Beyond Broadway: Analysis of Qualitative Characteristics of and Individual Responses to Creatively Able, a Music and Movement Intervention for Children with Autism

 , ,
, ,
Abstract
:1. Introduction
1.1. Physical Activity in Children with Autism
1.2. Physical Activity or Movement Interventions: Considering Contextual and Qualitative Factors
1.3. Music Interventions for Children with Autism
1.4. Creatively Able: A Music and Movement Intervention for Children with ASD
2. Materials and Methods
2.1. Recruitment and Participants
2.2. Creatively Able Pilot Intervention
2.3. Assessment of Intervention Sessions: Qualitative Features and Individual Engagement
2.4. Assessment of Individual Outcomes
2.5. Statistical Analysis of Individual Outcomes
3. Results
3.1. Study 1
3.2. Study 2
3.2.1. Feasibility of Recruitment and Implementation
3.2.2. Self-Reported Enjoyment
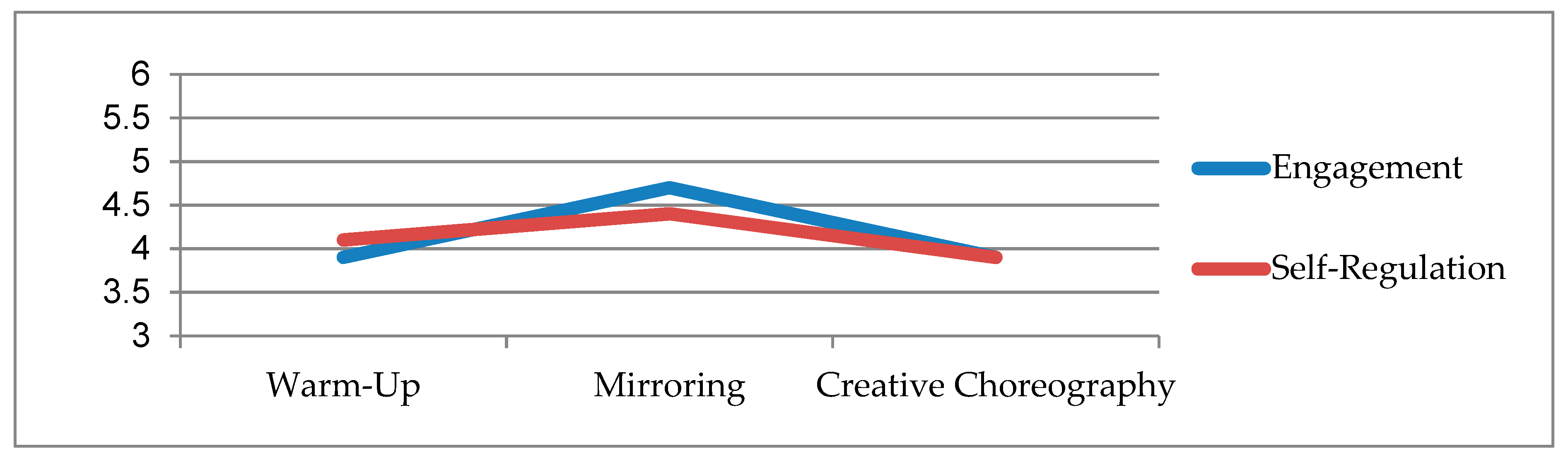
3.2.3. Participant Engagement and Self-Regulation during Intervention Sessions
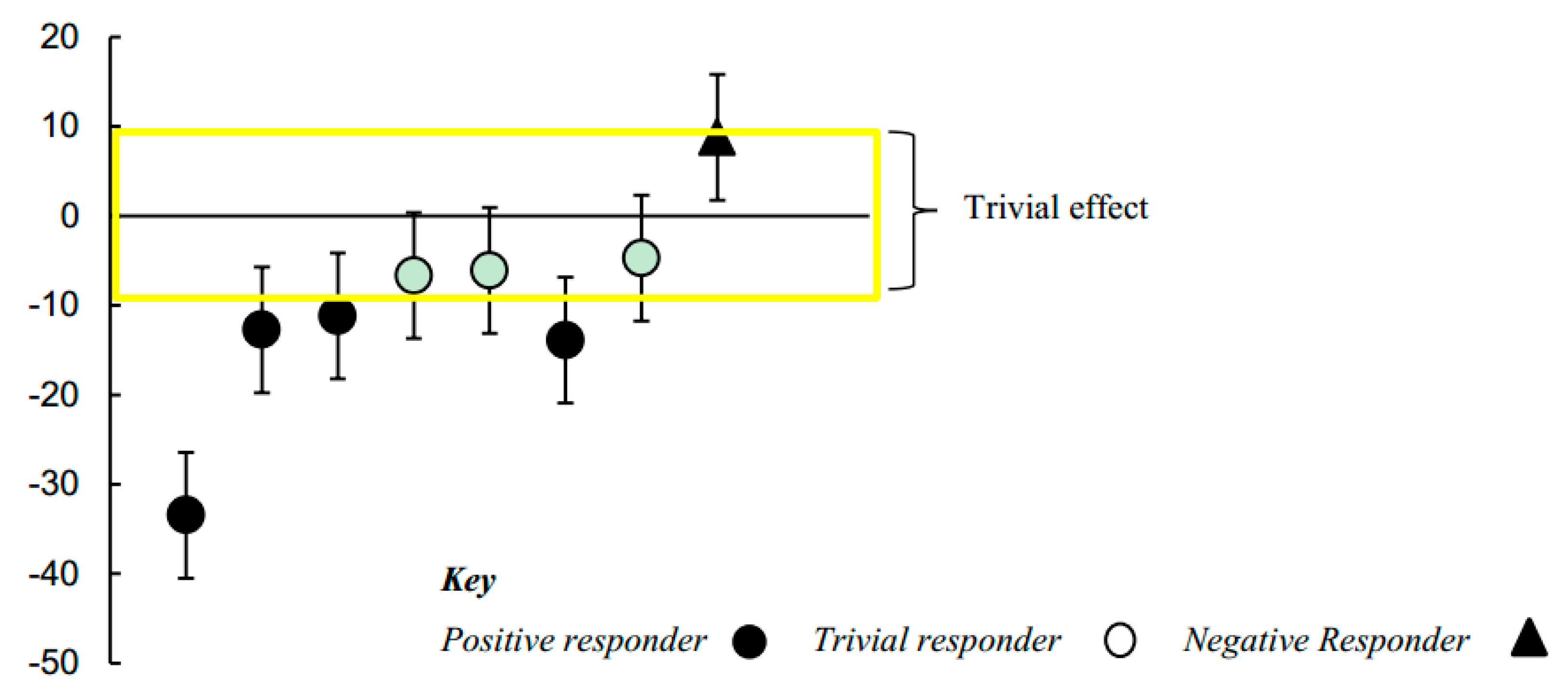
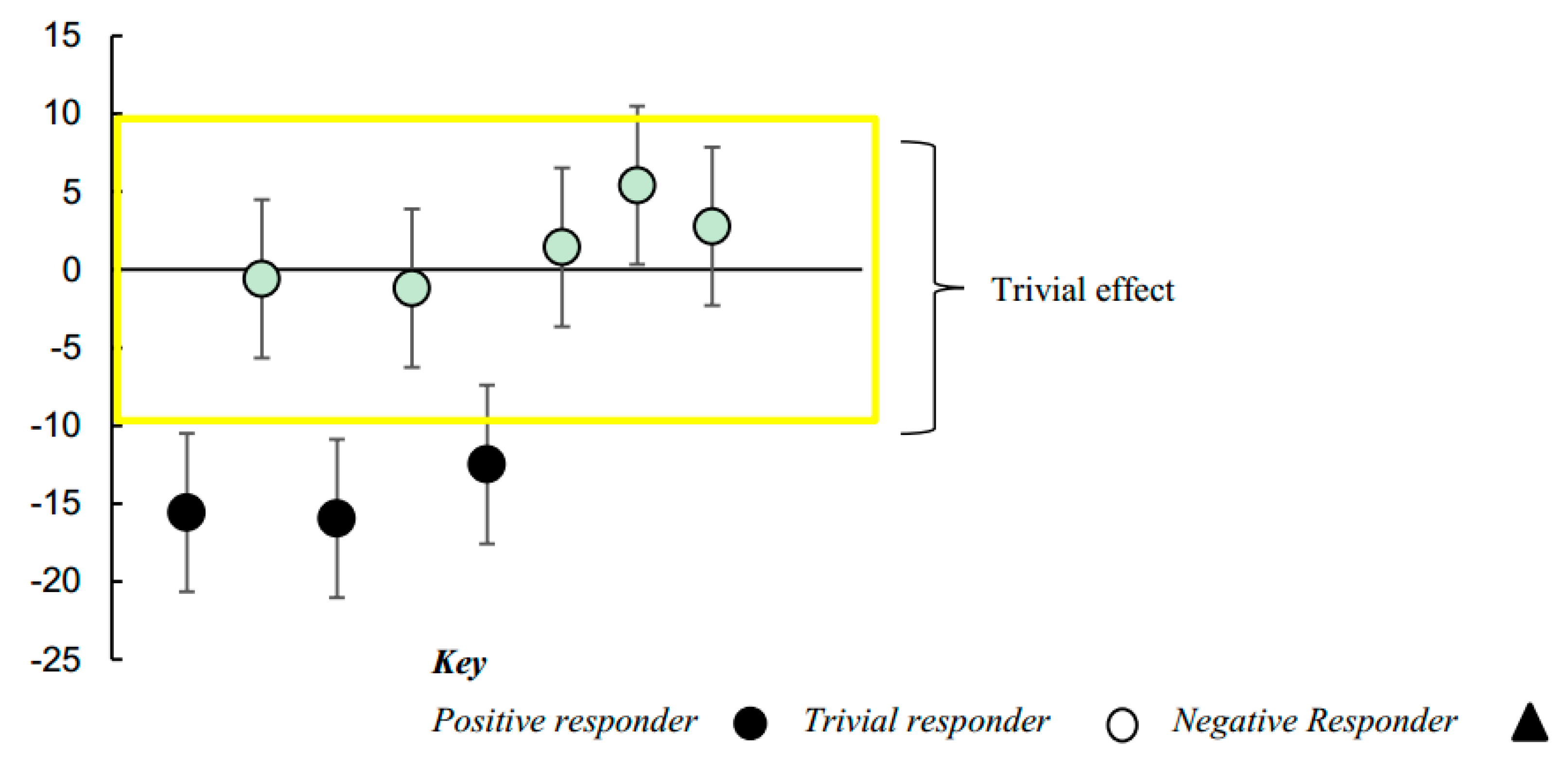
3.2.4. Improvements in Clinical Symptoms: Individual Responses to Intervention
4. Discussion
4.1. Creatively Able: A Music and Movement Intervention for Children with ASD
4.2. Studying Qualitative or Contextual Features of Physically Active Interventions
4.3. Studying Individual Responses to Intervention
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Press: Washington, DC, USA, 2013. [Google Scholar]
- U.S. Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Healthy People 2020; U.S. Department of Health and Human Services: Washington, DC, USA, 1953. Available online: http://www.healthypeople.gov/2020 (accessed on 15 April 2019).
