Medication Adherence, Burden and Health-Related Quality of Life in Adults with Predialysis Chronic Kidney Disease: A Prospective Cohort Study

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
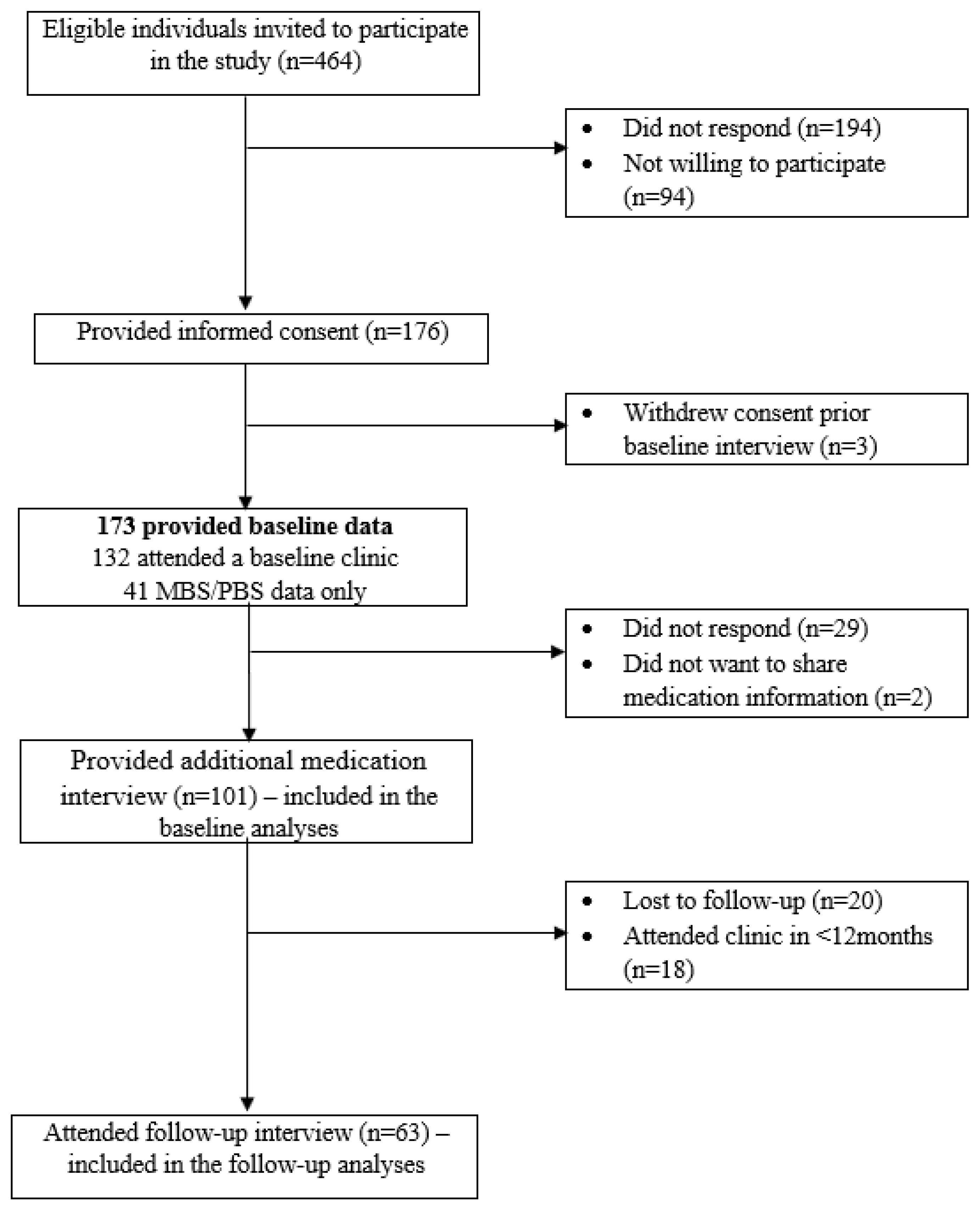
2.1. Study Design and Population
2.2. Measures
Medication-Related Factors
2.3. Covariates
3. Statistical Analyses
4. Results
4.1. Factors Associated with Medication Nonadherence
4.2. Factors Associated with Perceived and Actual Medication Burden
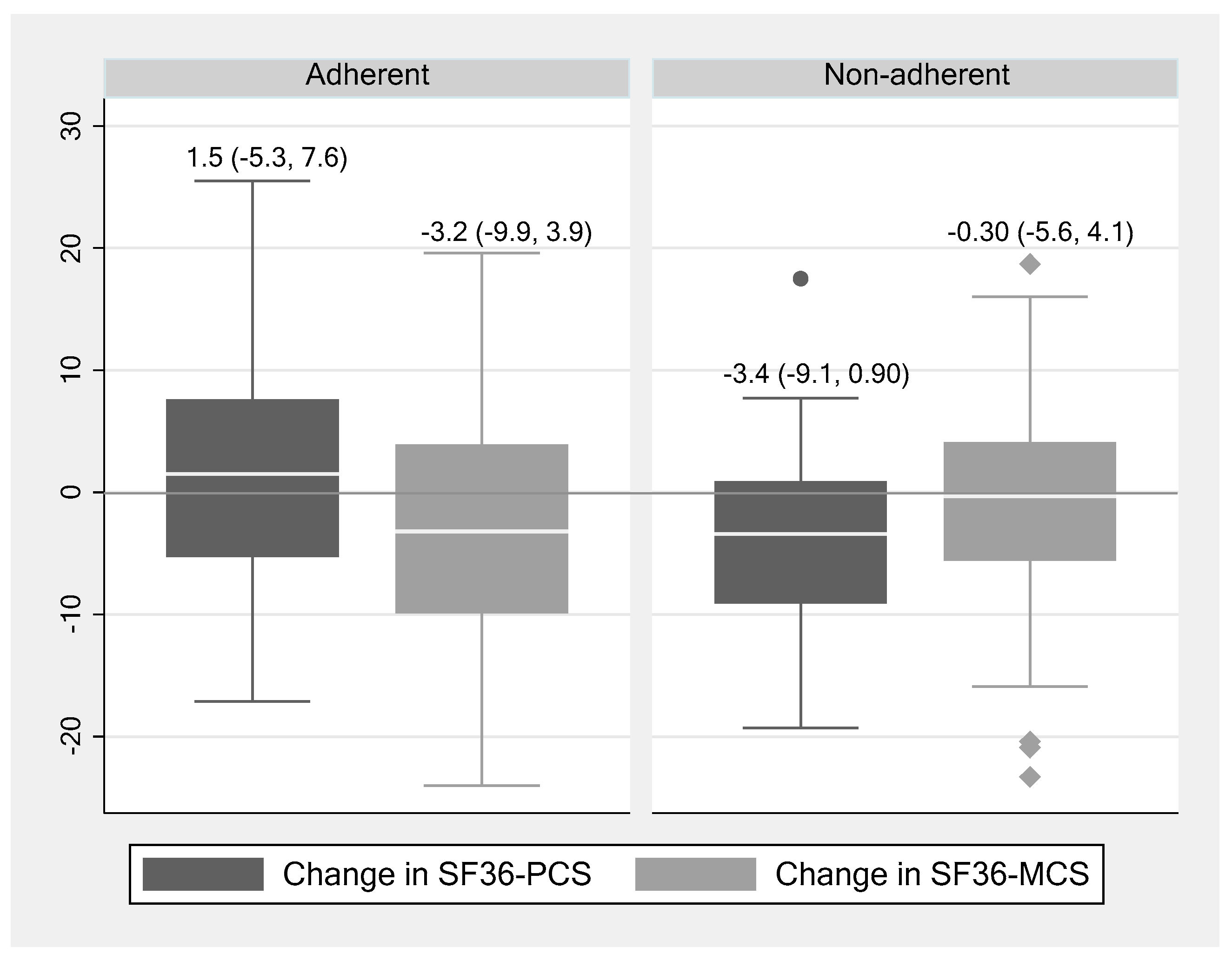
4.3. Changes in HRQOL and Its Association with Medication Nonadherence
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| HRQOL Scales | All Participants (n = 101) | Participants with Follow-Up Data | ||
|---|---|---|---|---|
| Kidney Disease-Related Scales (n = 63) | Baseline | Follow-Up | p-Value * | |
| Burden of kidney disease | 75 (24) | 77 (25) | 70 (31) | 0.01 |
| Symptoms | 79 (16) | 78 (16) | 77 (15) | 0.59 |
| Cognitive function | 81 (16) | 81 (15) | 79 (16) | 0.45 |
| Effect of kidney disease | 88 (13) | 88 (14) | 86 (17) | 0.19 |
| Sleep | 64 (19) | 62 (20) | 62 (22) | 0.80 |
| Social interaction | 82 (15) | 82 (15) | 82 (15) | 0.89 |
| Social support | 83 (25) | 87 (22) | 82 (27) | 0.18 |
| Work status | 43 (34) | 42 (33) | 41 (35) | 0.64 |
| Overall health status | 63 (18) | 62 (19) | 59 (19) | 0.08 |
| SF-36 scales (n = 60) | ||||
| Physical function | 56 (26) | 56 (26) | 55 (30) | 0.78 |
| Physical role limitations | 47 (42) | 49 (39) | 36 (38) | 0.01 |
| Pain | 60 (28) | 64 (27) | 60 (28) | 0.13 |
| General health | 49 (29) | 46 (20) | 44 (21) | 0.29 |
| Emotional well-being | 79 (22) | 77 (18) | 76 (19) | 0.57 |
| Emotional role limitations | 70 (40) | 77 (36) | 65 (38) | 0.02 |
| Social function | 77 (30) | 77 (26) | 68 (29) | 0.004 |
| Vitality | 55 (27) | 48 (23) | 45 (24) | 0.22 |
| SF36-PCS | 38 (10) | 38 (11) | 37 (11) | 0.22 |
| SF36-MCS | 51 (11) | 52 (11) | 49 (11) | 0.03 |
References
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karamanidou, C.; Clatworthy, J.; Weinman, J.; Horne, R. A systematic review of the prevalence and determinants of nonadherence to phosphate binding medication in patients with end-stage renal disease. BMC Nephrol. 2008, 9, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truong, V.T.; Moisan, J.; Kroger, E.; Langlois, S.; Gregoire, J.P. Persistence and compliance with newly initiated antihypertensive drug treatment in patients with chronic kidney disease. Patient Prefer. Adherence 2016, 10, 1121–1129. [Google Scholar] [PubMed] [Green Version]
