A Comparison of Infection Venues of COVID-19 Case Clusters in Northeast China


Abstract
:1. Introduction
2. Methods
2.1. Data Collection and Preparation
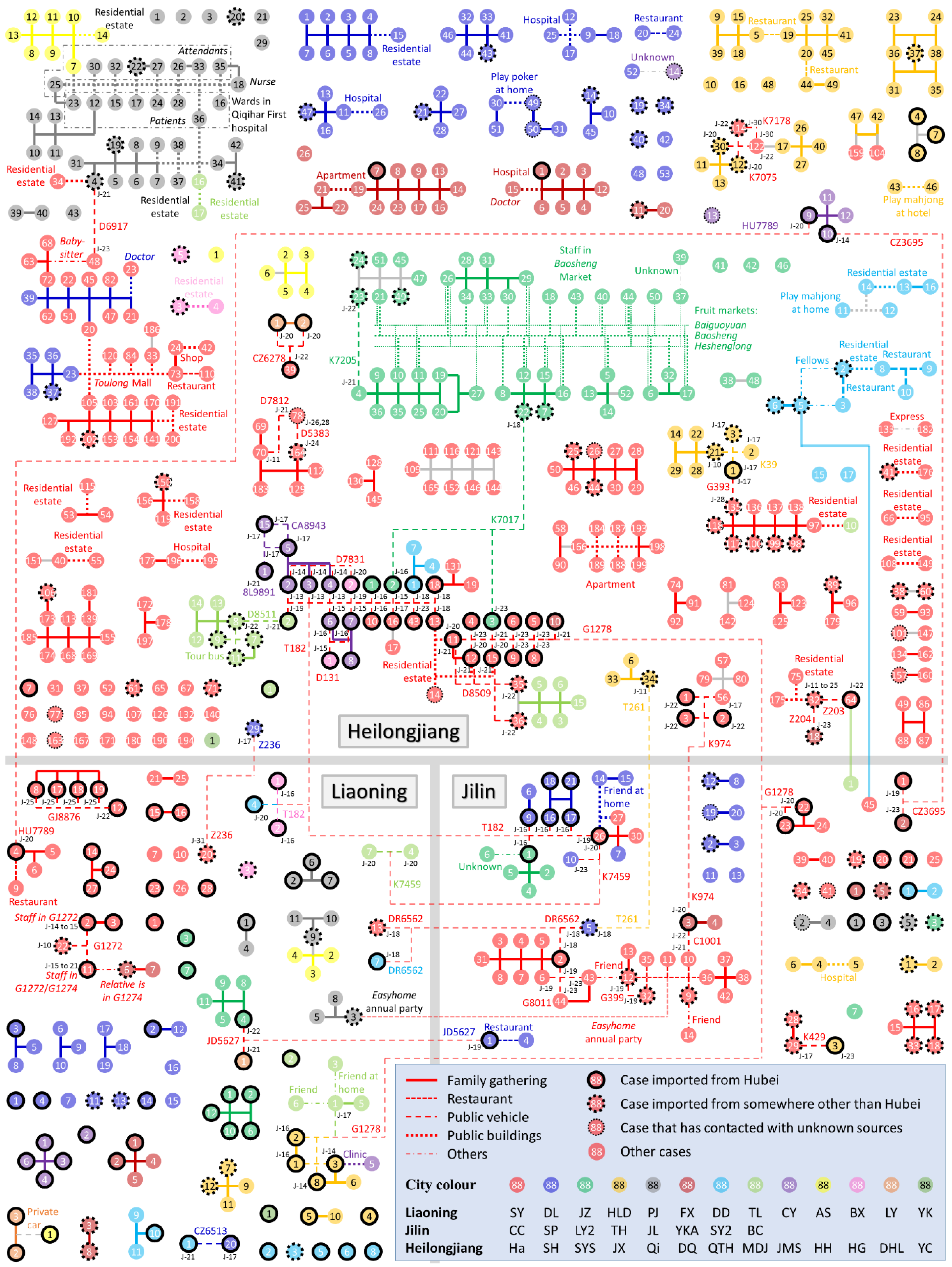
2.2. Identification of Case Clusters
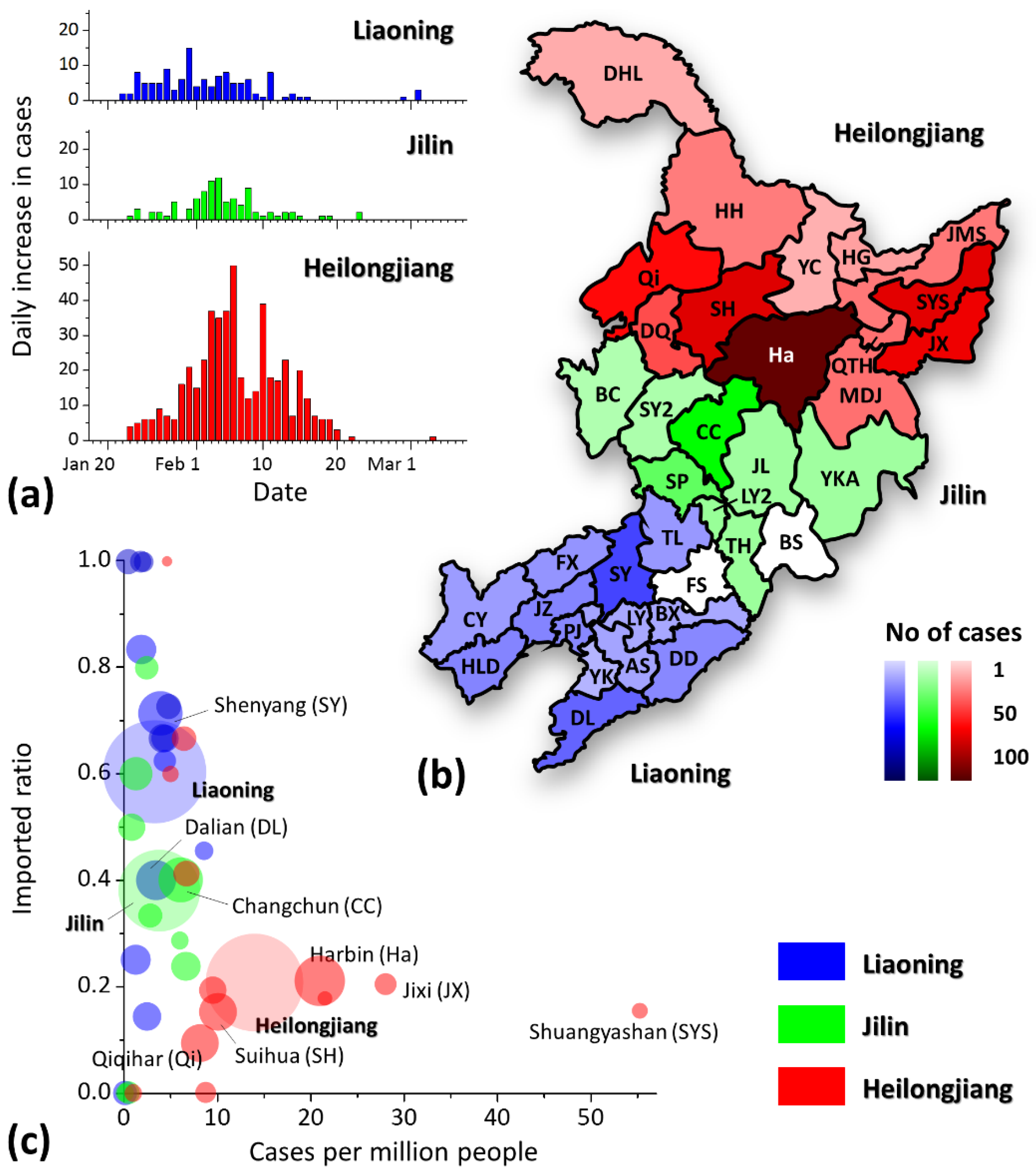
2.3. Epidemic Situation in Different Regions
