Physical Fitness of School-Age Children after Cancer Treatment

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Research Methods
2.3. Ethics
2.4. Statistical Analysis
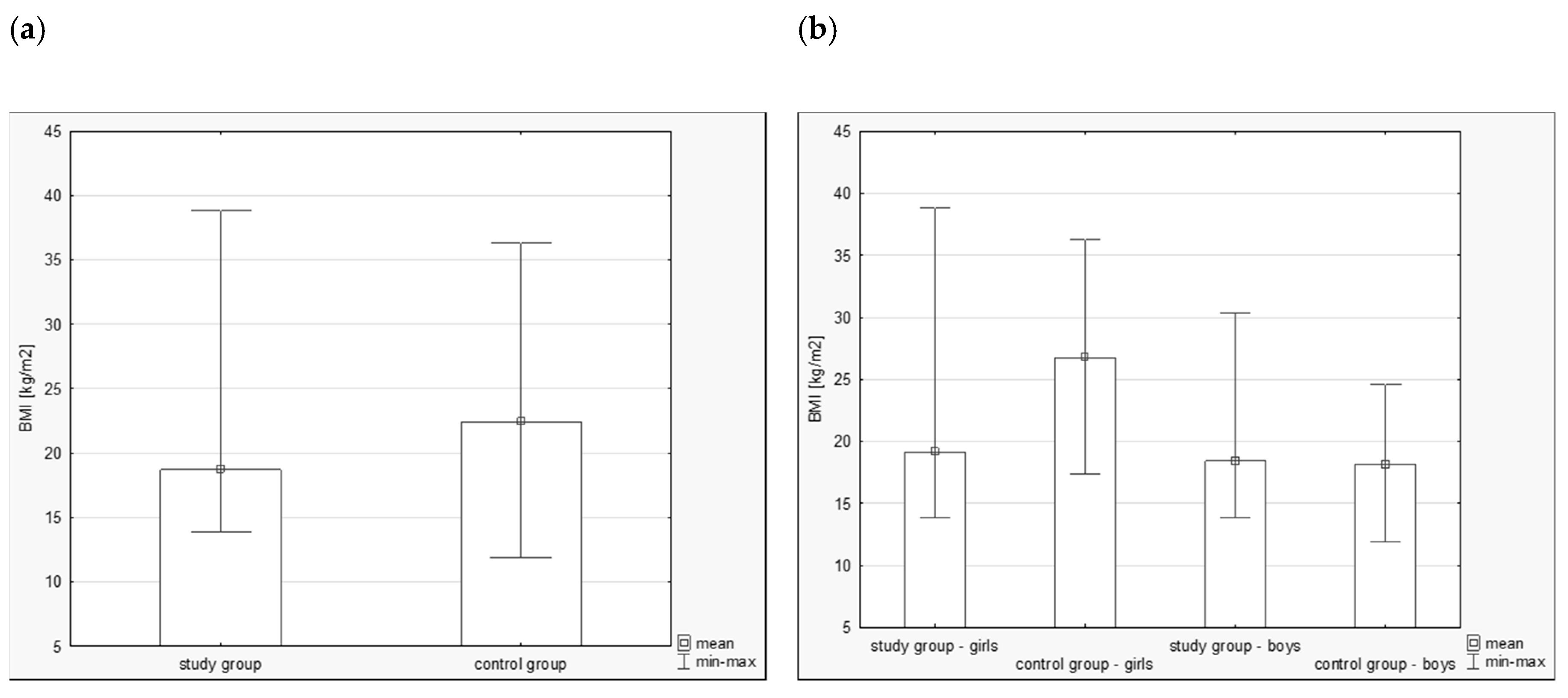
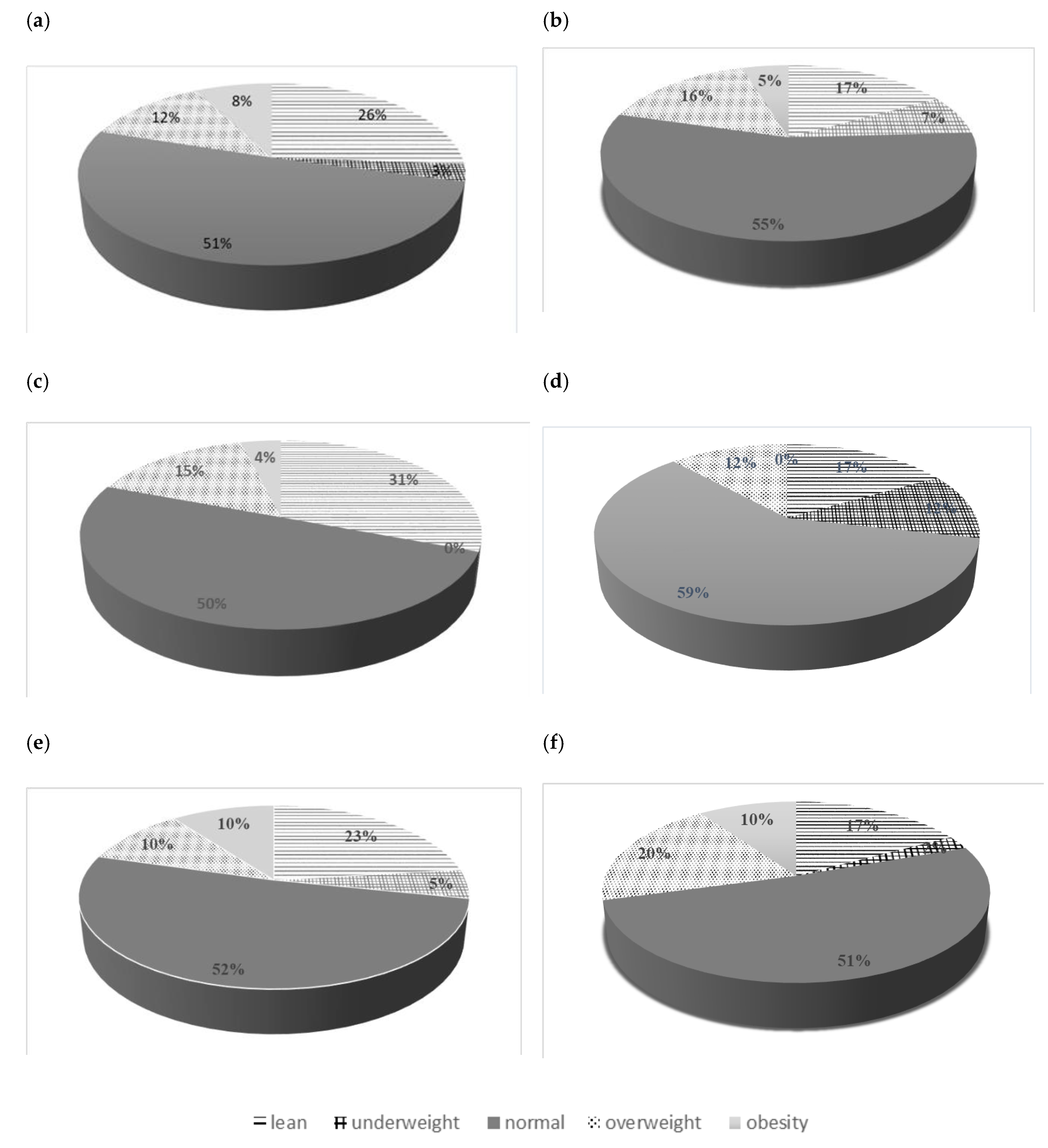
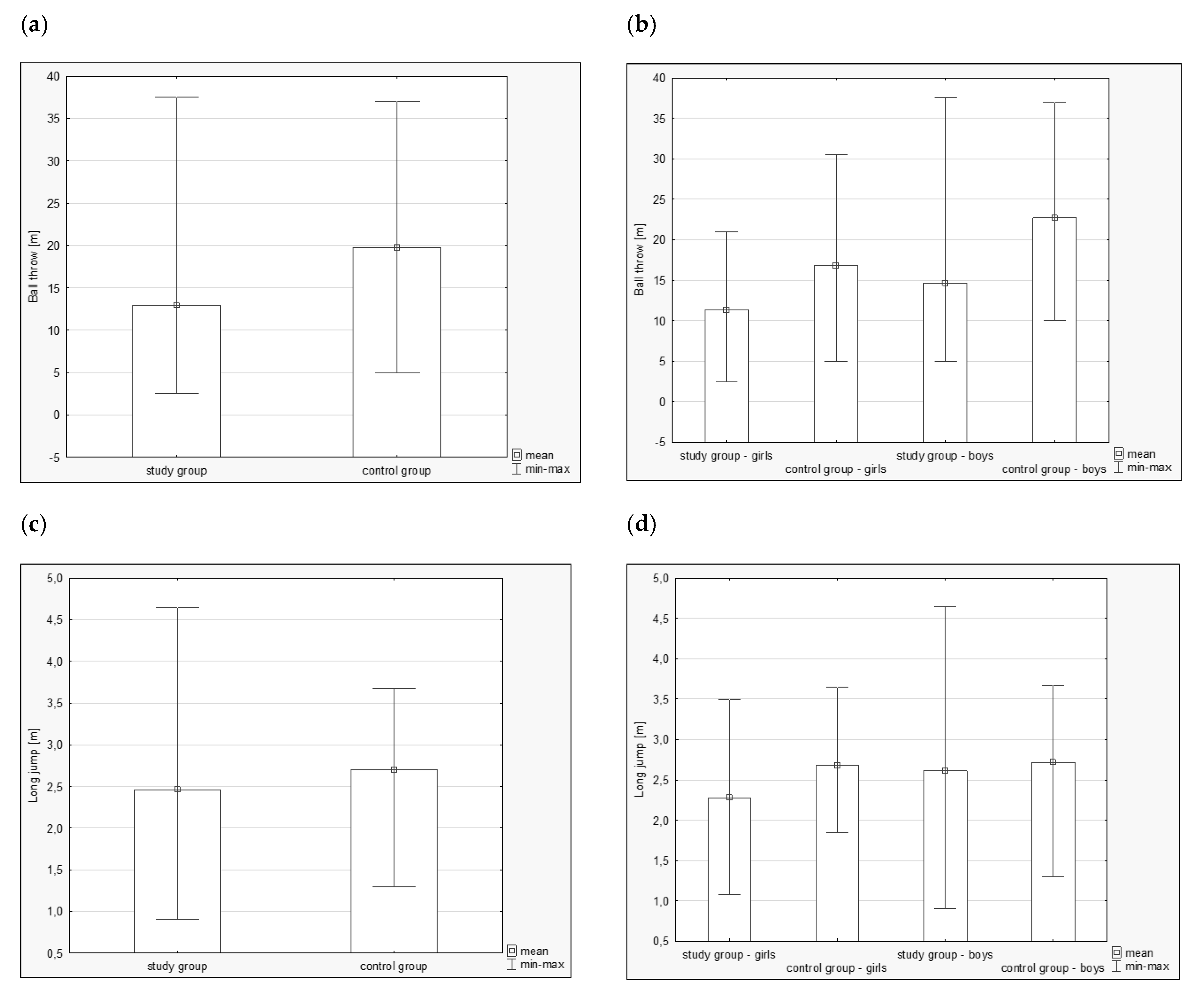
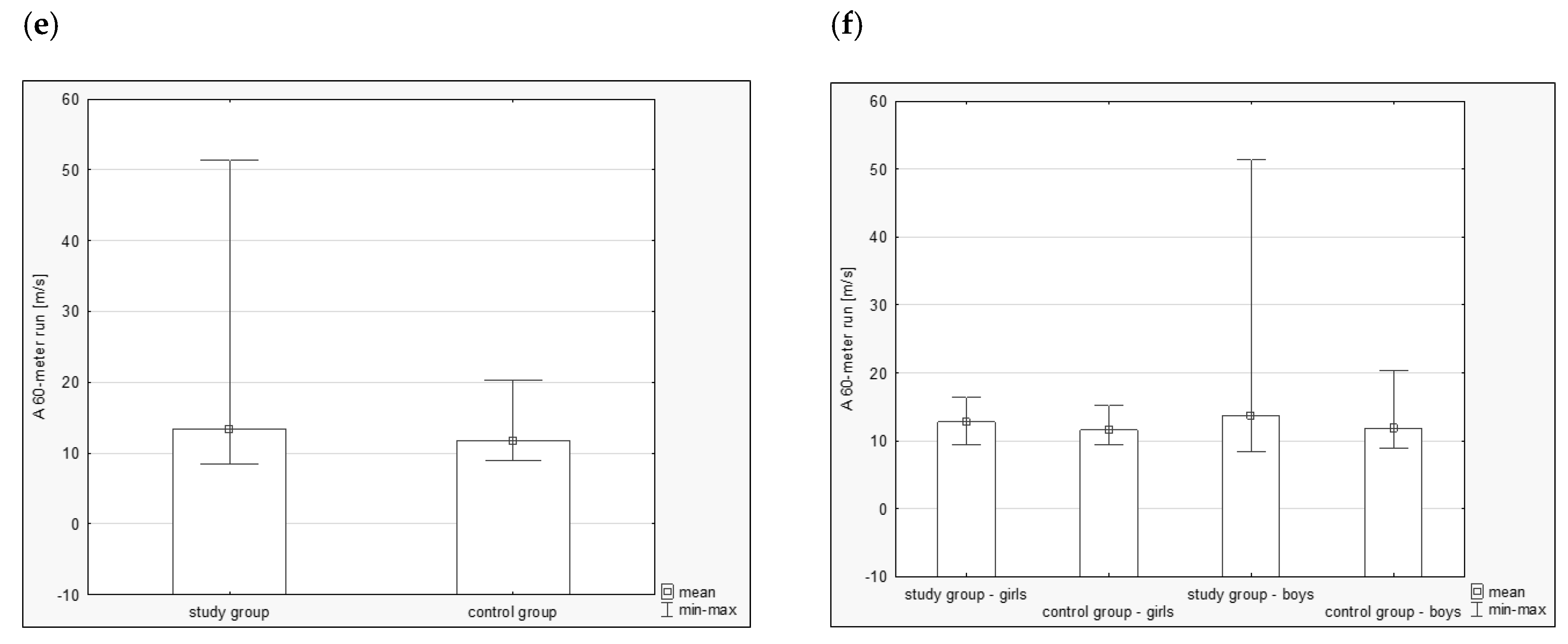
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rodriguez-Galindo, C.; Friedrich, P.; Alcasabas, P.; Antillon, F.; Banavali, S.; Castillo, L.; Quah, T.C. Toward the cure of all children with cancer through collaborative efforts: Pediatric oncology as a global challenge. J. Clin. Oncol. 2015, 33, 3065. [Google Scholar] [CrossRef] [PubMed]
- Winther, J.F.; Kenborg, L.; Byrne, J.; Hjorth, L.; Kaatsch, P.; Kremer, L.C.; Haupt, R. Childhood cancer survivor cohorts in Europe. Acta Oncol. 2015, 54, 655–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.T.; Ness, K.K. Exercise interventions in children with cancer: A review. Int. J. Pediatr. 2011, 2011, 11. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, L.; Haupt, R.; Skinner, R.; Grabow, D.; Byrne, J.; Karner, S.; Beck, J.D. Survivorship after childhood cancer: PanCare: A European Network to promote optimal long-term care. Eur. J. Cancer 2015, 51, 1203–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaatsch, P. Epidemiology of childhood cancer. Cancer Treat. Rev. 2010, 36, 277–285. [Google Scholar] [CrossRef]
- Geenen, M.M.; Cardous-Ubbink, M.C.; Kremer, L.C.; van den Bos, C.; van der Pal, H.J.; Heinen, R.C.; Jaspers, M.W.; Koning, C.C.; Oldenburger, F.; Langeveld, N.E.; et al. Medical Assessment of Adverse Health Outcomes in Long-term Survivors of Childhood Cancer. JAMA 2007, 297, 2705–2715. [Google Scholar] [CrossRef]