- Hsu, K.L.; Fink, J.C.; Ginsberg, J.S.; Yoffe, M.; Zhan, M.; Fink, W.; Woods, C.M.; Diamantidis, C.J. Self-reported Medication Adherence and Adverse Patient Safety Events in CKD. Am. J. Kidney Dis. 2015, 66, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Muntner, P.; Judd, S.E.; Krousel-Wood, M.; McClellan, W.M.; Safford, M.M. Low medication adherence and hypertension control among adults with CKD: Data from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) Study. Am. J. Kidney Dis. 2010, 56, 447–457. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, K.E.; Edie, C.F.; Laflam, P.; Simbartl, L.A.; Thakar, C.V. Adherence to antihypertensive agents and blood pressure control in chronic kidney disease. Am. J. Nephrol. 2010, 32, 541–548. [Google Scholar] [CrossRef]
- Molnar, M.Z.; Gosmanova, E.O.; Sumida, K.; Potukuchi, P.K.; Lu, J.L.; Jing, J.; Ravel, V.A.; Soohoo, M.; Rhee, C.M.; Streja, E.; et al. Predialysis Cardiovascular Disease Medication Adherence and Mortality After Transition to Dialysis. Am. J. Kidney Dis. 2016, 68, 609–618. [Google Scholar] [CrossRef] [Green Version]
- Dawson, J.; Doll, H.; Fitzpatrick, R.; Jenkinson, C.; Carr, A.J. The routine use of patient reported outcome measures in healthcare settings. BMJ 2010, 340, c186. [Google Scholar] [CrossRef]
- Ducharlet, K.; Sundarajan, V.; Philip, J.; Weil, J.; Barker, N.; Langham, R.G.; Burchell, J.; Gock, H. Patient-Reported outcome measures and their utility in the management of patients with advanced chronic kidney disease. Nephrology 2018, 24, 814–818. [Google Scholar] [CrossRef]
- Ghimire, S.; Peterson, G.M.; Castelino, R.L.; Jose, M.D.; Zaidi, S.T. Medication Regimen Complexity and Adherence in Haemodialysis Patients: An Exploratory Study. Am. J. Nephrol. 2016, 43, 318–324. [Google Scholar] [CrossRef]
- Neri, L.; Martini, A.; Andreucci, V.E.; Gallieni, M.; Rey, L.A.; Brancaccio, D. Regimen complexity and prescription adherence in dialysis patients. Am. J. Nephrol. 