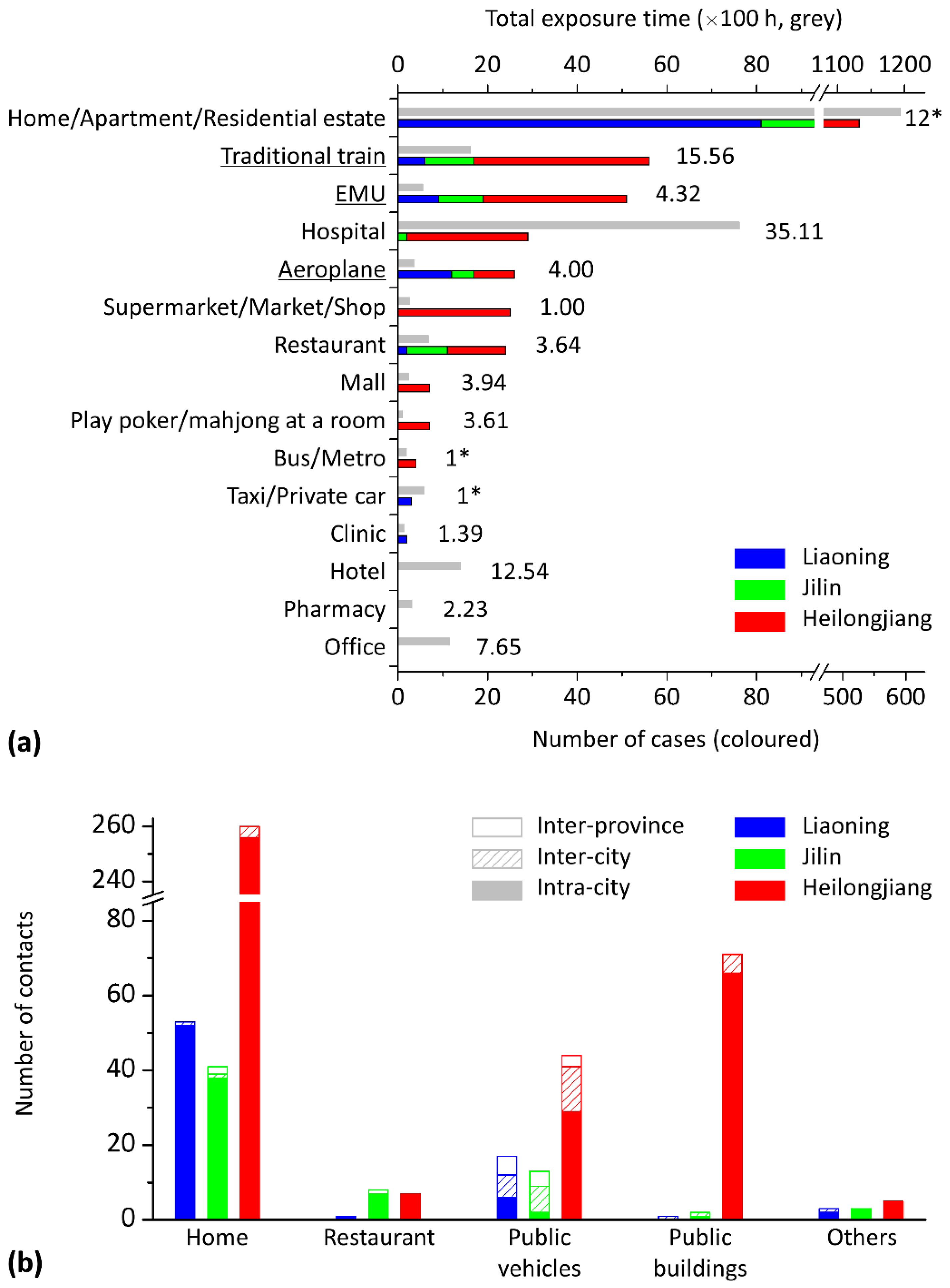
2.4. Case Clustering in Different Locations
2.5. Contact Times between Cases in Different Location Categories
- I.
