Investigation of the Trend in Adolescent Mental Health and its Related Social Factors: A Multi-Year Cross-Sectional Study For 13 Years


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethics Approval and Consent to Participate
2.3. Assessment
2.4. Social Index
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
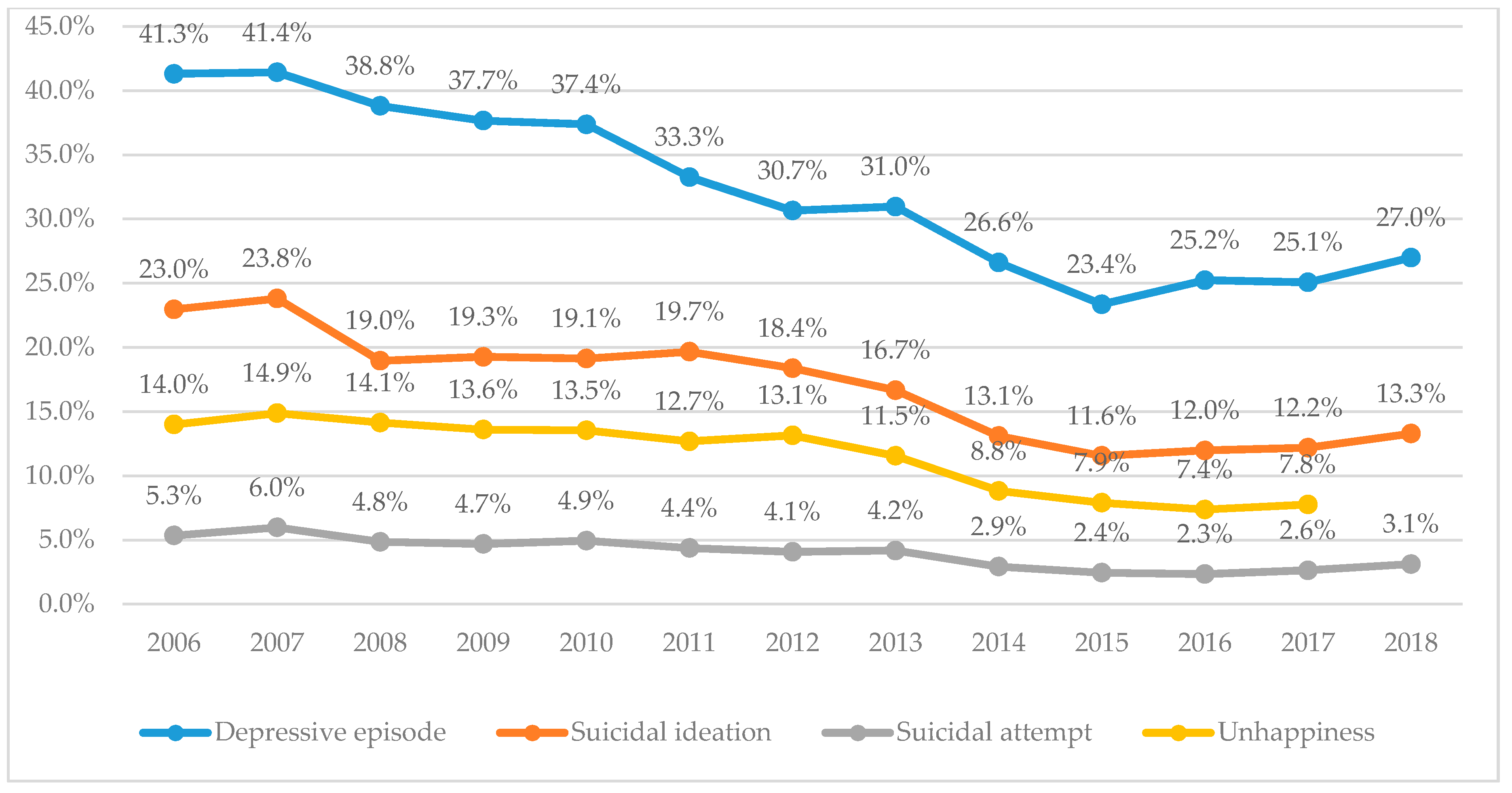
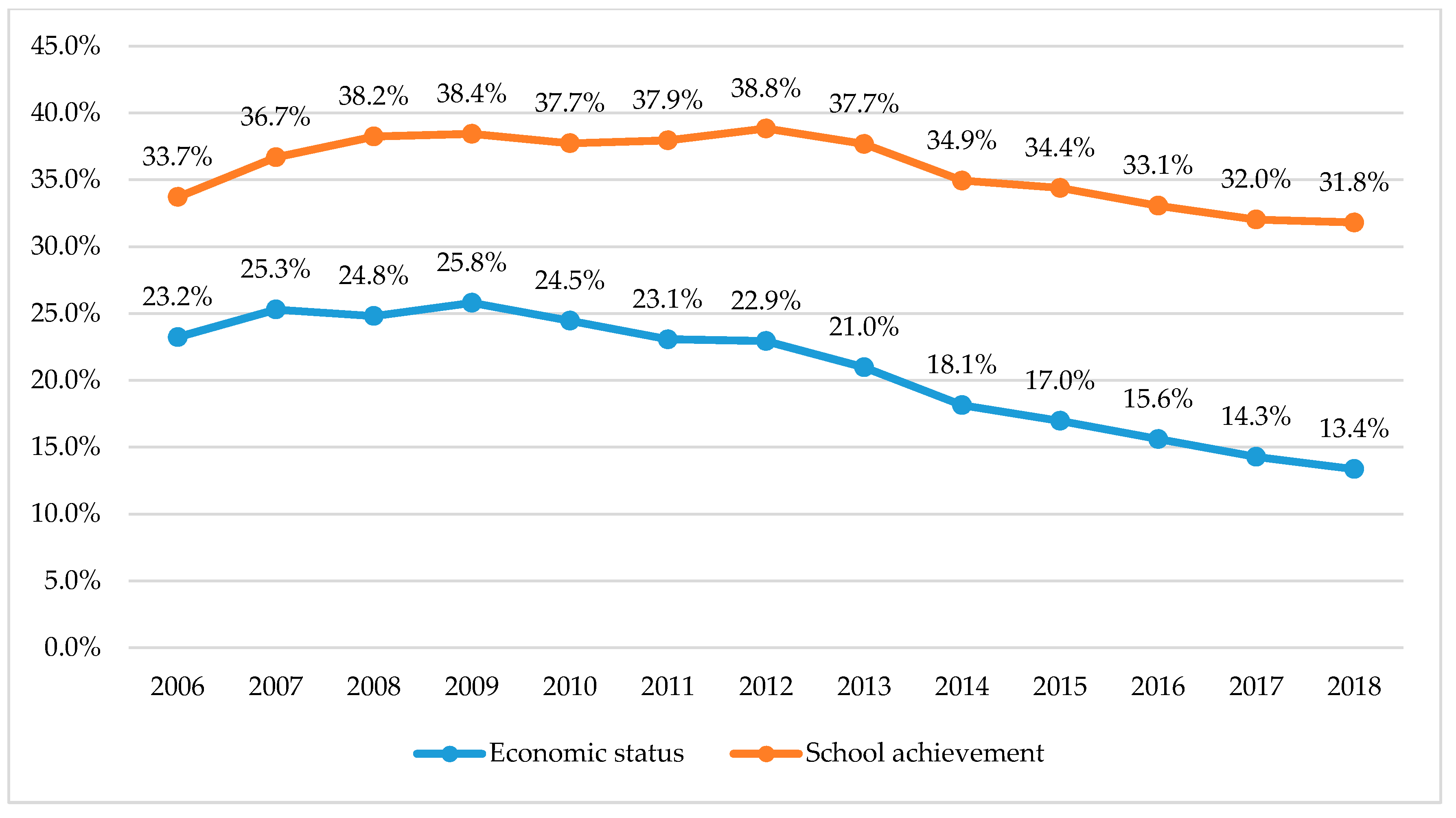
3.2. Change of Prevalence for Mental Health Outcome Variables at Each Year
3.3. Association Between the Mental Health Outcomes and the Demographic Variables
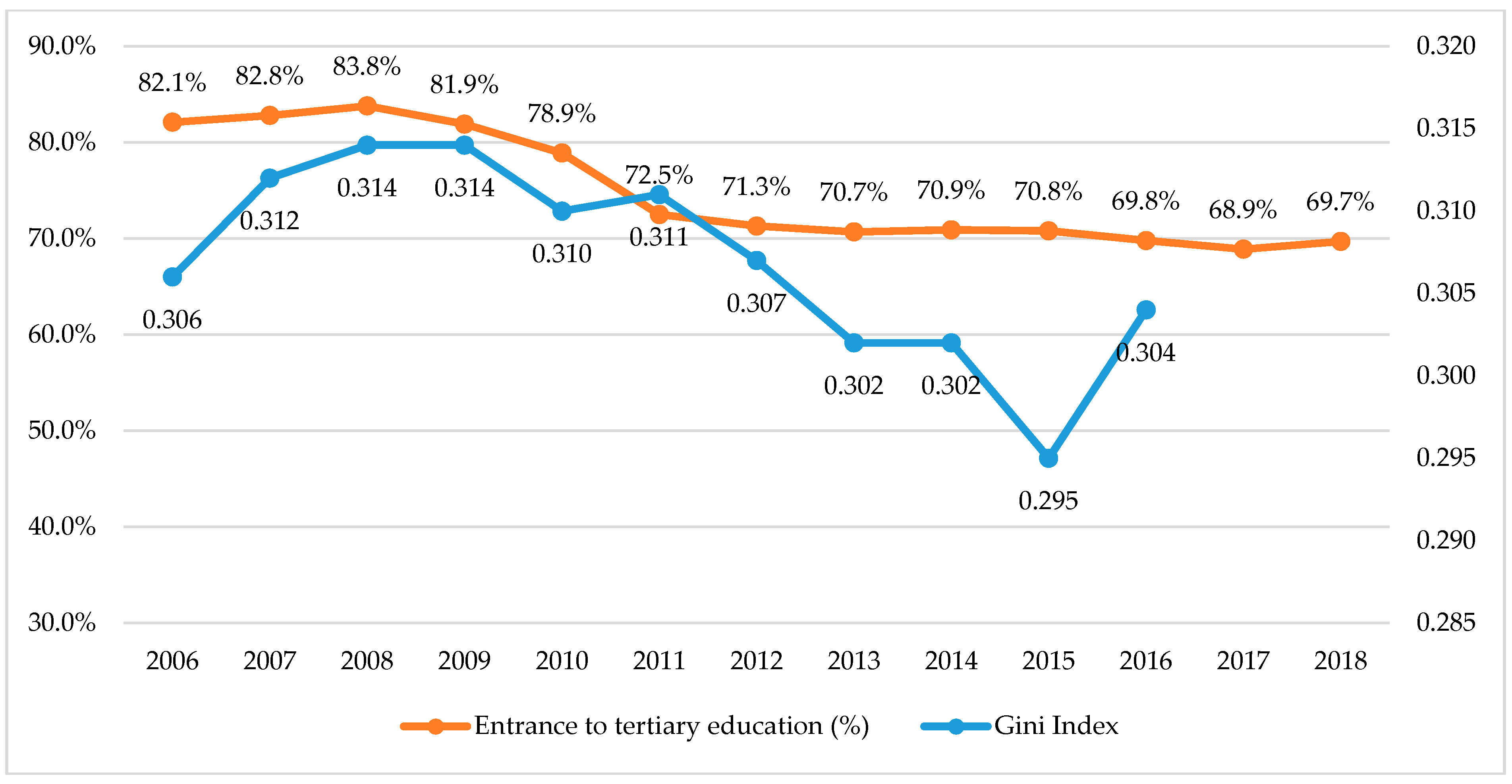
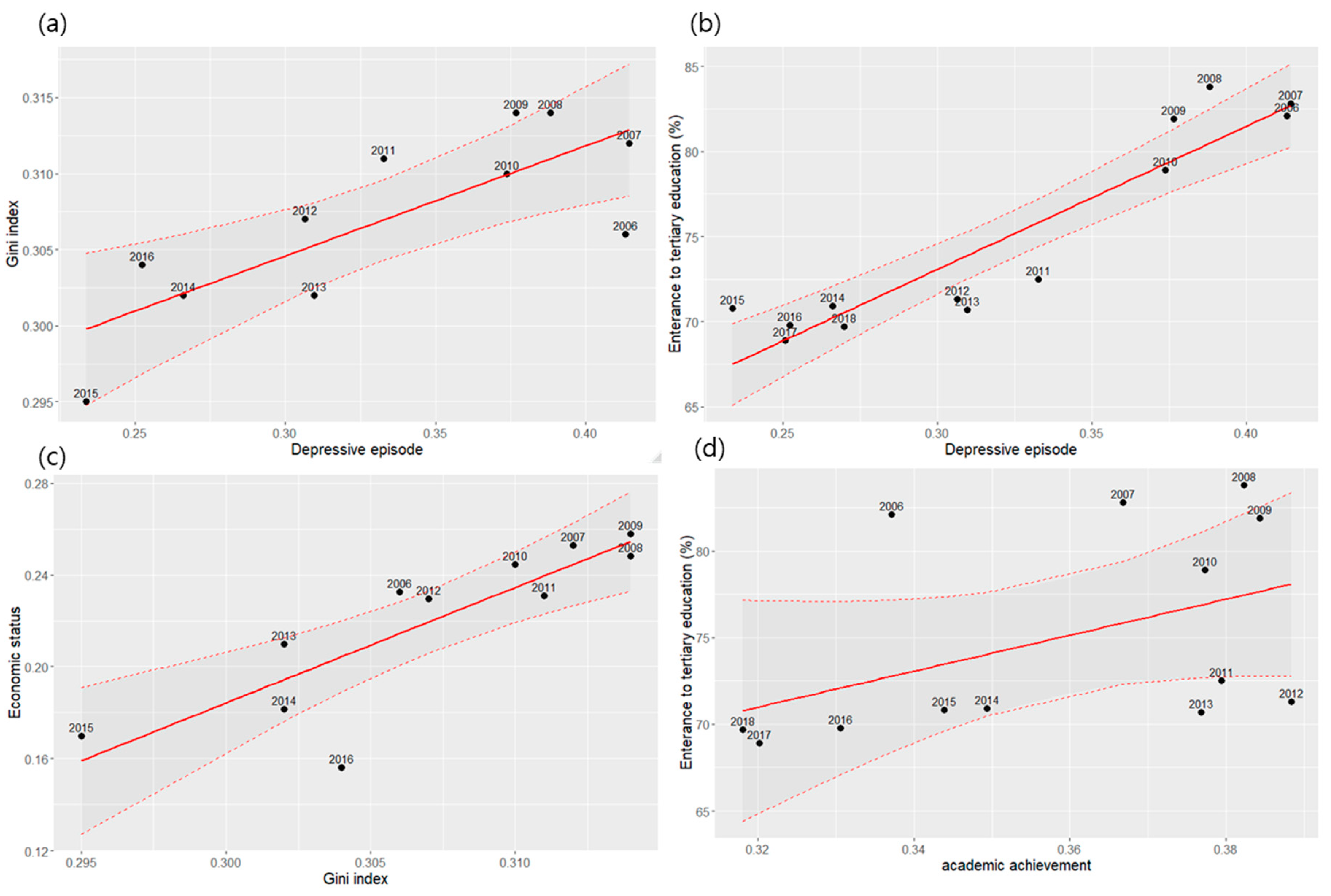
3.4. Association between the Change in Mental Health Outcome and Korean Social Index
4. Discussion
4.1. Economic Inequality
4.2. Academic Achievement
4.3. Parental Education
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Steinberg, L. Adolescence, 5th ed.; McGraw-Hill: Boston, MA, USA; New York, NY, USA, 1999. [Google Scholar]
- Griffin, A. Adolescent neurological development and implications for health and well-being. Healthcare 2017, 5, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smetana, J.G.; Campione-Barr, N.; Metzger, A. Adolescent development in interpersonal and societal contexts. Annu. Rev. Psychol. 