A Cognitive Reserve and Social Support-Focused Latent Class Analysis to Predict Self-Reported Confusion or Memory Loss among Middle-Aged World Trade Center Health Registry Enrollees

Abstract
:1. Introduction
2. Materials and Methods
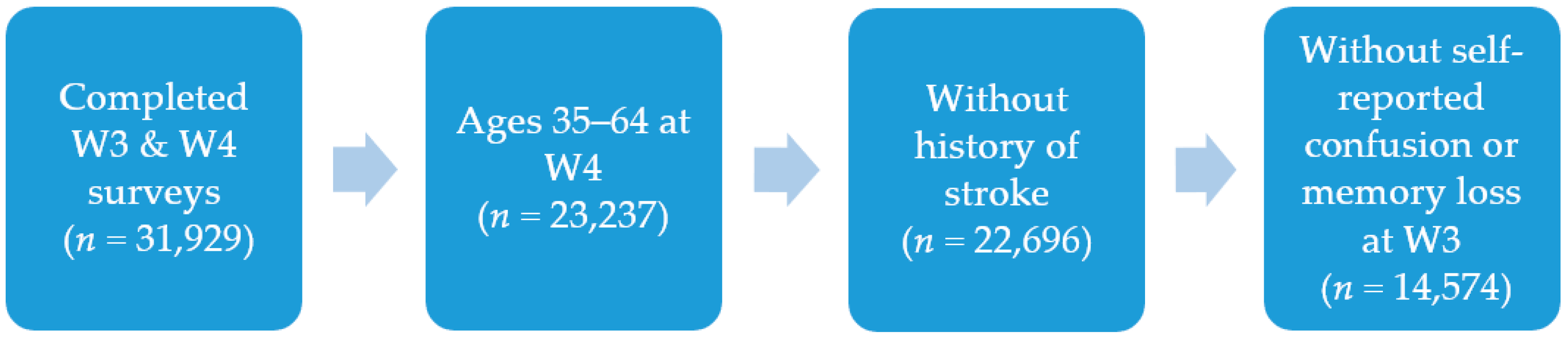
2.1. Study Population and Sample
2.2. Study Variables
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brackbill, R.M.; Hadler, J.L.; DiGrande, L.; Ekenga, C.C.; Farfel, M.R.; Friedman, S.; Perlman, S.E.; Stellman, S.D.; Walker, D.J.; Wu, D.; et al. Asthma and posttraumatic stress symptoms 5 to 6 years following exposure to the World Trade Center terrorist attack. JAMA 2009, 302, 502–516. [Google Scholar] [CrossRef]
- Li, J.; Brackbill, R.M.; Jordan, H.T.; Cone, J.E.; Farfel, M.R.; Stellman, S.D. Effect of asthma and PTSD on persistence and onset of gastroesophageal reflux symptoms among adults exposed to the 11 September 2001, terrorist attacks. Am. J. Ind. Med. 2016, 59, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Solan, S.; Wallenstein, S.; Shapiro, M.; Teitelbaum, S.L.; Stevenson, L.; Kochman, A.; Kaplan, J.; Dellenbaugh, C.; Kahn, A.; Biro, F.N.; et al. Cancer incidence in world trade center rescue and recovery workers, 2001–2008. Environ. Health Perspect. 2013, 121, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.; Bouldin, E.D.; McGuire, L.C. Subjective Cognitive Decline Among Adults Aged >/=45 Years—United States, 2015–2016. Morb. Mortal. Wkly. Rep. 2018, 67, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Langa, K.M.; Larson, E.B.; Karlawish, J.H.; Cutler, D.M.; Kabeto, M.U.; Kim, S.Y.; Rosen, A.B. Trends in the prevalence and mortality of cognitive impairment in the United States: Is there evidence of a compression of cognitive morbidity? Alzheimers Dement. J. Alzheimers Assoc. 2008, 4, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Ainamani, H.E.; Elbert, T.; Olema, D.K.; Hecker, T. PTSD symptom severity relates to cognitive and psycho-social dysfunctioning—A study with Congolese refugees in Uganda. Eur. J. Psychotraumatol. 2017, 8, 1283086. [Google Scholar] [CrossRef] [PubMed]
- Clausen, A.N.; Francisco, A.J.; Thelen, J.; Bruce, J.; Martin, L.E.; McDowd, J.; Simmons, W.K.; Aupperle, R.L. PTSD and cognitive symptoms relate to inhibition-related prefrontal activation and functional connectivity. Depress. Anxiety 2017, 34, 427–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumner, J.A.; Hagan, K.; Grodstein, F.; Roberts, A.L.; Harel, B.; Koenen, K.C. Posttraumatic stress disorder symptoms and cognitive function in a large cohort of middle-aged women. Depress. Anxiety 2017, 34, 356–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasterling, J.J.; Brailey, K.; Constans, J.I.; Sutker, P.B. Attention and memory dysfunction in posttraumatic stress disorder. Neuropsychology 1998, 12, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Vittinghoff, E.; Lindquist, K.; Barnes, D.; Covinsky, K.E.; Neylan, T.; Kluse, M.; Marmar, C. Posttraumatic stress disorder and risk of dementia among US veterans. Arch. Gen. Psychiatry 2010, 67, 608–613. [Google Scholar] [CrossRef]