- Ness, K.K.; Hudson, M.M.; Ginsberg, J.P.; Nagarajan, R.; Kaste, S.C.; Marina, N.; Gurney, J.G. Physical performance limitations in the Childhood Cancer Survivor Study cohort. J. Clin. Oncol. 2009, 27, 2382. [Google Scholar] [CrossRef]
- San Juan, A.F.; Chamorro-Viña, C.; Maté-Muñoz, J.L.; Del Valle, M.F.; Cardona, C.; Hernández, M.; Lucia, A. Functional capacity of children with leukemia. Int. J. Sports Med. 2008, 29, 163–167. [Google Scholar] [CrossRef]
- Roczniak, W.; Babuska, R.M.; Roczniak, A.; Roczniak, R.G. Assessment criteria of motor development of primary school children. Medycyna Ogólna i Nauki o Zdrowiu 2015, 21, 138–141. (In Polish) [Google Scholar] [CrossRef]
- Berkman, A.M.; Lakoski, S.G. Treatment, behavioral, and psychosocial components of cardiovascular disease risk among survivors of childhood and young adult cancer. J. Am. Heart Assoc. 2015, 4, e001891. [Google Scholar] [CrossRef]
- Langeveld, N.; Stam, H.; Grootenhuis, M.; Last, B. Quality of life in young adult survivors of childhood cancer. Support. Care Cancer 2002, 10, 579–600. [Google Scholar] [CrossRef] [PubMed]
- Zebrack, B.J.; Chesler, M.A. Quality of life in childhood cancer survivors. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2002, 11, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Stam, H.; Grootenhuis, M.A.; Caron, H.N.; Last, B. Quality of life and current coping in young adult survivors of childhood cancer: Positive expectations about the further course of the disease were correlated with better quality of life. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2006, 15, 31–43. [Google Scholar] [CrossRef]