2006, 57, 255–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarrett, N.; Eccles, J. The passage to adulthood: Challenges of late adolescence. New Dir. Youth Dev. 2006, 111, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Paus, T.; Keshavan, M.; Giedd, J.N. Why do many psychiatric disorders emerge during adolescence? Nat. Rev. Neurosci. 2008, 9, 947–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Avenevoli, S.; Merikangas, K.R. Mood disorders in children and adolescents: An epidemiologic perspective. Biol. Psychiatry 2001, 49, 1002–1014. [Google Scholar] [CrossRef]
- Green, H.; McGinnity, Á.; Meltzer, H.; Ford, T.; Goodman, R. Mental Health of Children and Young People in Great Britain, 2004; Palgrave Macmillan Basingstoke: London, UK, 2005. [Google Scholar]
- Hankin, B.L.; Abramson, L.Y.; Moffitt, T.E.; Silva, P.A.; McGee, R.; Angell, K.E. Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. J. Abnorm. Psychol. 1998, 107, 128. [Google Scholar] [CrossRef]
- Saluja, G.; Iachan, R.; Scheidt, P.C.; Overpeck, M.D.; Sun, W.; Giedd, J.N. Prevalence of and risk factors for depressive symptoms among young adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Twenge, J.M.; Nolen-Hoeksema, S. Age, gender, race, socioeconomic status, and birth cohort difference on the children’s depression inventory: A meta-analysis. J. Abnorm. Psychol. 2002, 111, 578. [Google Scholar] [CrossRef]
