Assessing Global Frailty Scores: Development of a Global Burden of Disease-Frailty Index (GBD-FI)





Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of the GBD-FI
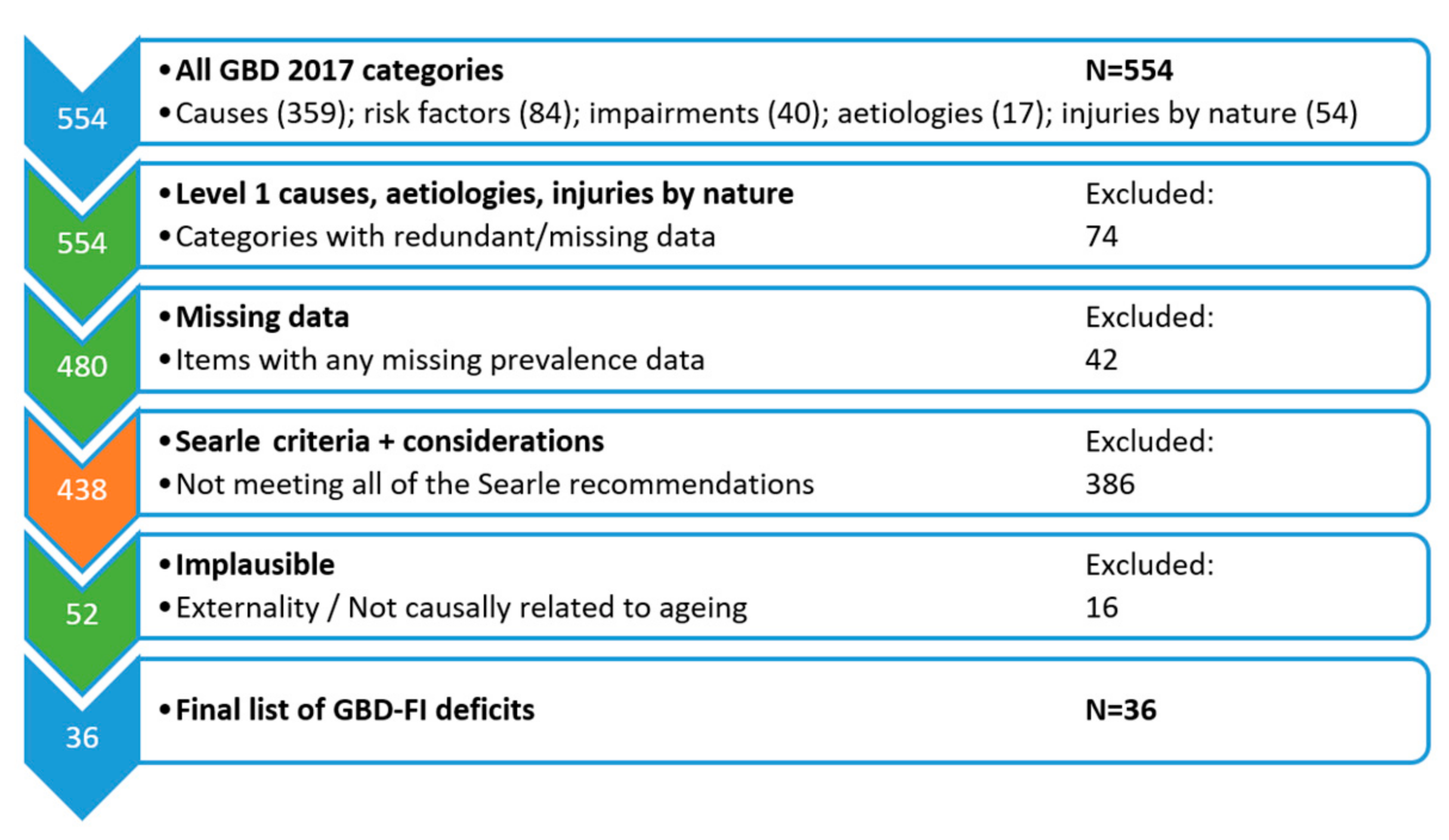
- Associated with health status: Deficits must have the potential to affect health. Hence, attributes that are not linked with health (e.g., greying hair) were not eligible for inclusion [11]. The GBD 2017 only includes items that result in poor health or cause death.
