Longitudinal Analysis of Work-to-Family Conflict and Self-Reported General Health among Working Parents in Germany



Abstract
:1. Introduction
1.1. Work–Family Conflicts and Health
1.2. The Role of Social Determinants
1.3. Contribution and Research Questions
2. Materials and Methods
2.1. Data
2.2. Dependent Variable
2.3. Independent Variable
2.4. Control Variables
2.5. Statistical Analyses
3. Results
3.1. Sample Description
3.2. Work-to-Family Conflicts and Health at T1
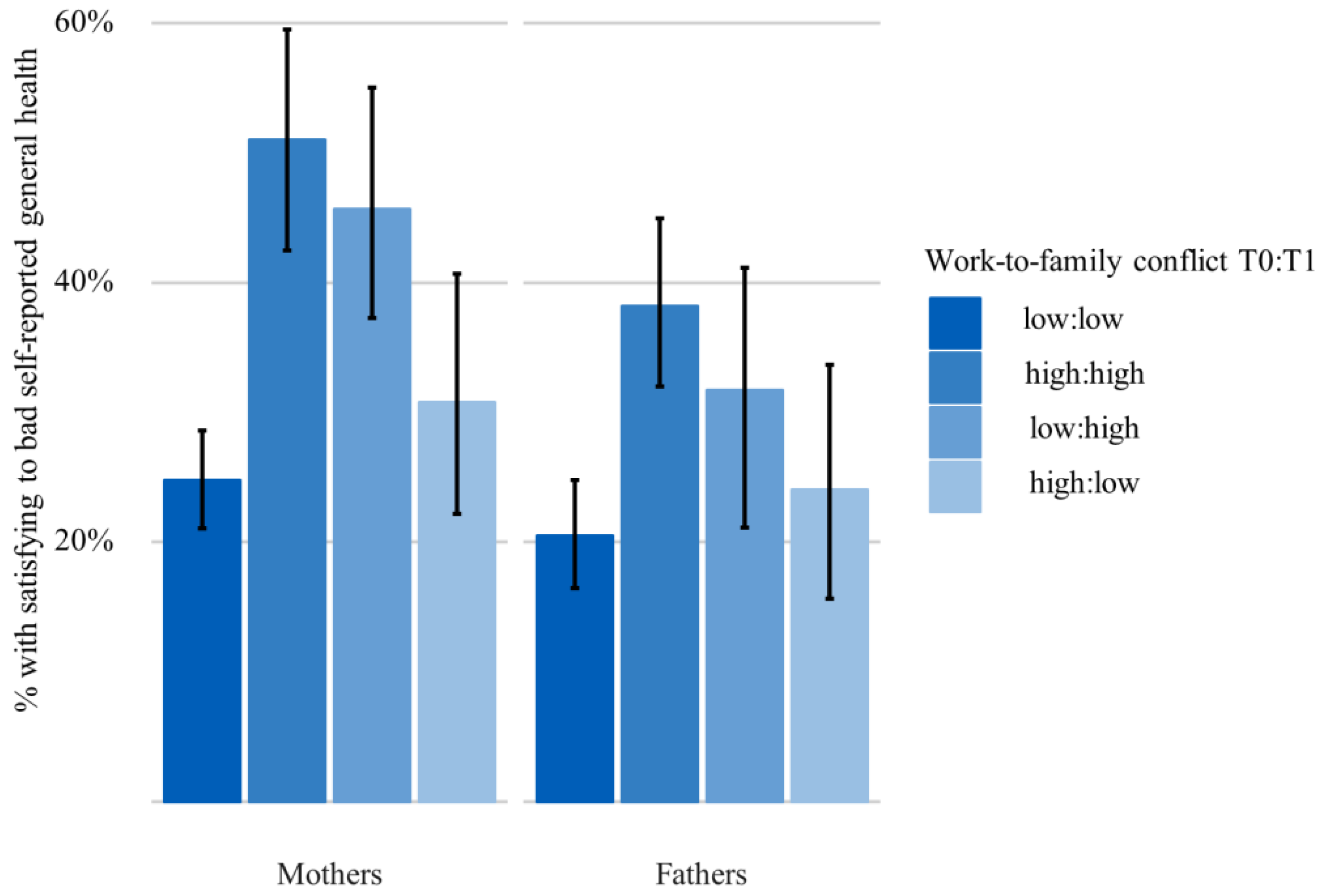
3.3. Work-to-Family Conflicts and Health over Time
3.4. The Role of Education
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gallie, D.; Russell, H. Work-family conflict and working conditions in Western Europe. Soc. Indic. Res. 2009, 93, 445–467. [Google Scholar] [CrossRef]
- McGinnity, F.; Whelan, C.T. Comparing work-life conflict in Europe: Evidence from the European social survey. Soc. Indic. Res. 2009, 93, 433–444. [Google Scholar] [CrossRef]
- OECD. Dare to Share—Deutschlands Weg zur Partnerschaftlichkeit in Familie und Beruf; OECD Publishing: Paris, France, 2017. [Google Scholar]
- German Federal Government. Rechtsanspruch für Unter Dreijährige (Legal Entitlement for Children under Three Years of Age). Available online: https://www.bundesregierung.de/breg-de/themen/rechtsanspruch-fuer-unter-dreijaehrige-413834 (accessed on 30 March 2020).
- Greenhaus, J.H.; Beutell, N. Sources of conflict between work and family roles. Acad. Manag. Rev. 1985, 10, 76–88. [Google Scholar] [CrossRef]
