Wider Dental Care Coverage Associated with Lower Oral Health Inequalities: A Comparison Study between Japan and England


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
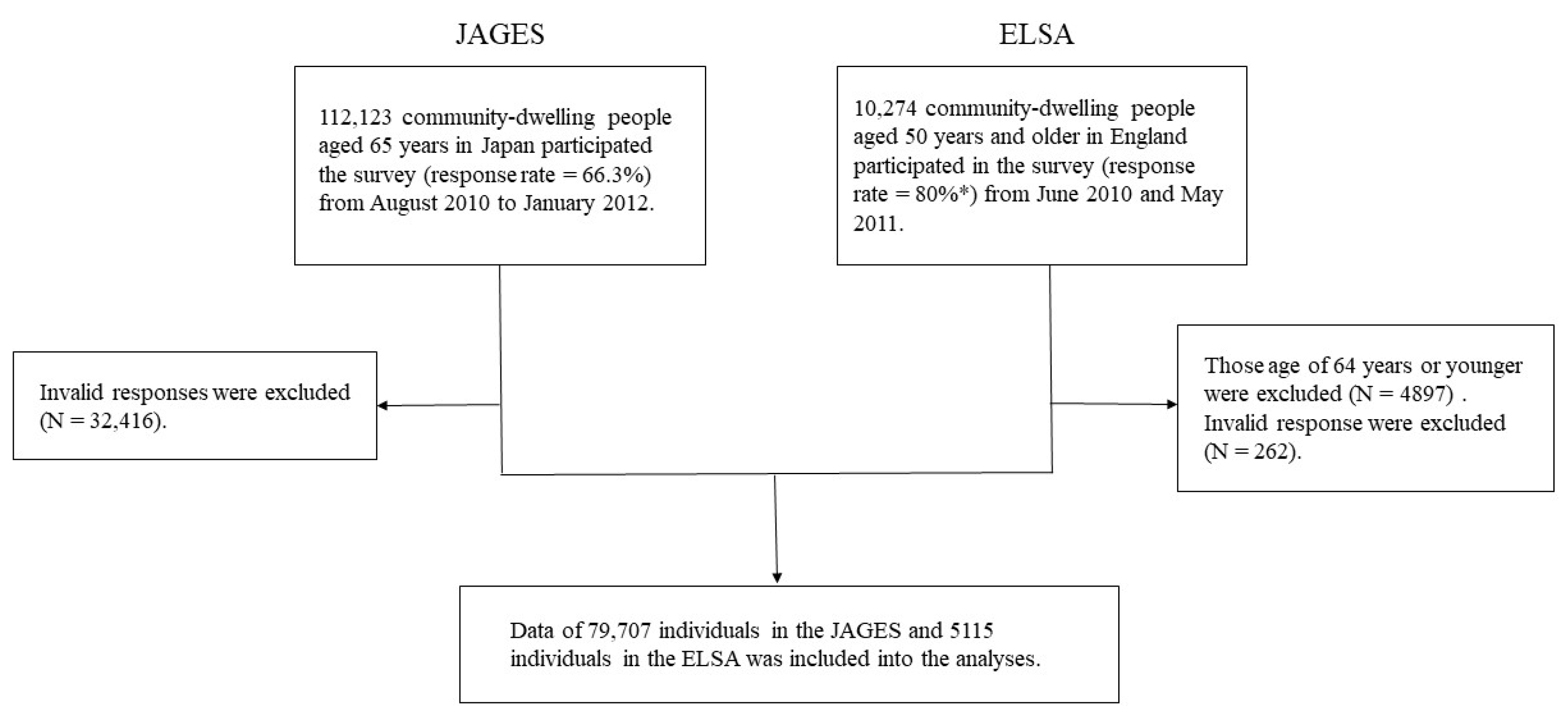
2.1. Participants
2.2. Ethical Considerations
2.3. Dependent Variable
2.4. Explanatory Variables
2.5. Data Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | Confidence Interval |
| ELSA | English Longitudinal Study of Ageing |
| OECD | Organisation for Economic Co-operation and Development |
| JAGES | Japan Gerontological Evaluation Study |
| NHS | National Health Service |
| RII | Relative Index of Inequality |
| UK | United Kingdom |
| SII | Slope Index of Inequality |
| WHO | World Health Organisation |
References
- Butkus, R.; Rapp, K.; Cooney, T.G.; Engel, L.S. Envisioning a better U.S. health care system for all: Reducing barriers to care and addressing social determinants of health. Ann. Intern. Med. 2020, 172, S50–S59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikegami, N.; Yoo, B.K.; Hashimoto, H.; Matsumoto, M.; Ogata, H.; Babazono, A.; Watanabe, R.; Shibuya, K.; Yang, B.M.; Reich, M.R.; et al. Japanese universal health coverage: Evolution, achievements, and challenges. Lancet 2011, 378, 1106–1115. [Google Scholar] [CrossRef]
- Baxter, S.; Johnson, M.; Chambers, D.; Sutton, A.; Goyder, E.; Booth, A. The effects of integrated care: A systematic review of UK and international evidence. BMC Health Serv. Res. 2018, 18, 350. [Google Scholar] [CrossRef] [PubMed]
- Ridic, G.; Gleason, S.; Ridic, O. Comparisons of health care systems in the United States, Germany and Canada. Mater. Socio Med. 2012, 24, 112–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreno, C.C.; Celeste, R.K.; et al. Ending the neglect of global oral health: Time for radical action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreno, C.C.; Celeste, R.K.; et al. The Lancet oral health series: Implications for oral and dental research. J. Dent. Res. 2020, 99, 8–10. [Google Scholar] [CrossRef]
- Zaitsu, T.; Saito, T.; Kawaguchi, Y. The oral healthcare system in Japan. Healthcare 2018, 6, 79. [Google Scholar] [CrossRef] [Green Version]
- NHS Dental Services in England: An Independent Review by Professor Jimmy Steele. Available online: http://www.sigwales.org/wp-content/uploads/dh_101180.pdf (accessed on 29 July 2020).
- OECD. Health Care Resources, Dentist’s Consultation. Available online: https://stats.oecd.org/index.aspx?queryid=30161 (accessed on 19 February 2020).
- Ministry of Internal Affairs and Communications. Family Income and Expenditure Survey. Available online: https://www.stat.go.jp/data/kakei/index3.html (accessed on 19 February 2020).