- Rimmer, J.A.; Rowland, J.L. Physical activity for youth with disabilities: A critical need in an underserved population. Dev. Neurorehabilit. 2008, 11, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, J.H.; Yamaki, K.; Lowry, B.M.D.; Wang, E.; Vogel, L.C. Obesity and obesity-related secondary conditions in adolescents with intellectual/ developmental disabilities. J. Intellect. Disabil. Res. 2010, 54, 787–794. [Google Scholar] [CrossRef]
- Must, A.; Phillips, S.M.; Curtin, C.; Anderson, S.E.; Maslin, M.; Lividini, K.; Bandini, L.G. Comparison of sedentary behaviors between children with autism spectrum disorders and typically developing children. Autism 2013, 18, 376–384. [Google Scholar] [CrossRef] [Green Version]
- Must, A.; Phillips, S.; Curtin, C.; Bandini, L.G. Barriers to physical activity in children with autism spectrum disorders: Relationship to physical activity and screen time. J. Phys. Act. Health 2015, 12, 529–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njelesani, J.; Leckie, K.; Drummond, J.; Cameron, D. Parental perceptions of barriers to physical activity in children with developmental disabilities living in Trinidad and Tobago. Disabil. Rehabil. 2015, 37, 290–295. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Story, M.; Hannan, P.J.; Tharp, T.; Rex, J. Factors associated with changes in physical activity: A cohort study of inactive adolescent girls. Arch. Pediatr. Adolesc. Med. 2003, 157, 803–810. [Google Scholar] [CrossRef]
- MacDonald, M.; Esposito, P.; Ulrich, D. The physical activity patterns of children with autism. BMC Res. Notes 2011, 4, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Hanson, E.; Kalish, L.A.; Bunce, E.; Curtis, C.; McDaniel, S.; Ware, J.; Petry, J. Use of complementary and alternative medicine among children diagnosed with autism spectrum disorder. J. Autism Dev. Disord. 2007, 37, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Lofthouse, N.; Hendren, R.; Hurt, E.; Arnold, L.E.; Butter, E. A review of complementary and alternative treatments for autism spectrum disorders. Autism Res. Treat. 2012, 2012, 21. [Google Scholar] [CrossRef] [PubMed]
- De Greeff, J.W.; Bosker, R.J.; Oosterlaan, J.; Visscher, C.; Hartman, E. Effects of physical activity on executive functions, attention and academic performance in preadolescent children: A meta-analysis. J. Sci. Med. Sport 2018, 21, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Gunnell, K.E.; Poitras, V.J.; LeBlanc, A.; Schibli, K.; Barbeau, K.; Hedayati, N.; Ponitfex, M.B.; Goldfield, G.S.; Dunlap, C.; Tremblay, M.S.; et al. Physical activity and brain structure, brain function, and cognition in children and youth: A systematic review of randomized controlled trials. Ment. Health Phys. Act. 2018. [Google Scholar] [CrossRef]
- Best, J.R. Effects of physical activity on children’s executive function: Contributions of experimental research on aerobic exercise. Dev. Rev. 2010, 30, 331–351. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A.; Ling, D.S. Conclusions about interventions, programs, and approaches for improving executive functions that appear justified and those that, despite much hype, do not. Dev. Cogn. Neurosci. 2016, 18, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Pesce, C. Shifting the focus from quantitative to qualitative exercise characteristics in exercise and cognition research. J. Sport Exerc. Psychol. 2012, 34, 766–786. [Google Scholar] [CrossRef] [PubMed]
- Pesce, C.; Ben-Soussan, T.D. ‘Cogito ergo sum’ or ‘ambulo ergo sum’? New developmental perspectives in exercise and cognition research. In Exercise-Cognition Interaction: Neuroscience Perspectives; McMorris, T., Ed.; Elsevier: London, UK, 2016. [Google Scholar]