- Merikangas, K.R.; He, J.-P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in US adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [Green Version]
- GH, S.; MJ, C. Prevalence of Depressive Symptoms among Adolescents Residing in Community. Psychiatry 1997, 22, 113–126. [Google Scholar]
- Radloff, L.S. A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Cho, S.J.; Jeon, H.J.; Kim, M.J.; Kim, J.K.; Kim, U.S.; Lyoo, I.K.; Cho, M.J. Prevalence and correlates of depressive symptoms among the adolescents in an urban area in Korea. J. Korean Neuropsychiatr. Assoc. 2001, 40, 627–639. [Google Scholar]
- Kim, M. The prevalence of depression of middle school students in a city, and the effect of depression on the school adjustment. Korean J. Couns. 2008, 9, 645–658. [Google Scholar]
- Jane Costello, E.; Erkanli, A.; Angold, A. Is there an epidemic of child or adolescent depression? J. Child Psychol. Psychiatry 2006, 47, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Collishaw, S. Trends in adolescent depression: A review of the evidence. In Depression in Childhood and Adolescence: The way Forward; Association of Child and Adolescent Mental Health: London, UK, 2009; pp. 7–18. [Google Scholar]
- Robinson, M.; Oddy, W.H.; Li, J.; Kendall, G.E.; De Klerk, N.H.; Silburn, S.R.; Zubrick, S.R.; Newnham, J.P.; Stanley, F.J.; Mattes, E. Pre-and postnatal influences on preschool mental health: A large-scale cohort study. J. Child Psychol. Psychiatry 2008, 49, 1118–1128. [Google Scholar] [CrossRef] [PubMed]