- Eurostat. Employment Rate by Gender, Age Group 15–64. Available online: https://appsso.eurostat.ec.europa.eu/nui/show.do?query=BOOKMARK_DS-053312_QID_-4AAC19A_UID_-3F171EB0&layout=SEX,L,X,0;GEO,L,Y,0;AGE,L,Z,0;UNIT,L,Z,1;TIME,C,Z,2;INDIC_EM,L,Z,3;INDICATORS,C,Z,4;&zSelection=DS-053312INDIC_EM,EMP_LFS;DS-053312AGE,Y15-64;DS-053312TIME,2015;DS-053312UNIT,PC_POP;DS-053312INDICATORS,OBS_FLAG;&rankName1=UNIT_1_2_-1_2&rankName2=AGE_1_2_-1_2&rankName3=INDICATORS_1_2_-1_2&rankName4=INDIC-EM_1_2_-1_2&rankName5=TIME_1_0_0_0&rankName6=SEX_1_2_0_0&rankName7=GEO_1_2_0_1&rStp=&cStp=&rDCh=&cDCh=&rDM=true&cDM=true&footnes=false&empty=false&wai=false&time_mode=ROLLING&time_most_recent=true&cfo=%23%23%23%2C%23%23%23.%23%23%23&lang=en (accessed on 24 May 2020).
- Eurostat. Percentage of Part-Time Employees by Gender, Age Group 15–64. Available online: https://ec.europa.eu/eurostat/databrowser/product/view/TPS00159?lang=en (accessed on 24 May 2020).
- Federal Statistical Office. Average Expected Duration of Paid Parental Leave in Germany 2019. Available online: https://www-genesis.destatis.de/genesis/online?operation=abruftabelleBearbeiten&levelindex=1&levelid=1590412587419&auswahloperation=abruftabelleAuspraegungAuswaehlen&auswahlverzeichnis=ordnungsstruktur&auswahlziel=werteabruf&code=22922-0109&auswahltext=&werteabruf=Werteabruf#astructure (accessed on 25 May 2020).
- Federal Statistical Office. Children under 3 Years of Age in Institutional Childcare on 1 March 2019 in Germany. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2019/09/PD19_379_225.html (accessed on 25 May 2020).
- German Federation of Trade Unions. DGB-Index Gute Arbeit (DGB Index Good Work). Available online: http://index-gute-arbeit.dgb.de/++co++614dfaea-bee1-11e7-98bf-52540088cada (accessed on 30 March 2020).
