Influence of an Aquatic Therapy Program on Perceived Pain, Stress, and Quality of Life in Chronic Stroke Patients: A Randomized Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Outcome Measures
2.3.1. The Visual Analog Scale (VAS)
2.3.2. Resilience
2.3.3. SF-36
2.4. Procedure
2.5. Intervention
2.5.1. Dry Land Physiotherapy (Control Group)
2.5.2. Aquatic Ai Chi (Experimental Group)
2.5.3. Combined Therapy Group
2.6. Stastistical Analysis
3. Results
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L. Stroke epidemiology in the developing world. Lancet 2005, 365, 2160–2161. [Google Scholar] [CrossRef]
- Warlow, C.P. Epidemiology of stroke. Lancet 1998, 352, 1–4. [Google Scholar] [CrossRef]
- Bejot, Y.; Daubail, B.; Giroud, M. Epidemiology of stroke and transient ischemic attacks: current knowledge and perspectives. Rev. Neurol. 2016, 172, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.G.; Thayabaranathan, T.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.L.; Norrving, B.; Donnan, G.A.; Cadilhac, D.A. Global stroke statistics. Int. J. Stroke 2017, 12, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Lamb, S.E.; Ferrucci, L.; Volapto, S.; Fried, L.P.; Guralnik, J.M. Risk factors for falling in home-dwelling older women with stroke. Stroke 2003, 34, 494–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, C.; Fang, M.; Liu, X.Y. The neurobiological pathogenesis of poststroke depression. Sci. World J. 2014. Available online: https://doi.org/10.1155/2014/521349 (accessed on 7 February 2020).
- Carod-Artal, F.J. Depresión postictus (I). Epidemiología, criterios diagnósticos y factores de riesgo. Rev. Neurol. 2006, 42, 169–675. [Google Scholar] [CrossRef]
- Dafer, R.M.; Rao, M.; Shareef, A.; Sharma, A. Poststroke depression. Top. Stroke Rehabil. 2008, 15, 13–31. [Google Scholar] [CrossRef]
- Angelelli, P.; Paolucci, S.; Bivona, U.; Piccardi, L.; Ciurli, P.; Cantagallo, A. Development of neuropsychiatric symptoms in poststroke patients: A cross-sectional study. Acta Psychiatr. Scand. 2004, 110, 53–55. [Google Scholar] [CrossRef]
- Lökk, J.; Delbari, A. Management of depression in elderly stroke patients. Neuropsychiatr. Dis. Treat. 2010, 6, 539–549. [Google Scholar]
- Robinson, R.G.; Spalletta, G. Poststroke depression: A review. Can. J. Psych. 2010, 55, 341–449. [Google Scholar] [CrossRef] [Green Version]
- Carnés-vendrell, A.; Deus-yela, J.; Molina-seguin, J.; Pifarré-paradero, J.; Purroy, F. Actualización de la depresión postictus: nuevos retos en pacientes con ictus minor o ataque isquémico transitorio. Rev. Neurol. 2016, 62, 460–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenzi, G.L.; Altieri, M.; Maestrini, I. Post-stroke depression. Rev. Neurol. 2008, 164, 837–840. [Google Scholar] [CrossRef] [PubMed]