- Tennant, C. Life events, stress and depression: A review of recent findings. Aust. N. Z. J. Psychiatry 2002, 36, 173–182. [Google Scholar] [CrossRef]
- Compton, M.T.; Shim, R.S. The social determinants of mental health. Focus 2015, 13, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Lund, C.; Brooke-Sumner, C.; Baingana, F.; Baron, E.C.; Breuer, E.; Chandra, P.; Haushofer, J.; Herrman, H.; Jordans, M.; Kieling, C. Social determinants of mental disorders and the Sustainable Development Goals: A systematic review of reviews. Lancet Psychiatry 2018, 5, 357–369. [Google Scholar] [CrossRef]
- Paananen, R.; Ristikari, T.; Merikukka, M.; Gissler, M. Social determinants of mental health: A Finnish nationwide follow-up study on mental disorders. J. Epidemiol. Community Health 2013, 67, 1025–1031. [Google Scholar] [CrossRef] [Green Version]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Pabayo, R.; Dunn, E.C.; Gilman, S.E.; Kawachi, I.; Molnar, B.E. Income inequality within urban settings and depressive symptoms among adolescents. J. Epidemiol. Community Health 2016, 70, 997–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elgar, F.J.; Roberts, C.; Parry-Langdon, N.; Boyce, W. Income inequality and alcohol use: A multilevel