The Emergence of Risk Communication Networks and the Development of Citizen Health-Related Behaviors during the COVID-19 Pandemic: Social Selection and Contagion Processes


Abstract
:1. Introduction
2. A Theoretical Conjecture on the Dynamics between Risk Communication Networks and Health-Related Behavioral Changes in Pandemic Settings
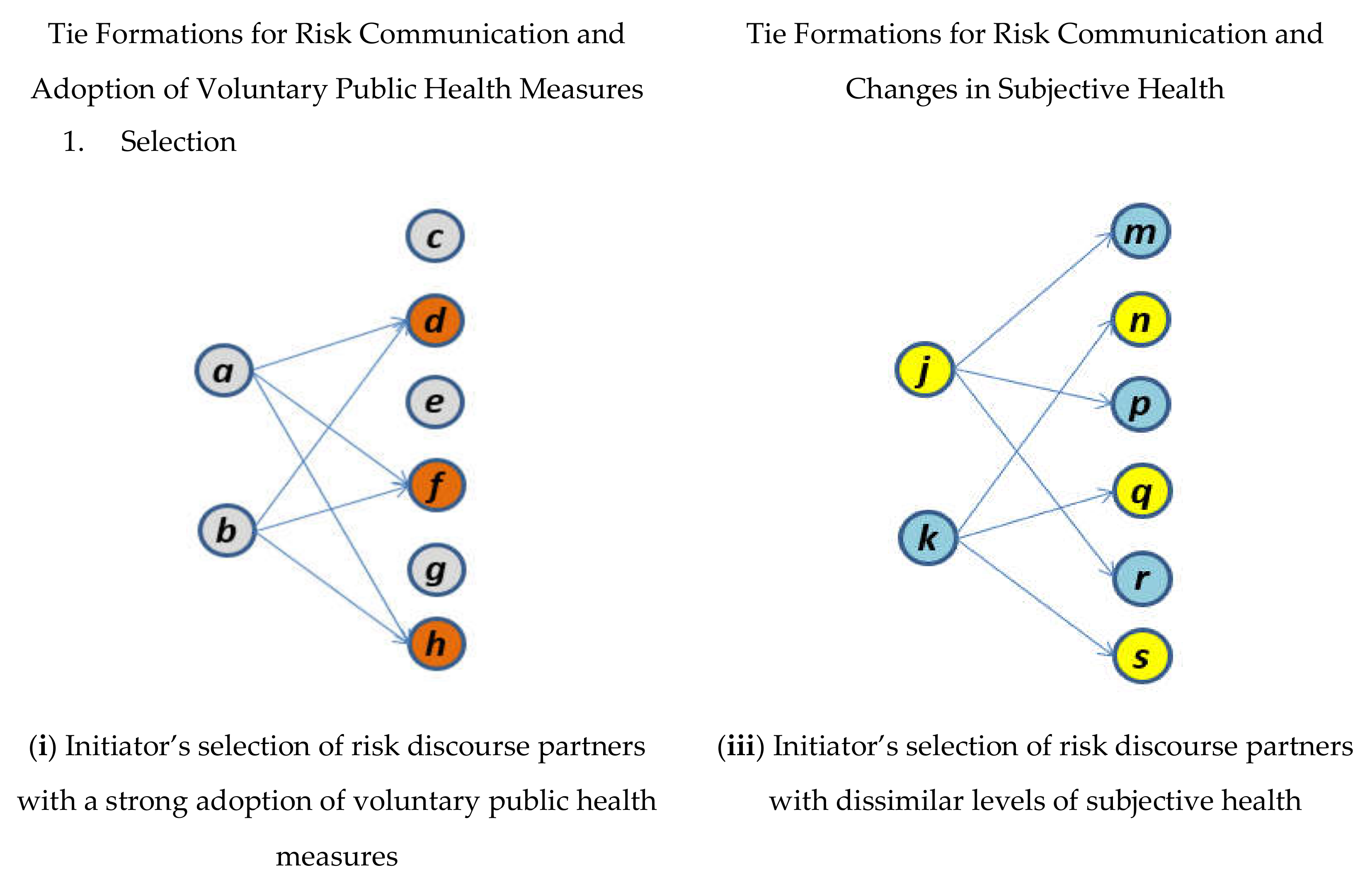
2.1. Risk Communication Network Dynamics
2.1.1. Health-Related Behavior Mechanism (the Selection Effect in the Coevolutionary Process)
Eligibility for and Entitlement to Risk Communication
Homophily
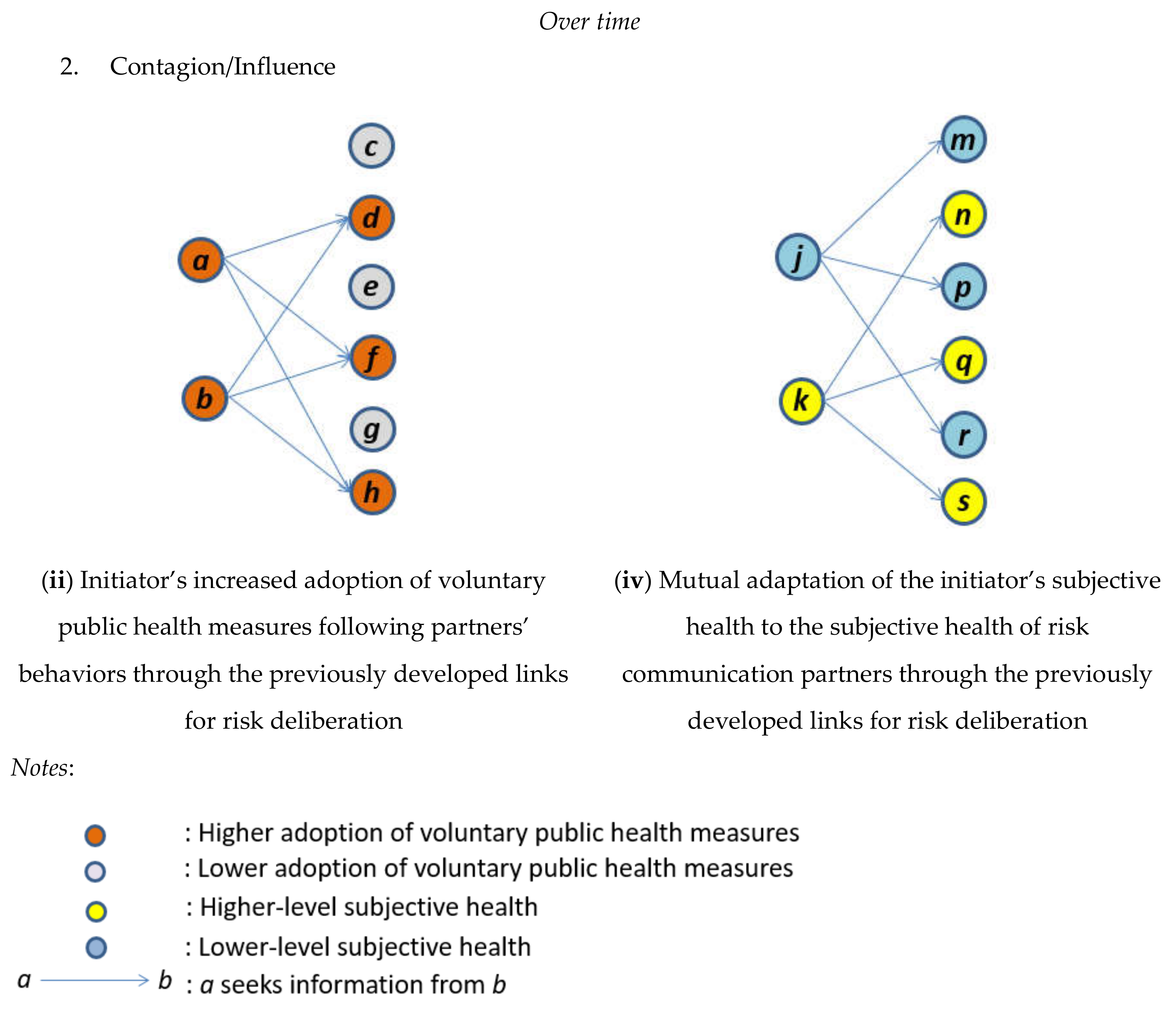
2.2. Health-Related Behavior Dynamics
2.2.1. Structural Mechanisms (the Degree Effect in the Coevolutionary Process)
Approaching Other People
Being Approached by Other People
2.2.2. Associational Mechanisms (the Mutual Adaption/Influence Effect in the Coevolutionary Process)
3. Stochastic Actor-Oriented Model and Data
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Coronavirus Disease 2019 Situation Report-89; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Cori, L.; Bianchi, F.; Cadum, E.; Anthonj, C. Risk perception and COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3114. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Berry, F.S.; Lee, K. Stakeholders in the same bed with different dreams: Semantic network analysis of issue interpretation in risk policy related to mad cow disease. J. Public Adm. Res. Theory 2016, 26, 79–93. [Google Scholar] [CrossRef]
- Allcott, H.; Boxell, L.; Conway, J.; Gentzkow, M.; Thaler, M.; Yang, D.Y. Polarization and Public Health: Partisan Differences in Social Distancing during the Coronavirus Pandemic; NBER Working Paper 2020, No. w26946; NBER: Cambridge, MA, USA, 2020. [Google Scholar]
- Cheung, H. Coronavirus: What Could the West Learn from Asia? Available online: https://www.bbc.com/news/world-asia-51970379 (accessed on 21 March 2020).