- Richter, D.; Koehler, M.; Friedrich, M.; Hilgendorf, I.; Mehnert, A.; Weißflog, G. Psychosocial interventions for adolescents and young adult cancer patients: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2015, 95, 370–386. [Google Scholar] [CrossRef]
- Quinn, G.P.; Gonçalves, V.; Sehovic, I.; Bowman, M.L.; Reed, D.R. Quality of life in adolescent and young adult cancer patients: A systematic review of the literature. Patient Relat. Outcome Meas. 2015, 6, 19–51. [Google Scholar] [CrossRef]
- Ritt-Olson, A.; Miller, K.; Baezconde-Garbanati, L.; Freyer, D.; Ramirez, C.; Hamilton, A.; Milam, J. Depressive Symptoms and Quality of Life Among Adolescent and Young Adult Cancer Survivors: Impact of Gender and Latino Culture. J. Adolesc. Young Adult Oncol. 2018, 7, 384–388. [Google Scholar] [CrossRef]
- Järvelä, L.S.; Kemppainen, J.; Niinikoski, H.; Hannukainen, J.C.; Lähteenmäki, P.M.; Kapanen, J.; Heinonen, O.J. Effects of a home-based exercise program on metabolic risk factors and fitness in long-term survivors of childhood acute lymphoblastic leukemia. Pediatr. Blood Cancer 2012, 59, 155–160. [Google Scholar] [CrossRef]
- Braam, K.I.; van der Torre, P.; Takken, T.; Veening, M.A.; van Dulmen-den Broeder, E.; Kaspers, G.J. Physical exercise training interventions for children and young adults during and after treatment for childhood cancer. Cochrane Database Syst. Rev. 2013, 4, CD008796. [Google Scholar]
- Thorsteinsson, T.; Larsen, H.B.; Schmiegelow, K.; Thing, L.F.; Krustrup, P.; Pedersen, M.T.; Christensen, K.B.; Mogensen, P.R.; Helms, A.S.; Andersen, L.B. Cardiorespiratory fitness and physical function in children with cancer from diagnosis throughout treatment. BMJ Open Sport Exerc. Med. 2017, 3, e000179. [Google Scholar] [CrossRef] [Green Version]