2011, 34, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Wyld, M.L.R.; Morton, R.L.; Clayton, P.; Wong, M.G.; Jardine, M.; Polkinghorne, K.; Chadban, S. The impact of progressive chronic kidney disease on health-related quality-of-life: A 12-year community cohort study. Qual. Life Res. 2019, 28, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Wee, H.L.; Seng, B.J.; Lee, J.J.; Chong, K.J.; Tyagi, P.; Vathsala, A.; How, P. Association of anemia and mineral and bone disorder with health-related quality of life in Asian pre-dialysis patients. Health Qual. Life Outcomes 2016, 14, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wimmer, B.C.; Cross, A.J.; Jokanovic, N.; Wiese, M.D.; George, J.; Johnell, K.; Diug, B.; Bell, J.S. Clinical Outcomes Associated with Medication Regimen Complexity in Older People: A Systematic Review. J. Am. Geriatr. Soc. 2017, 65, 747–753. [Google Scholar] [CrossRef]
- McKercher, C.M.; Venn, A.J.; Blizzard, L.; Nelson, M.R.; Palmer, A.J.; Ashby, M.A.; Scott, J.L.; Jose, M.D. Psychosocial factors in adults with chronic kidney disease: Characteristics of pilot participants in the Tasmanian Chronic Kidney Disease study. BMC Nephrol. 2013, 14, 83. [Google Scholar] [CrossRef] [Green Version]
- George, J.; Phun, Y.T.; Bailey, M.J.; Kong, D.C.; Stewart, K. Development and validation of the medication regimen complexity index. Ann. Pharm. 2004, 38, 1369–1376. [Google Scholar] [CrossRef]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- George, J.; Mackinnon, A.; Kong, D.C.; Stewart, K. Development and validation of the Beliefs and Behaviour Questionnaire (BBQ). Patient Educ. Couns. 2006, 64, 50–60. [Google Scholar] [CrossRef]
- Stewart, K.; Mc Namara, K.P.; George, J. Challenges in measuring medication adherence: Experiences from a controlled trial. Int. J. Clin. Pharm. 2014, 36, 15–19. [Google Scholar] [CrossRef]
- Socio-Economic Indexes for Areas. 2011. Available online: http://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 9 April 2018).
- Liu, J.; Huang, Z.; Gilbertson, D.T.; Foley, R.N.; Collins, A.J. An improved comorbidity index for outcome analyses among dialysis patients. Kidney Int. 2010, 77, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standardised measure of biological and pyschosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- McClellan, W.M.; Anson, C.; Birkeli, K.; Tuttle, E. Functional status and quality of life: Predictors of early mortality among patients entering treatment for end stage renal disease. J. Clin. Epidemiol. 1991, 44, 83–89. [Google Scholar] [CrossRef]
- Hill, S.A.; Laugharne, R. Decision making and information seeking preferences among psychiatric patients. J. Ment. Health 2006, 15, 75–84. [Google Scholar] [CrossRef]