- Tomporowski, P.D.; McCullick, B.; Pendleton, D.M.; Pesce, C. Exercise and children’s cognition: The role of exercise characteristics and a place for metacognition. J. Sport Health Sci. 2015, 4, 47–55. [Google Scholar] [CrossRef]
- Vazou, S.; Pesce, C.; Lakes, K.; Smiley-Oyen, A. More than one road leads to Rome: A narrative review and meta-analysis of physical activity intervention effects on children’s cognition. Int. J. Sport Exerc. Psychol. 2016. [Google Scholar] [CrossRef]
- Diamond, A. Effects of physical exercise on executive functions: Going beyond simply moving to moving with thought. Ann. Sports Med. Res. 2015, 2, 1011. [Google Scholar] [PubMed]
- Bhide, A.; Power, A.; Goswami, U. A rhythmic musical intervention for poor readers: A comparison of efficacy with a letter-based intervention. Mind Brain Educ. 2013, 7, 113–123. [Google Scholar] [CrossRef]
- Linardakis, M.; Trouli, K.; Chlapana, E. Effects of a Rhythm Development Intervention on the Phonological Awareness in Early Childhood. In Proceedings of the International Economics Development and Research, Washington, DC, USA, 14–16 April 2013; Volume 78. [Google Scholar]
- Diamond, A. Want to optimize executive functions and academic outcomes? Simple, just nourish the human spirit. Minn. Symp. Child Psychol. 2014, 37, 203–230. [Google Scholar] [CrossRef]
- Heaton, P.; Hermelin, B.; Pring, L. Can children with autistic spectrum disorders percieve affect in music? An experimental investigation. Psychol. Med. 1999, 29, 1405–1410. [Google Scholar] [CrossRef]
- Quintin, E.M.; Bhatara, A.; Poissant, H.; Fombonne, E.; Levitin, D.J. Emotion perception in music in high-functioning adolescents with Autism Spectrum Disorders. J. Autism Dev. Disord. 2011, 41, 1240–1255. [Google Scholar] [CrossRef] [PubMed]
- Hillier, A.; Kopec, J.; Poto, N.; Tivarus, M.; Beversdorf, D.Q. Increased physiological responsiveness to preferred music among young adults with autism spectrum disorders. Psychol. Music 2015, 44, 481–492. [Google Scholar] [CrossRef]
- Allen, R.; Davis, R.; Hill, E. The effects of autism and alexithymia on physiological and verbal responsiveness to music. J. Autism Dev. Disord. 2013, 43, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Bhat, A.N.; Srinivasan, S. A review of “music and movement” therapies for children with autism: Embodied interventions for multisystem development. Front. Integr. Neurosci. 2013, 7, 22. [Google Scholar]
- Geretsegger, M.; Elefant, C.; Mossler, K.A.; Gold, C. Music therapy for people with autism spectrum disorder. Cochrane Database Syst. Rev. 2014, 6, Cd004381. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Wigram, T.; Gold, C. The Effects of Improvisational Music Therapy on Joint Attention Behaviors in Autistic Children: A Randomized Controlled study. J. Autism Dev. Disord. 2008, 38, 1758. [Google Scholar] [CrossRef] [PubMed]
- Cheever, T.; Taylor, A.; Finkelstein, R.; Edwards, E.; Thomas, L.; Bradt, J.; Holochwost, S.J.; Johnson, J.K.; Limb, C.; Tottenham, N.; et al. NIH/Kennedy Center Workshop on Music and the Brain: Finding Harmony. Neuron 2018, 97, 1214–1218. [Google Scholar] [CrossRef]
- Dawson, G. Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Dev. Psychopathol. 2008, 20, 775–803. [Google Scholar] [CrossRef]
- Wilson, M. Six views of embodied cognition. Psychon. Bull. Rev. 2002, 9, 625–636. [Google Scholar] [CrossRef] [Green Version]
