How to Defend COVID-19 in Taiwan? Talk about People’s Disease Awareness, Attitudes, Behaviors and the Impact of Physical and Mental Health




Abstract
:
1. Introduction
2. Methods and Instruments
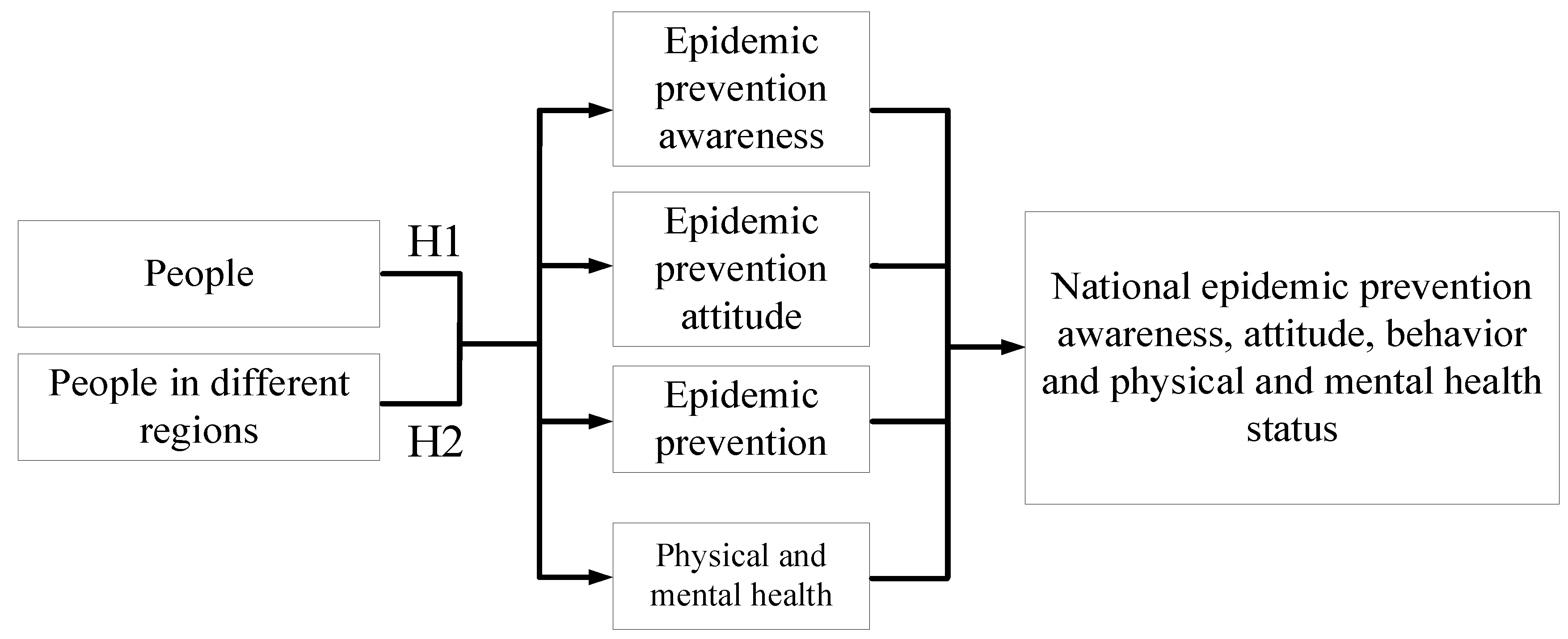
2.1. Study Framework and Hypotheses
2.2. Study Procedure and Instruments
2.3. Study Scope and Limitations
3. Analysis of Results
3.1. Demographics
3.2. Analysis of Awareness, Attitudes, and Behaviors in Relation to Epidemic Prevention among Taiwanese Nationals and of Their Physical and Mental Health Statuses
3.3. Analysis of Awareness, Attitudes, and Behaviors in Relation to COVID-19 Prevention among Citizens in Various Regions and of their Physical–Mental Health
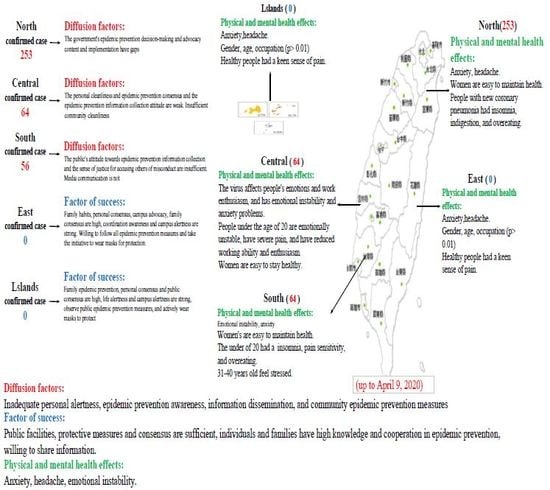
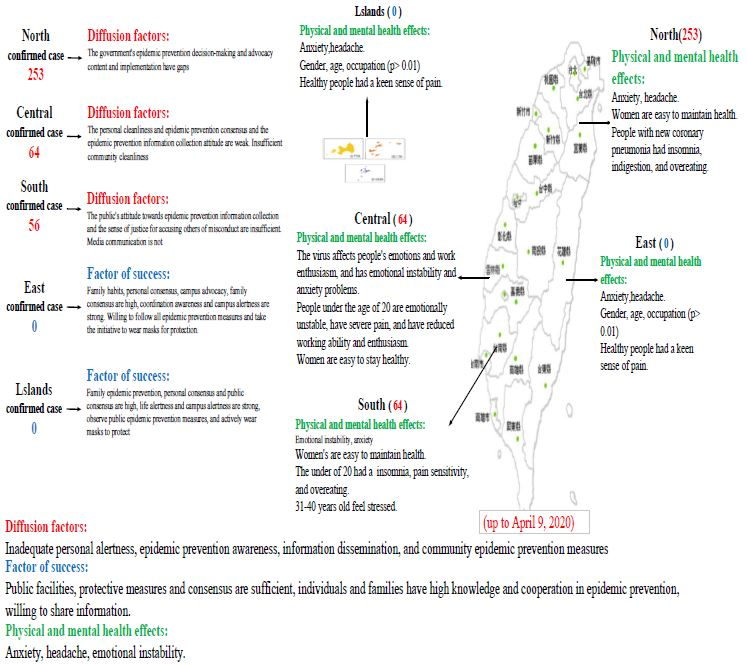
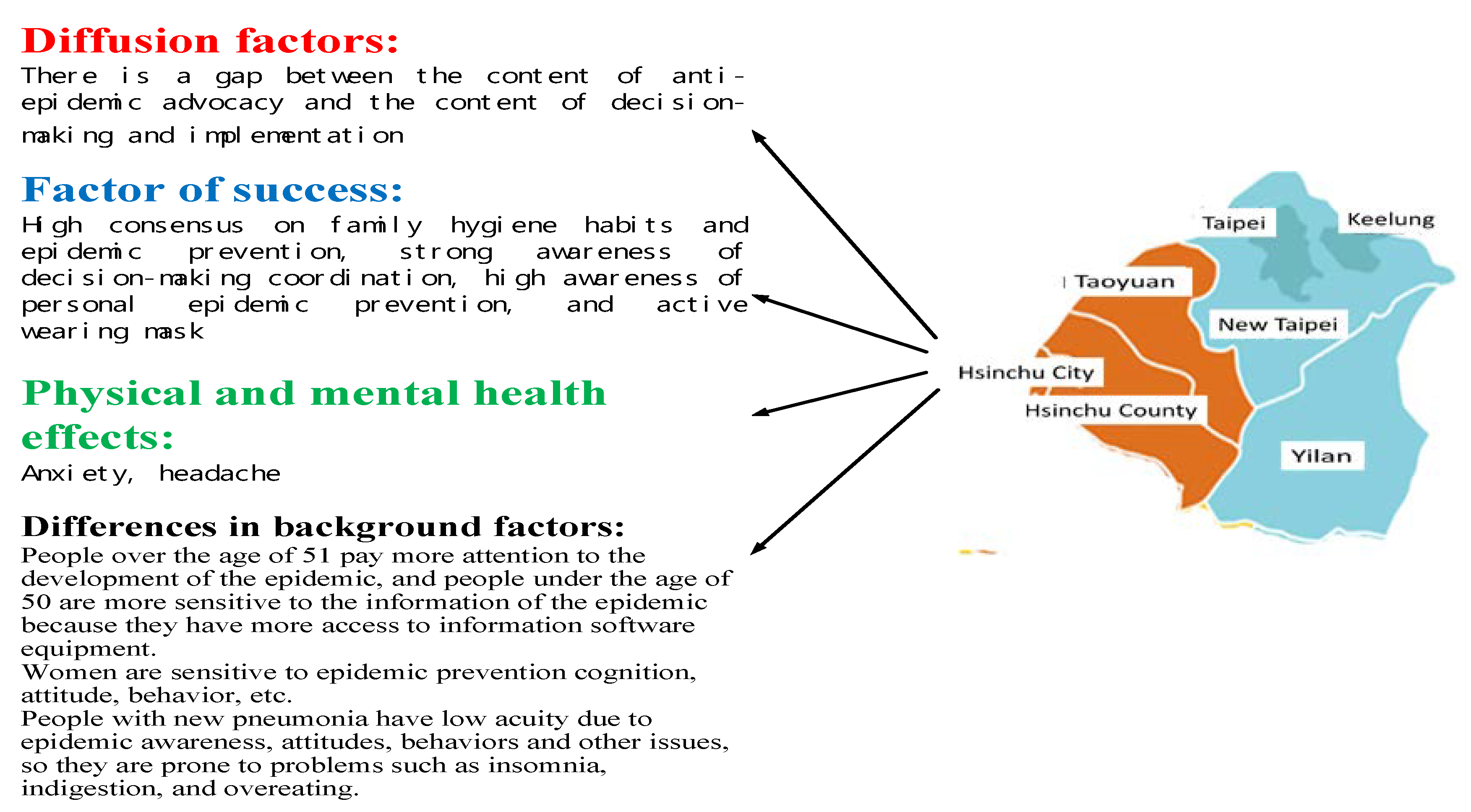
3.3.1. Northern Area
3.3.2. Central Area
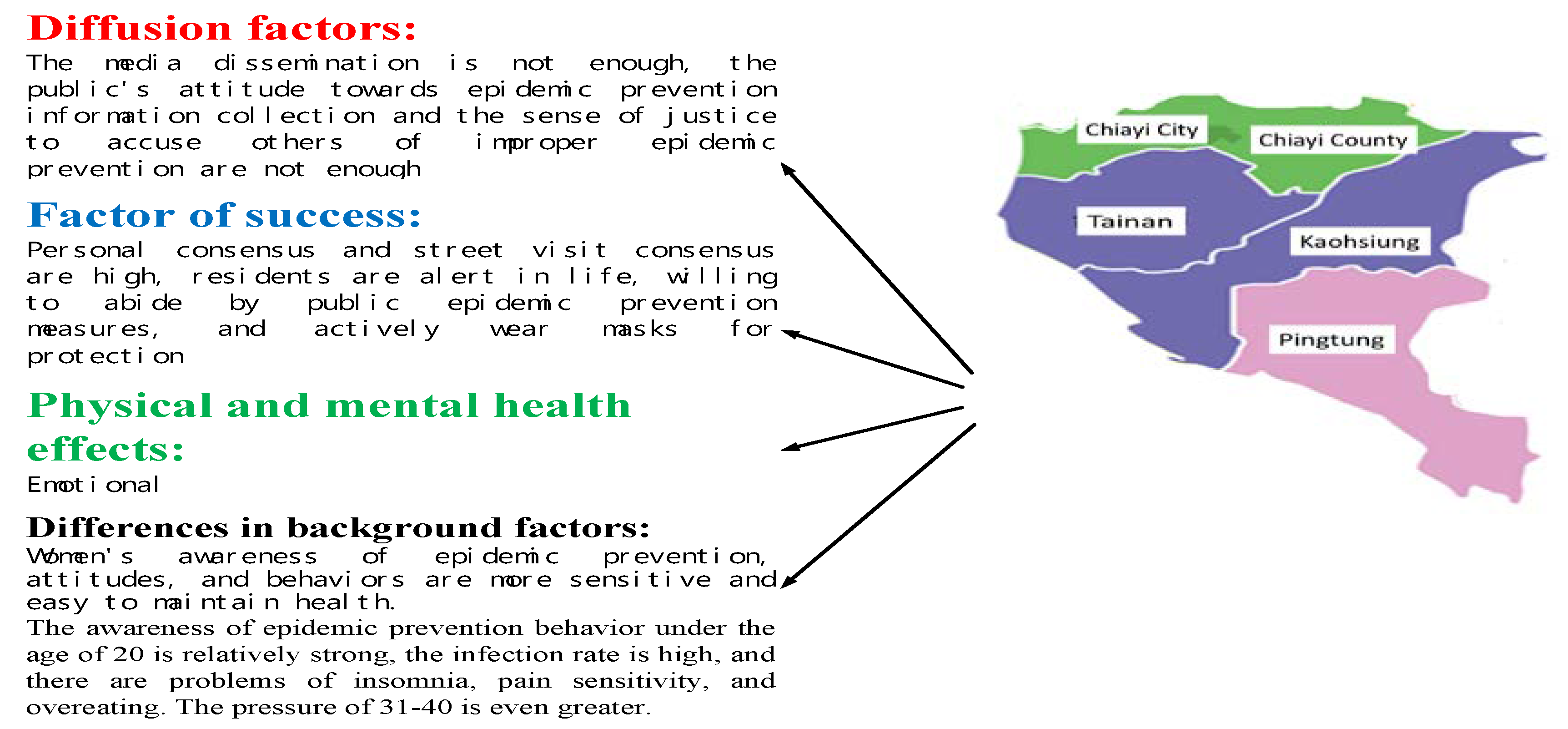
3.3.3. South Area
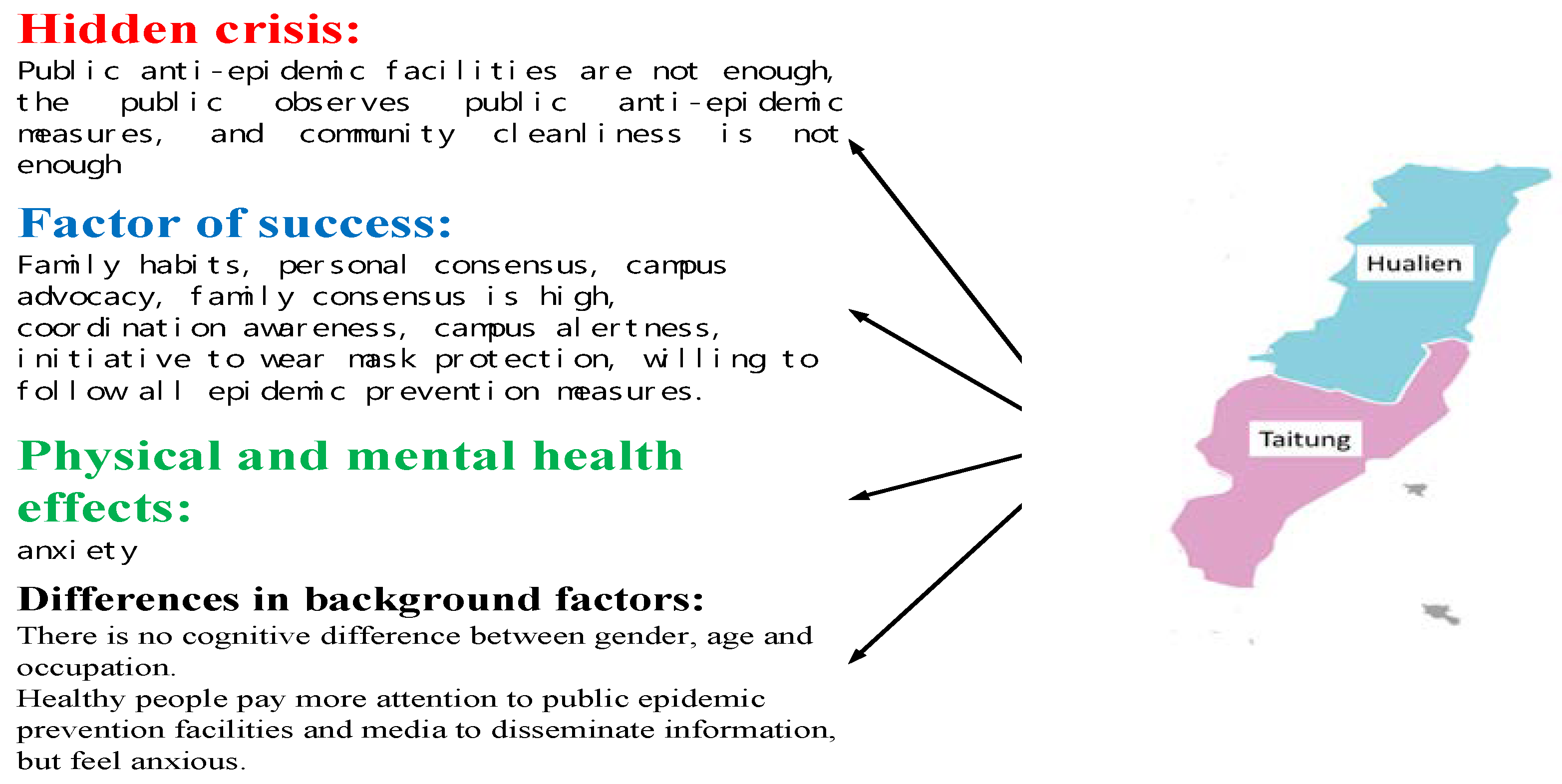
3.3.4. East Area
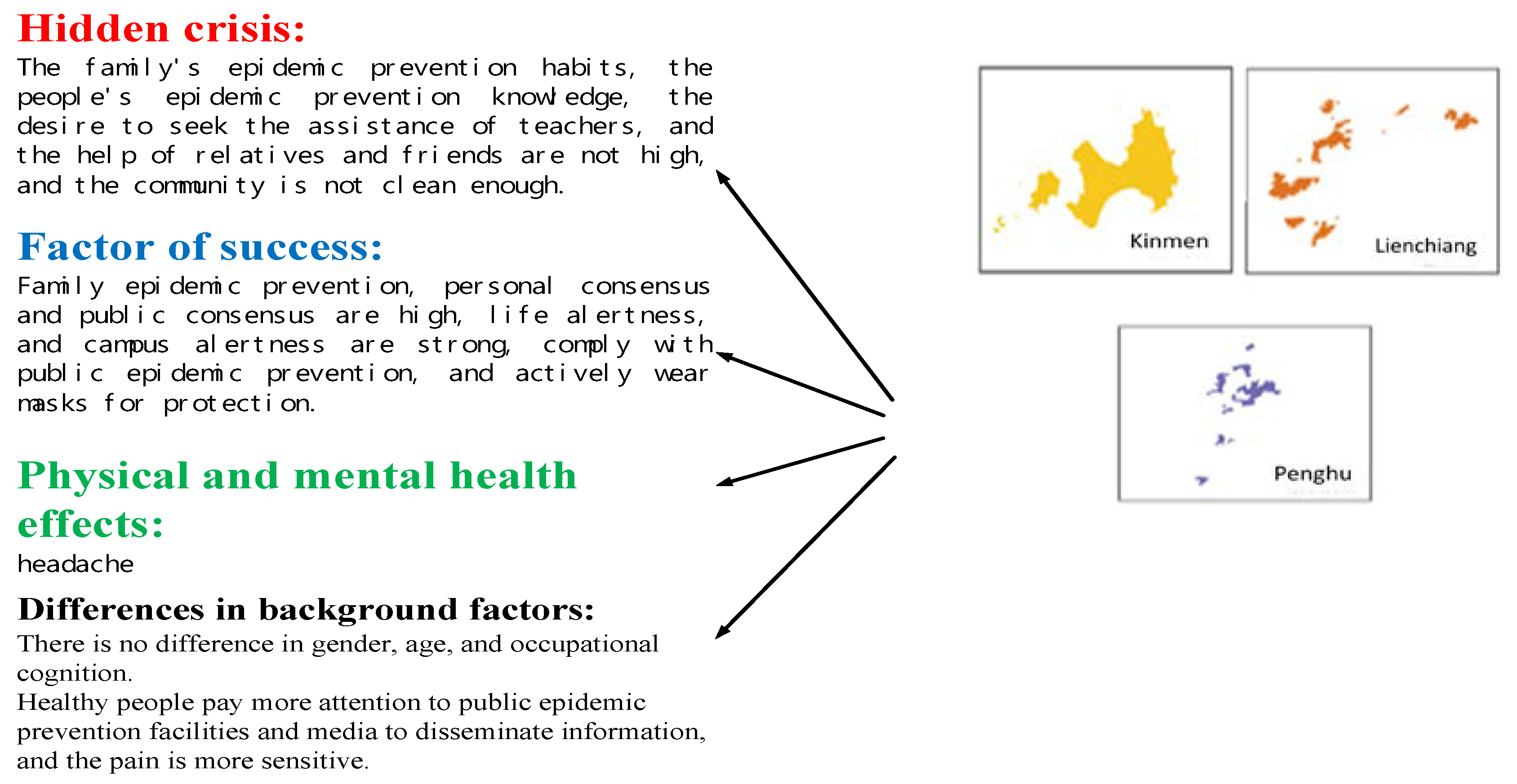
3.3.5. Offshore Islands
4. Conclusions and Recommendations
- (1)
- Recommendations for Epidemic PreventionUse mass media to convey correct epidemic prevention measures and information. Reinforce personal health habits and encourage people to remind and supervise each other on their habits. Reinforce the execution of administrative decisions in Northern Taiwan. Improve environmental cleanliness in Central Taiwan. Strengthen epidemic prevention consensus in Southern Taiwan. Increase the number of public epidemic prevention facilities in Eastern Taiwan. Last, change the attitudes of offshore island residents in addressing epidemic-related crises.