- Simioni, C.; Zauli, G.; Martelli, A.M.; Vitale, M.; Ultimo, S.; Milani, D.; Neri, L.M. Physical training interventions for children and teenagers affected by acute lymphoblastic leukemia and related treatment impairments. Oncotarget 2018, 9, 17199. [Google Scholar] [CrossRef] [PubMed]
- Kowaluk, A.; Woźniewski, M. Physical activity and quality of life in children treated for leukaemia. Physiother. Q. 2018, 2, 9–18. [Google Scholar] [CrossRef]
- Aznar, S.; Webster, A.L.; San Juan, A.F.; Chamorro-Vina, C.; Mate-Munoz, J.L.; Moral, S.; Lucia, A. Physical activity during treatment in children with leukemia: A pilot study. Appl. Physiol. Nutr. Metab. 2006, 31, 407–413. [Google Scholar] [CrossRef]
- Götte, M.; Kesting, S.; Winter, C.; Rosenbaum, D.; Boos, J. Comparison of self-reported physical activity in children and adolescents before and during cancer treatment. Pediatr. Blood Cancer 2014, 61, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Keats, M.R.; Courneya, K.S.; Danielsen, S.; Whitsett, S.F. Leisure-time physical activity and psychosocial well-being in adolescents after cancer diagnosis. J. Pediatr. Oncol. Nurs. 1999, 16, 180–188. [Google Scholar] [CrossRef]
- Klika, R.; Tamburini, A.; Galanti, G.; Mascherini, G.; Stefani, L. The Role of Exercise in Pediatric and Adolescent Cancers: A Review of Assessments and Suggestions for Clinical Implementation. J. Funct. Morphol. Kinesiol. 2018, 3, 7. [Google Scholar] [CrossRef]