- Bishop, D.V.; Norbury, C.F. Executive functions in children with communication impairments, in relation to autistic symptomatology: I: Generativity. Autism 2005, 9, 7–27. [Google Scholar] [CrossRef]
- Boyd, B.A.; McBee, M.; Holtzclaw, T.; Baranek, G.T.; Bodfish, J.W. Relationships among repetitive behaviors, sensory features, and executive functions in high functioning autism. Res. Autism Spectr. Disord. 2009, 3, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Lopez, B.R.; Lincoln, A.J.; Ozonoff, S.; Lai, Z. Examining the relationship between executive functions and restricted, repetitive symptoms of Autistic Disorder. J. Autism Dev. Disord. 2005, 35, 445–460. [Google Scholar] [CrossRef] [PubMed]
- Moscani, M.W.; Kay, M.; D’Cruz, A.M.; Seidenfeld, A. Impaired inhibitory control is associated with higher order repetitive behaviors in autism spectrum disorders. Psychol. Med. 2009, 39, 1559–1566. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive Function. Ann. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Reeve, J.; Jang, H.; Carrell, D.; Jeon, S.; Barch, J. Enhancing students’ engagement by increasing teachers’ autonomy support. Motiv. Emot. 2004, 28, 147–169. [Google Scholar] [CrossRef]
- Lakes, K.D. The Response to Challenge Scale (RCS): The development and construct validity of an observer-rated measure of children’s self-regulation. Int. J. Educ. Psychol. Assess. 2012, 10, 83–96. [Google Scholar]
- Lakes, K.D.; Hoyt, W.T. Applications of Generalizability Theory to clinical child and adolescent psychology research. J. Clin. Child Adolesc. Psychol. 2009, 38, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Bodfish, J.W.; Symons, F.J.; Parker, D.E.; Lewis, M.H. Varieties of repetitive behavior in autism: Comparisons to mental retardation. J. Autism Dev. Disord. 2000, 30, 237–243. [Google Scholar] [CrossRef]
- Kendzierski, D.; DeCarlo, K.J. Physical Activity Enjoyment Scale: Two validation studies. J. Sport Exerc. Psychol. 1991, 13, 50–64. [Google Scholar] [CrossRef]
- Hecksteden, A.; Kraushaar, J.; Scharhag-Rosenberger, F.; Theisen, D.; Senn, S.; Meyer, T. Individual response to exercise training-a statistical perspective. J. Appl. Physiol. 2015, 118, 1450–1459. [Google Scholar] [CrossRef]
- Hopkins, W.G. Individual responses made easy. J. Appl. Physiol. 2015, 118, 1444–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, W.G. Design and analysis of studies of individual responses. Sportscience 2018, 22, 39–51. [Google Scholar]
- Lam, K.S.L.; Aman, M.G. The Repetitive Behavior Scale-Revised: Independent validation in individuals with autism spectrum disorder. J. Autism Dev. Disord. 2007, 37, 855–866. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. How to obtain the P value from a confidence interval. BMJ Br. Med. J. 2011, 343. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Owen, K.B.; Parker, P.D.; Van Zanden, B.; MacMillan, F.; Astell-Burt, T.; Lonsdale, C. Physical activity and school engagement in youth: A systematic review and meta-analysis. Educ. Psychol. 2016, 51, 129–145. [Google Scholar] [CrossRef]
- Vazou, S.; Mischo, A.; Ladwig, M.A.; Ekkekakis, P.; Welk, G. Psychologically informed physical fitness practice in schools: A field experiment. Psychol. Sport Exerc. 2019, 40, 143–151. [Google Scholar] [CrossRef]
- Lubans, D.R.; Lonsdale, C.; Cohen, K.; Eather, N.; Beauchamp, M.R.; Morgan, P.J.; Sylvester, B.D.; Smith, J.J. Framework for the design and delivery of organized physical activity sessions for children and adolescents: Rationale and description of the ‘SAAFE’ teaching principles. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 24. [Google Scholar] [CrossRef]