- (2)
- Research SuggestionsFurther explore awareness, attitudes, and behaviors in relation to epidemic prevention among citizens living in various cities and counties along with their physical and mental health based on spatial factors or numbers of confirmed cases;the effects of demographics and behaviors on epidemic prevention awareness, attitudes, and behaviors and on physical and mental health among individuals; and the effects of various exercising behaviors and health habits on people’s resistance to COVID-19; the effects of the COVID-19 pandemic on various industries.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Health Service Commission of the PRC. The Latest Situation of the New Coronavirus Pneumonia Epidemic at 24 O’clock on 8 April 2020. Available online: http://www.nhc.gov.cn/xcs/yqtb/list_gzbd.shtml (accessed on 9 April 2020).
- Tencent New. New Coronavirus Pneumonia Epidemic Situation Follow-up Report. Available online: https://news.qq.com/zt2020/page/feiyan.htm (accessed on 9 April 2020).
- WHO. Coronavirus Disease (COVID-19) Pandemic-Outbreaks and Crises. Available online: http://www.who.int/ (accessed on 9 April 2020).
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Liu, Y.; A Gayle, A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report–67. Available online: http://apps.who.int/iris/bitstream/handle/10665/331613/nCoVsitrep27Mar2020-eng.pdf (accessed on 9 April 2020).
- McKibbin, W.J.; Fernando, R. The Global Macroeconomic Impacts of COVID-19: Seven Scenarios. SSRN Electron. J. 2020, 19, 1–45. [Google Scholar] [CrossRef] [Green Version]