- Office for National Statistics. Consumer Trends, UK Statistical Bulletins. Available online: https://www.ons.gov.uk/economy/nationalaccounts/satelliteaccounts/bulletins/consumertrends/previousReleases (accessed on 25 February 2020).
- Coronini-Cronberg, S.; Millett, C.; Laverty, A.A.; Webb, E. The impact of a free older persons’ bus pass on active travel and regular walking in England. Am. J. Public Health 2012, 102, 2141–2148. [Google Scholar] [CrossRef]
- Fujita, M.; Sato, Y.; Nagashima, K.; Takahashi, S.; Hata, A. Income related inequality of health care access in Japan: A retrospective cohort study. PLoS ONE 2016, 11, e0151690. [Google Scholar] [CrossRef] [Green Version]
- Kiuchi, S.; Aida, J.; Kusama, T.; Yamamoto, T.; Hoshi, M.; Yamamoto, T.; Kondo, K.; Osaka, K. Does public transportation reduce inequalities in access to dental care among older adults? Japan Gerontological Evaluation Study. Community Dent. Oral 2019. [Google Scholar] [CrossRef]
- Murakami, K.; Aida, J.; Ohkubo, T.; Hashimoto, H. Income-related inequalities in preventive and curative dental care use among working-age Japanese adults in urban areas: A cross-sectional study. BMC Oral Health 2014, 14, 117. [Google Scholar] [CrossRef] [Green Version]
- Nishide, A.; Fujita, M.; Sato, Y.; Nagashima, K.; Takahashi, S.; Hata, A. Income-related inequalities in access to dental care services in Japan. Int. J. Environ. Res. Public Health 2017, 14, 524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravaghi, V.; Hargreaves, D.S.; Morris, A.J. Persistent socioeconomic inequality in child dental caries in England despite equal attendance. JDR Clin. Trans. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe tooth loss: A systematic review and meta-analysis. JDR 2014, 93, 20s–28s. [Google Scholar] [CrossRef] [Green Version]
- Polzer, I.; Schimmel, M.; Muller, F.; Biffar, R. Edentulism as part of the general health problems of elderly adults. Int. Dental J. 2010, 60, 143–155. [Google Scholar]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. JDR 2013, 92, 592–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondo, K. Progress in aging epidemiology in Japan: The JAGES project. J. Epidemiol. 2016, 26, 331–336. [Google Scholar] [CrossRef] [Green Version]
- Steptoe, A.; Breeze, E.; Banks, J.; Nazroo, J. Cohort profile: The English longitudinal study of ageing. Int. J. Epidemiol. 2013, 42, 1640–1648. [Google Scholar] [CrossRef] [Green Version]
- Evidence from the English Longitudinal Study of Ageing 2002–2010 (Wave5) Technical Report. Available online: http://doc.ukdataservice.ac.uk/doc/5050/mrdoc/pdf/5050_elsa_w5_technical_report_v1.pdf (accessed on 29 July 2020).