- Prevalence increases with age: Deficits should generally increase with age, although reductions at very advanced ages due to survivor effects must be considered [11]. Spearman’s coefficient was calculated for prevalence across the adult age groups (25–29 to ≥95 years). A cut-off of ≥0.7, denoting strong positive correlation with age [27], was applied.
- Must not saturate too early: Conditions that increase with age but reach a very high prevalence before old age should be excluded e.g., presbyopia is almost universal by age 55 and thus should be excluded [11]. A cut-off of >80% prevalence has previously been applied to exclude very common conditions in older populations [20]. We also applied this cut-off for the GBD age group of ≥70 years.
- Cover a range of systems: If all the index items measure the same characteristic, for example if they all measure cognition, then they are not representative of frailty [11], which is characterised by a decline in function across multiple organ systems [28]. To address this, all sections of the GBD 2017 were considered during item selection including ‘causes’, ‘risk factors’ and ‘impairments’.
- A single frailty index is to be used serially on the same people: GBD data represents population-level estimates. However, items that were missing prevalence data were excluded so a consistent list of items was available if serially comparing the same population.
- Low prevalence: Items with a low prevalence lack the variability necessary for meaningful comparisons. A cut-off of ≥1% has previously been applied when creating a FI [20]. Since the GBD can be applied to different ages, we took the maximum prevalence from 5-year age groups between 25 and ≥95 years. Causes were excluded if this maximum estimated prevalence was <1%.
- Redundancy: The GBD 2017 contains different sections (i.e., ‘causes’, ‘risk factors’ and ‘impairments’) as well as a hierarchical categorisation of items. This means that many of the items are already included within other items. Which ones to include is largely subjective. In general, the more common item was considered more comprehensive and was chosen for inclusion. However, for six items (‘enteric infections’; ‘cardiovascular diseases’; ‘diabetes and kidney diseases’; ‘sense organ diseases’; ‘musculoskeletal disorders’ and ‘unintentional injuries’) the sub-groups were considered more appropriate for inclusion based on clinical judgement and comparison with an existing validated index [17]. The highest order (i.e., level 1) of GBD causes (n = 3) were also excluded as these items were considered too broad.
2.2. Face Validity of the GBD-FI
2.3. Construct Validity and Properties of the GBD-FI
2.4. Measuring YLD, YLL and DALY Estimates for the GBD-FI
2.5. Outcome Prediction (Internal Validation)
3. Results
3.1. Development of the GBD-FI
3.2. Face Validity of the GBD-FI
3.3. Construct Validity and Properties of the GBD-FI
3.4. Measuring YLD, YLL and DALY Estimates for the GBD-FI
3.5. Outcome Prediction (Internal Validation)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- O’Donovan, M.; Sezgin, D.; Galluzzo, L.; Laso, Á.R.; Van Der Heyden, J.; Ranhoff, A.H.; Koula, M.; Strandzheva, M.; Ciutan, M.; Carriazo, A.M.; et al. Frailty at Population Level in Europe: A Systematic Review and Meta-analysis. Age Ageing 2018, 47, v1–v12. [Google Scholar] [CrossRef] [Green Version]