- Clouston, S.; Pietrzak, R.H.; Kotov, R.; Richards, M.; Spiro, A., 3rd; Scott, S.; Deri, Y.; Mukherjee, S.; Stewart, C.; Bromet, E.; et al. Traumatic exposures, posttraumatic stress disorder, and cognitive functioning in World Trade Center responders. Alzheimers Dement. (N. Y.) 2017, 3, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Brandes, D.; Ben-Schachar, G.; Gilboa, A.; Bonne, O.; Freedman, S.; Shalev, A.Y. PTSD symptoms and cognitive performance in recent trauma survivors. Psychiatry Res. 2002, 110, 231–238. [Google Scholar] [CrossRef]
- Ranft, U.; Schikowski, T.; Sugiri, D.; Krutmann, J.; Kramer, U. Long-term exposure to traffic-related particulate matter impairs cognitive function in the elderly. Environ. Res. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.; Kotov, R.; Pietrzak, R.H.; Luft, B.J.; Gonzalez, A.; Richards, M.; Ruggero, C.J.; Spiro, A., 3rd; Bromet, E.J. Cognitive impairment among World Trade Center responders: Long-term implications of re-experiencing the 9/11 terrorist attacks. Alzheimers Dement. (Amst. Neth.) 2016, 4, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Evans, I.E.M.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social Isolation and Cognitive Function in Later Life: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2018, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Evans, I.E.M.; Llewellyn, D.J.; Matthews, F.E.; Woods, R.T.; Brayne, C.; Clare, L. Social isolation, cognitive reserve, and cognition in healthy older people. PLoS ONE 2018, 13, e0201008. [Google Scholar] [CrossRef] [PubMed]
- Ishiki, A.; Okinaga, S.; Tomita, N.; Kawahara, R.; Tsuji, I.; Nagatomi, R.; Taki, Y.; Takahashi, T.; Kuzuya, M.; Morimoto, S.; et al. Changes in Cognitive Functions in the Elderly Living in Temporary Housing after the Great East Japan Earthquake. PLoS ONE 2016, 11, e0147025. [Google Scholar] [CrossRef]
- Lee, H.; Waite, L.J. Cognition in Context: The Role of Objective and Subjective Measures of Neighborhood and Household in Cognitive Functioning in Later Life. Gerontologist 2018, 58, 159–169. [Google Scholar] [CrossRef]
- Yates, J.A.; Clare, L.; Woods, R.T. “You’ve got a friend in me”: Can social networks mediate the relationship between mood and MCI? BMC Geriatr. 2017, 17, 144. [Google Scholar] [CrossRef] [PubMed]
- Malek-Ahmadi, M.; Lu, S.; Chan, Y.; Perez, S.E.; Chen, K.; Mufson, E.J. Static and Dynamic Cognitive Reserve Proxy Measures: Interactions with Alzheimer’s Disease Neuropathology and Cognition. J. Alzheimers Dis. Parkinsonism 2017, 7, 390. [Google Scholar]
