Doctors’ Extended Shifts as Risk to Practitioner and Patient: South Africa as a Case Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Origins of Extended Shifts in Medical Practice
3. The Impact of Extended Shifts on Safety
4. Regulating Extended Shifts
5. Barriers to Change
5.1. Shortage of Doctors
5.2. The Hazards of Shift Work
5.3. Concerns about Education
5.4. Doctors’ Preference
6. Case Study: The Safe Working Hours Campaign in South Africa
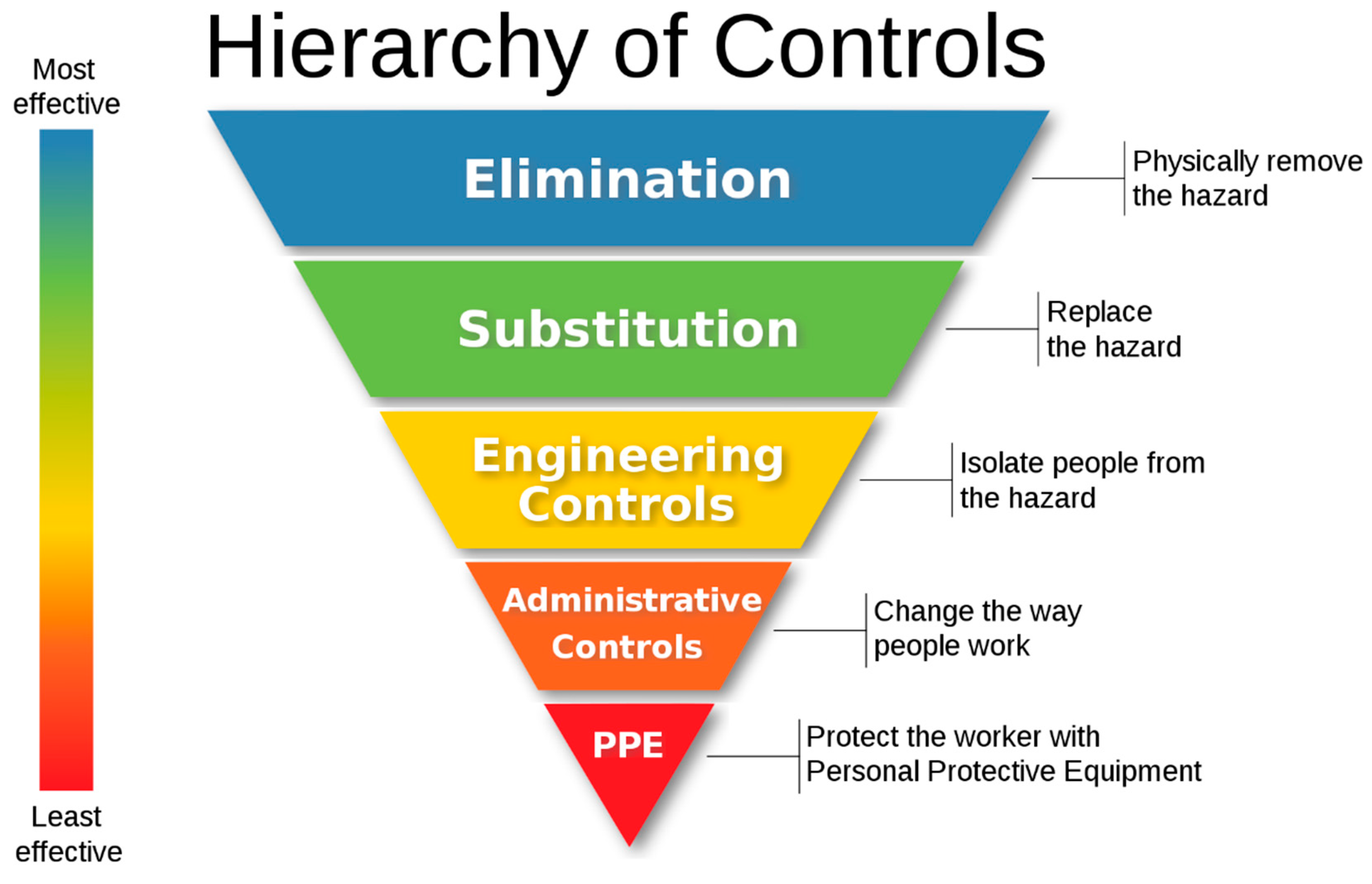
7. Extended Shifts as an Occupational Hazard

{kind=link}
{kind=link}
| Control | Examples as Applied to Extended Shifts |
|---|---|
| Elimination | Instituting a cap on shift durations |
| Substitution | Moving to one of a variety of alternative shift systems, within the safest acceptable parameters: |
| Environmental Measures | Providing rest facilities and ensuring that they are conducive to rest [37] Ensuring adequate light in the working environment in order to promote wakefulness [3] (p. 76) |
| Administrative Measures | Ensuring that employment contracts allow for a change from extended shifts to shorter shifts. (For example, not insisting that overtime can only be worked during certain hours of the day) * Providing schedulers assistance in drafting more complex after-hours schedules [23] Coupling the above changes with interventions to minimize the harm from shifts to patients and practitioners: |
| Personal Protective Measures | Preventing the increased risk posed to patients by those on extended shifts by:
|
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Walker, M.P. A sleep prescription for medicine. Lancet 2018, 391, 2598–2599. [Google Scholar] [CrossRef]
- Lockley, S.W.; Landrigan, C.P.; Barger, L.K.; Czeisler, C.A. When policy meets physiology: The challenge of reducing resident work hours. Clin. Orthop. Relat. Res. 2006, 449, 116–127. [Google Scholar] [CrossRef]
- Surani, S.; Subramanian, S. Sleep & Safety, 1st ed.; Bentham Science Publishers: Sharjah, United Arab Emirates, 2011. [Google Scholar]
- Kisting, S.; Dalvie, A.; Lewis, P. South Africa: Case Study on Working Time Organization and Its Effects in the Health Services Sector; ILO: Geneva, Switzerland, 2016; Available online: www.ilo.org/publns (accessed on 22 July 2020).