- Ende, J.; Kazis, L.; Moskowitz, M.A. Preferences for autonomy when patients are physicians. J. Gen. Intern. Med. 1990, 5, 506–509. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Watnick, S.; Wang, P.L.; Demadura, T.; Ganzini, L. Validation of 2 depression screening tools in dialysis patients. Am. J. Kidney Dis. 2005, 46, 919–924. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Bayliss, M.S.; McHorney, C.A.; Rogers, W.H.; Raczek, A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: Summary of results from the Medical Outcomes Study. Med. Care 1995, 33, 264–279. [Google Scholar]
- Chiu, Y.W.; Teitelbaum, I.; Misra, M.; de Leon, E.M.; Adzize, T.; Mehrotra, R. Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1089–1096. [Google Scholar] [CrossRef]
- Schneider, A.; Wensing, M.; Quinzler, R.; Bieber, C.; Szecsenyi, J. Higher preference for participation in treatment decisions is associated with lower medication adherence in asthma patients. Patient Educ. Couns. 2007, 67, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Demain, S.; Goncalves, A.C.; Areia, C.; Oliveira, R.; Marcos, A.J.; Marques, A.; Parmar, R.; Hunt, K. Living with, managing and minimising treatment burden in long term conditions: A systematic review of qualitative research. PLoS ONE 2015, 10, e0125457. [Google Scholar] [CrossRef] [PubMed]
- Karamanidou, C.; Weinman, J.; Horne, R. A qualitative study of treatment burden among haemodialysis recipients. J. Health Psychol. 2014, 19, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Holt, E.; Joyce, C.; Dornelles, A.; Morisky, D.; Webber, L.S.; Muntner, P.; Krousel-Wood, M. Sex differences in barriers to antihypertensive medication adherence: Findings from the cohort study of medication adherence among older adults. J. Am. Geriatr. Soc. 2013, 61, 558–564. [Google Scholar] [CrossRef]
- Krska, J.; Katusiime, B.; Corlett, S.A. Patient experiences of the burden of using medicines for long-term conditions and factors affecting burden: A cross-sectional survey. Health Soc. Care Community 2018, 26, 946–959. [Google Scholar] [CrossRef]
- Tran, V.T.; Montori, V.M.; Eton, D.T.; Baruch, D.; Falissard, B.; Ravaud, P. Development and description of measurement properties of an instrument to assess treatment burden among patients with multiple chronic conditions. BMC Med. 2012, 10, 68. [Google Scholar] [CrossRef] [Green Version]