- Dodich, A.; Carli, G.; Cerami, C.; Iannaccone, S.; Magnani, G.; Perani, D. Social and cognitive control skills in long-life occupation activities modulate the brain reserve in the behavioural variant of frontotemporal dementia. Cortex J. Devot. Study Nerv. Syst. Behav. 2018, 99, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.L.; Sajjad, A.; Bramer, W.M.; Ikram, M.A.; Tiemeier, H.; Stephan, B.C. Exploring strategies to operationalize cognitive reserve: A systematic review of reviews. J. Clin. Exp. Neuropsychol. 2015, 37, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Opdebeeck, C.; Martyr, A.; Clare, L. Cognitive reserve and cognitive function in healthy older people: A meta-analysis. Neuropsychol. Dev. Cogn. Sect. B Aging Neuropsychol. Cogn. 2016, 23, 40–60. [Google Scholar] [CrossRef] [PubMed]
- Robitaille, A.; van den Hout, A.; Machado, R.J.M.; Bennett, D.A.; Cukic, I.; Deary, I.J.; Hofer, S.M.; Hoogendijk, E.O.; Huisman, M.; Johansson, B.; et al. Transitions across cognitive states and death among older adults in relation to education: A multistate survival model using data from six longitudinal studies. Alzheimers Dement. J. Alzheimers Assoc. 2018, 14, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Reuser, M.; Willekens, F.J.; Bonneux, L. Higher education delays and shortens cognitive impairment: A multistate life table analysis of the US Health and Retirement Study. Eur. J. Epidemiol. 2011, 26, 395–403. [Google Scholar] [CrossRef]
- Bento-Torres, N.V.; Bento-Torres, J.; Tomas, A.M.; Costa, V.O.; Correa, P.G.; Costa, C.N.; Jardim, N.Y.; Picanco-Diniz, C.W. Influence of schooling and age on cognitive performance in healthy older adults. Braz. J. Med. Biol. Res. Rev. Bras. Pesqui. Med. Biol. 2017, 50, e5892. [Google Scholar] [CrossRef] [PubMed]
- Frankenmolen, N.L.; Fasotti, L.; Kessels, R.P.C.; Oosterman, J.M. The influence of cognitive reserve and age on the use of memory strategies. Exp. Aging Res. 2018, 44, 117–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Park, H.; Chey, J. Education as a Protective Factor Moderating the Effect of Depression on Memory Impairment in Elderly Women. Psychiatry Investig. 2018, 15, 70–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fratiglioni, L.; Wang, H.X. Brain reserve hypothesis in dementia. J. Alzheimers Dis. 2007, 12, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive reserve and Alzheimer disease. Alzheimers Dis. Assoc. Disord. 2006, 20, 112–117. [Google Scholar] [CrossRef]
- Stern, Y.; Tang, M.X.; Denaro, J.; Mayeux, R. Increased risk of mortality in Alzheimer’s disease patients with more advanced educational and occupational attainment. Ann. Neurol. 1995, 37, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD Checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Lanza, S.T.; Collins, L.M.; Lemmon, D.R.; Schafer, J.L. PROC LCA: A SAS Procedure for Latent Class Analysis. Struct. Equ. Model. Multidiscip. J. 2007, 14, 671–694. [Google Scholar] [CrossRef]
- Lanza, S.T.; Dziak, J.J.; Huang, L.; Wagner, A.; Collins, L.M. Proc LCA & Proc LTA Users’ Guide (Version 1.3.2); The Methodology Center, Penn State: University Park, TX, USA, 2015; Available online: methodology.psu.edu (accessed on 22 October 2018).
- Berglund, P.A. Latent Class Analysis Using Proc LCA: Paper 5500-2016. 2016. Available online: https://support.sas.com/resources/papers/proceedings16/5500-2016.pdf (accessed on 22 October 2018).