- Taiwan C.D.C. New Coronavirus Epidemic Prevention Course in Taiwan. Available online: https://www.tasw.org.tw (accessed on 9 April 2020).
- Taiwan Ministry of Health and Welfare. Precautions Against Severe Special Infectious Pneumonia (COVID-19, Wuhan Pneumonia). Available online: https://sites.google.com/cdc.gov.tw/2019ncov/global (accessed on 9 April 2020).
- WHO. Coronavirus Disease (COVID-2019) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 9 April 2020).
- Hsiao, R.; Schultz, K. Why Taiwan’s Coronavirus Response Shows Europe It Should Joint the World Health Organization. Available online: http://nationalinterest.org/feature/why-taiwans-coronavirus-response-shows-europe-it-should-join-world-health-organization?page=0%2C1 (accessed on 9 April 2020).
- Shih, C.H. A Study of Laboratory Safety-Hygiene Knowledge and Attitudes of the Teachers in Elementary School of Middle Area of Taiwan. Master’s Thesis, NTCU, Environmental Education Research Institute, Taichung, Taiwan, 2002. [Google Scholar]
- Shen, C.C. A Study of Safety-Hygiene Knowledge and Attitude toward Workplace for Graduating Students: A Case Study of Southern Taiwan University. Master’s Thesis, STUT, Technical Education and Human Resources Development Institute, Tainan, Taiwan, 2008. [Google Scholar]
- Huang, S.H. A Study on the Work Safety Awareness of Students in Technological Universities at Tainan Area. Master’s Thesis, STUT, Technical Education and Human Resources Development Institute, Tainan, Taiwan, 2009. [Google Scholar]