- Weaver, M.D.; Landrigan, C.P.; Sullivan, J.P.; O’Brien, C.S.; Qadri, S.; Viyaran, N.; Wang, W.; Vetter, C.; Vetter, C.A.; Barger, L.K. The Association Between Resident Physician Work-Hour Regulations and Physician Safety and Health. Am. J. Med. 2020, 133, e343–e354. [Google Scholar] [CrossRef]
- Philibert, I. Sleep loss and performance in residents and nonphysicians: A meta-analytic examination. Sleep 2005, 28, 1392–1402. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16335329 (accessed on 22 July 2020).
- Australian Medical Association. Managing the Risks of Fatigue in the Medical Workforce 2016. Available online: https://web.archive.org/web/20200810152216/https://ama.com.au/sites/default/files/documents/150717%20-%20AMA%20Safe%20Hours%20Audit%202016.pdf (accessed on 10 August 2020).
- Spirling, L.I.; Daniels, I.R. William Stewart Halsted—Surgeon extraordinaire: A story of ‘drugs, gloves and romance’. J. R. Soc. Promot. Health 2002, 122, 122–124. [Google Scholar] [CrossRef]
- Wallack, M.; Chao, L. Resident work hours. J. Neurosurg 2012, 116, 475–476. [Google Scholar] [CrossRef]
- Cameron, J.L. William Stewart Halsted: Our surgical heritage. Ann. Surg 1997, 225, 445–458. [Google Scholar] [CrossRef]
- Wagstaff, A.S.; Lie, J.A.S. Shift and night work and long working hours—A systematic review of safety implications. Scand. J. Work Environ. Heal 2011, 37, 173–185. [Google Scholar] [CrossRef] [Green Version]
- Gates, M.; Wingert, A.; Featherstone, R.; Samuels, C.; Simon, C.; Dyson, M.P. Impact of fatigue and insufficient sleep on physician and patient outcomes: A systematic review. BMJ Open 2018, 8, e021967. [Google Scholar] [CrossRef] [Green Version]
- Vincent, C. Patient Safety, 2nd ed.; John Wiley & Sons: West Sussex, UK, 2011. [Google Scholar]
- Landrigan, C.P.; Rothschild, J.M.; Cronin, J.W.; Kaushal, R.; Burdick, E.; Katz, J.T.; Lilly, C.M.; Stone, P.H.; Lockley, S.W.; Bates, D.W.; et al. Effect of Reducing Interns’ Work Hours on Serious Medical Errors in Intensive Care Units. N. Engl. J. Med. 2004, 351, 1838–1848. [Google Scholar] [CrossRef] [Green Version]
- British Medical Association. Fatigue and sleep deprivation—The impact of different working patterns on doctors. 2018. Available online: https://web.archive.org/web/20200810152830/https://www.bma.org.uk/media/1074/bma_fatigue-sleep-deprivation-briefing-jan2017.pdf (accessed on 10 August 2020).
