An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand


Abstract
:1. Introduction
2. Methodology
2.1. Estimation of Daily PM2.5/PM10 Ratios and PM2.5 Interpolation
2.2. Estimation of Correlation between PM2.5 and Meteorological Conditions
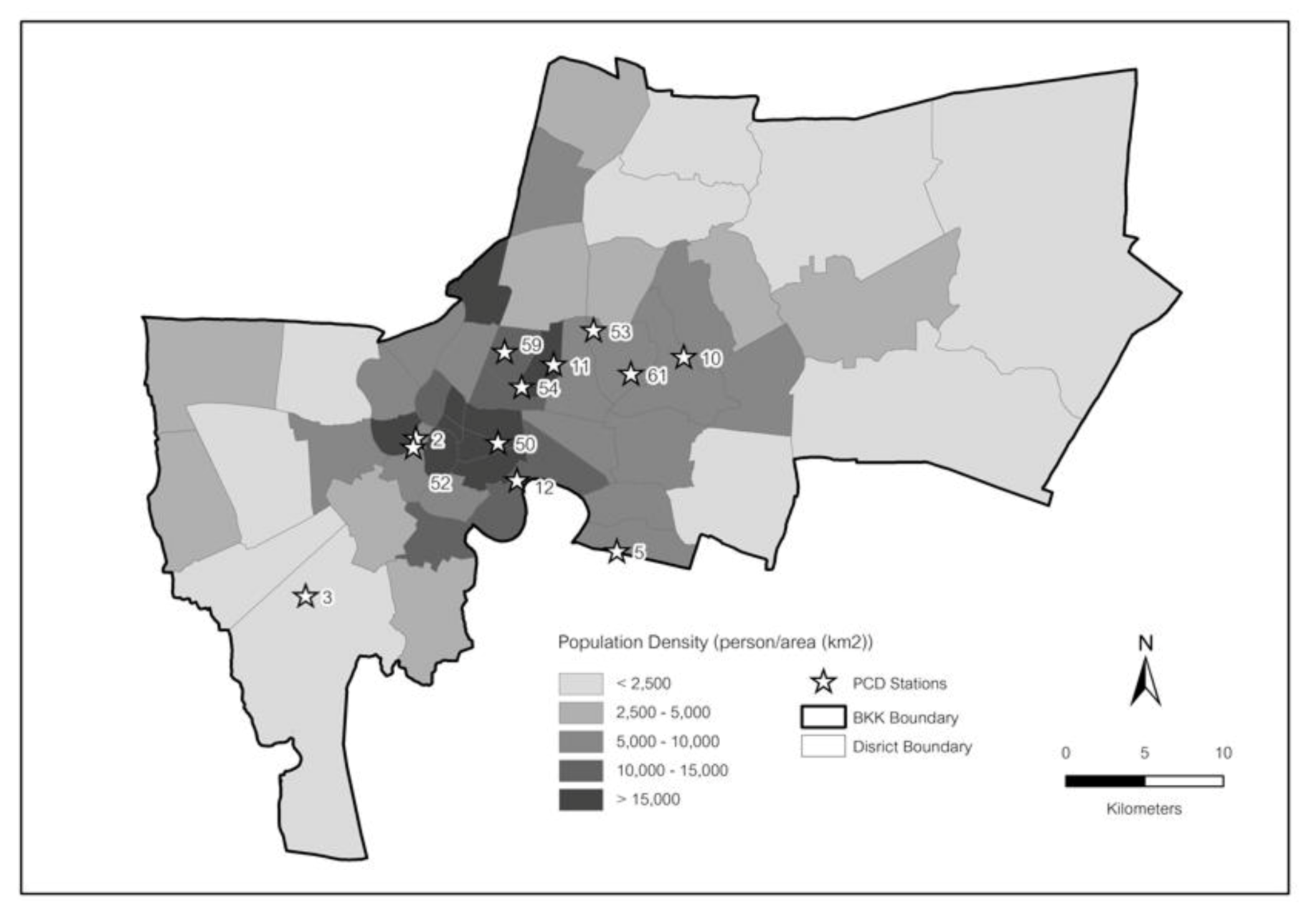
2.3. Mortality Data in Bangkok