- Mackenbach, J.P.; Kunst, A.E. Measuring the magnitude of socio-economic inequalities in health: An overview of available measures illustrated with two examples from Europe. Soc. Sci. Med. 1997, 44, 757–771. [Google Scholar] [CrossRef]
- Ernstsen, L.; Strand, B.H.; Nilsen, S.M.; Espnes, G.A.; Krokstad, S. Trends in absolute and relative educational inequalities in four modifiable ischaemic heart disease risk factors: Repeated cross-sectional surveys from the Nord-Trondelag Health Study (HUNT) 1984–2008. BMC Public Health 2012, 12, 266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakami, K.; Ohkubo, T.; Nakamura, M.; Ninomiya, T.; Ojima, T.; Shirai, K.; Nagahata, T.; Kadota, A.; Okuda, N.; Nishi, N.; et al. Socioeconomic inequalities in oral health among middle-aged and elderly Japanese: NIPPON DATA2010. J. Epidemiol. 2018, 28 (Suppl. 3), S59–S65. [Google Scholar] [CrossRef]
- Aida, J.; Kondo, K.; Kondo, N.; Watt, R.G.; Sheiham, A.; Tsakos, G. Income inequality, social capital and self-rated health and dental status in older Japanese. Soc. Sci. Med. 2011, 73, 1561–1568. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Angulo, E.K.; Mangal, M.; Bernabe, E. Socioeconomic inequalities in adult oral health across different ethnic groups in England. Health Qual. Life Out 2019, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Tsakos, G.; Demakakos, P.; Breeze, E.; Watt, R.G. Social gradients in oral health in older adults: Findings from the English longitudinal survey of aging. Am. J. Public Health 2011, 101, 1892–1899. [Google Scholar] [CrossRef]
- Delgado-Angulo, E.K.; Marcenes, W.; Harding, S.; Bernabe, E. Ethnicity, migration status and dental caries experience among adults in East London. Community Dent. Oral 2018, 46, 392–399. [Google Scholar] [CrossRef]
- Public Health England. National Dental Epidemiology Programme for England: Oral Health Survey of Five-Year-Old Children 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/768368/NDEP_for_England_OH_Survey_5yr_2017_Report.pdf (accessed on 29 July 2020).
- Delgado-Angulo, E.K.; Bernabe, E.; Marcenes, W. Ethnic inequalities in periodontal disease among British adults. J. Clin. Periodontol. 2016, 43, 926–933. [Google Scholar] [CrossRef] [Green Version]
- Hakeem, F.F.; Sabbah, W. Is there socioeconomic inequality in periodontal disease among adults with optimal behaviours. Acta Odontol. 2019, 77, 400–407. [Google Scholar] [CrossRef]
- McGrath, C.; Bedi, R.; Dhawan, N. Factors influencing older people’s self reported use of dental services in the UK. Gerodontology 1999, 16, 97–102. [Google Scholar] [CrossRef]
- Healthwatch England. Evidence Review, Access to NHS Dental Services: What People Told Local Healthwatch. Available online: https://www.caremanagementmatters.co.uk/wp-content/uploads/2019/08/access_to_nhs_dental_services_-_what_people_told_local_healthwatch_0.pdf (accessed on 29 July 2020).
- Hill, K.B.; White, D.A.; Morris, A.J.; Hall, A.C.; Goodwin, N.; Burke, F.J. National evaluation of personal dental services: A qualitative investigation into patients’ perceptions of dental services. Br. Dental J. 2003, 195, 654–656. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare. An Outline of the Japanese Medical System. Available online: https://www.mhlw.go.jp/bunya/iryouhoken/iryouhoken01/dl/01_eng.pdf (accessed on 27 July 2020).
- World Health Organisation and the International Bank for Reconstruction and Development. Tracking Universal Health Coverage: 2017 Global Monitoring Report. Available online: https://apps.who.int/iris/bitstream/handle/10665/259817/9789241513555-eng.pdf;jsessionid=1A842398D0610EBF0534E338380CAB2A?sequence=1 (accessed on 27 July 2020).