- Mak, N.T.; Li, J.; Wiseman, S.M. Resident Physicians are at Increased Risk for Dangerous Driving after Extended-duration Work Shifts: A Systematic Review. Cureus 2019, 11, e4843. [Google Scholar] [CrossRef] [Green Version]
- Barger, L.K.; Cade, B.E.; Ayas, N.T.; Cronin, J.W.; Rosner, B.; Speizer, F.E.; Czeisler, C.A. Extended work shifts and the risk of motor vehicle crashes among interns. N. Engl. J. Med. 2005, 352, 125–134. [Google Scholar] [CrossRef]
- Ayas, N.T.; Barger, L.K.; Cade, B.E.; Hashimoto, D.M.; Rosner, B.; Cronin, J.W.; Speizer, F.E.; Czeisler, C.A. Extended work duration and the risk of self-reported percutaneous injuries in interns. JAMA 2006, 296, 1055–1062. [Google Scholar] [CrossRef] [Green Version]
- Bilimoria, K.Y.; Chung, J.W.; Hedges, L.V.; Dahlke, A.R.; Love, R.; Cohen, M.E.; Hoyt, D.B.; Yang, A.D.; Tarpley, J.L.; Mellinger, J.D.; et al. National cluster-randomized trial of duty-hour flexibility in surgical training. N. Engl. J. Med. 2016, 374, 713–727. [Google Scholar] [CrossRef]
- Birkmeyer, J.D. Surgical resident duty-hour rules—Weighing the new evidence. N. Engl. J. Med. 2016, 374, 783–784. [Google Scholar] [CrossRef]
- World Health Organization. Global strategy on human resources for health: Workforce 2030. 2016. Available online: https://web.archive.org/web/20200810153104/https://apps.who.int/iris/bitstream/handle/10665/250368/9789241511131-eng.pdf;jsessionid=C02BD48BF949E4BBA7AEE9F1434507D3?sequence=1 (accessed on 10 August 2020).
- Goldacre, M.J.; Goldacre, R.; Lambert, T.W. Doctors who considered but did not pursue specific clinical specialties as careers: Questionnaire surveys. J. R. Soc. Med. 2012, 105, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Sun, N.Z.; Maniatis, T. Scheduling in the context of resident duty hour reform. BMC Med. Educ. 2014, 14, S1. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, A.C.; Paterson, J.L.; Ferguson, S.A.; Stanley, D.; Wright, K.P.; Dawson, D. The shift work and health research agenda: Considering changes in gut microbiota as a pathway linking shift work, sleep loss and circadian misalignment, and metabolic disease. Sleep Med. Rev. 2017, 34, 3–9. [Google Scholar] [CrossRef]
- Stimpfel, A.W.; Aiken, L.H. Hospital staff nurses’ shift length associated with safety and quality of care. J. Nurs. Care Qual. 2013, 28, 122. [Google Scholar] [CrossRef] [Green Version]
- Folkard, S.; Tucker, P. Shift work, safety and productivity. Occup Med. 2003, 53, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ji, A.; Zhu, Y.; Liang, Z.; Wu, J.; Li, S.; Meng, S.; Zheng, X.; Xie, L. A meta-analysis including dose-response relationship between night shift work and the risk of colorectal cancer. Oncotarget 2015, 6, 25046–25060. [Google Scholar] [CrossRef] [Green Version]
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Kolbe-Alexander, T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose-response relationship. Scand. J. Work Environ. Heal 2018, 44, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Adusumilli, J.; Landrigan, C. Effects of reducing or eliminating resident work shifts over 16 hours: A systematic review. Sleep 2010, 33, 1043–1053. Available online: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2910534&tool=pmcentrez&rendertype=abstract (accessed on 13 August 2014).
- Van Dongen, H.P.A.; Maislin, G.; Mullington, J.M.; Dinges, D.F. The cumulative cost of additional wakefulness: Dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep 2003, 26, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Republic of South Africa. Determination: Earnings Threshold. Gov Gaz 2014. Available online: https://web.archive.org/web/20200810153532/https://www.gov.za/sites/default/files/gcis_document/201409/37795gon531.pdf (accessed on 10 August 2020).
- Department of Labour. Code of Good Practice on the Arrangement of Working Time. 1997. Available online: https://web.archive.org/web/20200810153818/http://www.labour.gov.za/DocumentCenter/Code%20of%20Good%20Practice/Basic%20Condition/Code%20of%20Good%20Practice%20on%20the%20Arrangement%20of%20Working%20Time.PDF (accessed on 10 August 2020).