analysis of drinking and drunkenness in adolescents in 34 countries. Eur. J. Public Health 2005, 15, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.B.; Yates, S. Academic expectations as sources of stress in Asian students. Soc. Psychol. Educ. 2011, 14, 389–407. [Google Scholar] [CrossRef]
- Sonego, M.; Llácer, A.; Galán, I.; Simón, F. The influence of parental education on child mental health in Spain. Qual. Life Res. 2013, 22, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Von Rueden, U.; Gosch, A.; Rajmil, L.; Bisegger, C.; Ravens-Sieberer, U. Socioeconomic determinants of health related quality of life in childhood and adolescence: Results from a European study. J. Epidemiol. Community Health 2006, 60, 130–135. [Google Scholar] [CrossRef]
- Lee, J.-W. The Republic of Korea’s economic growth and catch-up: Implications for the People’s Republic of China. China World Econ. 2016, 24, 71–97. [Google Scholar] [CrossRef]
- Center for Educational Statistics Information. Situations after the Graduation from the High School; Chungbuk Center for Educational Statistics Information: Cheongju-si, Korea, 2018. [Google Scholar]
- Ahn, K. A study of determinants of the birthrate change in South Korea. Available online: https://www.martin.uky.edu/sites/martin.uky.edu/files/Capstone_Projects/Capstones_2015/Ahn.pdf (accessed on 30 May 2020).