- Sezgin, D.; O’Donovan, M.; Cornally, N.; Liew, A.; O’Caoimh, R. Defining frailty for healthcare practice and research: A qualitative systematic review with thematic analysis. Int. J. Nurs. Stud. 2019, 92, 16–26. [Google Scholar] [CrossRef]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.-P.; Morley, J.E.; Ong, P. Frailty: An emerging public health priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Mañas, L.; Féart, C.; Mann, G.; Viña, J.; Chatterji, S.; Chodzko-Zajko, W.; Gonzalez-Colaço Harmand, M.; Bergman, H.; Carcaillon, L.; Nicholson, C.; et al. Searching for an Operational Definition of Frailty: A Delphi Method Based Consensus Statement. The Frailty Operative Definition-Consensus Conference Project. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesari, M.; Gambassi, G.; Abellan van Kan, G.; Vellas, B. The frailty phenotype and the frailty index: Different instruments for different purposes. Age Ageing 2013, 43, 10–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin. Geriatr. Med. 2011, 27, 17–26. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Kojima, G.; Iliffe, S.; Morris, R.W.; Taniguchi, Y.; Kendrick, D.; Skelton, D.A.; Masud, T.; Bowling, A. Frailty predicts trajectories of quality of life over time among British community-dwelling older people. Qual. Life Res. 2016, 25, 1743–1750. [Google Scholar] [CrossRef] [Green Version]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Galluzzo, L.; Rodríguez-Laso, Á.; Van Der Heyden, J.; Hylen Ranhoff, A.; Lamprini-Koula, M.; Ciutan, M.; López Samaniego, L.; Carcaillon-Bentata, L.; Kennelly, S.; et al. Prevalence of frailty at population level in European ADVANTAGE Joint Action Member States: A systematic review and meta-analysis. Ann. Ist. Super. Sanità 2018, 54, 226–238. [Google Scholar] [PubMed]
- Biritwum, R.; Minicuci, N.; Yawson, A.; Theou, O.; Mensah, G.; Naidoo, N.; Wu, F.; Guo, Y.; Zheng, Y.; Jiang, Y. Prevalence of and factors associated with frailty and disability in older adults from China, Ghana, India, Mexico, Russia and South Africa. Maturitas 2016, 91, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, J.J.L.; Prina, A.M.; Acosta, D.; Guerra, M.; Huang, Y.; Jacob, K.; Jimenez-Velasquez, I.Z.; Salas, A.; Sosa, A.L.; Williams, J.D. The prevalence and correlates of frailty in urban and rural populations in Latin America, China, and India: A 10/66 population-based survey. J. Am. Med. Dir. Assoc. 2018, 19, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Theou, O.; Brothers, T.D.; Rockwood, M.R.; Haardt, D.; Mitnitski, A.; Rockwood, K. Exploring the relationship between national economic indicators and relative fitness and frailty in middle-aged and older Europeans. Age Ageing 2013, 42, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Clegg, A.; Bates, C.; Young, J.; Ryan, R.; Nichols, L.; Ann Teale, E.; Mohammed, M.A.; Parry, J.; Marshall, T. Development and validation of an electronic frailty index using routine primary care electronic health record data. Age Ageing 2016, 45, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Schneeweiss, S.; Glynn, R.J.; Lipsitz, L.A.; Rockwood, K.; Avorn, J. Measuring frailty in Medicare data: Development and validation of a claims-based frailty index. J. Gerontol. A 2018, 73, 980–987. [Google Scholar] [CrossRef]
- Williams, D.M.; Jylhava, J.; Pedersen, N.L.; Hagg, S. A frailty index for UK Biobank participants. J. Gerontol. A 2019, 74, 582–587. [Google Scholar] [CrossRef] [Green Version]
- Franconi, I.; Theou, O.; Wallace, L.; Malagoli, A.; Mussini, C.; Rockwood, K.; Guaraldi, G. Construct validation of a Frailty Index, an HIV Index and a Protective Index from a clinical HIV database. PLoS ONE 2018, 13, e0201394. [Google Scholar] [CrossRef]
- Jones, D.M.; Song, X.; Rockwood, K. Operationalizing a frailty index from a standardized comprehensive geriatric assessment. J. Am. Geriatr. Soc. 2004, 52, 1929–1933. [Google Scholar] [CrossRef] [PubMed]
- Guerard, E.J.; Deal, A.M.; Chang, Y.; Williams, G.R.; Nyrop, K.A.; Pergolotti, M.; Muss, H.B.; Sanoff, H.K.; Lund, J.L. Frailty index developed from a cancer-specific geriatric assessment and the association with mortality among older adults with cancer. J. Natl. Compr. Cancer Netw. 2017, 15, 894–902. [Google Scholar] [CrossRef] [PubMed]
- IHME. History. Available online: http://www.healthdata.org/about/history (accessed on 25 February 2020).