- YU, P.J. The Relationship on Workplace Safety and Hygiene Cognition, Attitude, and Behavior: A Study of Students in the Food and Beverage Management programs in the Vocational High School. Master’s Thesis, STUT, Catering Management Master Degree, Tainan, Taiwan, 2011. [Google Scholar]
- Bell, M.E. Learning and Instruction: Theory into Practice; McGraw-Hill: New York, NY, USA, 1986. [Google Scholar]
- Gifford, R.; Sussman, R. Environmental Attitudes. Environ. Attitudes 2012, 2, 241–270. [Google Scholar] [CrossRef]
- Chakravarti, D.; Eagly, A.H.; Chaiken, S. The Psychology of Attitudes. J. Mark. Res. 1997, 34, 298. [Google Scholar] [CrossRef]
- Bohner, G.; Dickel, N. Attitudes and Attitude Change. Annu. Rev. Psychol. 2011, 62, 391–417. [Google Scholar] [CrossRef] [Green Version]
- Brophy, J.; Leavitt, H.J. Managerial Psychology. Am. Cathol. Sociol. Rev. 1958, 19, 283. [Google Scholar] [CrossRef]
- Mao, Y.L. A Study of Oral Health Behaviors and Its Relevant Factors among Fifth and Sixth Grade Elementary School Students in Hsinchu County. Master’s Thesis, NTNU, Department of Health Promotion and Hygiene Education, Taipei, Taiwan, 2014. [Google Scholar]
- Halbreich, U.; Karkun, S. Cross-cultural and social diversity of prevalence of postpartum depression and depressive symptoms. J. Affect. Disord. 2006, 91, 97–111. [Google Scholar] [CrossRef]
- Hung, S.C. Influence of physical activity on mental health of the elderly. Sports Res. Rev. 2005, 78, 153–157. [Google Scholar] [CrossRef]
- National Taiwan University Hospital. Understanding of Mental Illness; Taiwan C.D.C.: Taipei, Taiwan, 2015.
