Sepsis-Associated Brain Dysfunction: A Review of Current Literature




Abstract
:1. Introduction
2. Materials and Methods
Epidemiology
3. Results
Clinical Presentation
4. Discussion
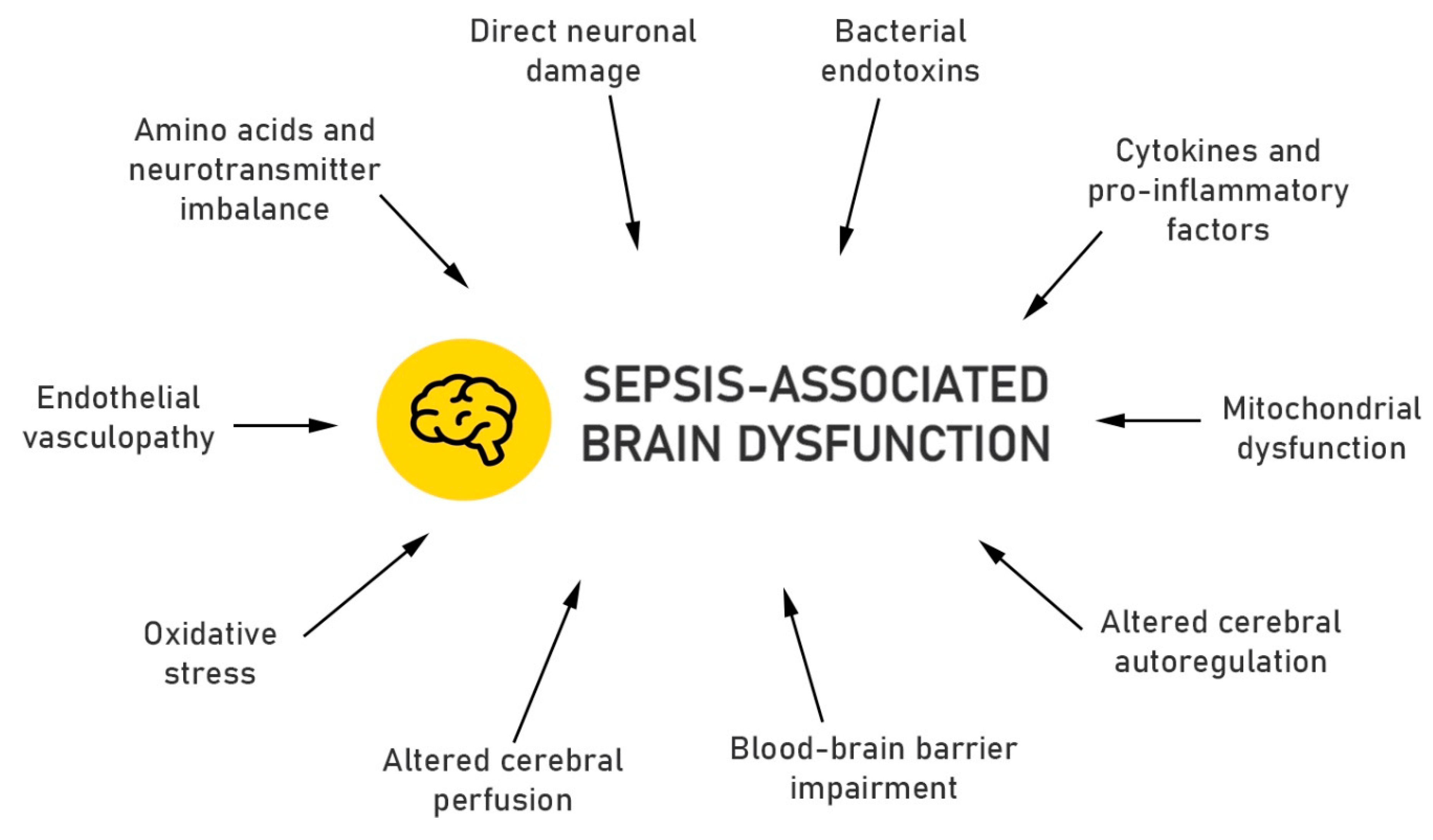
4.1. Pathogenesis/ Pathophysiology
4.2. Diagnosis
4.3. Management
4.4. Prevention
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Salluh, J.I.; Soares, M.; Teles, J.M.; Ceraso, D.; Raimondi, N.; Nava, V.S.; Blasquez, P.; Ugarte, S.; Ibanez-Guzman, C.; Centeno, J.V.; et al. Delirium epidemiology in critical care (DECCA): An international study. Crit. Care 2010, 14, R210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gofton, T.E.; Young, G.B. Sepsis-associated encephalopathy. Nat. Rev. Neurol. 2012, 8, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Bolton, C.F.; Young, G.B.; Zochodne, D.W. The neurological complications of sepsis. Ann. Neurol. 1993, 33, 94–100. [Google Scholar] [CrossRef]
- Bolton, C.F.; Young, G.B. Managing the nervous system effects of sepsis. Chest 2007, 131, 1273–1274. [Google Scholar] [CrossRef]
- Young, G.B.; Bolton, C.F.; Austin, T.W.; Archibald, Y.M.; Gonder, J.; Wells, G.A. The encephalopathy associated with septic illness. Clin. Investig. Med. 1990, 13, 297–304. [Google Scholar]
- Zhang, L.N.; Wang, X.T.; Ai, Y.H.; Guo, Q.L.; Huang, L.; Liu, Z.Y.; Yao, B. Epidemiological features and risk factors of sepsis-associated encephalopathy in intensive care unit patients: 2008–2011. Chin. Med. J. 2012, 125, 828–831. [Google Scholar]
- Eidelman, L.A.; Putterman, D.; Putterman, C.; Sprung, C.L. The spectrum of septic encephalopathy: Definitions, etiologies, and mortalities. JAMA 1996, 75, 470–473. [Google Scholar] [CrossRef]
- Mikkelsen, M.E.; Christie, J.D.; Lanken, P.N.; Biester, R.C.; Thompson, B.T.; Bellamy, S.L.; Localio, A.R.; Demissie, E.; Hopkins, R.O.; Angus, D.C. The adult respiratory distress syndrome cognitive outcomes study: Long-term neuropsychological function in survivors of acute lung injury. Am. J. Respir. Crit. Care Med. 2012, 185, 1307–1315. [Google Scholar] [CrossRef] [Green Version]
- Semmler, A.; Frisch, C.; Debeir, T.; Ramanathan, M.; Okulla, T.; Klockgether, T.; Heneka, M.T. Long-term cognitive impairment, neuronal loss and reduced cortical cholinergic innervation after recovery from sepsis in a rodent model. Exp. Neurol. 2007, 204, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Soriano, F.G. Quality of life: Late sequela in sepsis. Crit. Care Med. 2005, 33, 262–263. [Google Scholar] [CrossRef] [PubMed]
- Lazosky, A.; Young, G.B.; Zirul, S.; Phillips, R. Quality of life after septic illness. J. Crit. Care 2010, 25, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Ai, Y.H.; Gong, H.; Wu, L.; Ai, M.L.; Deng, S.Y.; Huang, L.; Peng, Q.Y.; Zhang, L.N. Characterization of Sepsis and Sepsis-Associated Encephalopathy. J. Intensive Care Med. 2019, 34, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Wintermann, G.B.; Brunkhorst, F.M.; Petrowski, K.; Strauss, B.; Oehmichen, F.; Pohl, M.; Rosendahl, J. Stress disorders following prolonged critical illness in survivors of severe sepsis. Crit. Care Med. 2015, 43, 1213–1222. [Google Scholar] [CrossRef]