- Shaw, R.; Kim, Y.-K.; Hua, J. Governance, technology and citizen behavior in pandemic: Lessons from COVID-19 in East Asia. Prog. Disaster Sci. 2020, 6, 100090. [Google Scholar] [CrossRef]
- Alarcon, R.D. Mental health in a pandemic state: The route from social isolation to loneliness. Available online: https://www.psychiatrictimes.com/coronavirus/mental-health-pandemic-state-route-social-isolation-loneliness (accessed on 25 March 2020).
- Gabbatt, A. Social recession: How isolation can affect physical and mental health. Available online: https://www.theguardian.com/world/2020/mar/18/coronavirus-isolation-social-recession-physical-mental-health (accessed on 18 March 2020).
- National Research Council. Improving Risk Communication; National Academy Press: Washington, DC, USA, 1989. [Google Scholar]
- National Research Council. Understanding Risk: Informing Decisions in a Democratic Society; National Academy Press: Washington, DC, USA, 1996. [Google Scholar]
- Reynolds, B.; Quinn, S.C. Effective communication during an influenza pandemic: The value of using a crisis and emergency risk communication framework. Health Promot. Pract. 2008, 9, 13S–17S. [Google Scholar] [CrossRef] [PubMed]
- Abrams, E.M.; Greenhawt, M. Risk communication during COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 1791–1794. [Google Scholar] [CrossRef] [PubMed]
- Husnayain, A.; Fuad, A.; Su, E.C. Applications of google search trends for risk communication in infectious disease management: A case study of COVID-19 outbreak in Taiwan. Int. J. Infect. Dis. 2020, 95, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Freimuth, V.S.; Jamison, A.; Hancock, G.; Musa, D.; Hilyard, K.; Quinn, S.C. The role of risk perception in flu vaccine behavior among African-American and white adults in the United States. Risk Anal. 2017, 37, 2150–2163. [Google Scholar] [CrossRef] [PubMed]
- Jehn, M.; Kim, Y.; Bradley, B.; Lant, T. Community knowledge, risk perception, and preparedness for the 2009 Influenza A/H1N1 Pandemic. J. Public Health Manag. Pract. 2011, 17, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Ju, Y.; You, M. The effects of social determinants on public health emergency preparedness mediated by health communication: The 2015 MERS outbreak in South Korea. Health Commun. 2019. [Google Scholar] [CrossRef] [PubMed]
- Shalizi, C.R.; Thomas, A.C. Homophily and contagion are generically confounded in observational social network studies. Sociol. Methods Res. 2011, 40, 211–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.; Nakazato, H. Co-evolving supportive networks and perceived community resilience across disaster-damaged areas after the Great East Japan Earthquake: Selection, influence, or both? J. Contin. Crisis Manag. 2019, 27, 116–129. [Google Scholar] [CrossRef]
- McPherson, J.M.; Smith-Lovin, L.; Cook, J.M. Birds of a feather. Annu. Rev. Sociol. 2001, 27, 415–444. [Google Scholar] [CrossRef] [Green Version]
- Leenders, R.T.A.J. Longitudinal behavior of network structure and actor attributes: Modeling interdependence of contagion and selection. In Evolution of Social Networks; Doreian, P., Stokman, F., Eds.; Routledge: Amsterdam, The Netherlands, 1997. [Google Scholar]
- Smith, K.P.; Christakis, N.A. Social networks and health. Annu. Rev. Sociol. 2008, 34, 405–429. [Google Scholar] [CrossRef] [Green Version]
- Steglich, C.E.G.; Snijders, T.A.B.; Pearson, M. Dynamic networks and behavior: Separating selection from influence. Sociol. Methodol. 2010, 40, 329–393. [Google Scholar] [CrossRef]
- Basu, A.; Dutta, M.J. The relationship between health information seeking and community participation: The roles of health information orientation and efficacy. Health Commun. 2008, 23, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Dutta-Bergman, M.J. An alternative approach to social capital: Exploring the linkage between health consciousness and community participation. Health Commun. 2004, 16, 393–409. [Google Scholar] [CrossRef]
- Pfeffer, J.; Salancik, G.R. The External Control of Organizations; Harper and Row: New York, NY, USA, 1978. [Google Scholar]