- Korpi, W.; Ferrarini, T.; Englund, S. Women’s opportunities under different family policy constellations: Gender, class, and inequality tradeoffs in western countries re-examined. Soc. Politics 2013, 20, 1–40. [Google Scholar] [CrossRef]
- Federal Agency for Civic Education. Erwerbstätigenquoten nach Bildungsstand (Employment Rates by Educational Level). Available online: http://www.bpb.de/nachschlagen/zahlen-und-fakten/europa/70590/erwerbstaetigkeit-nach-bildung (accessed on 30 March 2020).
- Pearlin, L.I.; Menaghan, E.G.; Lieberman, M.A.; Mullan, J.T. The Stress Process. J. Health Soc. Behav. 1981, 22, 337–356. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Schieman, S.; Fazio, E.M.; Meersman, S.C. Stress, Health, and the life course: Some conceptual perspectives. J. Health Soc. Behav. 2005, 46, 205–219. [Google Scholar] [CrossRef]
- Borgmann, L.-S.; Rattay, P.; Lampert, T. Health-related consequences of work-family conflict from a european perspective: Results of a scoping review. Front. Public Health 2019, 7, 189. [Google Scholar] [CrossRef] [Green Version]
- Greenhaus, J.H.; Allen, T.D.; Spector, P.E. Health Consequences of Work-Family Conflict: The Dark Side of the Work-Family Interface. In Employee Health, Coping and Methodologies, 1st ed.; Perrewé, P.L., Ganster, D.C., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2006; pp. 61–98. [Google Scholar]
- Allen, T.D.; Herst, D.; Bruck, C.; Sutton, M. Consequences associated with work-to-family conflict: A review and agenda for future research. J. Occup. Health Psychol. 2000, 5, 278–308. [Google Scholar] [CrossRef]
- Grzywacz, J.G.; Smith, A.M. Work-family conflict and health among working parents: Potential linkages for family studies and social neuroscience. J. Fam. Rel. 2016, 65, 176–190. [Google Scholar] [CrossRef] [Green Version]
- Cullati, S. The influence of work-family conflict trajectories on self-rated health trajectories in Switzerland: A life course approach. Soc. Sci. Med. 2014, 113, 23–33. [Google Scholar] [CrossRef]
- Leineweber, C.; Baltzer, M.; Magnusson Hanson, L.L.; Westerlund, H. Work-family conflict and health in swedish working women and Men: A 2-year prospective analysis. Eur. J. Public Health 2013, 23, 710–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.T. A two wave cross-lagged study of work-role conflict, work-family conflict and emotional exhaustion. Scan. J. Psychol. 2016, 57, 591–600. [Google Scholar] [CrossRef]
- Neto, M.; Carvalho, V.S.; Chambel, M.J.; Manuel, S.; Pereira, M.J.; de Fátima, R.M. Work-family conflict and employee well-being over time. The loss spiral effect. J. Occup. Environ. Med. 2016, 58, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, U.; Geurts, S.; Mauno, S. Work-to-family conflict and its relationship with satisfaction and well-being: A one-year longitudinal study on gender differences. Work Stress 2004, 18, 1–22. [Google Scholar] [CrossRef]
- Rantanen, J.; Kinnunen, U.; Feldt, T.; Pulkkinen, L. Work-family conflict and psychological well-being: Stability and cross-lagged relations within one- and six-year follow-ups. J. Vocat. Behav. 2008, 73, 37–51. [Google Scholar] [CrossRef]
- du Prel, J.-B.; Peter, R. Work–family conflict as a mediator in the association between work stress and depressive symptoms: Cross-sectional evidence from the German lidA-cohort study. Int. Arch. Occup. Environ. Health 2015, 88, 359–368. [Google Scholar] [CrossRef]
- Yucel, D.; Fan, W. Work–family conflict and well-being among German couples: A longitudinal and dyadic approach. J. Health Soc. Behav. 2019, 60, 377–395. [Google Scholar] [CrossRef]