- If a case is imported from Hubei, it is considered to be the infection source of the first order.
- II.
- If no cases are imported from Hubei but one is imported from outside the three provinces of Northeast China, it is considered to be the infection source of the second order.
- III.
- If no cases are imported from outside the three provinces of northeast China, but a case is imported that has been in close contact with some cases confirmed in other provinces, it is considered to be the infection source of the third order.
- IV.
- If there are multiple possible infection sources of the same order, or if there are no possible transmission sources, the first reported case (usually the case with the lowest serial number) among the cases of the highest order is considered to be the infection source.
- I.
- The disease spreads from the source case to the other cases step by step.
- II.
- The case upstream from an infected case is only selected from direct-connected cases (without an intermediate case).
- III.
- For an infected case with connected cases from different cities or provinces, the infection is first found from the cases of the same city, then from different cities in the same province, and then from different provinces.
- IV.
- For any two cases with more than one type of contact, we assume that the infection occurs in the category of contact with a smaller order in Table 1.
3. Results
3.1. Regional Epidemic Situations
3.2. Case Clustering in Various Locations
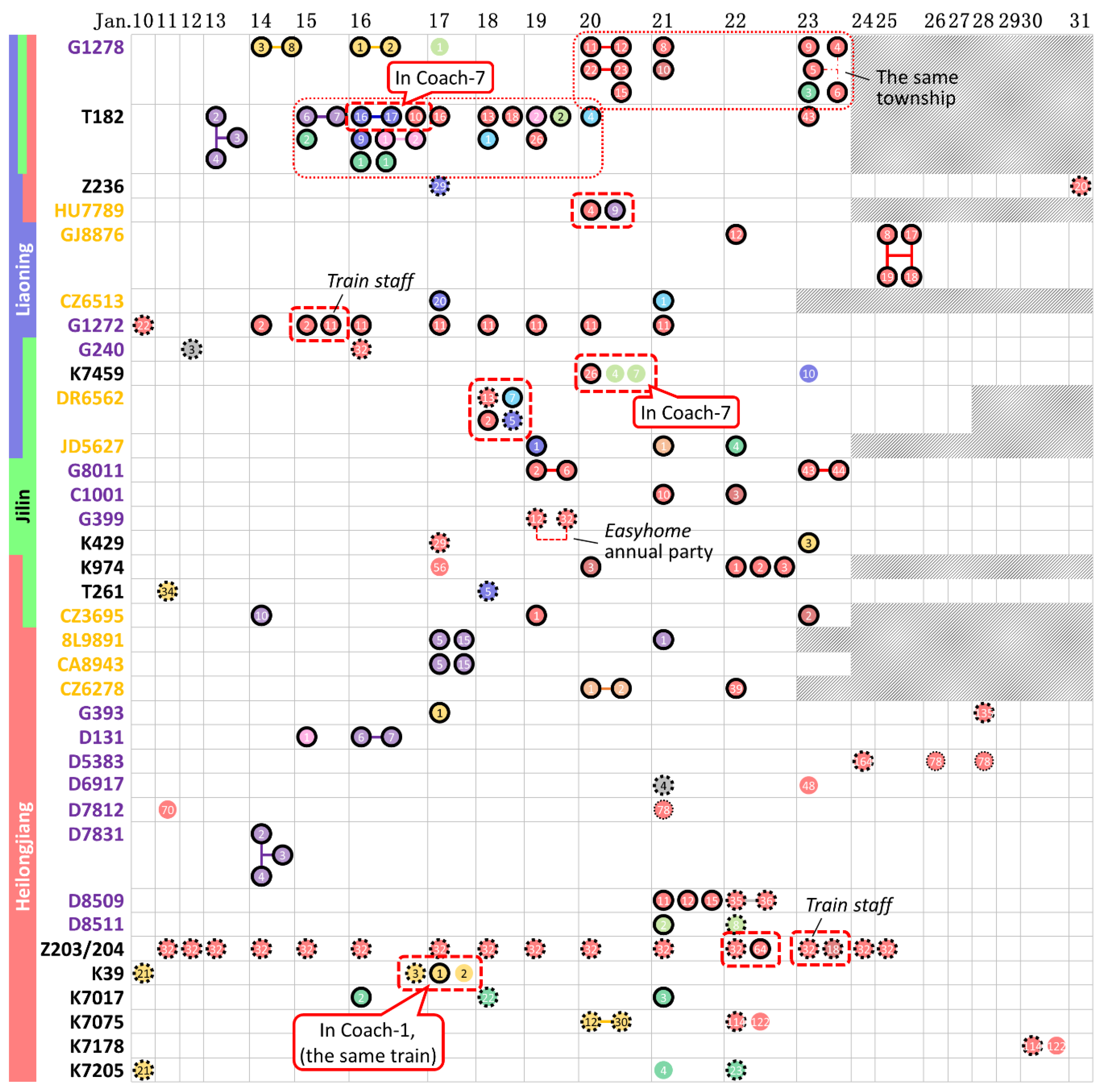
3.3. Case Contact on Public Transport
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [Green Version]
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilder-Smith, A.; Chiew, C.J.; Lee, V.J. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect. Dis. 2020, 20, e102–e107. [Google Scholar] [CrossRef] [Green Version]
- Shangguan, Z.; Wang, M.Y.; Sun, W. What caused the outbreak of COVID-19 in China: From the perspective of crisis management. Int. J. Environ. Res. Public Health 2020, 17, 3279. [Google Scholar] [CrossRef]
- Xiao, S.; Li, Y.; Sung, M.; Wei, J.; Yang, Z. A study of the probable transmission routes of MERS-CoV during the first hospital outbreak in the Republic of Korea. Indoor Air 2018, 28, 51–63. [Google Scholar] [CrossRef]