- De Matos, D.G.; Mazini Filho, M.L.; Moreira, O.C.; De Oliveira, C.E.; De Oliveira Venturini, G.R.; Da Silva-Grigoletto, M.E. Effects of eight weeks of functional training in the functional autonomy of elderly women: A pilot study. J. Sports Med. Phys. Fit. 2017, 57, 272–277. [Google Scholar]
- Moore, K.A.; Babyak, M.A.; Wood, C.E.; Napolitano, M.A.; Khatri, P.; Craighead, W.E. The Association Between Physical Activity and Depression in Older Depressed Adults. J. Aging Phys. Act. 1999, 7, 51–55. [Google Scholar] [CrossRef]
- Aidar, F.S.; Reis, A.J.; Carneiro, V.M.; Leite, A.M. Elderly and old adult: Aquatic physical activities and functional autonomy. Fit. Perform. J. 2006, 5, 271–276. [Google Scholar]
- Lambeck, J.; Bommer, A. Ai Chi®: Applications in Clinical Practice; Washington State University Publishing: Washington, DC, USA, 2010. [Google Scholar]
- So, B.C.L.; Kong, I.S.Y.; Lee, R.K.L.; Man, R.W.F.; Tse, W.H.K.; Fong, A.K.W.; Tsang, W.W.N. The effect of Ai Chi aquatic therapy on individuals with knee osteoarthritis: A pilot study. J. Phys. Sci. 2017, 29, 884–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Notario-Pacheco, B.; Solera-Martínez, M.; Serrano-Parra, M.D.; Bartolome-Gutierrez, R.; García-Campayo, J.; Martínez-Vizcaino, V. Reliability and validity of the Spanish version of the 10-item Connor-Davidson Resilience Scale (10-item CD-RISC) in young adults. Health Qual. Life Outc. 2011, 9, 63. [Google Scholar] [CrossRef] [Green Version]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. El Cuestionario de Salud SF-36 español: Una década de experiencia y nuevos desarrollos. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [Green Version]
- Rafsten, L.; Danielsson, A.; Sunnerhagen, K.S. Anxiety after stroke: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 769–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell Burton, C.A.; Murray, J.; Holmes, J.; Astin, F.; Greenwood, D.; Knapp, P. Frequency of anxiety after stroke: A systematic review and meta-analysis of observational studies. Int. J. Stroke 2013, 8, 545–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carod-Artal, J.; Egido, J.A.; Luis González, J.; Varela de Seijas, E. Quality of life among stroke survivors evaluated 1 year after stroke: Experience of a stroke unit. Stroke 2000, 31, 2995–3000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, S.; Arima, H.; Bertmar, C.; Hirakawa, Y.; Priglinger, M.; Evans, K. Depression but not anxiety predicts recurrent cerebrovascular events. Acta Neurol. Scand. 2016, 134, 29–34. [Google Scholar] [CrossRef]
- Ayerbe, L.; Ayis, S.; Wolfe, C.D.; Rudd, A.G. Natural history, predictors and outcomes of depression after stroke: Systematic review and meta-analysis. Br. J. Psychiatry 2013, 202, 14–21. [Google Scholar] [CrossRef]
- Adam, D.; Ramli, A.; Shahar, S. Effectiveness of a Combined Dance and Relaxation Intervention on Reducing Anxiety and Depression and Improving Quality of Life among the Cognitively Impaired Elderly. Sultan Qaboos Univ. Med. J. 2016, 16, 47–53. [Google Scholar] [CrossRef]