- Höge, T. When work strain transcends psychological boundaries: An inquiry into the relationship between time pressure, irritation, work–family conflict and psychosomatic complaints. Stress Health 2009, 25, 41–51. [Google Scholar] [CrossRef]
- Hagqvist, E.; Gådin, K.G.; Nordenmark, M. Work–family conflict and well-being across Europe: The role of gender context. Soc. Indic. Res. 2017, 132, 785–797. [Google Scholar] [CrossRef]
- Frone, M.R.; Russell, M.; Barnes, G.M. Work-family conflict, gender, and health-related outcomes: A study of employed parents in two community samples. J. Occup. Health Psychol. 1996, 1, 57–69. [Google Scholar] [CrossRef]
- Amstad, F.T.; Meier, L.L.; Fasel, U.; Elfering, A.; Semmer, N.K. A meta-analysis of work–family conflict and various outcomes with a special emphasis on cross-domain versus matching-domain relations. J. Occup. Health Psychol. 2011, 16, 151–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianchi, S.M.; Milkie, M.A. Work and family research in the first decade of the 21st century. J. Marriage Fam. 2010, 72, 705–725. [Google Scholar] [CrossRef]
- Kobayashi, T.; Honjo, K.; Eshak, E.S.; Isa, H.; Sawada, N.; Tsugane, S. Work-family conflict and self-rated health among japanese workers: How household income modifies associations. PLoS ONE 2017, 12, e0169903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolte, G.; Lahn, U. Geschlecht in der Public-Health-Forschung zu gesundheitlichen Ungleichheiten: Potenziale und Begrenzungen des Intersektionalitätsansatzes (Gender in public health research on health inequalities: Potentials and limitations of an intersectionality approach). GENDER 2015, 7, 51–67. [Google Scholar] [CrossRef] [Green Version]
- Pöge, K.; Rommel, A.; Mena, E.; Holmberg, C.; Sass, A.C.; Bolte, G. AdvanceGender—Verbundprojekt für eine geschlechtersensible und intersektionale Forschung und Gesundheitsberichterstattung (Advance Gender—Joint project for sex/gender-sensitive and intersectional research and health reporting). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2019, 62, 102–107. [Google Scholar] [CrossRef]
- Brüderl, J.; Drobnič, S.; Hank, K.; Nauck, B.; Neyer, F.J.; Walper, S.; Alt, P.; Bozoyan, C.; Buhr, P.; Finn, C.; et al. The German Family Panel (pairfam). GESIS Data Archive, Cologne. ZA5678 Data File Version 10.0.0. 2019. [Google Scholar] [CrossRef]
- Huinik, J.; Brüderl, J.; Nauck, B.; Walper, S.; Castiglioni, L.; Feldhaus, M. Panel analysis of intimate relationships and family dynamics (pairfam): Conceptual framework and design. Zeitschrift für Familienforschung 2011, 23, 77–100. [Google Scholar]
- Lampert, T.; Schmidtke, C.; Borgmann, L.-S.; Poethko-Müller, C.; Kuntz, B. The subjective health of adults in German. J. Health Monit. 2018, 3, 61–68. [Google Scholar]
- Borgmann, L.-S.; Kroll, L.E.; Müters, S.; Rattay, P.; Lampert, T. Work-family conflict, self-reported general health and work-family reconciliation policies in Europe: Results from the European working conditions survey 2015. SSM Popul. Health 2019, 9, 100465. [Google Scholar] [CrossRef]
- Finnäs, F.; Nyqvist, F.; Saarela, J. Some methodological remarks on self-rated health. Open Publ. Health J. 2008, 1, 32–39. [Google Scholar] [CrossRef]
- Thönnissen, C.; Wilhelm, B.; Alt, P.; Fiedrich, S.; Walper, S. Pairfam Scales and Instruments Manual Waves 1–8. 2016. Available online: https://www.pairfam.de/fileadmin/user_upload/redakteur/publis/Dokumentation/Manuals/Scales_Manual_pairfam_8.0.pdf (accessed on 30 March 2020).