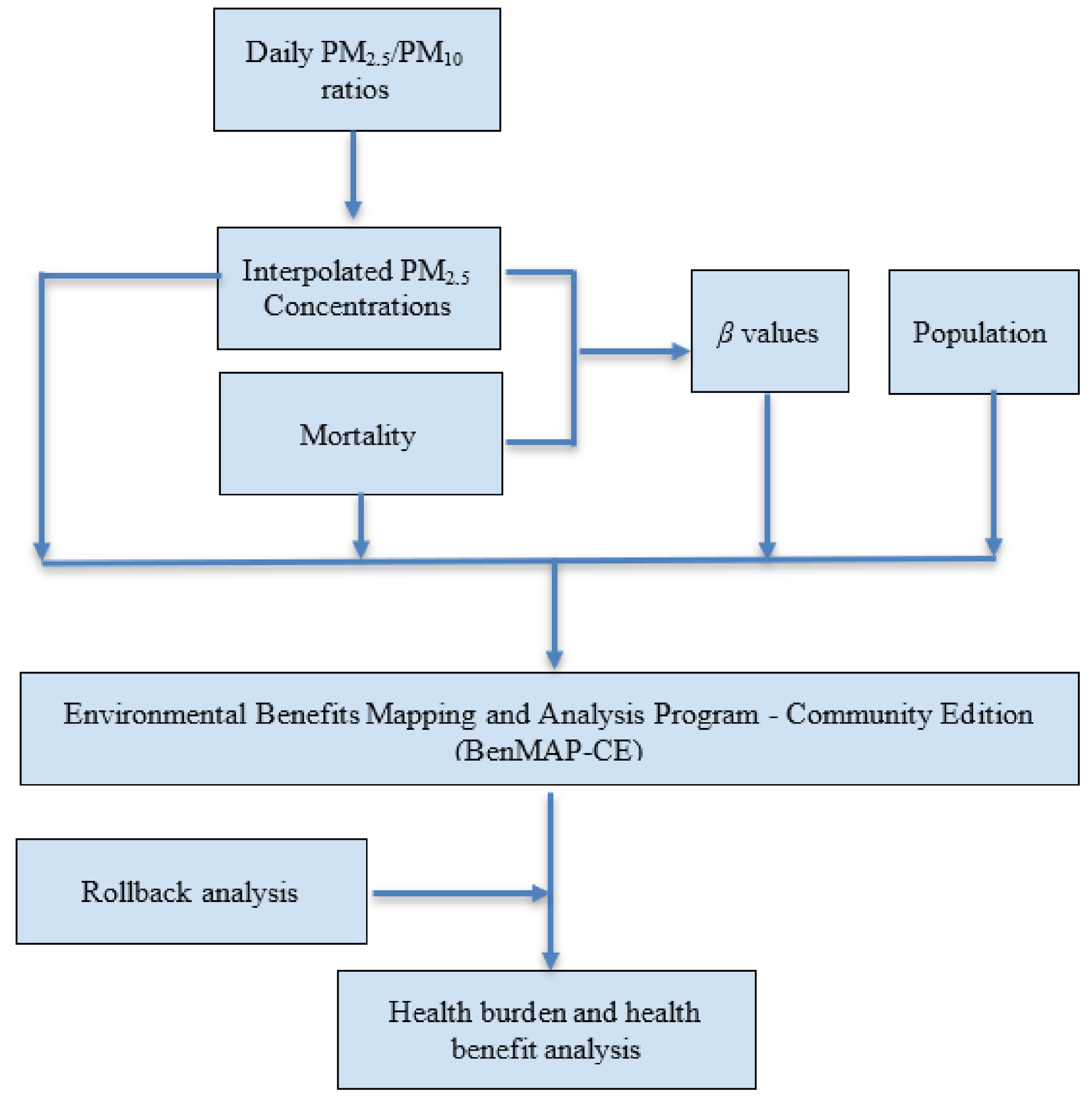
2.4. Health Impact Assessment Using BenMAP
- ΔY is the change in incidence rate;
- Y0 is the baseline incidence rate of the health effects;
- β is the C-R coefficient;
- pop is the exposed population, and
- ∆PM2.5 is the change in PM2.5 concentration to some target or health standard value.