- Kim, I. Socioeconomic Concentration in the Seoul metropolitan Area and its implications in the urbanization process of Korea. Korea J. Sociol. 2010, 44, 111–128. [Google Scholar]
- Yoo, G. Changing views on family diversity in urban Korea. J. Comp. Fam. Stud. 2006, 37, 59–74. [Google Scholar] [CrossRef]
- Lee, H.; Rhee, C. Lessons from the 1997 and the 2008 Crises in Korea. Asian Econ. Policy Rev. 2012, 7, 47–64. [Google Scholar] [CrossRef]
- Chan, C.H.; Caine, E.D.; You, S.; Fu, K.W.; Chang, S.S.; Yip, P.S.F. Suicide rates among working-age adults in South Korea before and after the 2008 economic crisis. J. Epidemiol. Community Health 2014, 68, 246–252. [Google Scholar] [CrossRef]
- Kim, Y.; Choi, S.; Chun, C.; Park, S.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea youth risk behavior web-based survey (KYRBS). Int. J. Epidemiol. 2016, 45, 1076. [Google Scholar] [CrossRef] [Green Version]
- Statistics Korea. Income Distribution Index; Statistics Korea: Daejeon, Korea, 2016.
- Giugni, C. Variabilità e mutabilità: Contributo allo Studio delle Distribuzioni e delle Relazioni Statistiche; Cuppini: Bologna, Italy, 1912. [Google Scholar]
- Statistics Korea. Suicide in Adolescents Aged 15–19; Statistics Korea: Daejeon, Korea, 2018. [Google Scholar]
- OECD. Health at a Glance. 2018: OECD Indicators; OECD Publishing: Paris, France, 2018; p. 56. [Google Scholar]
- Statistics Korea. Causes of Death Statistics in Adolescent Aged 15–19; Statistics Korea: Daejeon, Korea, 2018.
- Statistics Korea. Suicide in Adults; Statistics Korea: Daejeon, Korea, 2018.
- Mojtabai, R.; Olfson, M.; Han, B. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics 2016, 138, e20161878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letourneau, N.L.; Duffett-Leger, L.; Levac, L.; Watson, B.; Young-Morris, C. Socioeconomic status and child development: A meta-analysis. J. Emot. Behav. Disord. 2013, 21, 211–224. [Google Scholar] [CrossRef]
- Patel, V.; Lund, C.; Hatherill, S.; Plagerson, S.; Corrigall, J.; Funk, M.; Flisher, A.J. Mental disorders: Equity and social determinants. In Equity Social Determinants and Public Health Programmes; WHO: Geneva, Switzerland, 2010; pp. 115–134. [Google Scholar]
- Catalano, R.; Goldman-Mellor, S.; Saxton, K.; Margerison-Zilko, C.; Subbaraman, M.; LeWinn, K.; Anderson, E. The health effects of economic decline. Annu. Rev. Public Health 2011, 32, 431–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, K.A.; Costello, E.J.; Leblanc, W.; Sampson, N.A.; Kessler, R.C. Socioeconomic status and adolescent mental disorders. Am. J. Public Health 2012, 102, 1742–1750. [Google Scholar] [CrossRef]
- Yu, Z.; Wang, F. Income inequality and happiness: An inverted U-shaped curve. Front. Psychol. 2017, 8, 2052. [Google Scholar] [CrossRef]
- Popov, V. Billionaires, Millionaires, Inequality, and Happiness. Available online: https://ideas.repec.org/p/pra/mprapa/94081.html (accessed on 25 July 2020).