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int. J. Epidemiol. 2020, dyaa033. [Google Scholar] [CrossRef] [Green Version]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance 2020, 25, 2000062. [Google Scholar] [CrossRef] [Green Version]
- Zheng, R.; Xu, Y.; Wang, W.; Ning, G.; Bi, Y. Spatial transmission of COVID-19 via public and private transportation in China. Travel Med. Infect. Dis. 2020, 34, 101626. [Google Scholar] [CrossRef]
- Zhao, S.; Lin, Q.; Ran, J.; Musa, S.S.; Yang, G.; Wang, W.; Lou, Y.; Gao, D.; Yang, L.; He, D.; et al. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. Int. J. Infect. Dis. 2020, 92, 214–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, P.; Zhu, J.; Zhang, Z.; Han, Y. A familial cluster of infection associated with the 2019 novel coronavirus indicating possible person-to-person transmission during the incubation period. J. Infect. Dis. 2020, 221, 1757–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Fu, J.-B.; Li, K.-F.; Chen, Y.; Wang, H.-L.; Liu, L.-J.; Liu, J.-N.; Zhang, Y.-L.; Liu, S.-L.; Tang, A.; et al. Transmission of COVID-19 in the terminal stage of incubation period: A familial cluster. Int. J. Infect. Dis. 2020, 96, 452–453. [Google Scholar] [CrossRef]
- Qian, G.; Yang, N.; Ma, A.H.Y.; Wang, L.; Li, G.; Chen, X.; Chen, X. COVID-19 transmission within a family cluster by presymptomatic carriers in China. Clin. Infect. Dis. 2020, ciaa316. [Google Scholar] [CrossRef]
- Pung, R.; Chiew, C.J.; Young, B.E.; Chin, S.; Chen, M.I.; Clapham, H.E.; Cook, A.R.; Maurer-Stroh, S.; Toh, M.P.; Poh, C. Investigation of three clusters of COVID-19 in Singapore: Implications for surveillance and response measures. Lancet 2020, 395, 1039–1046. [Google Scholar] [CrossRef]
- Zhang, J.; Tian, S.; Lou, J.; Chen, Y. Familial cluster of COVID-19 infection from an asymptomatic. Crit. Care 2020, 24, 119. [Google Scholar] [CrossRef] [Green Version]