- Tesfaye, W.H.; Peterson, G.M.; Castelino, R.L.; McKercher, C.; Jose, M.; Zaidi, S.T.R.; Wimmer, B.C. Medication-Related Factors and Hospital Readmission in Older Adults with Chronic Kidney Disease. J. Clin. Med. 2019, 8, 395. [Google Scholar] [CrossRef] [Green Version]


| Adherence (MGLS) | Adherence (TABS) | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Total (n = 101) | Yes (n = 58) | No (n = 43) | p | Yes (n = 40) | No (n = 61) | p |
| Sociodemographic | |||||||
| Age (years) | 72 (11) | 73 (11) | 70 (11) | 0.12 | 74 (11) | 70 (11) | 0.06 |
| Male gender, n (%) | 68 (67) | 36 (53) | 32 (47) | 0.19 | 31 (46) | 37 (54) | 0.08 |
| Level of education (year 12 or less), n (%) | 63 (62) | 38 (60) | 25 (40) | 0.45 | 26 (41) | 37 (59) | 0.66 |
| Married/de facto, n (%) | 65 (49) | 36 (55) | 29 (45) | 0.58 | 27 (41) | 38 (59) | 0.59 |
| Government pension, n (%) | 64 (63) | 37 (58) | 27 (42) | 0.6 | 27 (42) | 37 (58) | 0.67 |
| Index of Disadvantage (highest quartile) | 33 (33) | 19 (58) | 14 (42) | 0.3 | 11 (33) | 22 (67) | 0.47 |
| Autonomy preference index | |||||||
| Decision-making | 45 (17) | 42 (15) | 49 (18) | 0.04 | 41 (13) | 47 (18) | 0.1 |
| Information-seeking | 82 (11) | 83 (11) | 82 (11) | 0.78 | 82 (11) | 83 (11) | 0.74 |
| Karnofsky performance scale | 87 (10) | 86 (8) | 88 (12) | 0.54 | 87 (9) | 86 (12) | 0.65 |
| Major depression (PHQ-9 score ≥ 10) | 12 (12) | 5 (42) | 7 (58) | 0.24 | 6 (50) | 6 (50) | 0.61 |
| Clinical | |||||||
| Smoking (former/current), n (%) | 51 (50) | 29 (57) | 22 (43) | 0.91 | 23 (45) | 28 (55) | 0.25 |
| Comorbidity index, median (IQR) | 3 (1–4) | 3 (1–5) | 2 (1–3) | 0.38 | 3 (2–4) | 2 (1–3) | 0.04 |
| Common comorbidities, n (%) | |||||||
| Hypertension | 90 (94) | 52 (58) | 38 (42) | 0.71 | 38 (42) | 52 (58) | 0.67 |
| Diabetes mellitus | 39 (40) | 28 (72) | 11 (28) | 0.02 | 13 (33) | 26 (67) | 0.19 |
| Atherosclerotic disease | 36 (37) | 20 (56) | 16 (44) | 0.74 | 18 (50) | 18 (50) | 0.18 |
| Congestive heart failure | 17 (18) | 7 (41) | 10 (59) | 0.12 | 9 (53) | 8 (47) | 0.27 |
| Peripheral vascular disease | 13 (13) | 6 (46) | 7 (54) | 0.37 | 8 (61.5) | 5 (38.5) | 0.11 |
| Malignant neoplasm | 20 (21) | 14 (70) | 6 (30) | 0.22 | 13 (65) | 7 (35) | 0.01 |
| Body mass index, kg/m2 | 30 (6) | 31 (6) | 30 (5) | 0.67 | 28 (26–31) | 32 (27–35) | 0.02 |