- Carlson, D.; Grzywacz, J. Reflections and Future Directions on Measurement in Work-Family Research. In Handbook of Work-Family Integration Research, Theory, and Best Practices, 1st ed.; Korabik, K., Lero, D., Whitehead, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2008; pp. 57–73. [Google Scholar]
- Wolff, H.-G.; Höge, T. Konflikte zwischen Arbeit und Familie. Eine deutschsprachige Adaptation der mehrdimensionalen Skala von Carlson, Kacmar und Williams (Conflicts between work and family. A German adaption of the multidimensional scale by Carlson, Kacmar, and Williams). Zeitschrift für Arbeits-und Organisationspsychologie A&O 2011, 55, 143–152. [Google Scholar]
- Greenland, S.; Poole, C. Problems in common interpretations of statistics in scientific articles, expert reports, and testimony. Jurimetrics 2011, 51, 113–129. [Google Scholar]
- Greenland, S.; Senn, S.J.; Rothman, K.J.; Carlin, J.B.; Poole, C.; Goodman, S.N.; Altman, D.G. Statistical tests, p values, confidence intervals, and power: A guide to misinterpretations. Eur. J. Epidemiol. 2016, 31, 337–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oshio, T.; Inoue, A.; Tsutsumi, A. Does work-to-family conflict really matter for health? Cross-sectional, prospective cohort and fixed-effects analyses. Soc. Sci. Med. 2017, 175, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Casper, W.J.; De Hauw, S.; Wayne, J.H. Concepts and Measures in the Work-Family Interface: Implications for Work-Family Integration. In Handbook of Work-Life Integration among Professionals Challenges and Opportunities, 1st ed.; Major, D.A., Burke, R.J., Eds.; Edward Elgar: Cheltenham, UK; Northampton, MA, USA, 2013; pp. 35–57. [Google Scholar]
- Greenhaus, J.H.; Allen, T.D. Work-Family Balance: A Review and Extension of the Literature. In Handbook of Occupational Health Psychology, 2nd ed.; Quick, J., Tetrick, L., Eds.; American Psychological Association: Washington, DC, USA, 2011; pp. 165–183. [Google Scholar]
- Lavassani, K.M.; Movahedi, B. Developments in theories and measures of work-family relationships: From conflict to balance. Contemp. Res. Organ. Admin. 2014, 2, 6–19. [Google Scholar]
- McNall, L.A.; Nicklin, J.M.; Masuda, A.D. A meta-analytic review of the consequences associated with work-family enrichment. J. Bus. Psychol. 2010, 25, 381–396. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Mothers | Fathers | Total | ||
|---|---|---|---|---|---|
| Low WTFC (n = 532) | High WTFC (n = 259) | Low WTFC (n = 429) | High WTFC (n = 294) | n = 1514 | |
| Self-Reported General Health | |||||
| Good to very good | 395 (74.2%) | 133 (51.4%) | 338 (78.8%) | 187 (63.6%) | 1053 (69.6%) |
| Satisfying to bad | 137 (25.8%) | 126 (48.6%) | 91 (21.2%) | 107 (36.4%) | 461 (30.4%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Age Group | |||||
| 18–35 | 153 (28.8%) | 73 (28.2%) | 139 (32.4%) | 81(27.6%) | 446 (29.5%) |
| 36–45 | 379 (71.2%) | 186 (71.8%) | 290 (67.6%) | 213 (72.4%) | 1068 (70.5%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Area of Residence | |||||