- Brand, R.; Ekkekakis, P. Affective-reflective theory of physical inactivity and exercise: Foundations and preliminary evidence. Ger. J. Exerc. Sport Res. 2018, 48, 48–58. [Google Scholar] [CrossRef]
- Isen, A.M.; Reeve, J. The influence of positive affect on intrinsic and extrinsic motivation: Facilitating enjoyment of play, responsible work behavior, and self-control. Motiv. Emot. 2005, 29, 295–323. [Google Scholar] [CrossRef]
- Masi, A.; DeMayo, M.M.; Glozier, N.; Guastella, A.J. An Overview of Autism Spectrum Disorder, Heterogeneity and Treatment Options. Neurosci. Bull. 2017, 33, 183–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weitlauf, A.S.; McPheeters, M.L.; Peters, B.; Sathe, N.; Travis, R.; Aiello, R.; Warren, Z. Therapies for Children with Autism Spectrum Disorder: Behavioral Interventions Update; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Item | Disagree a Lot (%) | Disagree (%) | I Am Not Sure (%) | Agree (%) | Agree a Lot (%) |
|---|---|---|---|---|---|
| I enjoyed it | 0 | 0 | 14 | 29 | 57 |
| I found it fun | 0 | 14 | 0 | 29 | 57 |
| It was very pleasant | 0 | 14 | 29 | 29 | 29 |
| It gave me energy | 0 | 29 | 0 | 43 | 29 |
| My body feels good | 0 | 14 | 14 | 14 | 57 |
| It feels good | 0 | 0 | 0 | 43 | 57 |
| I got something out of it | 0 | 14 | 14 | 29 | 43 |
| It was very exciting | 0 | 14 | 0 | 14 | 71 |
| It gave me a strong feeling of success | 0 | 29 | 14 | 14 | 43 |
| I feel bored | 43 | 14 | 14 | 0 | 29 |
| I disliked it | 71 | 29 | 0 | 0 | 0 |
| It made me sad | 57 | 14 | 14 | 14 | 0 |
| It was not fun at all | 71 | 0 | 14 | 14 | 0 |
| It frustrated me | 71 | 0 | 0 | 29 | 0 |
| It was not at all interesting | 43 | 14 | 29 | 0 | 14 |
| I feel as though I would rather be doing something else | 43 | 14 | 29 | 14 | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakes, K.D.; Neville, R.; Vazou, S.; Schuck, S.E.B.; Stavropoulos, K.; Krishnan, K.; Gonzalez, I.; Guzman, K.; Tavakoulnia, A.; Stehli, A.; et al. Beyond Broadway: Analysis of Qualitative Characteristics of and Individual Responses to Creatively Able, a Music and Movement Intervention for Children with Autism. Int. J. Environ. Res. Public Health 2019, 16, 1377. https://doi.org/10.3390/ijerph16081377
Lakes KD, Neville R, Vazou S, Schuck SEB, Stavropoulos K, Krishnan K, Gonzalez I, Guzman K, Tavakoulnia A, Stehli A, et al. Beyond Broadway: Analysis of Qualitative Characteristics of and Individual Responses to Creatively Able, a Music and Movement Intervention for Children with Autism. International Journal of Environmental Research and Public Health. 2019; 16(8):1377. https://doi.org/10.3390/ijerph16081377
Chicago/Turabian StyleLakes, Kimberley D., Ross Neville, Spyridoula Vazou, Sabrina E. B. Schuck, Katherine Stavropoulos, Kavita Krishnan, Irene Gonzalez, Kayla Guzman, Arya Tavakoulnia, Annamarie Stehli, and et al. 2019. "Beyond Broadway: Analysis of Qualitative Characteristics of and Individual Responses to Creatively Able, a Music and Movement Intervention for Children with Autism" International Journal of Environmental Research and Public Health 16, no. 8: 1377. https://doi.org/10.3390/ijerph16081377
APA StyleLakes, K. D., Neville, R., Vazou, S., Schuck, S. E. B., Stavropoulos, K., Krishnan, K., Gonzalez, I., Guzman, K., Tavakoulnia, A., Stehli, A., & Palermo, A. (2019). Beyond Broadway: Analysis of Qualitative Characteristics of and Individual Responses to Creatively Able, a Music and Movement Intervention for Children with Autism. International Journal of Environmental Research and Public Health, 16(8), 1377. https://doi.org/10.3390/ijerph16081377