- Ahn, J.; Chae, D. The influences of socio-individual determinants and health information seeking on health-promoting behaviors among migrant women: A cross-sectional study. Jpn. J. Nurs. Sci. 2019, 16, 481–490. [Google Scholar] [CrossRef]
- Griffin, R.J.; Yang, Z.; Huurne, E.T.; Boerner, F.; Ortiz, S.; Dunwoody, S. After the flood: Anger, attribution, and the seeking of information. Sci. Commun. 2008, 29, 285–315. [Google Scholar] [CrossRef] [Green Version]
- Lagoe, C.; Atkin, D. Health anxiety in the digital age: An exploration of psychological determinants of online health information seeking. Comput. Hum. Behav. 2015, 52, 484–491. [Google Scholar] [CrossRef]
- Centola, D. An experimental study of homophily in the adoption of health behavior. Science 2011, 334, 1269–1272. [Google Scholar] [CrossRef] [PubMed]
- Crook, B.; Stephens, K.K.; Pastorek, A.E.; Mackert, M.; Donovan, E.E. Sharing health information and influencing behavioral intentions: The role of health literacy, information overload, and the Internet in the diffusion of healthy heart information. Health Commun. 2016, 31, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.; Huang, Y.; Tseng, K.; Yen, C.; Yang, L. Social capital and health-protective behavior intentions in an influenza pandemic. PLoS ONE 2015, 10, e0122970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almedom, A.M. Social capital and mental health. Soc. Sci. Med. 2005, 61, 943–964. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Kreps, G.L.; Shin, C. The role of social support and social networks in health information-seeking behavior among Korean Americans. Int. J. Equity Health 2015, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Hanson-Easey, S.; Every, D.; Hansen, A.; Bi, P. Risk communication for new and emerging communities: The contingent role of social capital. Int. J. Disaster Risk Reduct. 2018, 28, 620–628. [Google Scholar] [CrossRef]
- Poortinga, W. Community resilience and health: The role of bonding, bridging, and linking aspects of social capital. Health Place 2012, 18, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Christakis, N.A.; Fowler, J.H. Social contagion theory: Examining dynamic social networks and human behavior. Stat. Med. 2013, 32, 556–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, D.; Golberstein, E.; Whitlock, J.L.; Downs, M.F. Social contagion of mental health: Evidence from college roommates. Health Econ. 2013, 22, 965–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.A.; Zhu, X.; Shartle, K.; Glick, L.; M’ikanatha, N.M. Understanding the public’s intentions to purchase and to persuade others to purchase antibiotic-free meat. Health Commun. 2017, 32, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, H.; Lim, S. Evolutionary process of social capital formation through community currency organizations: The Japanese case. VOLUNTAS Int. J. Volunt. Nonprofit Organ. 2016, 27, 1171–1194. [Google Scholar] [CrossRef]
- Nakazato, H.; Lim, S. Community rebuilding processes in a disaster-damaged area through community currency: The pilot project of “Domo” in Kamaishi, Japan. Disaster Prev. Manag. 2017, 26, 79–93. [Google Scholar] [CrossRef]
- Snijders, T.A.B.; van de Bunt, G.G.; Steglich, C.E.G. Introduction to actor-based models for network dynamics. Soc. Netw. 2010, 32, 44–60. [Google Scholar] [CrossRef]
- Snijders, T.A.B.; Pickup, M. Stochastic actor oriented models for network dynamics. In The Oxford Handbook of Political Networks; Victor, J.N., Montgomery, A.H., Lubell, M., Eds.; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Knoke, D.; Yang, S. Social Network Analysis, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Vaughan, E.; Tinker, T. Effective health risk communication about pandemic influenza for vulnerable populations. Am. J. Public Health 2009, 99, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Gomez, O.A. Lessons from international students’ reaction to the 2011 Great East Japan Earthquake: The case of the School of Engineering at Tohoku University. Int. J. Disaster Risk Sci. 2013, 4, 137–149. [Google Scholar] [CrossRef] [Green Version]
- Takashima, M.; Narita, M.; Oiwa, Y.; Abe, A. Officials plead with young people to stop partying during pandemic. Available online: http://www.asahi.com/ajw/articles/13260124 (accessed on 31 March 2020).