| ADL | 5.8 (0.4) | 5.9 (0.3) | 5.7 (0.5) | 0.1 | 5.8 (0.4) | 5.8 (0.4) | 0.36 |
| IADL | 5.5 (1.4) | 5.5 (1.4) | 5.2 (1.1) | 0.06 | 5.4 (1.4) | 5.6 (1.5) | 0.34 |
| Cognitive impairment (MOCA < 26), n (%) | 65 (67) | 41 (72) | 24 (60) | 0.22 | 23 (35) | 42 (65) | 0.17 |
| Laboratory | |||||||
| Haemoglobin (g/L) | 119 (18) | 117 (15) | 121 (22) | 0.3 | 119 (20) | 119 (17) | 0.99 |
| Serum creatinine (μmol/L) | 265 (112) | 249 (101) | 288 (122) | 0.03 | 266 (101) | 265 (119) | 0.97 |
| eGFR (mL/min/1.73 m2) | 21 (7) | 22 (6) | 21 (7) | 0.51 | 21 (7) | 21 (6.5) | 0.89 |
| Medical | |||||||
| No. of medications, median (IQR) | 8 (6–11) | 8 (6–11) | 8 (6–11) | 0.73 | 8 (5–11) | 8 (6–10) | 0.73 |
| MRCI, median (IQR) | 19 (14–27) | 20 (9–28) | 17 (14–27) | 0.41 | 19 (17–27) | 19 (14–27) | 0.76 |
| PBM, median (IQR) | 1.17 (1–1.33) | 1 (1–1.33) | 1.33 (1–1.33) | 0.01 | 1 (1–1.33) | 1.33 (1–1.33) | 0.04 |
| HRQOL (SF-36) | |||||||
| PCS | 39 (10) | 39 (10) | 39 (10) | 0.65 | 39 (10) | 39 (10) | 0.96 |
| MCS | 51 (10) | 51 (9) | 50 (11) | 0.62 | 51 (10) | 51 (10) | 0.96 |
| a. Nonadherence (MGLS) | Unadjusted ORs (95% CIs) | Adjusted ORs (95% CIs) * |
| No. of medications | 0.97 (0.87–1.08) | 0.96 (0.85–1.07) |
| MRCI (cont.) | 0.83 (0.55–1.26) | 0.89 (0.56–1.44) |
| PBM (cont.) | 4.02 (1.03–16) | 4.89 (1.02–23.5) |
| Having diabetes | 0.37 (0.15–0.91) | 0.36 (0.14–0.89) |
| Decision making (cont.) | 1.11 (1.001–1.23) | 1.15 (1.02–1.29) |
| Decision-making (cat; score > 50) | 3.29 (1.41–7.69) | 4.56 (1.68–12.35) |
| b. Nonadherence (TABS) | Unadjusted ORs (95% CIs) | Adjusted ORs (95% CIs) |
| No. of medications | 1.02 (0.91–1.13) | 1.04 (0.92–1.18) |
| MRCI (cont.) | 1.003 (0.96–1.05) | 1.01 (0.96–1.06) |
| PBM (cont.) | 3.67 (0.84–16.1) | 2.78 (0.53–14.5) |
| BMI (≥30 kg/m2) | 2.85 (0.21–2.6) | 3.81 (1.01–14.5) |
| a. Perceived Medication Burden (PBM)—Continuous | ||
| Variables | Unadjusted β (95% CIs) | Adjusted β (95% CIs) |
| No. of medications | 0.02 (0.01, 0.04) | 0.02 (0.01, 0.04) |
| MRCI (cont.) | 0.08 (0.02, 0.14) | 0.10 (0.03, 0.15) |
| Dosage form | 0.023 (−0.001, 0.05) | 0.024 (−0.001, 0.05) |
| Dosing frequency | 0.02 (0.01, 0.03) | 0.02 (0.01, 0.03) |
| Additional instructions | 0.01 (−0.01, 0.02) | 0.01 (−0.01, 0.03) |
| Age (cont.) | −0.01 (−0.014, −0.004) | −0.01 (−0.015, −0.005) |
| API Decision-making (cont.) | 0.02 (0.01, 0.03) | 0.02 (0.01, 0.03) |