- World Bank Data. GDP Per Capita (Current US$)—Korea, Rep. Ghana, Japan. 2018. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?end=1960&locations=KR-GH-JP&start=1960&view=bar (accessed on 20 October 2019).
- Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Soc. Sci. Med. 2013, 90, 24–31. [Google Scholar] [CrossRef]
- Ang, R.P.; Klassen, R.M.; Chong, W.H.; Huan, V.S.; Wong, I.Y.; Yeo, L.S.; Krawchuk, L.L. Cross-cultural invariance of the academic expectations stress inventory: Adolescent samples from Canada and Singapore. J. Adolesc. 2009, 32, 1225–1237. [Google Scholar] [CrossRef]
- OECD. Education at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Lee, M.; Larson, R. The Korean ‘examination hell’: Long hours of studying, distress, and depression. J. Youth Adolesc. 2000, 29, 249–271. [Google Scholar] [CrossRef]
- Kim, K. What makes adolescents psychologically distressed? Life events as riskfactors for depression and suicide. Eur Child. Adolesc Psychiatry 2020, 30, 2020. [Google Scholar]
- McLaughlin, K.A.; Breslau, J.; Green, J.G.; Lakoma, M.D.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Childhood socio-economic status and the onset, persistence, and severity of DSM-IV mental disorders in a US national sample. Soc. Sci. Med. 2011, 73, 1088–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiss, F.; Meyrose, A.-K.; Otto, C.; Lampert, T.; Klasen, F.; Ravens-Sieberer, U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: Results of the German BELLA cohort-study. PLoS ONE 2019, 14, e0213700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, O.; Harmon, C.; Walker, I. The Impact of Parental Income and Education on Child Health: Further Evidence for England. Available online: https://ideas.repec.org/p/wrk/warwec/788.html (accessed on 24 July 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unweighted n (%) | |
|---|---|
| Total | 919,855 (100.0) |
| Male | 474,264 (51.6) |
| Female | 445,591 (48.4) |
| Age; mean (SD) | 15.46 (1.72) |
| Grade | |
| 7th (Middle school 1st) | 154,385 (16.8) |
| 8th (Middle school 2nd) | 155,759 (16.9) |
| 9th (Middle school 3rd) | 157,107 (17.1) |
| 10th (High school 1st) | 152,425 (16.6) |
| 11th (High school 2nd) | 151,834 (16.5) |
| 12th (High school 3rd) | 148,345 (16.1) |
| Economic status | |
| High | 69,370 (7.5) |
| High middle | 223,162 (24.3) |
| Middle | 434,453 (47.2) |
| Low middle | 148,476 (16.1) |
| Low | 44,394 (4.8) |
| Academic achievement | |
| High | 111,030 (12.1) |
| High middle | 224,742 (24.4) |
| Middle | 253,275 (27.5) |
| Low middle | 224,026 (24.4) |
| Low | 106,782 (11.6) |
| Paternal educational level | |
| <12 years | 44,838 (4.9) |
| 12 years | 306,340 ((33.3) |
| >12 years | 394,845 (42.9) |
| Unknown | 173,882 (18.9) |
| Maternal educational level | |
| <12 years | 45,177 (4.9) |
| 12 years | 387,817 (42.2) |
| >12 years | 316,408 (34.4) |
| Unknown | 170,453 (18.5) |
| Depressive episode | |
| Yes | 299,056 (32.5) |
| No | 620,796 (67.5) |
| Suicidal ideation | |
| Yes | 158,193 (17.2) |
| No | 761,659 (82.8) |
| Suicidal attempt | |
| Yes | 37,201 (4.0) |
| No | 882,654 (96.0) |
| Variables | Model 1 (n = 859.815) | Model 2 (n = 651.533) | ||||
|---|---|---|---|---|---|---|
| F | p | Partial η2 | F | p | Partial η2 | |