- Health Professions Council of South Africa. Handbook on Internship Training; Health Professions Council of South Africa: Pretoria, South Africa, 2013. [Google Scholar]
- Safe Working Hours. Share Your Safe Working Hours Story. Youtube. Available online: https://www.youtube.com/watch?v=lDGwc7UAAmE&feature=youtu.be (accessed on 12 August 2020).
- Wahl, F. Township ER Trailer. Youtube. Available online: https://www.youtube.com/watch?v=RuGLeIV6v9g (accessed on 12 August 2020).
- Health Professions Council of South Africa. Handbook on Internship Training; Health Professions Council of South Africa: Pretoria, South Africa, 2017. [Google Scholar]
- The Safe Working Hours Campaign. The 2017 Limit on Continuous Shifts for South African Junior Doctors. 2019. Available online: https://web.archive.org/web/20200810154144/https://17d779f3-c893-4fa9-a652-42f3e43cc691.filesusr.com/ugd/068754_8ceab80918ba423abbfc8f23d0c76a46.pdf?index=true (accessed on 10 August 2020).
- Republic of South Africa. Occupational Health and Safety Act, 1993 (Act no 85 of 1993); Government Gazette: Randburg, South Africa, 1993.
- Republic of South Africa. National Health Act, 2004 (Act No. 61 of 2003). 2004. Available online: https://web.archive.org/web/20200810154543/https://www.gov.za/sites/default/files/gcis_document/201409/a61-03.pdf (accessed on 10 August 2020).
- The National Institute for Occupational Safety and Health (NIOSH). Hierarchy of Controls. Available online: https://web.archive.org/web/20200703112701/https://www.cdc.gov/niosh/topics/hierarchy/default.html (accessed on 3 July 2020).
- Pittman, M. NIOSH’s ‘Hierarchy of Controls’. Wikipedia. Available online: https://commons.wikimedia.org/wiki/File:NIOSH’s_“Hierarchy_of_Controls_infographic”_as_SVG.svg (accessed on 11 August 2020).
- Arora, V.; Dunphy, C.; Chang, V.Y.; Ahmad, F.; Humphrey, J.H.; Meltzer, D. The effects of on-duty napping on intern sleep time and fatigue. Ann. Intern. Med. 2006, 144, 792–798. [Google Scholar] [CrossRef]
- Tucker, P.; Brown, M.; Dahlgren, A.; Davies, G.; Ebden, P.; Folkard, S.; Hutchings, H.; Åkerstedt, T. The impact of junior doctors’ worktime arrangements on their fatigue and well-being. Scand. J. Work Environ. Heal 2010, 36, 458–465. [Google Scholar] [CrossRef] [Green Version]
- Michael, E.; Patel, C. Improving medical handover at the weekend: A quality improvement project. BMJ Qual. Improv. Rep. 2015, 4. [Google Scholar] [CrossRef] [Green Version]
- McKenna, H.; Wilkes, M. Optimising sleep for night shifts. Br. Med. J. 2018, 360, j5637. [Google Scholar] [CrossRef]
- Isaacs, L. Armbands to Show Doctor Fatigue Levels. Independent Online. Available online: https://web.archive.org/web/20200703113016/https://www.iol.co.za/capetimes/news/armbands-to-show-doctor-fatigue-levels-2072590 (accessed on 3 July 2020).


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotze, K.; van der Westhuizen, H.-M.; van Loggerenberg, E.; Jawitz, F.; Ehrlich, R. Doctors’ Extended Shifts as Risk to Practitioner and Patient: South Africa as a Case Study. Int. J. Environ. Res. Public Health 2020, 17, 5853. https://doi.org/10.3390/ijerph17165853
Kotze K, van der Westhuizen H-M, van Loggerenberg E, Jawitz F, Ehrlich R. Doctors’ Extended Shifts as Risk to Practitioner and Patient: South Africa as a Case Study. International Journal of Environmental Research and Public Health. 2020; 17(16):5853. https://doi.org/10.3390/ijerph17165853
Chicago/Turabian StyleKotze, Koot, Helene-Mari van der Westhuizen, Eldi van Loggerenberg, Farah Jawitz, and Rodney Ehrlich. 2020. "Doctors’ Extended Shifts as Risk to Practitioner and Patient: South Africa as a Case Study" International Journal of Environmental Research and Public Health 17, no. 16: 5853. https://doi.org/10.3390/ijerph17165853
APA StyleKotze, K., van der Westhuizen, H. -M., van Loggerenberg, E., Jawitz, F., & Ehrlich, R. (2020). Doctors’ Extended Shifts as Risk to Practitioner and Patient: South Africa as a Case Study. International Journal of Environmental Research and Public Health, 17(16), 5853. https://doi.org/10.3390/ijerph17165853