- Mostel, Z.; Perl, A.; Marck, M.; Mehdi, S.F.; Lowell, B.; Bathija, S.; Santosh, R.; Pavlov, V.A.; Chavan, S.S.; Roth, J. Post-sepsis syndrome—An evolving entity that afflicts survivors of sepsis. Mol. Med. 2019, 26, 6. [Google Scholar] [CrossRef] [Green Version]
- Lund-Sorensen, H.; Benros, M.E.; Madsen, T.; Sorensen, H.J.; Eaton, W.W.; Postolache, T.T.; Nordentoft, M.; Erlangsen, A. A Nationwide Cohort Study of the Association between Hospitalization with Infection and Risk of Death by Suicide. JAMA Psychiatry 2016, 73, 912–919. [Google Scholar] [CrossRef]
- Annane, D.; Sharshar, T. Cognitive decline after Sepsis. Lancet Respir. Med. 2015, 3, 61–69. [Google Scholar] [CrossRef]
- Sharshar, T.; Annane, D.; de la Grandmaison, G.L.; Brouland, J.P.; Hopkinson, N.S.; Françoise, G. The Neuropathology of Septic Shock. Brain Pathol. 2004, 14, 21–33. [Google Scholar] [CrossRef]
- Jackson, A.C.; Gilbert, J.J.; Young, G.B.; Bolton, C.F. The encephalopathy of sepsis. Can. J. Neurol. Sci. 1985, 12, 303–307. [Google Scholar] [CrossRef] [Green Version]
- Sharshar, T.; Polito, A.; Checinski, A.; Stevens, R.D. Septic-associated encephalopathy-everything starts at a microlevel. Crit. Care 2010, 14, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, J.X.; Young, G.B. Progress in clinical neurosciences: Sepsis-associated encephalopathy: Evolving concepts. Can. J. Neurol. Sci. 2003, 30, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonneville, R.; Derese, I.; Marques, M.B.; Langouche, L.; Derde, S.; Chatre, L.; Chrétien, F.; Annane, D.; Sharshar, T.; Van den Berghe, G.; et al. Neuropathological Correlates of Hyperglycemia During Prolonged Polymicrobial Sepsis in Mice. Shock 2015, 44, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Sharshar, T.; Porcher, R.; Siami, S.; Rohaut, B.; Bailly-Salin, J.; Hopkinson, N.S.; Clair, B.; Guidoux, C.; Iacobone, E.; Sonneville, R.; et al. Brainstem Responses Can Predict Death and Delirium in Sedated Patients in Intensive Care Unit. Crit. Care Med. 2011, 39, 1960–1967. [Google Scholar] [CrossRef]
- Stare, J.; Siami, S.; Trudel, E.; Prager-Khoutorsky, M.; Sharshar, T.; Bourque, C.W. Effects of peritoneal sepsis on rat central osmoregulatory neurons mediating thirst and vasopressin release. J. Neurosci. 2015, 35, 12188–12197. [Google Scholar] [CrossRef]
- Muscatell, K.A.; Dedovic, K.; Slavich, G.M.; Jarcho, M.R.; Breen, E.C.; Bower, J.E.; Irwin, M.R.; Eisenberger, N.I. Greater amygdala activity and dorsomedial prefrontal-amygdala coupling are associated with enhanced inflammatory responses to stress. Brain Behav. Immun. 2015, 43, 46–53. [Google Scholar] [CrossRef] [Green Version]
- van Gool, W.A.; van de Beek, D.; Eikelenboom, P. Systemic infection and delirium: When cytokines and acetylcholine collide. Lancet 2010, 375, 773–775. [Google Scholar] [CrossRef]
- Jacob, A.; Brorson, J.R.; Alexander, J.J. Septic encephalopathy: Inflammation in man and mouse. Neurochem. Int. 2011, 58, 472–476. [Google Scholar] [CrossRef]