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreno, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | JAGES (N = 79,707) | Total | ELSA (N = 5115) | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | ||||
| Age | |||||||
| 65–69 year old | 24,567 | 1331 | 5.4% | 1537 | 172 | 11.2% | |
| 70–74 year old | 23,911 | 2322 | 9.7% | 1411 | 244 | 17.3% | |
| 75–79 year old | 17,152 | 2904 | 16.9% | 1029 | 239 | 23.2% | |
| 80–84 year old | 9506 | 2586 | 27.2% | 640 | 190 | 29.7% | |
| 85+ year old | 4571 | 1881 | 41.2% | 498 | 209 | 42.0% | |
| Sex | |||||||
| Men | 39,568 | 5491 | 13.9% | 2334 | 417 | 17.9% | |
| Women | 40,139 | 5533 | 13.8% | 2781 | 637 | 22.9% | |
| Income | |||||||
| Lowest | 21,076 | 4513 | 21.4% | 1278 | 356 | 27.9% | |
| Low | 19,455 | 2386 | 12.3% | 1280 | 322 | 25.2% | |
| Middle | 18,916 | 2058 | 10.9% | 1279 | 247 | 19.3% | |
| High | 20,260 | 2067 | 10.2% | 1278 | 129 | 10.1% | |
| Educational attainment | |||||||
| Low | 36,085 | 1934 | 21.0% | 2815 | 779 | 27.7% | |
| Middle | 28,603 | 714 | 10.5% | 1645 | 233 | 14.2% | |
| High | 15,019 | 297 | 8.2% | 655 | 42 | 6.4% | |
| JAGES (N = 79,707) | ELSA (N = 5115) | ||||
|---|---|---|---|---|---|
| Univariate Model | Age and Sex Adjusted Model | Univariate Model | Age and Sex Adjusted Model | ||
| Income | SII (%) (95% CI) | 11.77 (11.04; 12.50) | 9.24 (8.58; 9.90) | 18.46 (15.02; 21.90) | 14.35 (10.97; 17.73) |
| RII (95% CI) | 2.47 (2.34; 2.61) | 2.07 (1.96; 2.18) | 2.40 (2.03; 2.83) | 1.92 (1.63; 2.27) | |
| Educational attainment | SII (%) (95% CI) | 15.00 (14.18; 15.83) | 9.93 (9.19; 10.68) | 31.93 (28.22; 35.64) | 26.65 (23.11; 30.20) |
| RII (95% CI) | 3.36 (3.13; 3.61) | 2.45 (2.29; 2.63) | 5.88 (4.55; 7.61) | 4.79 (3.70; 6.19) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, K.; Cable, N.; Yamamoto, T.; Suzuki, K.; Kondo, K.; Osaka, K.; Tsakos, G.; Watt, R.G.; Aida, J. Wider Dental Care Coverage Associated with Lower Oral Health Inequalities: A Comparison Study between Japan and England. Int. J. Environ. Res. Public Health 2020, 17, 5539. https://doi.org/10.3390/ijerph17155539
Ito K, Cable N, Yamamoto T, Suzuki K, Kondo K, Osaka K, Tsakos G, Watt RG, Aida J. Wider Dental Care Coverage Associated with Lower Oral Health Inequalities: A Comparison Study between Japan and England. International Journal of Environmental Research and Public Health. 2020; 17(15):5539. https://doi.org/10.3390/ijerph17155539
Chicago/Turabian StyleIto, Kanade, Noriko Cable, Tatsuo Yamamoto, Kayo Suzuki, Katsunori Kondo, Ken Osaka, Georgios Tsakos, Richard G. Watt, and Jun Aida. 2020. "Wider Dental Care Coverage Associated with Lower Oral Health Inequalities: A Comparison Study between Japan and England" International Journal of Environmental Research and Public Health 17, no. 15: 5539. https://doi.org/10.3390/ijerph17155539
APA StyleIto, K., Cable, N., Yamamoto, T., Suzuki, K., Kondo, K., Osaka, K., Tsakos, G., Watt, R. G., & Aida, J. (2020). Wider Dental Care Coverage Associated with Lower Oral Health Inequalities: A Comparison Study between Japan and England. International Journal of Environmental Research and Public Health, 17(15), 5539. https://doi.org/10.3390/ijerph17155539