- WHO, Chronicle of the World Health Organization Volume 1; World Health Organization Interim Commission: Geneva, Switzerland, 1947.
- Chen, Q.Z. How Much Do You Know about Stress? (Last) The Way the Body Responds to Chronic Stress. 2004. Available online: http://www.chinalife.com.tw/servlet/msg_001?step=2&input_1=E000000303 (accessed on 9 April 2020).
- Weiten, W.; Lloyd, M.A. Psychology Applied to Modern Life: Adjustment in the 90s, 4th ed.; Brooks: Pacific Grove, CA, USA, 1994. [Google Scholar]
- Chen, H.F. The Relationship of TV News Reporters’ Jobstress, Physical and Mental Health the Relationship of TV News Reporters’ Job and Stress, Physical and Mental Health Leisure Activities. Master’s Thesis, ASIA, Department of Leisure and Recreation Management, Taichung, Taiwan, 2009. [Google Scholar]
- Maslach, C.; Goldberg, J. Prevention of burnout: New perspectives. Appl. Prev. Psychol. 1998, 7, 63–74. [Google Scholar] [CrossRef]
- Lai, S.H.; Lee, P.F.; Chen, C.H. Analysis of the relationship between leisure activity participation and health for seniors:A case in northern Taiwan. J. Tour. Health Sci. 2014, 13, 29–44. [Google Scholar] [CrossRef]
- Atkeson, A. What Will Be the Economic Impact of COVID-19 in the US? Rough Estimates of Disease Scenarios. Natl. Bur. Econ. Res. 2020, 26867. [Google Scholar] [CrossRef]
- Yiengprugsawan, V.; Kelly, M.; Tawatsupa, B. Kessler Psychological Distress Scale. In Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014; pp. 3469–3470. [Google Scholar]
- Lin, H.H. The Study on Tourism Policy, Current Development Status, and Impact Perception of Sun Moon Lake. Ph.D. Thesis, Institute of Environmental Engineering Department, DaYeh University, Changhua, Taiwan, 2019. [Google Scholar]
- Construction Agency of the Ministry of Internal Affairs of the R.O.C. National Land Project; Ministry of the Interior: Taipei, Taiwan, 2018. [Google Scholar]
- Zanin, G.M.; Gentile, E.; Parisi, A.; Spasiano, D. A Preliminary Evaluation of the Public Risk Perception Related to the COVID-19 Health Emergency in Italy. Int. J. Environ. Res. Public Heal. 2020, 17, 3024. [Google Scholar] [CrossRef] [PubMed]
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian Medical Students; A Survey on Their Related-Knowledge, Preventive Behaviors and Risk Perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y.-F. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Lankford, S.V.; Howard, D.R. Developing a tourism impact attitude scale. Ann. Tour. Res. 1994, 21, 121–139. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Grounded Theory Procedures and Techniques, 2nd ed.; Sage: Sozende Oaks, CA, USA, 1998. [Google Scholar]
- Janesick, V.J. The Choreography of Qualitative Research Design: Minuets, improvisations, and Crystallization. In Handbook of Qualitative Research; Denzin, N.K., Lincoln, Y.S., Eds.; Sage: Thousand Oak, CA, USA, 2000; pp. 379–399. [Google Scholar]
- Gursoy, D.; Jurowski, C.; Uysal, M. Resident attitudes. Ann. Tour. Res. 2002, 29, 79–105. [Google Scholar] [CrossRef]
- Strauss & Corbin. Basics of Qualitative Research: Grounded Theory Procedures and Techniques; Sage: Newbury Park, CA, USA.
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Zaichkowsky, J.L. Measuring the Involvement Construct. J. Consum. Res. 1985, 12, 341. [Google Scholar] [CrossRef]
- Bowen, L.; Chaffee, S.H. Product Involvement and Pertinent Advertising Appeals. J. Q. 1974, 51, 613–621. [Google Scholar] [CrossRef]
- Xie, Y.; DeVellis, R.F. Scale Development: Theory and Applications. Contemp. Sociol. A 1992, 21, 876. [Google Scholar] [CrossRef]
- Ministry of the Interior, Taiwan, R.O.C. Internal Statistics Bulletin. Available online: https://www.tasw.org.tw (accessed on 9 April 2020).
- Lin, H.Z. 83 days after COVID-19 Attacked Taiwan, What Changes and Changes Have Been Made in Taiwan’s Epidemic Prevention Policy-A Complete Description of the Epidemic Situation Center and Expert Analysis. Available online: https://www.twreporter.org/a/covid-19-taiwan-epidemic-prevention-policies-change (accessed on 9 April 2020).
- Yang, H.J.; Zhang, Z.W.; Chen, L.T. Health Inequality-Taiwan’s Three Largest Child Death Areas. 2018. Available online: https://www.twreporter.org/a/child-health-care-remote-areas-inequality (accessed on 8 May 2020).