- Ahmad Kiadaliri, A. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- IHME. GHDx: GBD Results Tool. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 23 January 2019).
- Chan, Y. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Chen, X.; Mao, G.; Leng, S.X. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433. [Google Scholar]
- Hubbard, R.E.; Lang, I.A.; Llewellyn, D.J.; Rockwood, K. Frailty, body mass index, and abdominal obesity in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Winterstein, A.G.; Fillingim, R.B.; Wei, Y.-J. Body weight, frailty, and chronic pain in older adults: A cross-sectional study. BMC Geriatr. 2019, 19, 143. [Google Scholar] [CrossRef] [Green Version]
- Rietman, M.L.; Van Oostrom, S.; Picavet, H.; Dollé, M.; Van Steeg, H.; Verschuren, W.; Spijkerman, A. The association between BMI and different frailty domains: A U-shaped curve? J. Nutr. Health Aging 2018, 22, 8–15. [Google Scholar] [CrossRef]
- De Vries, N.M.; Staal, J.B.; Olde Rikkert, M.G.; Nijhuis-van der Sanden, M.W. Evaluative frailty index for physical activity (EFIP): A reliable and valid instrument to measure changes in level of frailty. Phys. Ther. 2013, 93, 551–561. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.; Nyunt, M.S.Z.; Feng, L.; Yap, K.B.; Ng, T.P. Frailty predicts new and persistent depressive symptoms among community-dwelling older adults: Findings from Singapore longitudinal aging study. J. Am. Med. Dir. Assoc. 2014, 15, 76.e7–76.e12. [Google Scholar] [CrossRef] [PubMed]
- Theou, O.; Brothers, T.D.; Mitnitski, A.; Rockwood, K. Operationalization of frailty using eight commonly used scales and comparison of their ability to predict all-cause mortality. J. Am. Geriatr. Soc. 2013, 61, 1537–1551. [Google Scholar] [CrossRef] [PubMed]
- Kulminski, A.; Yashin, A.; Arbeev, K.; Akushevich, I.; Ukraintseva, S.; Land, K.; Manton, K. Cumulative index of health disorders as an indicator of aging-associated processes in the elderly: Results from analyses of the National Long Term Care Survey. Mech. Ageing Dev. 2007, 128, 250–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramaniam, S.; Aalberg, J.J.; Soriano, R.P.; Divino, C.M. New 5-factor modified frailty index using American College of Surgeons NSQIP data. J. Am. Coll. Surg. 2018, 226, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.-C.; Chen, L.-K.; Hsiao, F.-Y. Predicting mortality and hospitalization of older adults by the multimorbidity frailty index. PLoS ONE 2017, 12, e0187825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlett, S.E.; Rockwood, M.R.; Mitnitski, A.; Rockwood, K. Standard laboratory tests to identify older adults at increased risk of death. BMC Med. 2014, 12, 171. [Google Scholar] [CrossRef] [Green Version]
- IHME. Global Burden of Disease Study 2017 (GBD 2017) Population Estimates 1950–2017. Available online: http://ghdx.healthdata.org/record/ihme-data/gbd-2017-population-estimates-1950-2017 (accessed on 7 May 2020).