- Armitage, R.; Nellums, L.B. COVID-19 and the consequences of isolating the elderly. Lancet Public Health 2020, 5, e256. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhou, M.; Liu, F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J. Hosp. Infect. 2020, 105, 100–101. [Google Scholar] [CrossRef] [Green Version]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; y Piontti, A.P.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Duan, S.; Yu, I.T.; Wong, T.W. Multi-zone modeling of probable SARS virus transmission by airflow between flats in Block E, Amoy Gardens. Indoor Air 2005, 15, 96–111. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Tang, J.W.; Li, Y. Airborne or fomite transmission for norovirus? A case study revisited. Int. J. Env. Res. Public Health 2017, 14, 1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Bi, Y.; Tian, H.; Li, X.; Liu, D.; Wu, Y.; Jin, T.; Wang, Y.; Chen, Q.; Chen, Z.; et al. Human infection with influenza virus A(H10N8) from live poultry markets, China, 2014. Emerging Infect. Dis. 2014, 20, 2076–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, P.; Chan, P.-T.; Gao, Y.; Lai, H.-W.; Zhang, T.; Li, Y. Physical factors that affect microbial transfer during surface touch. Build. Environ. 2019, 158, 28–38. [Google Scholar] [CrossRef]
- Liu, L.; Li, Y.; Nielsen, P.V.; Wei, J.; Jensen, R.L. Short-range airborne transmission of expiratory droplets between two people. Indoor Air 2017, 27, 452–462. [Google Scholar] [CrossRef]
- Marks, P.J.; Vipond, I.B.; Carlisle, D.; Deakin, D.; Fey, R.E.; Caul, E.O. Evidence for airborne transmission of Norwalk-like virus (NLV) in a hotel restaurant. Epidemiol. Infect. 2000, 124, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect virus transmission in cluster of COVID-19 cases, Wenzhou, China, 2020. Emerging Infect. Dis. 2020, 26, 1343–1345. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Wu, T.; Liu, Q.; Ya, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.-Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Li, Y. Transmission of influenza A in a student office based on realistic person-to-person contact and surface touch behaviour. Int. J. Environ. Res. Public Health 2018, 15, 1699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baidu Migration. Available online: http://qianxi.baidu.com (accessed on 14 May 2020).
- Administrative Division. Available online: http://english.www.gov.cn/archive/china_abc/2014/08/27/content_281474983873401.htm (accessed on 14 May 2020).