- Ministry of Health, Labour and Welfare. About Coronavirus Disease 2019; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2020. [Google Scholar]
- Goldberg, D.P.; Williams, P. A User’s Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires, 3rd ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Saijo, T. The Stay-at-home advisory as a hawk-dove game. Available online: https://www.tkfd.or.jp/en/research/detail.php?id=743 (accessed on 4 June 2020).
- Jennings, E.T.; Hall, J.L. Evidence-based practice and the use of information in state agency decision making. J. Public Adm. Res. Theory 2012, 22, 245–266. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Coefficients | Standard Error |
|---|---|---|
| Formation of Risk Communication Networks(Effects on Risk Communication Activity): | ||
| 1. Rate of change from t1 to t2 | 4.40 *** | 1.07 |
| 2. Rate of change from t2 to t3 | 3.76 *** | 0.83 |
| 3. Out-degree (density) | −0.94 *** | 0.35 |
| 4. Eligibility for risk communication 1 (effect of partner’s adoption of voluntary public health measures on link formation) | 0.26 ** | 0.13 |
| 5. Entitlement to risk communication 1 (effect of one’s own adoption of voluntary public health measures on link formation) | 0.35 | 0.32 |
| 6. Homophily 1 (partner selection based on similarity in voluntary adoption of public health measures) | 2.43 | 1.90 |
| 7. Eligibility for risk communication 2 (effect of partner’s higher subjective health condition on link formation) | 0.41 | 0.27 |
| 8. Entitlement to risk communication 2 (effect of one’s own higher subjective health condition on link formation) | 0.22 | 0.29 |
| 9. Homophily 2 (partner selection based on similarity in subjective health) | −1.25 ** | 0.63 |
| 10. Reciprocity | 1.54 *** | 0.37 |
| 11. Transitive triplets | 1.06 *** | 0.22 |
| 12. In-degree popularity (sqrt) | −1.39 *** | 0.49 |
| 13. Three cycles | −0.95 ** | 0.46 |
| 14. Same country | 1.06 *** | 0.22 |
| 15. Same gender | 0.35 | 0.22 |
| Development of Health-Related Behaviors 1 (Effects on Voluntary Public Health Measures): | ||
| 16. Rate of change from t1 to t2 | 0.77 *** | 0.28 |
| 17. Rate of change from t2 to t3 | 2.81 ** | 1.38 |
| 18. Linear shape (tendency) | 0.10 | 0.47 |
| 19. Quadratic shape (effect of voluntary public health measures on itself) | 0.01 | 0.11 |
| 20. Effect of one’s own out-degree ties | −0.08 | 0.11 |
| 21. Effect of one’s own in-degree ties | 0.16 | 0.28 |
| 22. Mutual influence (average similarity with partners) | 0.35 ** | 0.17 |
| Development of Health-Related Behaviors 2 (Effects on Subjective Health): | ||
| 23. Rate of change from t1 to t2 | 1.98 | 1.37 |
| 24. Rate of change from t2 to t3 | 0.62 ** | 0.25 |
| 25. Linear shape (tendency) | −0.82 | 1.20 |
| 26. Quadratic shape (effect of subjective health conditions on itself) | −1.04 | 0.82 |
| 27. Effect of one’s own out-degree ties | −0.47 | 0.42 |
| 28. Effect of one’s own in-degree ties | 0.84 | 0.93 |
| 29. Mutual influence (average similarity with partners) | 0.65 * | 0.34 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.; Nakazato, H. The Emergence of Risk Communication Networks and the Development of Citizen Health-Related Behaviors during the COVID-19 Pandemic: Social Selection and Contagion Processes. Int. J. Environ. Res. Public Health 2020, 17, 4148. https://doi.org/10.3390/ijerph17114148
Lim S, Nakazato H. The Emergence of Risk Communication Networks and the Development of Citizen Health-Related Behaviors during the COVID-19 Pandemic: Social Selection and Contagion Processes. International Journal of Environmental Research and Public Health. 2020; 17(11):4148. https://doi.org/10.3390/ijerph17114148
Chicago/Turabian StyleLim, Seunghoo, and Hiromi Nakazato. 2020. "The Emergence of Risk Communication Networks and the Development of Citizen Health-Related Behaviors during the COVID-19 Pandemic: Social Selection and Contagion Processes" International Journal of Environmental Research and Public Health 17, no. 11: 4148. https://doi.org/10.3390/ijerph17114148
APA StyleLim, S., & Nakazato, H. (2020). The Emergence of Risk Communication Networks and the Development of Citizen Health-Related Behaviors during the COVID-19 Pandemic: Social Selection and Contagion Processes. International Journal of Environmental Research and Public Health, 17(11), 4148. https://doi.org/10.3390/ijerph17114148