- Murray, C.J.L.; Lopez, A.D.; World Health Organization. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary; Harvard University Press: Boston, MA, USA, 1996. [Google Scholar]
- Mathers, C.D.; Vos, T.; Lopez, A.D.; Salomon, J.A.; Ezzati, M. National Burden of Disease Studies: A Practical Guide, 2nd ed.; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Fullman, N.; Yearwood, J.; Abay, S.M.; Abbafati, C.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; Abebe, Z.; Abebo, T.A.; Aboyans, V. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018, 391, 2236–2271. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, J. Modelling and prediction of global non-communicable diseases. BMC Public Health 2020, 20, 1–13. [Google Scholar] [CrossRef]
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [Green Version]
- Goggins, W.B.; Woo, J.; Sham, A.; Ho, S.C. Frailty index as a measure of biological age in a Chinese population. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1046–1051. [Google Scholar] [CrossRef] [Green Version]
- Hoover, M.; Rotermann, M.; Sanmartin, C.; Bernier, J. Validation of an index to estimate the prevalence of frailty among community-dwelling seniors. Health Rep. 2013, 24, 10–17. [Google Scholar] [PubMed]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Lucchesi, L.R.; Bisignano, C.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Henry, N.J.; Krohn, K.J.; Liu, Z.; et al. The global burden of falls: Global, regional and national estimates of morbidity and mortality from the Global Burden of Disease Study 2017. Inj. Prev. 2020. Available online: https://injuryprevention.bmj.com/content/early/2020/01/14/injuryprev-2019-043286 (accessed on 8 July 2020). [CrossRef] [PubMed] [Green Version]
- Franse, C.B.; Rietjens, J.A.; Burdorf, A.; van Grieken, A.; Korfage, I.J.; Van Der Heide, A.; Raso, F.M.; Van Beeck, E.; Raat, H. A prospective study on the variation in falling and fall risk among community-dwelling older citizens in 12 European countries. BMJ Open 2017, 7, e015827. [Google Scholar] [CrossRef] [Green Version]
- Theou, O.; Rockwood, M.R.; Mitnitski, A.; Rockwood, K. Disability and co-morbidity in relation to frailty: How much do they overlap? Arch. Gerontol. Geriatr. 2012, 55, e1–e8. [Google Scholar] [CrossRef]
- Ritt, M.; Ritt, J.I.; Sieber, C.C.; Gassmann, K.-G. Comparing the predictive accuracy of frailty, comorbidity, and disability for mortality: A 1-year follow-up in patients hospitalized in geriatric wards. Clin. Interv. Aging 2017, 12, 293. [Google Scholar] [CrossRef] [Green Version]
- Hogan, D.B.; Ebly, E.M.; Fung, T.S. Disease, Disability, and Age in Cognitively Intact Seniors: Results From the Canadian Study of Health and Aging. J. Gerontol. A 1999, 54, M77–M82. [Google Scholar] [CrossRef] [Green Version]
- O’Donovan, M.; Sezgin, D.; Liew, A.; O’Caoimh, R. 348 Developing a Frailty Index: Does the Composition of Functional and Disease or Risk Items Influence Frailty Estimates? Age Ageing 2019, 48, iii1–iii16. [Google Scholar] [CrossRef] [Green Version]