3. Results and Discussion
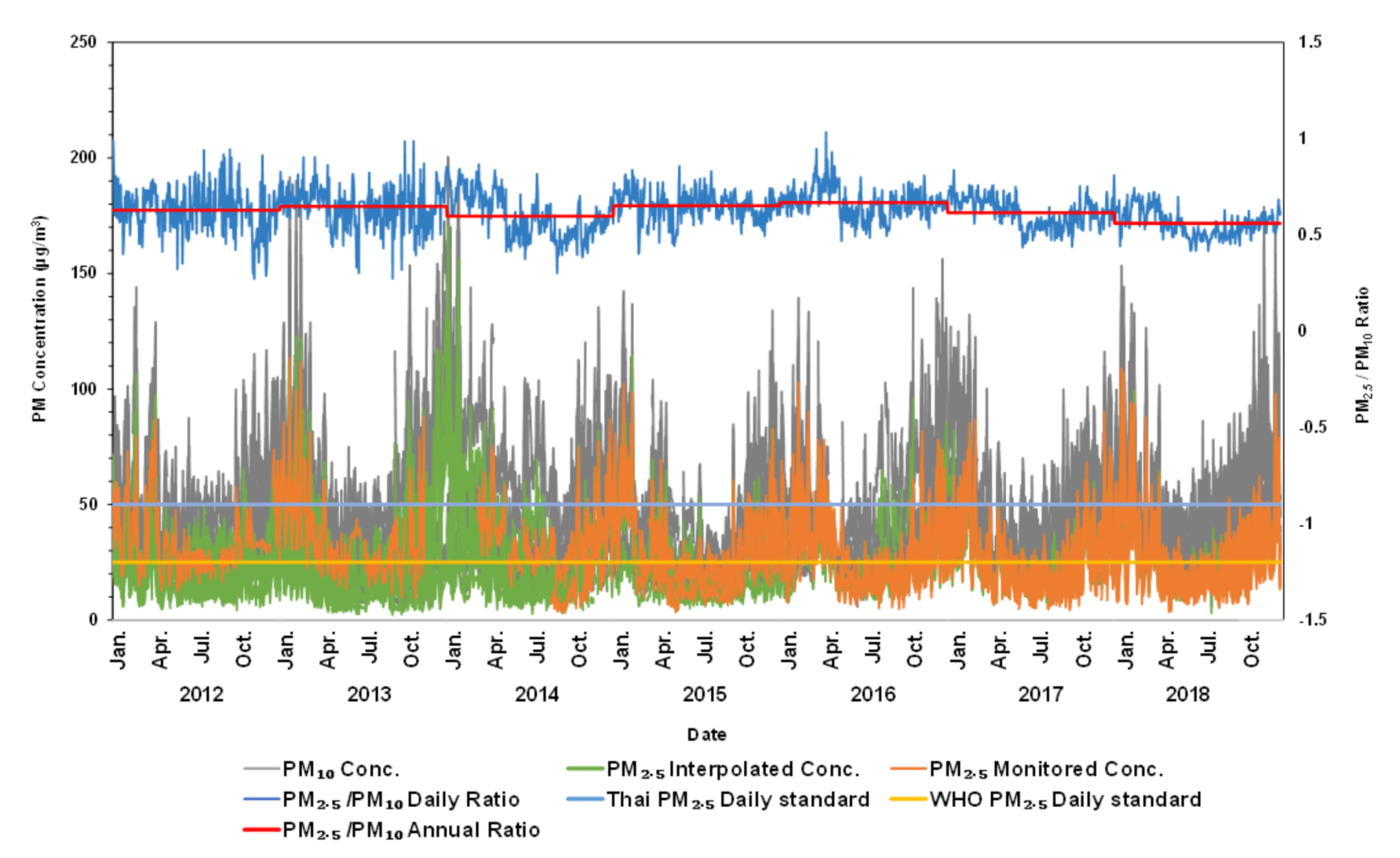
3.1. PM2.5 Interpolation
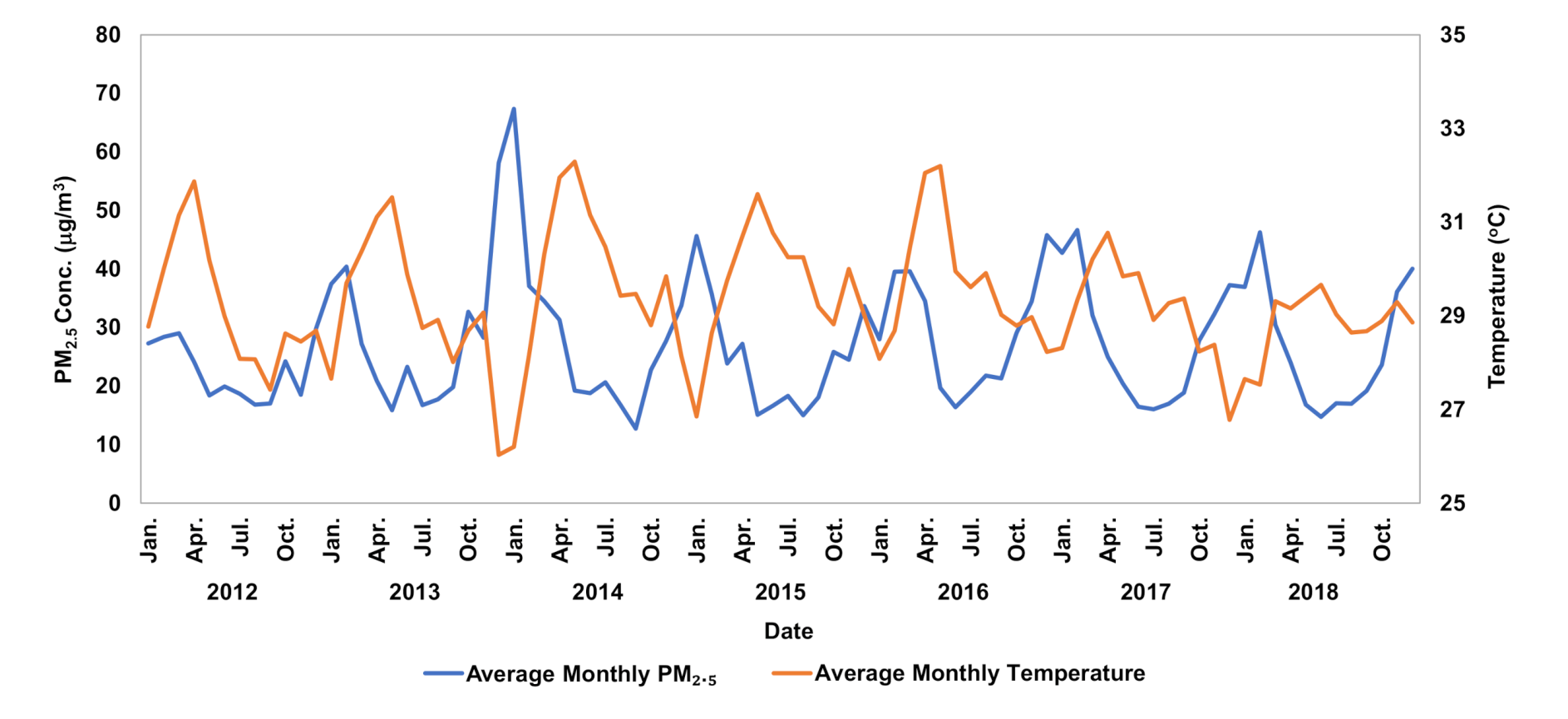
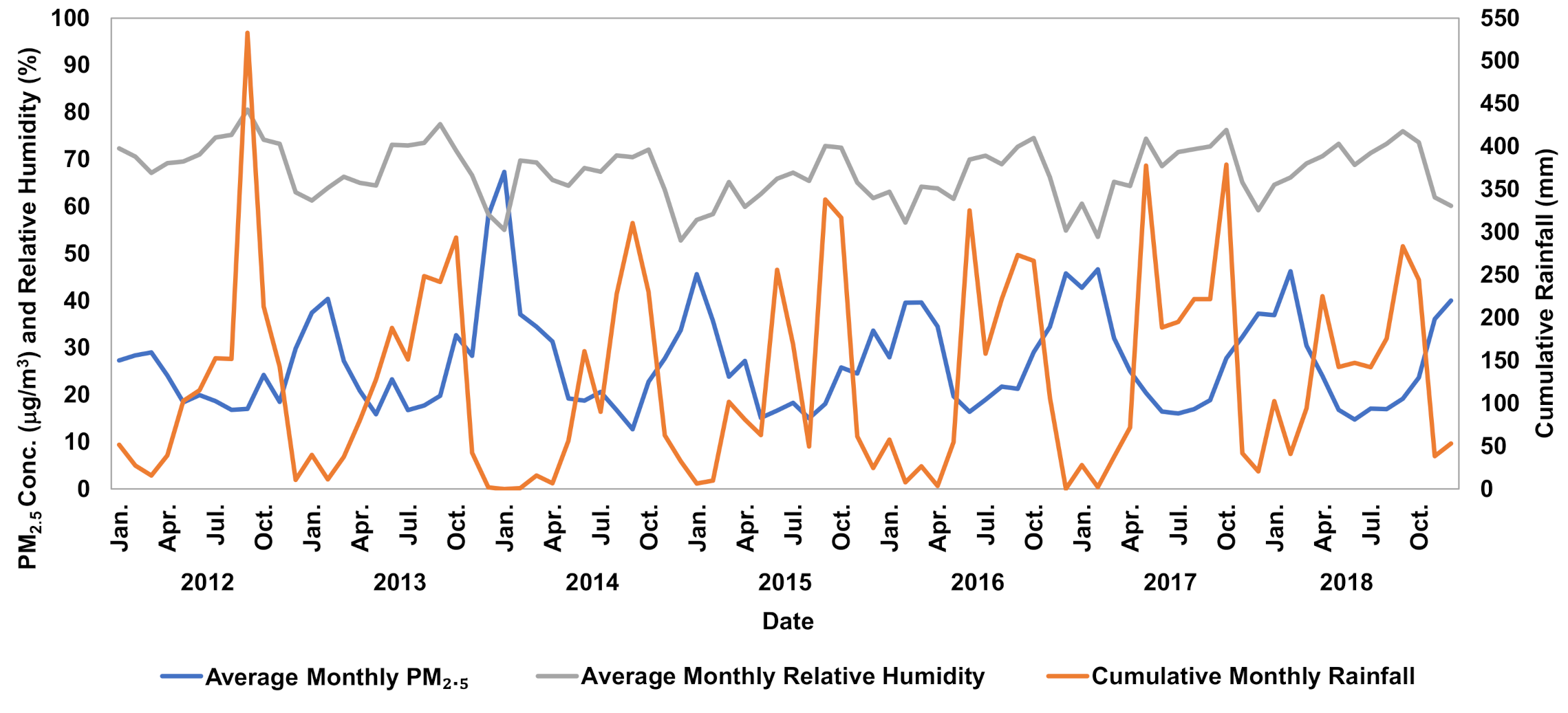
3.2. Correlation between PM2.5 and Meteorological Conditions
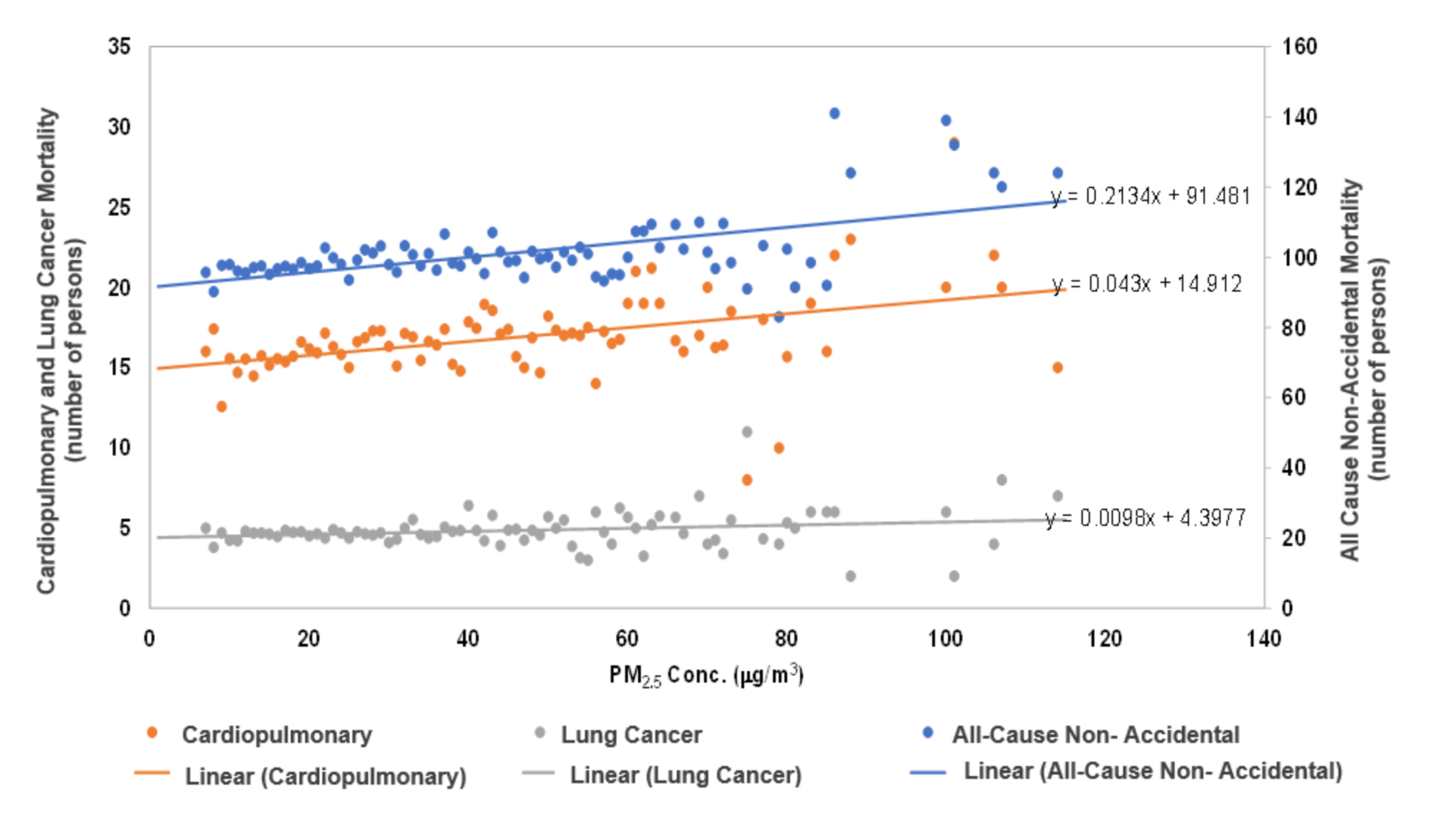
3.3. Health Benefit Analysis
3.4. Uncertainty of the Analysis