- Brown, D.R.; Morgan, W.P.; Raglin, J.S. Effects of exercise and rest on the state anxiety and blood pressure of physically challenged college students. J. Sports Med. Phys. Fit. 1993, 33, 300–305. [Google Scholar]
- Byrne, A.; Byrne, D.G. The effect of exercise on depression, anxiety and other mood states: A review. J. Psychosom. Res. 1993, 37, 565–574. [Google Scholar] [CrossRef]
- Antunes, H.K.; Stella, S.G.; Santos, R.F.; Bueno, O.F.; de Mello, M.T. Depression, anxiety and quality of life scores in seniors after an endurance exercise program. Braz. J. Psychiatry 2005, 27, 266–271. [Google Scholar] [CrossRef] [Green Version]
- Schuch, F.B.; Deslandes, A.C.; Stubbs, B.; Gosmann, N.P.; Silva, C.T.; Fleck, M.P. Neurobiological effects of exercise on major depressive disorder: A systematic review. Neurosci. Biobehav. Rev. 2016, 61, 1–11. [Google Scholar] [CrossRef]
- Russo, S.J.; Murrough, J.W.; Han, M.H.; Charney, D.S.; Nestler, E.J. Neurobiology of resilience. Nat. Neurosci. 2012, 15, 1475–1484. [Google Scholar] [CrossRef] [Green Version]
- Almaguer-Melián, W.; Bergado-Rosado, J.A. Interacciones entre el hipocampo y la amígdala en proceso de plasticidad sináptica. Una clave para entender las relaciones entre motivación y memoria. Revista de Neurología 2002, 35, 586–593. [Google Scholar]
- Sostres-Bayón, F.; Sierra-Mercado, D.; Padilla-Delgado, E.; Quirk, G. Gating of fear in prelimbic cortex by hippocampal and amygdala inputs. Neuron 2012, 47, 804–812. [Google Scholar]
- Bocchio, M.; Nabavi, S.; Capogna, M. Synaptic plasticity, engrams, and network oscillations in amygdala circuits for storage and retrieval of emotional memories. Neuron 2017, 94, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Kootker, J.A.; Van Mierlo, M.L.; Hendriks, J.C.; Sparidans, J.; Rasquin, S.M.; de Kort, P.L. Risk factors for symptoms of depression and anxiety one year poststroke: A longitudinal study. Arch. Phys. Med. Rehabil. 2016, 97, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Ford, A.H.; Hankey, G.J.; Golledge, J.; Yeap, B.B.; Flicker, L. Depression, antidepressants and the risk of cardiovascular events and death in older men. Maturitas 2019, 128, 4–9. [Google Scholar] [CrossRef]
- Robinson, R.G.; Jorge, R.E. Post-Stroke Depression: A Review. Am. J. Psychiatry 2016, 173, 221–231. [Google Scholar] [CrossRef] [Green Version]
- Pérez-de la Cruz, S. Mental health in Parkinson’s disease after receiving aquatic therapy: A clinical trial. Acta Neurol. Belg. 2019, 119, 193–200. [Google Scholar]
- Ihle-Hansen, H.; Langhammer, B.; Lydersen, S.; Gunnes, M.; Indredavik, B.; Askim, T. A physical activity intervention to prevent cognitive decline after stroke: Secondary results from the Life After Stroke study, an 18-month randomized controlled trial. J. Rehabil. Med. 2019, 51, 646–651. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Pre | Post | 1 Month | Time | Treatment*Time | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | F(g.l.); p-Value (eta2) | F(g.l.); p-Value (eta2) | |