- Berg, R.M.; Moller, K.; Bailey, D.M. Neuro-oxidative-nitrosative stress in sepsis. J. Cereb. Blood Flow Metab. 2011, 31, 1532–1544. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, L.C. Mitochondrial dysfunction during sepsis. Endocr. Metab. Immune Disord. Drug Targets 2010, 10, 214–223. [Google Scholar] [CrossRef]
- Brealey, D.; Karyampudi, S.; Jacques, T.S.; Novelli, M.; Stidwill, R.; Taylor, V.; Smolenski, R.S.; Singer, M. Mitochondrial Dysfunction in a Long-Term Rodent Model of Sepsis and Organ Failure. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 286, 491–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cepinskas, G.; Wilson, J.X. Inflammatory response in microvascular endothelium in sepsis: Role of oxidants. J. Clin. Biochem. Nutr. 2008, 42, 175–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkhart, C.S.; Siegemund, M.; Steiner, L.A. Cerebral perfusion in sepsis. Crit. Care 2010, 14, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szatmari, S.; Vegh, T.; Csomos, A.; Hallay, J.; Takacs, I.; Molnar, C.; Fülesdi, B. Impaired Cerebrovascular Reactivity in Sepsis-Associated Encephalopathy Studied by Acetazolamide Test. Crit. Care 2010, 14, R50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taccone, F.S.; Castanares-Zapatero, D.; Peres-Bota, D.; Vincent, J.-L.; Berre, J.; Melot, C. Cerebral Autoregulation Is Influenced by Carbon Dioxide Levels in Patients With Septic Shock. Neurocrit. Care 2010, 12, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.M.; Taudorf, S.; Bailey, D.M.; Lundby, C.; Larsen, F.S.; Pedersen, B.K.; Møller, K. Cerebral net exchange of large neutral amino acids after lipopolysaccharide infusion in healthy humans. Crit. Care 2010, 14, R16. [Google Scholar] [CrossRef] [Green Version]
- Davies, D.C. Blood-brain Barrier Breakdown in Septic Encephalopathy and Brain Tumours. J. Anat. 2002, 200, 639–646. [Google Scholar] [CrossRef]
- Sprung, C.L.; Cerra, F.B.; Freund, H.R.; Schein, R.M.; Konstantinides, F.N.; Marcial, E.H.; Pena, M. Amino acid alterations and encephalopathy in the sepsis syndrome. Crit. Care Med 1991, 19, 753–757. [Google Scholar] [CrossRef]
- van Eijk, M.M.; Roes, K.C.; Honing, M.L.; Kuiper, M.A.; Karakus, A.; van der Jagt, M.; Spronk, P.E.; van Gool, W.A.; van der Mast, R.C.; Kesecioglu, J.; et al. Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: A multicentre, double-blind, placebo-controlled randomized trial. Lancet 2010, 376, 1829–1837. [Google Scholar] [CrossRef] [Green Version]
- Girard, T.; Exline, M.C.; Carson, S.S.; Hough, C.L.; Rock, P. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness. N. Engl. J. Med. 2018, 379, 2506–2516. [Google Scholar] [CrossRef]
- Reade, M.C.; Eastwood, G.M.; Peck, L.; Bellomo, R.; Baldwin, I. Routine use of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) by bedside nurses may underdiagnose delirium. Crit. Care Resusc. 2011, 13, 217–224. [Google Scholar]