- Marciniak, A.; Lewandowski, J. Speed of running of 16-year-old adolescents in the aspect of somatic-motor conditionings. Rocznik Lubuski 2014, 40, 65–77. (In Polish) [Google Scholar]
- Ness, K.K.; Kaste, S.C.; Zhu, L.; Pui, C.H.; Jeha, S.; Nathan, P.C.; Karlage, R.E. Skeletal, neuromuscular and fitness impairments among children with newly diagnosed acute lymphoblastic leukemia. Leuk. Lymphoma 2015, 56, 1004–1011. [Google Scholar] [CrossRef]
- Zhou, F.; Zhang, M.; Han, J.; Hao, J.; Xiao, Y.; Liu, Q.; Jin, R.; Mei, H. Skeletal abnormalities detected by SPECT is associated with increased relapse risk in pediatric acute lymphoblastic leukemia. Oncotarget 2017, 8, 79347. [Google Scholar] [CrossRef]
- Chabros, E.; Charzewska, J.; Rogalska-Niedźwiedź, M.; Wojszczyk, B.; Chwojnowska, Z.; Fabiszewska, J. Low physical activity of adolescents promotes development of obesity. Probl. Hig. Epidemiol. 2008, 89, 58–61. (In Polish) [Google Scholar]
- Deisenroth, A.; Söntgerath, R.; Schuster, A.J.; von Busch, C.; Huber, G.; Eckert, K.; Wiskemann, J. Muscle strength and quality of life in patients with childhood cancer at early phase of primary treatment. Pediatr. Hematol. Oncol. 2016, 33, 393–407. [Google Scholar] [CrossRef]
- Beltran-Valls, M.R.; Janssen, X.; Farooq, A.; Adamson, A.J.; Pearce, M.S.; Reilly, J.K.; Reilly, J.J. Longitudinal changes in vigorous intensity physical activity from childhood to adolescence: Gateshead Millennium Study. J. Sci. Med. Sport 2019, 22, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J. When does it all go wrong? Longitudinal studies of changes in moderate-to-vigorous-intensity physical activity across childhood and adolescence. J. Exerc. Sci. Fit. 2016, 14, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Withycombe, J.S.; Smith, L.M.; Meza, J.L.; Merkle, C.; Faulkner, M.S.; Ritter, L.; Moore, K. Weight change during childhood acute lymphoblastic leukemia induction therapy predicts obesity: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2015, 62, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Loeffen, E.A.; Brinksma, A.; Miedema, K.G.; De Bock, G.H.; Tissing, W.J. Clinical implications of malnutrition in childhood cancer patients—infections and mortality. Support. Care Cancer 2015, 23, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Levy, E.; Samoilenko, M.; Morel, S.; England, J.; Amre, D.; Bertout, L.; Lefebvre, G. Cardiometabolic Risk Factors in Childhood, Adolescent and Young Adult Survivors of Acute Lymphoblastic Leukemia—A Petale Cohort. Sci. Rep. 2017, 7, 17684. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.S.; Valenzuela, P.L.; Rincón-Castanedo, C.; Takken, T.; Fiuza-Luces, C.; Santos-Lozano, A.; Lucia, A. Exercise training in childhood cancer: A systematic review and meta-analysis of randomized controlled trials. Cancer Treat. Rev. 2018, 70, 154–167. [Google Scholar] [CrossRef]
- Braam, K.I.; van Dijk-Lokkart, E.M.; Kaspers, G.J.; Takken, T.; Huisman, J.; Buffart, L.M.; van Dulmen-den Broeder, E. Effects of a combined physical and psychosocial training for children with cancer: A randomized controlled trial. BMC Cancer 2018, 18, 1289. [Google Scholar] [CrossRef] [PubMed]
- Fauteux, V.; Pode, T. Overview of QALY elicitation methods. Int. J. Health Prefer. Res. 2017, 1, 2–14. [Google Scholar]
- Weinstein, M.; Torrance, G.; McGuire, A. QALYs: The Basics. Value Health 2009, 12, S5–S9. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Study Group (Mean ± SD) | Control Group (Mean ± SD) | ||