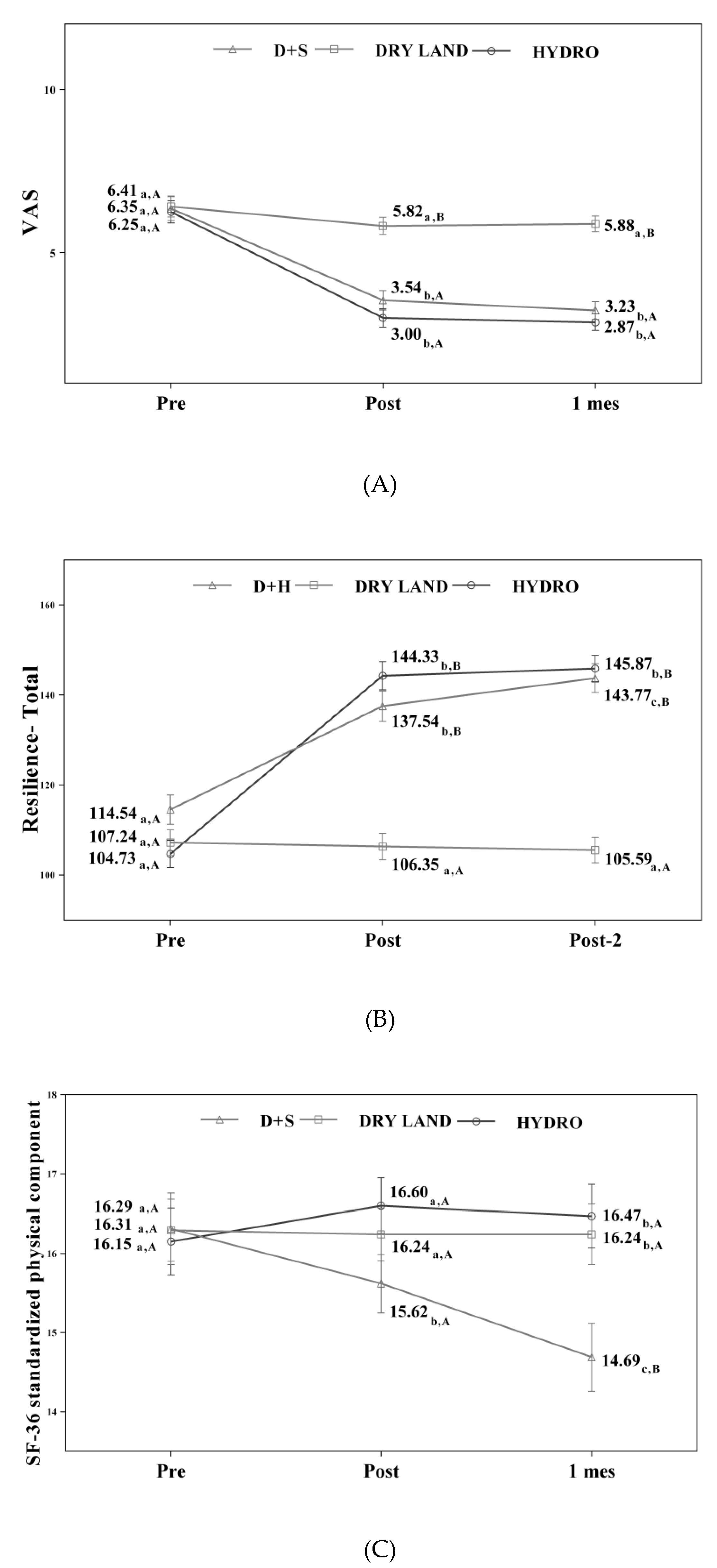
| VAS Scale | F(1.3;56.5) = 158.28; p < 0.001 (0,790) | F(2.7;56.5) = 24.91; p < 0.001* (0.543) | |||
| H+D (13) | 6.35 (1.0) | 3.54 (0.8) | 3.23 (0.9) | ||
| Dry Land (17) | 5.41 (1.5) | 5.82 (1.1) | 5.88 (1.0) | ||
| AT (15) | 6.25 (1.4) | 3.00 (1.3) | 2.87 (1.0) | ||
| Personal Satisfaction resilience | F(1.2;52.3) = 67.77; p < 0.001 (0.617) | F(2.5;52.3) = 27.13; p < 0.001* (0.564) | |||
| H+D (13) | 18.62 (3.1) | 23.69 (3.2) | 24.54 (3.8) | ||
| Dry Land (17) | 1665 (3.2) | 16.59 (3.1) | 16.24 (2.9) | ||
| AT (15) | 18.20 (2.6) | 24.80 (3.4) | 25.07 (3.5) | ||
| Feeling Good on My Own resilience | F(1.4;58.5) = 77.50; p < 0.001 (0.649) | F(2.8;58.5) = 21.25; p < 0.01* (0.503) | |||
| H+D (13) | 13.15 (2.8) | 14.92 (3.3) | 16.46 (3.2) | ||
| Dry Land (17) | 14.77 (2.4) | 14.94 (2.2) | 14.77 (2.1) | ||
| AT (15) | 14.33 (2.4) | 19.67 (1.2) | 20.27 (1.0) | ||
| Self Confidence resilience | F(1.1;47.4) = 85.14; p < 0.001 (0.670) | F(2.3;47.4) = 25.09; p < 0.001* (0.544) | |||
| H+D (13) | 29.62 (5.9) | 37.54 (5.2) | 38.85 (5.3) | ||
| Dry Land (17) | 29.82 (4.8) | 29.71 (5.0) | 29.47 (4.7) | ||
| AT (15) | 29.73 (5.1) | 38.73 (3.4) | 39.07 (3.2) | ||
| Equanimity resilience | F(1.1;47.9) = 92.26; p < 0.001 (0.687) | F(2.3;47.9) = 58.82; p < 0.001* (0.737) | |||
| H+D (13) | 15.15 (2.8) | 22.54 (2.0) | 22.92 (1.8) | ||
| Dry Land (17) | 14.65 (1.6) | 14.53 (1.4) | 14.35 (1.3) | ||
| AT (15) | 14.40 (2.1) | 21.40 (2.6) | 21.67 (2.4) | ||
| Perseverance resilience | F(1.3;55.3) = 91.52; p < 0.001 (0.685) | F(2.6;55.3) = 35.92; p < 0.001* (0.631) | |||
| H+D (13) | 31.50 (4.7) | 38.85 (4.8) | 41.00 (4.5) | ||
| Dry Land (17) | 31.35 (4.3) | 30.59 (4.4) | 30.18 (4.0) | ||
| AT (15) | 30.87 (5.3) | 39.73 (4.7) | 39.80 (4.6) | ||
| Total resilience | F(1.2;51.7) = 167.48; p < 0.001 (0.799) | F(2.5;51.7) = 57.91; p < 0.001* (0.734) | |||
| H+D (13) | 114.54 (13.9) | 137.54 (14.7) | 143.77 (15.2) | ||
| DRY LAND (17) | 107.24 (11,6) | 106.35 (11.1) | 105.59 (9.3) | ||
| AT (15) | 104.73 (9.8) | 144.33 (10.8) | 145.87 (9.8) |
| Pre | Post | 1 Month | Time | Treatment*Time | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | F(g.l.); p-Value (eta2) | F(g.l.); p-Value (eta2) | |
| Physical Function | F(1.2;51.8) = 149.34; p < 0.001 (0.781) | F(2.5;51.8) = 36.90; p < 0.001* (0.637) | |||
| H+D (13) | 16.92 (4.4) | 22.08 (3.4) | 23.46 (3.5) | ||
| Dry Land (17) | 17.06 (2.5) | 17.24 (2.8) | 17.24 (2.8) | ||
| AT (15) | 17.07 (3.5) | 23.20 (2.5) | 24.47 (2.4) | ||
| Physical Role | F(1.3;53.5) = 87.19; p < 0.001 (0.675) | F(2.5;53.5) = 16.60; p < 0.001* (0.442) | |||
| H+D (13) | 5.15 (1.4) | 7.62 (1.0) | 7.85 (0.6) | ||
| Dry Land (17) | 5.24 (1.6) | 5.59 (1.4) | 5.59 (1.4) | ||