- Boeckxstaens, P.; Vaes, B.; Legrand, D.; Dalleur, O.; De Sutter, A.; Degryse, J.-M. The relationship of multimorbidity with disability and frailty in the oldest patients: A cross-sectional analysis of three measures of multimorbidity in the BELFRAIL cohort. Eur. J. Gen. Pract. 2015, 21, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Akhtar, A.J. Acute diarrhea in frail elderly nursing home patients. J. Am. Med. Dir. Assoc. 2003, 4, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Troeger, C.; Forouzanfar, M.; Rao, P.C.; Khalil, I.; Brown, A.; Reiner, R.C., Jr.; Fullman, N.; Thompson, R.L.; Abajobir, A.; Ahmed, M. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 909–948. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, C.; Ioannidis, G.; Rockwood, K.; Thabane, L.; Adachi, J.; Kirkland, S.; Pickard, L.; Papaioannou, A. A Frailty Index predicts 10-year fracture risk in adults age 25 years and older: Results from the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos. Int. 2014, 25, 2825–2832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walston, J.D.; Bandeen-Roche, K. Frailty: A tale of two concepts. BMC Med. 2015, 13, 185. [Google Scholar] [CrossRef] [PubMed]
- Liotta, G.; Ussai, S.; Illario, M.; O’Caoimh, R.; Cano, A.; Holland, C.; Roller-Wirnsberger, R.; Capanna, A.; Grecuccio, C.; Ferraro, M. Frailty as the Future Core Business of Public Health: Report of the Activities of the A3 Action Group of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA). Int. J. Environ. Res. Public Health 2018, 15, 2843. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GBD-FI Items (n = 36) | GBD Grouping | GBD Level 5 | All | Female | Male |
|---|---|---|---|---|---|
| Diarrheal diseases (from enteric infections) | Communicable | 3 | 1.8% | 1.9% | 1.8% |
| Protein-energy malnutrition | Nutritional | 3 | 1.2% | 1.1% | 1.3% |
| Neoplasms | Non-communicable | 2 | 6.3% | 5.1% | 7.8% |
| Ischemic heart disease | Non-communicable | 3 | 12.3% | 10.9% | 14.0% |
| Stroke | Non-communicable | 3 | 8.4% | 8.3% | 8.5% |
| Non-rheumatic valvular heart disease | Non-communicable | 3 | 3.6% | 3.6% | 3.5% |
| Cardiomyopathy and myocarditis | Non-communicable | 3 | 0.6% | 0.6% | 0.6% |
| Atrial fibrillation and flutter | Non-communicable | 3 | 5.1% | 4.6% | 5.7% |
| Peripheral artery disease | Non-communicable | 3 | 12.0% | 12.2% | 11.7% |
| Other cardiovascular and circulatory diseases 1 | Non-communicable | 3 | 5.0% | 4.3% | 5.9% |
| Chronic respiratory diseases | Non-communicable | 3 | 26.1% | 25.7% | 26.5% |
| Peptic ulcer disease | Non-communicable | 3 | 0.7% | 0.8% | 0.7% |
| Gallbladder and biliary diseases | Non-communicable | 3 | 1.1% | 1.2% | 1.0% |
| Alzheimer’s disease and other dementias | Non-communicable | 3 | 8.6% | 9.7% | 7.3% |
| Parkinson’s disease | Non-communicable | 3 | 1.2% | 1.1% | 1.4% |
| Major depressive disorder | Non-communicable | 3 | 3.7% | 4.4% | 2.9% |
| Diabetes mellitus | Non-communicable | 3 | 22.0% | 21.3% | 22.8% |
| Chronic kidney disease | Non-communicable | 3 | 40.4% | 45.7% | 33.7% |