- McNutt, L.A.; Wu, C.; Xue, X.; Hafner, J.P. Estimating the relative risk in cohort studies and clinical trials of common outcomes. Am. J. Epidemiol. 2003, 157, 940–943. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, A.; Kotozaki, Y.; Sugiura, M.; Nouchi, R.; Takeuchi, H.; Hanawa, S.; Nakagawa, S.; Miyauchi, C.M.; Araki, T.; Sakuma, A.; et al. Long-term effects of postearthquake distress on brain microstructural changes. BioMed Res. Int. 2014, 2014, 180468. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, L.; Sandblom, J.; Jones, S.; Neely, A.S.; Petersson, K.M.; Ingvar, M.; Backman, L. Neural correlates of training-related memory improvement in adulthood and aging. Proc. Natl. Acad. Sci. USA 2003, 100, 13728–13733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speer, M.E.; Soldan, A. Cognitive reserve modulates ERPs associated with verbal working memory in healthy younger and older adults. Neurobiol. Aging 2015, 36, 1424–1434. [Google Scholar] [CrossRef] [PubMed]
- Steffener, J.; Reuben, A.; Rakitin, B.C.; Stern, Y. Supporting performance in the face of age-related neural changes: Testing mechanistic roles of cognitive reserve. Brain Imaging Behav. 2011, 5, 212–221. [Google Scholar] [CrossRef]
- Lopez-Higes, R.; Martin-Aragoneses, M.T.; Rubio-Valdehita, S.; Delgado-Losada, M.L.; Montejo, P.; Montenegro, M.; Prados, J.M.; de Frutos-Lucas, J.; Lopez-Sanz, D. Efficacy of Cognitive Training in Older Adults with and without Subjective Cognitive Decline Is Associated with Inhibition Efficiency and Working Memory Span, Not with Cognitive Reserve. Front. Aging Neurosci. 2018, 10, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muir, S.W.; Gopaul, K.; Montero Odasso, M.M. The role of cognitive impairment in fall risk among older adults: A systematic review and meta-analysis. Age Ageing 2012, 41, 299–308. [Google Scholar] [CrossRef]
- De Bruijn, R.F.; Akoudad, S.; Cremers, L.G.; Hofman, A.; Niessen, W.J.; van der Lugt, A.; Koudstaal, P.J.; Vernooij, M.W.; Ikram, M.A. Determinants, MRI correlates, and prognosis of mild cognitive impairment: The Rotterdam Study. J. Alzheimers Dis. 2014, 42 (Suppl. 3), S239–S249. [Google Scholar] [CrossRef]
- Ganguli, M. Depression, cognitive impairment and dementia: Why should clinicians care about the web of causation? Indian J. Psychiatry 2009, 51 (Suppl. 1), S29–S34. [Google Scholar]
- Caselli, R.J.; Chen, K.; Locke, D.E.; Lee, W.; Roontiva, A.; Bandy, D.; Fleisher, A.S.; Reiman, E.M. Subjective cognitive decline: Self and informant comparisons. Alzheimers Dement. J. Alzheimers Assoc. 2014, 10, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, J.D.; Scult, M.A.; Caspi, A.; Arseneault, L.; Belsky, D.W.; Hariri, A.R.; Harrington, H.; Houts, R.; Ramrakha, S.; Poulton, R.; et al. Is low cognitive functioning a predictor or consequence of major depressive disorder? A test in two longitudinal birth cohorts. Dev. Psychopathol. 2017, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatto, N.M.; Henderson, V.W.; Hodis, H.N.; St John, J.A.; Lurmann, F.; Chen, J.C.; Mack, W.J. Components of air pollution and cognitive function in middle-aged and older adults in Los Angeles. Neurotoxicology 2014, 40, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lioy, P.J.; Weisel, C.P.; Millette, J.R.; Eisenreich, S.; Vallero, D.; Offenberg, J.; Buckley, B.; Turpin, B.; Zhong, M.; Cohen, M.D.; et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ. Health Perspect. 2002, 110, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Self-reported increased confusion or memory loss and associated functional difficulties among adults aged >/= 60 years—21 States, 2011. Morb. Mortal. Wkly. Rep. 2013, 62, 347–350. [Google Scholar]