- van Eijk, M.M.; van den Boogaard, M.; van Marum, R.J.; Benner, P.; Eikelenboom, P.; Honing, M.L.; van der Hoven, B.; Horn, J.; Izaks, G.J.; Kalf, A.; et al. Routine use of the confusion assessment method for the intensive care unit: A multicenter study. Am. J. Respir. Crit. Care Med. 2011, 184, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Young, G.B.; Bolton, C.F.; Archibald, Y.M.; Austin, T.W.; Wells, G.A. The electroencephalogram in sepsis-associated encephalopathy. J. Clin. Neurophysiol. 1992, 9, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, P.W. The EEG in metabolic encephalopathy and coma. J. Clin. Neurophysiol. 2004, 21, 307–318. [Google Scholar] [PubMed]
- Azabou, E.; Magalhaes, E.; Braconnier, A.; Yahiaoui, L.; Moneger, G.; Heming, N.; Annane, D.; Mantz, J.; Chrétien, F.; Durand, M.-C.; et al. Early standard electroencephalogram abnormalities predict mortality in septic intensive care unit patients. PLoS ONE 2015, 10, e0139969. [Google Scholar] [CrossRef] [PubMed]
- Luitse, M.J.; van Asch, C.J.; Klijn, C.J. Deep coma and diffuse white matter abnormalities caused by sepsis-associated encephalopathy. Lancet 2013, 381, 2222. [Google Scholar] [CrossRef]
- Sharshar, T.; Carlier, R.; Bernard, F.; Guidoux, C.; Brouland, J.-P.; Nardi, O.; de la Grandmaison, G.L.; Aboab, J.; Gray, F.; Menon, D.; et al. Brain lesions in septic shock: A magnetic resonance imaging study. Intensive Care Med. 2007, 33, 798–806. [Google Scholar] [CrossRef]
- Ahmed, M.; Sureka, J.; Mathew, V.; Jakkani, R.K.; Abhilash, K.P. Magnetic resonance imaging findings in a fatal case of Salmonella typhi-associated encephalopathy: A case report and literature review. Neurol. India 2011, 59, 270–272. [Google Scholar] [CrossRef]
- Gunther, M.L.; Morandi, A.; Krauskopf, E.; Pandharipande, P.; Girard, T.D.; Jackson, J.C.; Thompson, J.; Shintani, A.K.; Geevarghese, S.; Miller, R.R.; et al. The association between brain volumes, delirium duration, and cognitive outcomes in intensive care unit survivors: The VISIONS cohort magnetic resonance imaging study. Crit. Care Med. 2012, 40, 2022–2032. [Google Scholar] [CrossRef] [Green Version]
- Kulkarni, A.A.; Sharma, V.K. Role of transcranial Doppler in cerebrovascular disease. Neurol. India 2016, 64, 995–1001. [Google Scholar] [CrossRef]
- Pierrakos, C.; Attou, R.; Decorte, L.; Kolyviras, A.; Malinverni, S.; Gottignies, P.; Devriendt, J.; De Bels, D. Transcranial Doppler to assess sepsis-associated encephalopathy in critically ill patients. BMC Anesthesiol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Czempik, P.F.; Gąsiorek, J.; Bąk, A.; Krzych, L.J. Ultrasonic Assessment of Optic Nerve Sheath Diameter in Patients at Risk of Sepsis-Associated Brain Dysfunction: A Preliminary Report. Int. J. Environ. Res. Public Health 2020, 17, 3656. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.N.; Spapen, H.; Su, F.; Schiettecatte, J.; Shi, L.; Hachimi-Idrissi, S.; Huyghens, L. Elevated serum levels of S-100beta protein and neuron-specific enolase are associated with brain injury in patients with severe sepsis and septic shock. Crit. Care Med. 2006, 34, 1967–1974. [Google Scholar] [CrossRef] [PubMed]
- Moss, R.F.; Parmar, N.K.; Tighe, D.; Davies, D.C. Adrenergic agents modify cerebral edema and microvessel ultrastructure in porcine sepsis. Crit. Care Med. 2004, 32, 1916–1921. [Google Scholar] [CrossRef] [PubMed]