|---|---|---|---|---|
| Girls (n = 30) | Boys (n = 41) | Girls (n = 42) | Boys (n = 43) | |
| Age [years] | 11.57 ± 3.67 | 10.97 ± 2.70 | 10.70 ± 1.25 | 10.72 ± 1.20 |
| Body height [m] | 1.45 ± 0.18 | 1.45 ± 0.16 | 1.41 ± 0.07 | 1.43 ± 0.06 |
| Body weight [kg] | 40.74 ± 13.70 | 39.74 ± 15.45 | 35.02 ± 7.18 | 37.54 ± 8.13 |
| BMI [kg/m²] | 19.26 ± 4.86 | 18.40 ± 4.31 | 26.78 ± 4.76 | 18.17 ± 2.95 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malicka, I.; Mrowiec, J.; Sajkiewicz, N.; Siewierska, K.; Czajkowska, M.; Woźniewski, M. Physical Fitness of School-Age Children after Cancer Treatment. Int. J. Environ. Res. Public Health 2019, 16, 1436. https://doi.org/10.3390/ijerph16081436
Malicka I, Mrowiec J, Sajkiewicz N, Siewierska K, Czajkowska M, Woźniewski M. Physical Fitness of School-Age Children after Cancer Treatment. International Journal of Environmental Research and Public Health. 2019; 16(8):1436. https://doi.org/10.3390/ijerph16081436
Chicago/Turabian StyleMalicka, Iwona, Joanna Mrowiec, Natalia Sajkiewicz, Katarzyna Siewierska, Maria Czajkowska, and Marek Woźniewski. 2019. "Physical Fitness of School-Age Children after Cancer Treatment" International Journal of Environmental Research and Public Health 16, no. 8: 1436. https://doi.org/10.3390/ijerph16081436
APA StyleMalicka, I., Mrowiec, J., Sajkiewicz, N., Siewierska, K., Czajkowska, M., & Woźniewski, M. (2019). Physical Fitness of School-Age Children after Cancer Treatment. International Journal of Environmental Research and Public Health, 16(8), 1436. https://doi.org/10.3390/ijerph16081436