- Farias, S.T.; Mungas, D.; Jagust, W. Degree of discrepancy between self and other-reported everyday functioning by cognitive status: Dementia, mild cognitive impairment, and healthy elders. Int. J. Geriatr. Psychiatry 2005, 20, 827–834. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample Characteristics | Total Study Sample (n = 14,574) 1,2 n (%) | Confusion or Memory Loss at W4 (n = 3262, 22%) 1,2 n (%) | No Confusion or Memory Loss at W4 (n = 11,312, 78%) 1,2 n (%) |
|---|---|---|---|
| Probable PTSD | |||
| Yes | 1213 (8.3%) | 550 (16.7%) | 663 (5.9%) |
| No | 13,252 (90.9%) | 2675 (82.0%) | 10,577 (93.5%) |
| Gender | |||
| Male | 8975 (61.6%) | 2016 (61.8%) | 6959 (61.5%) |
| Female | 5599 (38.4%) | 1246 (38.2%) | 4353 (38.5%) |
| Age group | |||
| 35–44 years | 2827 (19.4%) | 570 (17.5%) | 2257 (20.0%) |
| 45–54 years | 5526 (37.9%) | 1277 (39.2%) | 4249 (37.6%) |
| 55–64 years | 6221 (42.7%) | 1415 (43.4%) | 4806 (42.5%) |
| Educational attainment | |||
| Bachelor’s degree or more | 8693 (59.7%) | 1666 (51.1%) | 7027 (62.1%) |
| Less than a bachelor’s degree | 5820 (39.9%) | 1576 (48.3%) | 4244 (37.5%) |
| Marital status | |||
| Married or living with partner | 10,482 (71.9%) | 2269 (69.6%) | 8213 (72.6%) |
| Divorced/separated, widowed, or never married | 4033 (27.7%) | 979 (30.0%) | 3054 (27.0%) |
| Employment status | |||
| Currently employed | 12,193 (83.7%) | 2671 (81.9%) | 9522 (84.2%) |
| Not currently employed | 2335 (16.0%) | 579 (17.8%) | 1756 (15.5%) |
| Number of close friends | |||
| Have 3 or more close friends | 12,719 (87.3%) | 2720 (83.4%) | 9999 (88.4%) |
| Have 0–2 close friends | 1452 (10.0%) | 448 (13.7%) | 1004 (8.9%) |
| Communicate with friends | |||
| Visited/talked/emailed with friends at least twice in last 30 days | 13,681 (93.9%) | 2950 (90.4%) | 10,731 (94.9%) |
| Did not visit/talk/email with friends at least twice in last 30 days | 729 (5.0%) | 265 (8.1%) | 464 (4.1%) |
| People who understand your problems | |||
| Someone is available to understand your problems most or all of the time | 9952 (68.3%) | 1888 (57.9%) | 8064 (71.3%) |
| Someone is available to understand your problems none to some of the time | 4401 (30.2%) | 1311 (40.2%) | 3090 (27.3%) |
| Physical activity | |||
| Very or somewhat physically active in general | 11,413 (78.3%) | 2287 (70.1%) | 9126 (80.7%) |
| Not or not very physically active in general | 3096 (21.2%) | 951 (29.2%) | 2145 (19.0%) |
| Cognitive Reserve Indicators | Probable PTSD (n = 1,213) 1,2 | Not Probable PTSD (n = 13,252) 1,2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Class 1 (14.5%) | Class 2 (8.3%) | Class 3 (36.9%) | Class 4 (40.3%) | Class 1 (5.1%) | Class 2 (15.6%) | Class 3 (18.4%) | Class 4 (60.9%) | |
| Proportion in each latent class | ||||||||
| Bachelor’s degree or more | 0.345 | 0.050 | 0.588 | 0.504 | 0.331 | 0.183 | 0.673 | 0.725 |
| Married or living with partner | 0.572 | 0.665 | 0.466 | 0.797 | 0.772 | 0.817 | 0.445 | 0.792 |
| Currently employed | 0.747 | 0.080 | 0.768 | 0.809 | 0.778 | 0.697 | 0.850 | 0.895 |