| Skin and subcutaneous diseases | Non-communicable | 3 | 52.3% | 52.7% | 51.9% |
| Other sense organ diseases 2 | Non-communicable | 3 | 6.0% | 6.5% | 5.4% |
| Rheumatoid arthritis | Non-communicable | 3 | 1.0% | 1.3% | 0.6% |
| Osteoarthritis | Non-communicable | 3 | 22.4% | 25.4% | 18.4% |
| Low back pain | Non-communicable | 3 | 19.1% | 20.7% | 17.0% |
| Gout | Non-communicable | 3 | 2.8% | 1.7% | 4.2% |
| Urinary system diseases 3 | Non-communicable | 3 | 5.6% | 0.2% | 12.5% |
| Genital prolapse | Non-communicable | 4 | 4.5% | 8.0% | 0% |
| Endocrine, metabolic, blood, and immune disorders 4 | Non-communicable | 3 | 2.4% | 2.4% | 2.4% |
| Edentulism and severe tooth loss | Non-communicable | 4 | 23.5% | 27.1% | 18.9% |
| Falls (injurious) | Injury | 3 | 21.8% | 22.8% | 20.5% |
| Low physical activity | Risk factor | 3 | 1.0% | 0.9% | 1.0% |
| High LDL cholesterol | Risk factor | 3 | 35.0% | 38.4% | 30.7% |
| High systolic blood pressure | Risk factor | 3 | 32.2% | 34.2% | 29.7% |
| Low bone mineral density | Risk factor | 3 | 22.7% | 27.1% | 16.9% |
| Hearing loss | Impairment | 1 | 74.8% | 74.0% | 75.8% |
| Heart failure | Impairment | 1 | 8.8% | 9.0% | 8.6% |
| Blindness and vision impairment | Impairment | 1 | 63.6% | 65.0% | 61.9% |
| Mean GBD-FI score | Mixed | Mixed | 0.155 | 0.161 | 0.148 |
| GBD-FI Items (n = 36) | Asia | Americas | Africa | Europe | China | Hungary | UK |
|---|---|---|---|---|---|---|---|
| Diarrheal diseases (from enteric infections) | 2.0% | 2.3% | 2.7% | 0.9% | 1.1% | 2.7% | 1.5% |
| Protein-energy malnutrition | 1.3% | 1.4% | 1.0% | 0.8% | 1.9% | 0.1% | 0.6% |
| Neoplasms | 4.0% | 12.9% | 2.1% | 8.0% | 4.1% | 6.0% | 12.7% |
| Ischemic heart disease | 10.7% | 12.5% | 13.3% | 15.8% | 9.2% | 21.1% | 15.7% |
| Stroke | 8.5% | 8.2% | 6.8% | 8.5% | 11.3% | 11.4% | 6.4% |
| Non-rheumatic valvular heart disease | 2.2% | 5.7% | 1.7% | 5.9% | 1.3% | 6.1% | 6.7% |
| Cardiomyopathy and myocarditis | 0.3% | 0.8% | 0.7% | 1.0% | 0.1% | 1.6% | 0.4% |
| Atrial fibrillation and flutter | 3.9% | 8.0% | 3.4% | 6.3% | 4.2% | 6.2% | 7.7% |
| Peripheral artery disease | 10.7% | 15.2% | 11.9% | 12.6% | 11.0% | 12.4% | 12.3% |
| Other cardiovascular and circulatory diseases 1 | 3.5% | 5.5% | 5.9% | 8.1% | 1.6% | 9.3% | 8.3% |
| Chronic respiratory diseases | 25.6% | 27.1% | 21.8% | 27.5% | 24.3% | 38.2% | 33.4% |
| Peptic ulcer disease | 0.7% | 0.7% | 1.0% | 0.7% | 0.6% | 1.2% | 0.4% |
| Gallbladder and biliary diseases | 0.9% | 1.2% | 0.5% | 1.6% | 1.2% | 2.2% | 1.2% |
| Alzheimer’s disease and other dementias | 8.3% | 8.1% | 7.2% | 10.2% | 9.0% | 10.1% | 8.9% |
| Parkinson’s disease | 1.2% | 1.2% | 1.0% | 1.3% | 1.4% | 1.4% | 1.2% |
| Major depressive disorder | 4.0% | 2.5% | 5.5% | 3.6% | 4.2% | 4.4% | 3.0% |
| Diabetes mellitus | 18.8% | 24.8% | 27.5% | 26.1% | 13.4% | 28.8% | 27.1% |
| Chronic kidney disease | 35.9% | 47.8% | 52.4% | 43.0% | 26.4% | 43.3% | 34.9% |
| Skin and subcutaneous diseases | 50.7% | 51.3% | 54.0% | 56.7% | 51.1% | 53.4% | 59.8% |
| Other sense organ diseases 2 | 6.0% | 6.1% | 5.8% | 6.2% | 6.0% | 6.3% | 6.1% |