| AT (15) | 5.07 (1.2) | 7.60 (0.6) | 7.93 (0.3) | ||
| Body Pain | F(1.3;53.8) = 134.65; p < 0.001 (0.762) | F(2.6;53.8) = 36.34; p < 0.001* (0.634) | |||
| H+D (13) | 6.93 (2.6) | 3.39 (1.2) | 2.77 (0.7) | ||
| Dry Land (17) | 6.94 (1.1) | 6.94 (1.2) | 6.94 (1.2) | ||
| AT (15) | 7.00 (1.3) | 3.67 (0.7) | 2.93 (1.0) | ||
| General Health | F(1.7;71.6) = 8.00; p = 0.001 (0.160) | F(3.4;71,6) = 3.13; p = 0.026 (0.130) | |||
| H+D (13) | 16.31 (2.1) | 15.62 (1.7) | 14.69 (2.1) | ||
| Dry Land (17) | 16.29 (1.3) | 16.24 (1.4) | 16.24 (1.4) | ||
| AT (15) | 16.15 (1.5) | 16.60 (0.8) | 16.47 (1.1) | ||
| Vitality | F(1.2;48.9) = 1.72; p = 0.196 (0.039) | F(2.3;48.9) = 3.69; p = 0.026 (0.149) | |||
| H+D (13) | 16.23 (1.3) | 15.31 (1.3) | 15.77 (1.6) | ||
| Dry Land (17) | 16.29 (2.2) | 16.65 (2.0) | 16.65 (2.0) | ||
| AT (15) | 16.21 (2.2) | 15.47 (0.6) | 15.63 (0.9) | ||
| Social Function | F(1.3;56.1) = 5.25; p = 0.017 (0.111) | F(2.7;56.1) = 1.75; p = 0.172 (0.077) | |||
| H+D (13) | 5.71 (0.9) | 5.85 (0.8) | 6.15 (0.7) | ||
| Dry Land (17) | 5.69 (1.2) | 5.65 (1.2) | 5.65 (1.2) | ||
| AT (15) | 5.72 (1.2) | 6.20 (0.7) | 6.13 (0.6) | ||
| Emotional Role | F(1.3;53.3) = 28.50; p < 0.001 (0.404) | F(2.5;53.3) = 10.94; p < 0.001* (0.343) | |||
| H+D (13) | 4.46 (1.2) | 5.31 (1.1) | 5.62 (0.9) | ||
| Dry Land (17) | 4.65 (1.0) | 4.53 (0.9) | 4.53 (0.9) | ||
| AT (15) | 4.67 (1.0) | 5.93 (0.3) | 6.00 (0.0) | ||
| Mental Health | F(1.4;58.4) = 41.05; p < 0.001 (0.494) | F(2.8;58.4) = 8.83; p < 0.001* (0.296) | |||
| H+D (13) | 20.00 (2.6) | 20.77 (1.7) | 21.69 (1.7) | ||
| Dry Land (17) | 20.35 (1.1) | 20.53 (1.1) | 20.53 (1.1) | ||
| AT (15) | 20.40 (1.5) | 22.20 (1.1) | 22.73 (0.9) |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-de la Cruz, S. Influence of an Aquatic Therapy Program on Perceived Pain, Stress, and Quality of Life in Chronic Stroke Patients: A Randomized Trial. Int. J. Environ. Res. Public Health 2020, 17, 4796. https://doi.org/10.3390/ijerph17134796
Pérez-de la Cruz S. Influence of an Aquatic Therapy Program on Perceived Pain, Stress, and Quality of Life in Chronic Stroke Patients: A Randomized Trial. International Journal of Environmental Research and Public Health. 2020; 17(13):4796. https://doi.org/10.3390/ijerph17134796
Chicago/Turabian StylePérez-de la Cruz, Sagrario. 2020. "Influence of an Aquatic Therapy Program on Perceived Pain, Stress, and Quality of Life in Chronic Stroke Patients: A Randomized Trial" International Journal of Environmental Research and Public Health 17, no. 13: 4796. https://doi.org/10.3390/ijerph17134796
APA StylePérez-de la Cruz, S. (2020). Influence of an Aquatic Therapy Program on Perceived Pain, Stress, and Quality of Life in Chronic Stroke Patients: A Randomized Trial. International Journal of Environmental Research and Public Health, 17(13), 4796. https://doi.org/10.3390/ijerph17134796