| API Information-seeking (cont.) | 0.02 (0.01, 0.04) | 0.02 (0.01, 0.04) |
| b. Actual Medication Burden (MRCI)—Continuous | ||
| Variables | Unadjusted β (95% CIs) | Adjusted β (95% CIs) |
| No. of medications | 2.44 (2.26, 2.63) | 2.49 (2.31, 2.67) |
| Having diabetes | 7.31 (3.57, 11.1) | 7.54 (3.43, 11.6) |
| Kidney disease-targeted scales | ||
| Symptom | −0.26 (−0.38, −0.15) | −0.25 (−0.37, −0.17) |
| Effects of kidney disease | −0.19 (−0.34, −0.06) | −0.23 (−0.39, −0.08) |
| Burden of kidney disease | −0.12 (−0.19, −0.04) | −1.64 (−0.25, −0.08) |
| Work status | −0.09 (−0.15, −0.04) | −0.09 (−0.14, −0.03) |
| SF-36 generic scales | ||
| MCS | −0.15 (−0.35, 0.04) | −0.21 (−0.43, −0.01) |
| PCS | −0.43 (−0.61, −0.26) | −0.44 (−0.62, −0.26) |
| Unadjusted β (95% CIs) | Adjusted β (95% CIs) * | |
|---|---|---|
| SF36-PCS | ||
| Nonadherence | −3.99 (−8.29, 0.31) | −4.64 (−9.10, −0.17) |
| SF36-MCS | ||
| Nonadherence | 1.82 (−3.12, 6.78) | 2.03 (−2.99, 7.05) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tesfaye, W.H.; McKercher, C.; Peterson, G.M.; Castelino, R.L.; Jose, M.; Zaidi, S.T.R.; Wimmer, B.C. Medication Adherence, Burden and Health-Related Quality of Life in Adults with Predialysis Chronic Kidney Disease: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 371. https://doi.org/10.3390/ijerph17010371
Tesfaye WH, McKercher C, Peterson GM, Castelino RL, Jose M, Zaidi STR, Wimmer BC. Medication Adherence, Burden and Health-Related Quality of Life in Adults with Predialysis Chronic Kidney Disease: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(1):371. https://doi.org/10.3390/ijerph17010371
Chicago/Turabian StyleTesfaye, Wubshet H., Charlotte McKercher, Gregory M. Peterson, Ronald L. Castelino, Matthew Jose, Syed Tabish R. Zaidi, and Barbara C. Wimmer. 2020. "Medication Adherence, Burden and Health-Related Quality of Life in Adults with Predialysis Chronic Kidney Disease: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 1: 371. https://doi.org/10.3390/ijerph17010371
APA StyleTesfaye, W. H., McKercher, C., Peterson, G. M., Castelino, R. L., Jose, M., Zaidi, S. T. R., & Wimmer, B. C. (2020). Medication Adherence, Burden and Health-Related Quality of Life in Adults with Predialysis Chronic Kidney Disease: A Prospective Cohort Study. International Journal of Environmental Research and Public Health, 17(1), 371. https://doi.org/10.3390/ijerph17010371