| Rheumatoid arthritis | 0.9% | 1.2% | 0.8% | 1.1% | 0.8% | 0.8% | 1.7% |
| Osteoarthritis | 19.9% | 29.6% | 19.1% | 24.0% | 15.2% | 20.1% | 27.4% |
| Low back pain | 15.4% | 21.2% | 22.6% | 25.8% | 9.8% | 31.4% | 24.3% |
| Gout | 2.5% | 3.3% | 2.7% | 3.0% | 2.1% | 2.1% | 4.2% |
| Urinary system diseases 3 | 5.1% | 5.1% | 9.7% | 6.2% | 4.7% | 5.4% | 5.1% |
| Genital prolapse | 4.0% | 4.7% | 8.6% | 4.5% | 3.2% | 4.4% | 5.9% |
| Endocrine, metabolic, blood, and immune disorders 4 | 2.2% | 3.3% | 2.3% | 2.4% | 1.6% | 2.1% | 2.5% |
| Edentulism and severe tooth loss | 19.9% | 30.6% | 16.2% | 29.0% | 20.1% | 31.1% | 25.6% |
| Falls (injurious) | 14.3% | 25.3% | 11.7% | 39.9% | 10.3% | 81.0% | 29.7% |
| Low physical activity | 0.9% | 1.0% | 0.9% | 1.1% | 0.8% | 0.8% | 1.1% |
| High LDL cholesterol | 32.6% | 35.9% | 26.9% | 42.1% | 33.3% | 39.0% | 42.2% |
| High systolic blood pressure | 31.7% | 27.3% | 37.1% | 35.8% | 31.5% | 58.6% | 28.2% |
| Low bone mineral density | 25.2% | 19.5% | 25.9% | 18.0% | 26.3% | 18.0% | 17.0% |
| Hearing loss | 75.9% | 73.8% | 74.7% | 72.9% | 76.4% | 75.4% | 68.9% |
| Heart failure | 8.3% | 9.9% | 8.1% | 9.5% | 8.1% | 13.3% | 8.0% |
| Blindness and vision impairment | 77.1% | 44.4% | 85.9% | 39.9% | 71.3% | 51.9% | 22.2% |
| Mean GBD-FI score | 0.149 | 0.161 | 0.161 | 0.167 | 0.139 | 0.195 | 0.156 |
| Country-Level One Year Mortality from Non-Communicable Diseases in 2017 per 100,000 | Age | Sex | SDI | HAQ | SDI HAQ | SDI HAQ Age | SDI HAQ Sex | SDI HAQ Age Sex | |
|---|---|---|---|---|---|---|---|---|---|
| Model adj r2 | - | 14.1% | 6.8% | 5.6% | 11.1% | 16.9% | 18.5% | 24.0% | 27.0% |
| Model + GBD-FI adj r2 | 14.3% | 30.7% | 17.1% | 26.3% | 32.4% | 35.2% | 35.4% | 38.6% | 39.6% |
| Improvement in adj r2 | +14.3% | +16.6% | +10.3% | +20.7% | +21.3% | +18.3% | +16.9% | +14.6% | +12.6% |
| p-value for r2 difference | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Donovan, M.; Sezgin, D.; Kabir, Z.; Liew, A.; O’Caoimh, R. Assessing Global Frailty Scores: Development of a Global Burden of Disease-Frailty Index (GBD-FI). Int. J. Environ. Res. Public Health 2020, 17, 5695. https://doi.org/10.3390/ijerph17165695
O’Donovan M, Sezgin D, Kabir Z, Liew A, O’Caoimh R. Assessing Global Frailty Scores: Development of a Global Burden of Disease-Frailty Index (GBD-FI). International Journal of Environmental Research and Public Health. 2020; 17(16):5695. https://doi.org/10.3390/ijerph17165695
Chicago/Turabian StyleO’Donovan, Mark, Duygu Sezgin, Zubair Kabir, Aaron Liew, and Rónán O’Caoimh. 2020. "Assessing Global Frailty Scores: Development of a Global Burden of Disease-Frailty Index (GBD-FI)" International Journal of Environmental Research and Public Health 17, no. 16: 5695. https://doi.org/10.3390/ijerph17165695
APA StyleO’Donovan, M., Sezgin, D., Kabir, Z., Liew, A., & O’Caoimh, R. (2020). Assessing Global Frailty Scores: Development of a Global Burden of Disease-Frailty Index (GBD-FI). International Journal of Environmental Research and Public Health, 17(16), 5695. https://doi.org/10.3390/ijerph17165695