| Have three or more close friends | 0.398 | 0.728 | 0.742 | 0.901 | 0.421 | 0.955 | 0.818 | 0.969 |
| Visited/talked/emailed with friends at least twice in last 30 days | 0.245 | 0.766 | 0.998 | 0.966 | 0.527 | 0.939 | 0.978 | 0.995 |
| Someone is available to understand your problems most or all of the time | 0.083 | 0.432 | 0.036 | 0.866 | 0.266 | 0.880 | 0.005 | 0.933 |
| Very or somewhat physically active in general | 0.491 | 0.255 | 0.662 | 0.730 | 0.627 | 0.724 | 0.725 | 0.859 |
| Sample Characteristics | Probable PTSD n = 1213 | Not Probable PTSD n = 13,252 | ||
|---|---|---|---|---|
| RR (95% CI) | p-Value | RR (95% CI) | p-Value | |
| Latent class | ||||
| Class 1: low cognitive reserve | 1.13 (0.90, 1.47) | 0.292 | 1.81 (1.55, 2.11) | <0.0001 |
| Class 2: medium-low cognitive reserve | 1.35 (1.08, 1.69) | 0.008 | 1.36 (1.21, 1.52) | <0.0001 |
| Class 3: medium-high cognitive reserve | 1.15 (0.98, 1.34) | 0.080 | 1.44 (1.33, 1.56) | <0.0001 |
| Class 4: high cognitive reserve | Referent | -- | Referent | -- |
| Gender | ||||
| Female | 0.84 (0.72, 0.97) | 0.017 | 0.93 (0.86, 1.00) | 0.055 |
| Male | Referent | -- | Referent | -- |
| Race/ethnicity | ||||
| White non-Hispanic | Referent | -- | Referent | -- |
| Black non-Hispanic | 1.06 (0.84, 1.34) | 0.609 | 1.16 (1.02, 1.31) | 0.020 |
| Hispanic | 1.09 (0.90, 1.32) | 0.376 | 1.06 (0.95, 1.20) | 0.304 |
| Other races | 0.89 (0.67, 1.20) | 0.451 | 1.19 (1.04, 1.35) | 0.010 |
| Health conditions | ||||
| History of depression | 1.15 (0.99, 1.33) | 0.074 | 1.26 (1.14, 1.39) | <0.0001 |
| History of anxiety | 1.01 (0.86, 1.18) | 0.908 | 1.13 (1.00, 1.27) | 0.050 |
| History of drug or alcohol use problems | 1.26 (1.03, 1.53) | 0.024 | 1.40 (1.20, 1.65) | <0.0001 |
| Smoking status | ||||
| Never smoker | Referent | -- | Referent | -- |
| Former smoker | 1.11 (0.95, 1.29) | 0.187 | 1.20 (1.11, 1.29) | <0.0001 |
| Current smoker | 1.16 (0.98, 1.38) | 0.087 | 1.18 (1.05, 1.33) | 0.005 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seil, K.; Yu, S.; Alper, H. A Cognitive Reserve and Social Support-Focused Latent Class Analysis to Predict Self-Reported Confusion or Memory Loss among Middle-Aged World Trade Center Health Registry Enrollees. Int. J. Environ. Res. Public Health 2019, 16, 1401. https://doi.org/10.3390/ijerph16081401
Seil K, Yu S, Alper H. A Cognitive Reserve and Social Support-Focused Latent Class Analysis to Predict Self-Reported Confusion or Memory Loss among Middle-Aged World Trade Center Health Registry Enrollees. International Journal of Environmental Research and Public Health. 2019; 16(8):1401. https://doi.org/10.3390/ijerph16081401
Chicago/Turabian StyleSeil, Kacie, Shengchao Yu, and Howard Alper. 2019. "A Cognitive Reserve and Social Support-Focused Latent Class Analysis to Predict Self-Reported Confusion or Memory Loss among Middle-Aged World Trade Center Health Registry Enrollees" International Journal of Environmental Research and Public Health 16, no. 8: 1401. https://doi.org/10.3390/ijerph16081401
APA StyleSeil, K., Yu, S., & Alper, H. (2019). A Cognitive Reserve and Social Support-Focused Latent Class Analysis to Predict Self-Reported Confusion or Memory Loss among Middle-Aged World Trade Center Health Registry Enrollees. International Journal of Environmental Research and Public Health, 16(8), 1401. https://doi.org/10.3390/ijerph16081401