| Economic status | 7936 | <0.001 | 0.0356 | 5180 | <0.001 | 0.0308 |
| Academic achievement | 2662 | <0.001 | 0.0122 | 2110 | <0.001 | 0.0128 |
| Sex | 2748 | <0.001 | 0.0032 | 1565 | <0.001 | 0.0024 |
| Grade | 553 | <0.001 | 0.0032 | 332 | <0.001 | 0.0025 |
| Paternal educational level | 49 | <0.001 | 0.0002 | |||
| Maternal educational level | 116 | <0.001 | 0.0004 | |||
| Depressive Episode | Suicidal Ideation | Suicidal Attempt | |
|---|---|---|---|
| Sex a | |||
| Male | referent | referent | referent |
| Female | 1.63 * | 1.71 * | 1.77 * |
| Grade a | |||
| 7th | referent | referent | referent |
| 8th | 1.10 * | 1.05 * | 1.00 |
| 9th | 1.20 * | 1.04 * | 0.92 * |
| 10th | 1.25 * | 0.95 * | 0.77 * |
| 11th | 1.32 * | 0.95 * | 0.70 * |
| 12th | 1.45 * | 0.91* | 0.63 * |
| Economic status a | |||
| High | referent | referent | referent |
| High middle | 0.92 * | 0.88 * | 0.63 * |
| Middle | 0.89 * | 0.87 * | 0.58 * |
| Low middle | 1.26* | 1.36 * | 0.89 * |
| Low | 1.80* | 2.13 * | 1.77 * |
| Academic achievements a | |||
| High | referent | referent | referent |
| High middle | 1.08 * | 0.98 | 0.86 * |
| Middle | 1.16 * | 1.01 | 0.99 |
| Low middle | 1.39 * | 1.24 * | 1.31 * |
| Low | 1.71* | 1.55* | 1.97 * |
| Paternal educational level b | |||
| >12 years | referent | referent | referent |
| 12 years | 0.93 * | 0.93 * | 0.98 |
| <12 years | 1.00 | 1.03 | 1.15 * |
| Maternal educational level b | |||
| >12 years | referent | referent | referent |
| 12 years | 1.02 | 1.00 | 0.99 |
| <12 years | 1.13 * | 1.16* | 1.15* |
| n = 13 (between 2006 and 2018) | Depressive Episode | Suicidal Ideation | Suicidal Attempt | Subjective Unhappiness | Economic Status | School Achievement | |
|---|---|---|---|---|---|---|---|
| Social index | Gini index | 0.789 ** | 0.724 * | 0.740 ** | 0.798 ** | 0.845 ** | 0.616 * |
| Tertiary education (%) | 0.930 ** | 0.809 ** | 0.851 ** | 0.813 ** | 0.812 ** | 0.453 | |
| Subjective response | Economic status | 0.880 ** | 0.882 ** | 0.890 ** | 0.972 ** | 1 | 0.852 ** |
| School achievement | 0.542 | 0.582 * | 0.608 * | 0.724 ** | 0.852 ** | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.M.; Kim, D.; Chung, U.S. Investigation of the Trend in Adolescent Mental Health and its Related Social Factors: A Multi-Year Cross-Sectional Study For 13 Years. Int. J. Environ. Res. Public Health 2020, 17, 5405. https://doi.org/10.3390/ijerph17155405
Kim KM, Kim D, Chung US. Investigation of the Trend in Adolescent Mental Health and its Related Social Factors: A Multi-Year Cross-Sectional Study For 13 Years. International Journal of Environmental Research and Public Health. 2020; 17(15):5405. https://doi.org/10.3390/ijerph17155405
Chicago/Turabian StyleKim, Kyoung Min, Dohyun Kim, and Un Sun Chung. 2020. "Investigation of the Trend in Adolescent Mental Health and its Related Social Factors: A Multi-Year Cross-Sectional Study For 13 Years" International Journal of Environmental Research and Public Health 17, no. 15: 5405. https://doi.org/10.3390/ijerph17155405
APA StyleKim, K. M., Kim, D., & Chung, U. S. (2020). Investigation of the Trend in Adolescent Mental Health and its Related Social Factors: A Multi-Year Cross-Sectional Study For 13 Years. International Journal of Environmental Research and Public Health, 17(15), 5405. https://doi.org/10.3390/ijerph17155405