- Toklu, H.Z.; Uysal, M.K.; Kabasakal, L.; Sirvanci, S.; Ercan, F.; Kaya, M. The Effects of Riluzole on Neurological, Brain Biochemical, and Histological Changes in Early and Late Term of Sepsis in Rats. J. Surg. Res. 2009, 152, 238–248. [Google Scholar] [CrossRef]
- Andonegui, G.; Zelinski, E.L.; Schubert, C.L.; Knight, D.; Craig, L.A.; Winston, B.W.; Spanswick, S.C.; Petri, B.; Jenne, C.N.; Sutherland, J.C.; et al. Targeting inflammatory monocytes in sepsis-associated encephalopathy and long-term cognitive impairment. JCI Insight 2018, 3, e99364. [Google Scholar] [CrossRef]
- Pfister, D.; Schmidt, B.; Smielewski, P.; Siegemund, M.; Strebel, S.P.; Ruegg, S.; Marsch, S.C.U.; Pargger, H.; Steiner, L.A. Intracranial pressure in patients with sepsis. Acta Neurochir. Suppl. 2008, 102, 71–75. [Google Scholar] [CrossRef]
- Pandharipande, P.P.; Sanders, R.D.; Girard, T.D.; McGrane, S.; Thompson, J.L.; Shintani, A.K.; Herr, D.L.; Maze, M.; Ely, W.E. MENDS investigators Effect of dexmedetomidine versus lorazepam on outcome in patients with sepsis: An a priori-designed analysis of the MENDS randomized controlled trial. Crit. Care 2010, 14, R38. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.-L.; Shehabi, Y.; Walsh, T.S.; Pandharipande, P.P.; Ball, J.A.; Spronk, P.; Longrois, D.; Strøm, T.; Conti, G.; Funk, G.-C. Comfort and Patient-Centred Care without Excessive Sedation: The eCASH Concept. Intensive Care Med. 2016, 42, 962–9671. [Google Scholar] [CrossRef] [Green Version]
- Sonneville, R.; de Montmollin, E.; Poujade, J.; Garrouste-Orgeas, M.; Souweine, B.; Darmon, M.; Mariotte, E.; Argaud, L.; Barbier, F.; Goldgran-Toledano, D.; et al. Potentially modifiable factors contributing to sepsis-associated encephalopathy. Intensive Care Med. 2017, 43, 1075–1084. [Google Scholar] [CrossRef]


{kind=link}
| Acute Problems | Long-Term Problems |
|---|---|
| Fluctuations of Vigilance | Lower health-related quality of life [10,11,12,13,14] |
| Lethargy | Anxiety |
| Delirium | Post-traumatic stress disorder [15]/Post-sepsis syndrome [16] |
| Coma | Depression |
| Polyneuropathy | Suicidal behavior [17] |
| Dementia [18] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czempik, P.F.; Pluta, M.P.; Krzych, Ł.J. Sepsis-Associated Brain Dysfunction: A Review of Current Literature. Int. J. Environ. Res. Public Health 2020, 17, 5852. https://doi.org/10.3390/ijerph17165852
Czempik PF, Pluta MP, Krzych ŁJ. Sepsis-Associated Brain Dysfunction: A Review of Current Literature. International Journal of Environmental Research and Public Health. 2020; 17(16):5852. https://doi.org/10.3390/ijerph17165852
Chicago/Turabian StyleCzempik, Piotr F., Michał P. Pluta, and Łukasz J. Krzych. 2020. "Sepsis-Associated Brain Dysfunction: A Review of Current Literature" International Journal of Environmental Research and Public Health 17, no. 16: 5852. https://doi.org/10.3390/ijerph17165852
APA StyleCzempik, P. F., Pluta, M. P., & Krzych, Ł. J. (2020). Sepsis-Associated Brain Dysfunction: A Review of Current Literature. International Journal of Environmental Research and Public Health, 17(16), 5852. https://doi.org/10.3390/ijerph17165852