| West Germany | 340 (63.9%) | 158 (61.0%) | 263 (61.3%) | 186 (63.3%) | 947(62.5%) |
| East Germany | 192 (36.1%) | 101 (39.0%) | 166 (38.7%) | 108 (36.7%) | 567 (37.5%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Net Household Income | |||||
| High | 122 (25.4%) | 76 (32.6%) | 118 (28.9%) | 85 (31.0%) | 401 (28.7%) |
| Middle/low | 359 (74.6%) | 157 (67.4%) | 291 (71.1%) | 189 (69.0%) | 996 (71.3%) |
| Missing | 51 | 26 | 20 | 20 | 117 |
| Education (Highest Vocational Degree) | |||||
| High | 211 (39.7%) | 120 (46.3%) | 186 (43.4%) | 145 (49.3%) | 662 (43.7%) |
| Middle/low | 321 (60.3%) | 139 (53.7%) | 243 (56.6%) | 149 (50.7%) | 852 (56.3%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Number of Children Under 18 Living in Household | |||||
| 1 | 178 (33.5%) | 101 (39.0%) | 131 (30.5%) | 70(23.8%) | 480 (31.7%) |
| 2 | 276 (51.9%) | 130 (50.2%) | 221 (51.5%) | 160 (54.4%) | 787 (52.0%) |
| >2 | 78 (14.7%) | 28 (10.8%) | 77 (17.9%) | 64 (21.8%) | 247 (16.3%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Age of the Youngest Child | |||||
| 0–4 | 51 (9.6%) | 32 (12.4%) | 149 (34.7%) | 88(29.9%) | 320 (21.1%) |
| 5–13 | 358 (67.3%) | 166 (64.1%) | 231 (53.8%) | 169 (57.5%) | 924 (61.0%) |
| 14–17 | 123 (23.1%) | 61 (23.6%) | 49 (11.4%) | 37 (12.6%) | 270 (17.8%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Marital Status | |||||
| Never married | 85 (16.0%) | 43 (16.7%) | 47 (11.0%) | 25 (8.5%) | 200 (13.2%) |
| Married/civil union | 385 (72.4%) | 182 (70.8%) | 362 (84.4%) | 257 (87.7%) | 1186 (78.5%) |
| Divorced/widowed | 62 (11.7%) | 32 (12.5%) | 20 (4.7%) | 11 (3.8%) | 125 (8.3%) |
| Missing | 0 | 2 | 0 | 1 | 3 |
| Partner Living in Household | |||||
| No | 100 (18.8%) | 41 (15.8%) | 19 (4.4%) | 10 (3.4%) | 170 (11.2%) |
| Yes | 432 (81.2%) | 218 (84.2%) | 410 (95.6%) | 284 (96.6%) | 1344 (88.8%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Division of Labor Between Anchor Person and Partner in Childcare | |||||
| Anchor person | 355 (68.3%) | 155 (61.5%) | 28 (6.6%) | 16 (5.5%) | 384 (25.8%) |
| 50/50 | 162 (31.2%) | 86 (34.1%) | 174 (41.0%) | 89 (30.5%) | 511 (34.3%) |
| Partner | 3 (0.6%) | 11 (4.4%) | 222 (52.4%) | 187 (64.0%) | 423 (28.4%) |
| Missing | 12 | 7 | 5 | 2 | 26 |
| Employment Status | |||||
| Full time | 147 (27.6%) | 113 (43.6%) | 379 (88.3%) | 242 (82.3%) | 881 (58.2%) |
| Part time | 331 (62.2%) | 120 (46.3%) | 12 (2.8%) | 7 (2.4%) | 470 (31.0%) |
| Self employed | 54 (10.2%) | 26 (10.0%) | 38 (8.9%) | 45 (15.3%) | 163 (10.8%) |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Shiftwork | |||||
| No shiftwork | 432 (81.4%) | 186 (71.8%) | 336 (78.5%) | 235 (79.9%) | 1189 (78.6%) |
| Shiftwork | 99 (18.6%) | 73 (28.2%) | 92 (21.5%) | 59 (20.1%) | 323 (21.4%) |
| Missing | 1 | 0 | 1 | 0 | 2 |
| Employment Status of Partner | |||||
| Not working | 16 (3.2%) | 13 (5.2%) | 98 (23.5%) | 66 (22.9%) | 193 (13.3%) |
| Full time/self employed | 396 (80.0%) | 191 (76.7%) | 129 (30.9%) | 89 (30.9%) | 805 (55.6%) |