- Deng, L.P. We Can Never GO back! MIT: Social Distance Will Become the New Normal in Life. Available online: https://www.gvm.com.tw/article/71817 (accessed on 15 May 2020).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area | County Name | Total |
|---|---|---|
| North | Taipei, New Taipei, Keelung, Taoyuan, Hsinchu County, Hsinchu City, Yilan | 7 |
| Central | Miaoli, Taichung, Changhua, Nantou, Yunlin | 5 |
| South | Chiayi City, Chiayi County, Tainan, Kaohsiung, Pingtung | 5 |
| East | Hualien, Taitung | 2 |
| islands | Kinmen, Lienchiang, Penghu | 3 |
| Dimension | Subdimension | Subject (M) | Cronbach’α |
|---|---|---|---|
| Physical and mental health | Psychological status (5) | Unstable mood(3.02), feelings of anxiety and panic(3.28), reduced ability(2.67), reduced enthusiasm(2.91), and limited time(2.94) | 0.943–0.948 |
| Spiritual status (5) | Headaches(2.62), fatigue(2.57), pain(2.44), back pain(2.32), and insomnia(2.32) | 0.942–0.943 | |
| Attitude and health (6) | Stomach ache(2.25), increased smoking frequency(2.17), irritability(2.36), lack of confidence(2.15), loss of life purpose(2.25), and suicidal thoughts(2.05) | 0.942–0.946 | |
| Epidemic prevention awareness | Epidemic prevention awareness (4) | Effectiveness of epidemic prevention campaigns(3.88), family influences on individual prevention habits(3.88), formation of prevention habits in families(4.15), and prevention consensus between the public and individuals(4.18) | 0.967–0.970 |
| Consensus on decision-making (4) | Epidemic prevention campaigns(4.18), campus prevention campaigns(4.13), family prevention consensus(4.19), and prevention consensus among interviewees(4.19) | 0.966–0.967 | |
| Emergency response (6) | Effect of prevention campaigns on health(3.97), the effects of prevention measures(3.98), the effectiveness of self-protection awareness(3.93), prevention campaigns in public spaces(4.02), prevention campaigns in the media(3.95), and prevention facility installment in public spaces(4.04) | 0.967–0.968 | |
| Epidemic prevention attitude | Perception (4) | Compliance with prevention measures(4.14), increased prevention vigilance in daily life(4.09), increased campus prevention vigilance(4.13), and the effects of prevention knowledge on infection rate(4.1) | 0.959–0.961 |
| Explicit reaction (4) | Prevention information acquisition(3.99), compliance with teachers’ epidemic prevention advice(4.04), compliance with public space prevention measures(4.07), and informational research of prevention knowledge(3.93) | 0.929–0.962 | |
| Epidemic prevention behavior | Daily life adaptability (11) | Adequate compliance with the epidemic prevention measures(3.99), active compliance with prevention measures(4.03), correct naming of all prevention processes(3.79), compliance with public space regulations(4.04), wearing of masks(4.08), consultation of experts and scholars for advice(3.92), consultation of online media for advice(3.88), reporting to parents or teachers(3.76), reporting to relatives or friends(3.84), active maintenance of personal hygiene(3.93), active maintenance of cleanliness at home(3.94), medical waste recycling(3.97) | 0.967–0.968 |
| Individual performance (4) | Sharing of prevention knowledge(3.76), reminding persons of inappropriate individual behavior(3.67), active community cleaning(3.67), reminding persons of inappropriate public behavior(3.68) | 0.967–0.969 |
| Gender | Age | Occupation | Area | Gender | Age | Occupation | Area |
|---|---|---|---|---|---|---|---|
| male | 22 | student | northern | male | 55 | education | central |
| female | 22 | Service industry | south | male | 38 | Tourism | central |
| male | 21 | student | northern | female | 56 | administration staff | northern |
| male | 45 | education | islands | male | 57 | administrative | northern |
| female | 42 | financial | south | female | 24 | student | east |
| Level | interview topics description | ||||||
| Cognition | How do you know your epidemic awareness, decision consensus, and resilience? Where does local information generally come from? | ||||||
| attitude | How do you know your epidemic alert settings and information? Where do local information generally come from? | ||||||
| behavior | How do you know your personal anti-epidemic attitude and self-protection measures? Where do local information generally come from? | ||||||
| Physical and mental health | What is the impact of the epidemic on an individual’s physical and mental health? What industry has the greatest impact? Where does the local information generally come from? | ||||||
| Based on the above, which one has the greatest impact on people, regions, and occupations? And give your opinion? | |||||||
| Area | No. | % | Gender | No. | % | Occupation | No. | % |
|---|---|---|---|---|---|---|---|---|
| Northern | 711 | 33.3% | male | 842 | 39.5% | student | 1505 | 70.60% |
| Central | 1129 | 52.9% | female | 1290 | 60.5% | Restaurant Catering | 131 | 6.10% |
| South | 211 | 9.9% | Age | No. | % | tourism | 28 | 1.30% |
| East | 25 | 1.2% | Under 20 | 1068 | 50.1% | Leisure sport | 19 | 0.90% |
| islands | 58 | 2.7% | 21–30 | 769 | 36.1% | Marketing media | 13 | 0.60% |
| Health status | No. | % | 31–40 | 105 | 4.9% | Teachers and civil servants | 21 | 1% |
| Good health | 1960 | 91.9% | 41–50 | 111 | 5.2% | Legal administration | 13 | 0.60% |
| other illnesses | 29 | 1.4% | 51–60 | 57 | 2.7% | Human Resources | 17 | 0.80% |
| chronic | 53 | 2.5% | Over 61 | 22 | 1% | Finance/Insurance/Accounting | 34 | 1.60% |
| general | 43 | 2% | education level | No. | % | Business services | 53 | 2.50% |
| new coronary | 20 | 0.9% | Elementary | 19 | 0.9% | real estate | 23 | 1.10% |
| general trauma | 27 | 1.3% | Junior | 56 | 2.6% | Transportation | 10 | 0.50% |
| Leisure behavior | No. | % | Senior | 301 | 14.1% | Aviation industry and petroleum industry | 2 | 0.10% |
