071294
Chicago/Turabian StyleZhang, Li, Jiao Yang, Zhangyi Liao, Xiaomeng Zhao, Xuefeng Hu, Wenli Zhu, and Zhaofeng Zhang. 2019. "Association between Diabetes and Cognitive Function among People over 45 Years Old in China: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 7: 1294. https://doi.org/10.3390/ijerph16071294
APA StyleZhang, L., Yang, J., Liao, Z., Zhao, X., Hu, X., Zhu, W., & Zhang, Z. (2019). Association between Diabetes and Cognitive Function among People over 45 Years Old in China: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 16(7), 1294. https://doi.org/10.3390/ijerph16071294