| Part-time | 19 (3.8%) | 14 (5.6%) | 179 (42.9%) | 128 (44.4%) | 340 (23.5%) |
| No partner in household | 64 (12.9%) | 31 (12.4%) | 11 (2.6%) | 5 (1.7%) | 111 (7.7%) |
| Missing | 37 | 10 | 12 | 6 | 65 |
| WTFC T0:T1 | Crude Model | Health at T0 | Socio-Demographics | Family Characteristics | Work Characteristics | Full Model |
|---|---|---|---|---|---|---|
| (0) | (1) | (2) | (3) | (4) | (5) | |
| n | 791 | 791 | 714 | 770 | 743 | 653 |
| WTFC T0:T1 | ||||||
| Low:Low | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| High:High | 3.23 | 2.80 | 3.24 | 2.95 | 2.54 | 2.94 |
| (2.17, 4.80) | (1.86, 4.22) | (2.09, 5.05) | (1.92, 4.53) | (1.65, 3.92) | (1.81, 4.80) | |
| Low:High | 2.54 | 2.38 | 2.44 | 2.34 | 2.10 | 2.13 |
| (1.67, 3.87) | (1.54, 3.68) | (1.54, 3.88) | (1.48, 3.69) | (1.39, 3.44) | (1.29, 3.51) | |
| High:Low | 1.38 | 1.25 | 1.28 | 1.28 | 1.01 | 1.03 |
| (0.82, 2.31) | (0.72, 2.11) | (0.72, 2.23) | (0.72, 2.21) | (0.56, 1.78) | (0.54, 1.89) | |
| AIC | 974.64 | 930.12 | 839.23 | 906.63 | 888.59 | 786.98 |
| WTFC T0:T1 | Crude Model | Health at T0 | Socio-Demographics | Family Characteristics | Work Characteristics | Full Model |
|---|---|---|---|---|---|---|
| (0) | (1) | (2) | (3) | (4) | (5) | |
| n | 723 | 723 | 683 | 715 | 705 | 661 |
| WTFC T0:T1 | ||||||
| Low:Low | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| High:High | 2.39 | 2.03 | 2.15 | 2.05 | 2.14 | 2.21 |
| (1.63, 3.51) | (1.36, 3.02) | (1.41, 3.27) | (1.37, 3.09) | (1.42, 3.23) | (1.42, 3.45) | |
| Low:High | 1.81 | 1.78 | 1.84 | 1.91 | 1.84 | 1.96 |
| (1.07, 3.07) | (1.03, 3.04) | (1.04, 3.19) | (1.09, 3.29) | (1.05, 3.17) | (1.09 3.47) | |
| High:Low | 1.22 | 1.01 | 1.11 | 1.03 | 1.04 | 1.11 |
| (0.69, 2.15) | (0.55, 1.79) | (0.59, 2.02) | (0.55, 1.84) | (0.55, 1.88) | (0.57, 2.07) | |
| AIC | 836.30 | 803.81 | 749.90 | 810.51 | 791.94 | 746.98 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borgmann, L.-S.; Rattay, P.; Lampert, T. Longitudinal Analysis of Work-to-Family Conflict and Self-Reported General Health among Working Parents in Germany. Int. J. Environ. Res. Public Health 2020, 17, 3966. https://doi.org/10.3390/ijerph17113966
Borgmann L-S, Rattay P, Lampert T. Longitudinal Analysis of Work-to-Family Conflict and Self-Reported General Health among Working Parents in Germany. International Journal of Environmental Research and Public Health. 2020; 17(11):3966. https://doi.org/10.3390/ijerph17113966
Chicago/Turabian StyleBorgmann, Lea-Sophie, Petra Rattay, and Thomas Lampert. 2020. "Longitudinal Analysis of Work-to-Family Conflict and Self-Reported General Health among Working Parents in Germany" International Journal of Environmental Research and Public Health 17, no. 11: 3966. https://doi.org/10.3390/ijerph17113966
APA StyleBorgmann, L. -S., Rattay, P., & Lampert, T. (2020). Longitudinal Analysis of Work-to-Family Conflict and Self-Reported General Health among Working Parents in Germany. International Journal of Environmental Research and Public Health, 17(11), 3966. https://doi.org/10.3390/ijerph17113966