| yes | 260 | 12.2% | universities | 1697 | 79.6% | E-commerce | 3 | 0.10% |
| no | 1872 | 87.8% | Over institute | 59 | 2.8% | Export trade | 13 | 0.60% |
| Travel habits | No. | % | Epidemic prevention message | No. | % | Industrial manufacturing | 38 | 1.80% |
| yes | 1482 | 69.4% | Oral | 118 | 5.5% | Machining | 27 | 1.30% |
| no | 652 | 30.6% | Proclamation | 42 | 2% | Agriculture, Forestry and Fisheries | 10 | 0.50% |
| Health education knowledge | No. | % | newspapers | 105 | 4.9% | Soldiers and police | 22 | 1% |
| family | 115 | 5.4% | TV | 989 | 46.4% | Human agency | 4 | 0.20% |
| School | 246 | 11.5% | Online social platform | 878 | 41.2% | Retail and wholesale | 34 | 1.60% |
| Government | 299 | 14.0% | Computer communication | 22 | 1% | |||
| Mass media | 956 | 44.8% | Performance of art | 10 | 0.50% | |||
| Online social platform | 516 | 24.2% | Housekeeping freelance | 80 | 3.80% | |||
| Highly Recognized | M | Low Recognition | M | Total Score | Actual Score | ||
|---|---|---|---|---|---|---|---|
| Epidemic prevention awareness | Epidemic prevention awareness | prevention consensus between the individuals | 4.18 | Effectiveness of epidemic prevention campaigns | 3.88 | 20 | 16.10 |
| Consensus on decision-making | family prevention consensus | 4.19 | campus prevention campaigns | 4.13 | 20 | 16.70 | |
| Emergency response | prevention facility installment in public spaces | 4.04 | Effect of prevention campaigns on health | 3.93 | 30 | 23.89 | |
| Epidemic prevention attitude | Perception | Compliance with prevention measures | 4.14 | increased prevention vigilance in daily life | 4.09 | 20 | 16.45 |
| Explicit reaction | compliance with teachers’ epidemic prevention advice | 4.07 | informational research of prevention knowledge | 3.93 | 20 | 16.03 | |
| Epidemic prevention behavior | Daily life adaptability | active compliance with prevention measures and wearing of masks | 4.08 | reporting to parents or teachers | 3.76 | 55 | 47.17 |
| Individual performance | Sharing of prevention knowledge | 3.76 | active community cleaning | 3.67 | 20 | 14.77 | |
| Physical and mental health | Psychological status | feelings of anxiety and panic | 3.28 | reduced ability | 2.67 | 25 | 14.81 |
| Spiritual status | headaches | 2.62 | insomnia | 2.57 | 25 | 12.27 | |
| Attitude and health | irritability | 2.36 | suicidal thoughts | 2.05 | 30 | 13.22 | |
| Background | Cognition | Attitude | Behavior | Physical and Mental Health |
|---|---|---|---|---|
| High cognition(M) | Family habits (4.3) Family consensus (4.3) Public measures (4.1) | Cooperation with policies (4.2) Compliance with public measures (4.1) | Voluntarily wearing masks (4.2) Gathering medical waste (4.0) Sharing information (3.8) | Anxiety (3.2) Headache (3.2) Irritability (2.4) |
| Low cognition(M) | Epidemic-prevention campaign (3.9) Campus epidemic prevention (4.1) Advocacy to promote health (3.9) | Alertness (4.0) Information gathering (3.9) | Conveying epidemic prevention information (3.8) Home cleaning (3.9) Community cleaning (3.6) | Capability (2.6) Lumbago (2.3) Suicidal ideation (2.0) |
| Different gender (t) | Epidemic prevention advocacy (3.8:4.1) * family habits (3.8:4.1) * self-epidemic prevention (4:4.4) * health protection (3.8:4.0) * public protection (3.8:4.3) * | Media information (3.8:4.1) * teacher suggestions (3.9:4.2) * public measures (3.9:4.3) * search information (3.8:4.1) | Epidemic prevention steps (3.8:4.2) * personal execution (3.8:4.2) * seeking solutions (3.7:4.0) * wear mask (3.8:4.2) * health management (3.8:4.2) * | Mood (3:3.1) * pain sensitivity (2.6:2.4) * eating disorders (2.5:2.2) * lack of confidence (2.4:2.0) * |
| Different age (F) | Family habits (Under 20,21–30,31–40,41–50 > 51–60) * | Campus epidemic prevention (51–60 > Under 20,21–30) *, teacher suggestions (51–60 > 41–50) * | Teachers (51–60 > 41–50) * relatives and friends for help (51–60 > Under 20,21–30,41–50) * information sharing (51–60 > Under 20,21–30,41–50) * epidemic prevention supervision (51–60 > Under 20,41–50) * | Emotions (21–30,3 > 51–60) * Stress (Under 20,21–30 > 51–60) * pain sensitivity (Under 20,21–30,41–50 > 51–60) * insomnia (41–50 > 51–60) * lack of self-confidence (Under 20,41–50 > 51–60) * seeking death (Under 20 > 21–30) * |
| Different Health status(F) 1: Good 2: common cold 3: new coronavirus 4. chronic disease 5. common trauma 6. other | public consensus (1,4,2,5,6 > 3) * health protection (1,4,2,5,6 > 3) * public protection and facilities (1,6 > 4,3) * | Campus epidemic prevention (1,2,5,6 > 3) * media information (1,2,6 > 3) * public measures (1,6 > 4,3) * | Epidemic prevention steps (1,6 > 3) * personal execution (1,4,2,5,6 > 3) * seeking solutions (1 > 3) * wear mask and health management (1,4,2,5,6 > 3) * information sharing (1,4,2,5,6 > 3) * epidemic prevention supervision (1,4,2,5,6 > 3) * | pain sensitivity (6 > 1) * insomnia (4,3 > 1,2,5) * indigestion (3 ,6 > 1,5) * eating disorders (3 > 1) * lack of self-confidence (4 > 1) * seeking death (4,6 > 1,2) * |
| Background | Cognition | Attitude | Behavior | Physical and Mental Health |
|---|---|---|---|---|
| High cognition | Epidemic-prevention campaign (4.2) Campus consensus (4.2) Media outreach (4.0) | Life alertness (4.2) Compliance with public epidemic prevention (4.1) | Voluntarily wearing masks (4.0) Consulting the media for advice (3.9) Reminding persons of inappropriate public behavior (3.8) | Anxiety (3.0) Mental weakness (2.6) Irritability (2.7) |
| Low cognition | Personal consensus (2.7) Advocacy to promote health (3.9) Public measures (3.9) | Information gathering (3.0) Personal cleaning (3.6) | Compliance with public regulations (3.7) Personal cleaning (3.6) Community cleaning (3.6) | Enthusiasm (2.6) Indigestion (2.3) Sense of loss (2.1) |