- Zhang, N.; Su, B.; Chan, P.-T.; Miao, T.; Wang, P.; Li, Y. Infection spread and high-resolution detection of close contact behaviors. Int. J. Environ. Res. Public Health 2020, 17, 1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Jiang, X. Evolving transmission network dynamics of COVID-19 cluster infections in south Korea: A descriptive study. medRxiv 2020, 1, 1–15. [Google Scholar] [CrossRef]
- Department of Urban Survey, National Bureau of Statistics of China. China City Statistical Yearbook—2018; China Academic Journal Electronic Publishing House: Beijing, China, 2018. [Google Scholar]
- Zhang, N.; Huang, H.; Su, B.; Ma, X.; Li, Y. A human behavior integrated hierarchical model of airborne disease transmission in a large city. Build. Environ. 2018, 127, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, S.; Yu, K. COVID-19 infection epidemic: The medical management strategies in Heilongjiang Province, China. Crit. Care 2020, 24, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, Y.; Chen, X.; Shi, W. Impacts of social and economic factors on the transmission of coronavirus disease 2019 (COVID-19) in China. J. Popul. Econ. 2020, 1, 1–46. [Google Scholar] [CrossRef]
- Tian, H.; Liu, Y.; Li, Y.; Wu, C.-H.; Chen, B.; Kraemer, M.U.; Li, B.; Cai, J.; Xu, B.; Yang, Q. An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China. Science 2020, 368, 638–642. [Google Scholar] [CrossRef] [Green Version]
- Nishiura, H.; Oshitani, H.; Kobayashi, T.; Saito, T.; Sunagawa, T.; Matsui, T.; Wakita, T.; COVID, M.; Suzuki, M. Closed environments facilitate secondary transmission of coronavirus disease 2019 (COVID-19). medRxiv 2020, 1, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Qian, H.; Miao, T.; Li, L.; Zheng, X.; Luo, D.; Li, Y. Indoor transmission of SARS-CoV-2. medRxiv 2020, 1, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Bourouiba, L. Turbulent gas clouds and respiratory pathogen emissions: Potential implications for reducing transmission of COVID-19. JAMA 2020, 323, 1837–1838. [Google Scholar] [CrossRef]
- Anzai, A.; Kobayashi, T.; Linton, N.M.; Kinoshita, R.; Hayashi, K.; Suzuki, A.; Yang, Y.; Jung, S.-M.; Miyama, T.; Akhmetzhanov, A.R.; et al. Assessing the impact of reduced travel on exportation dynamics of novel coronavirus infection (COVID-19). J. Clin. Med. 2020, 9, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, S.; Hu, N.; Lou, J.; Chen, K.; Kang, X.; Xiang, Z.; Chen, H.; Wang, D.; Liu, N.; Liu, D.; et al. Characteristics of COVID-19 infection in Beijing. J. Infect. 2020, 80, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, M. Covid-19: Four fifths of cases are asymptomatic, China figures indicate. Br. Med. J. Publ. Group 2020, 369, m1375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVID-19: What Proportion are Asymptomatic? Available online: https://www.cebm.net/covid-19/covid-19-what-proportion-are-asymptomatic/ (accessed on 14 May 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Categories | Infection Locations | Activities Involved |
|---|---|---|---|
| 1 | Home | Estate (own home/relative’s home) | Dining and long-term or repeated household close contacts |
| 2 | Restaurant | Restaurant | Dining |
| 3 | Public vehicles | Traditional train; EMUs; aeroplane; taxi/private car; bus/metro. | Long-term close contacts |
| 4 | Public buildings | Residence (apartment/residential estate/friend’s home); supermarket/market/shop; hotel; hospital; clinic; pharmacy; mall; office; poker/mahjong room | Close contacts |
| 5 | Others | Infection locations cannot be determined | Unknown |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, P.; Zhang, N.; Li, Y. A Comparison of Infection Venues of COVID-19 Case Clusters in Northeast China. Int. J. Environ. Res. Public Health 2020, 17, 3955. https://doi.org/10.3390/ijerph17113955
Zhao P, Zhang N, Li Y. A Comparison of Infection Venues of COVID-19 Case Clusters in Northeast China. International Journal of Environmental Research and Public Health. 2020; 17(11):3955. https://doi.org/10.3390/ijerph17113955
Chicago/Turabian StyleZhao, Pengcheng, Nan Zhang, and Yuguo Li. 2020. "A Comparison of Infection Venues of COVID-19 Case Clusters in Northeast China" International Journal of Environmental Research and Public Health 17, no. 11: 3955. https://doi.org/10.3390/ijerph17113955
APA StyleZhao, P., Zhang, N., & Li, Y. (2020). A Comparison of Infection Venues of COVID-19 Case Clusters in Northeast China. International Journal of Environmental Research and Public Health, 17(11), 3955. https://doi.org/10.3390/ijerph17113955