| Different gender (t) | personal and family habits (3.5:4.0) * personal (2.9:2.7) * family (3.8:4.3) * consensus with the public (3.8:4.4) * health protection (3.9:4.4) * public protection and facilities (3.7:4.2) * | Media information (3.8:4.3) * teachers ’suggestions (3.7:4.2) * public measures (3.8: 4.2) * | Epidemic prevention steps (3.7:3.9) * personal execution (3.8:4.2) * seeking solutions (3.8:4.2) * health management (3.8:4.2) * | Insomnia (2.4: 2.2) * Pain (2.8: 3.0) * Indigestion (2.8: 2.3) * reduced enthusiasm (2.4:2.3) * eating disorders(2.4:2.1) * |
| Different age (F) | Personal consensus (Under 20 > 21–30) family consensus (Under 20 > 21–30) * epidemic prevention advocacy acceptance (Under 20 > 21–30) * | Sensitivity (Under 20 > 21–30) teacher suggestions (Under 20 > 21–30) * public measures(Under 20 > 21–30) * | Epidemic prevention steps (Under 20 > 21–30) * seeking solutions(Under 20 > 21–30) * | Emotions (Under 20 > Over 61) * work ability (Under 20,21–30,31–40,41–50 > Over 61) *enthusiasm (Under 20,21–30,31–40,41–50 > 51–60) * pain sensitivity (Under 20 > 21–30,51–60,6) * insomnia (31–40,41–50, Over 61 > 51–60) * lack of self-confidence (41–50 > 51–60) * |
| Different Health status(F) 1: Good 2: common cold 3: new coronavirus 4. chronic disease 5. common trauma 6. other | NS | NS | NS | Emotions(1,4,6 > 5) enthusiasm(4,6 > 5) |
| Background | Cognition | Attitude | Behavior | Physical and Mental Health |
|---|---|---|---|---|
| High cognition | Personal consensus (4.3) Street visit consensus (4.3) Public measures (4.1) | Campus alertness (4.2) Compliance with public measures (4.2) | Voluntarily wearing masks (4.2) Community cleaning (3.7) | Emotions (3.2) Mental weakness (2.5) Overeating (2.2) |
| Low cognition | Epidemic-prevention campaign (4.0) Campus epidemic prevention (4.2) Media outreach (3.9) | Life alertness (4.1) Acquiring information from media (4.0) | Teachers’ reactions (3.7) Sense of justice (3.5) | Ability deterioration (2.6) Lumbago (2.1) Suicidal ideation (1.9) |
| Different gender (t) | Public consensus (3.7:4.2) * | NS | NS | NS |
| Different age (F) | NS | NS | Expert advice(Under 20 > 21–30) * | Stress (31–40 > 21–30) * Insomnia (21–30 > Under 20) * pain sensitivity (21–30 > Under 20) * eating disorders(21–30 > Under 20) * |
| Background | Cognition | Attitude | Behavior | Physical and Mental Health |
|---|---|---|---|---|
| High cognition | Family habits (3.9) Personal consensus (3.9) Campus advocacy (3.9) Family consensus (3.9) Public consensus (3.7) Advocacy to promote health (3.7) Public epidemic-prevention campaign (3.7) Media epidemic-prevention campaign (3.7) Public epidemic-prevention facilities (3.7) | Cooperation awareness (4.1) Campus alertness (4.1) | Compliance with epidemic prevention measures (3.9) Sense of justice (3.1) | Anxiety (3.6) Headache (2.8) Sense of loss (2.0) |
| Low cognition | Propaganda and Epidemic Prevention (3.5) Public anti-epidemic facilities (3.4) | Life alertness (3.8) Comply with public anti-epidemic measures (3.2) | Community cleanliness (3.0) Teacher response, reflection from relatives and friends (3.4) | Decreased ability (2.6) Insomnia (1.9) Suicide (1.8) |
| Different Health status(F) 1: Good 2: common cold 3: new coronavirus 4. chronic disease 5. common trauma 6. other | Public places(1 > 3,2) * media outreach(1 > 3,2) * | NS | NS | pain sensitivity(4 > 1) * |
| Cognition | Attitude | Behavior | Physical and Mental Health | |
|---|---|---|---|---|
| High cognition | Family epidemic prevention, personal consensus, public consensus (4.3) Advocacy to promote health (3.9) | Life alertness, campus alertness (4.2) | Compliance with public measures, voluntarily wearing masks (4.1) Sense of justice (3.9) | Anxiety (3.1) Headache (3.0) Indigestion (2.5) |
| Low cognition | Family habits (3.8) Campus epidemic prevention (4.2) Public epidemic prevention (4.0) | Epidemic prevention knowledge, teachers’ advice (3.9) | Suggestions from friends and family, community cleaning (3.6) | Sense of urgency (2.9) Insomnia (2.6) Suicidal ideation (2.1) |
| Different gender (t) | Epidemic Prevention(4.3:3.5) * | NS | Message sharing(3.8:3.9) * | Pain sensitivity (2.6:3.2) * Indigestion (2.2:2.7) * abnormal diet (2.4:2.5) * insomnia (2.4:2.8) * emotional instability (2.3:2.8) * confidence (2.5:2.4) * life goals (2.4:2.5) * |
| Different age (F) | NS | Media information (Under 20,21–30,31–40,41–50 > Over 61; Under 20 > 31–40) * | Epidemic prevention steps (Under 20,21–30,31–40,41–50 > Over 61) * epidemic prevention supervision (Under 20,21–30,31–40,41–50 > Over 61) * | Pain sensitivity (4 > Under 20,21–30,31–40) * abnormal diet (41–50 > Under 20) * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-H.; Lin, H.-H.; Wang, C.-C.; Jhang, S. How to Defend COVID-19 in Taiwan? Talk about People’s Disease Awareness, Attitudes, Behaviors and the Impact of Physical and Mental Health. Int. J. Environ. Res. Public Health 2020, 17, 4694. https://doi.org/10.3390/ijerph17134694
Hsu C-H, Lin H-H, Wang C-C, Jhang S. How to Defend COVID-19 in Taiwan? Talk about People’s Disease Awareness, Attitudes, Behaviors and the Impact of Physical and Mental Health. International Journal of Environmental Research and Public Health. 2020; 17(13):4694. https://doi.org/10.3390/ijerph17134694
Chicago/Turabian StyleHsu, Chin-Hsien, Hsiao-Hsien Lin, Chun-Chih Wang, and Shangwun Jhang. 2020. "How to Defend COVID-19 in Taiwan? Talk about People’s Disease Awareness, Attitudes, Behaviors and the Impact of Physical and Mental Health" International Journal of Environmental Research and Public Health 17, no. 13: 4694. https://doi.org/10.3390/ijerph17134694
APA StyleHsu, C. -H., Lin, H. -H., Wang, C. -C., & Jhang, S. (2020). How to Defend COVID-19 in Taiwan? Talk about People’s Disease Awareness, Attitudes, Behaviors and the Impact of Physical and Mental Health. International Journal of Environmental Research and Public Health, 17(13), 4694. https://doi.org/10.3390/ijerph17134694