4. Conclusions and Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organisation Ambient (Outdoor) Air Quality and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient- (accessed on 23 June 2019).
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Morawska, L.; Pope, C.A., III; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 6736, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Xing, Y.-F.; Xu, Y.-H.; Shi, M.-H.; Lian, Y.-X. The impact of PM2.5 on the human respiratory system. J. Thorac. Dis. 2016, 8, E69–E74. [Google Scholar] [CrossRef] [PubMed]
- Kloog, I.; Ridgway, B.; Koutrakis, P.; Coull, B.; Schwartz, J. Long- and short-term exposure to PM2.5 and mortality. Epidemiology 2013, 24. [Google Scholar] [CrossRef] [PubMed]
- Krzyzanowski, M.; Künzli, N.; Gutschmidt, K.; Pope, A.; Romieu, I.; Samet, J.M.; Smith, K. The global burden of disease due to outdoor air pollution. J. Toxicol. Environ. Health Part A 2005, 68, 1301–1307. [Google Scholar] [CrossRef]
- Afshin, A.; Abate, K.H.; Cristiana, A.; Abbastabar, H. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease. Lancet 2018, 392, 1923–1924. [Google Scholar] [CrossRef] [Green Version]
- Burnett, R.; Chen, H.; Szyszkowicz, M.; Fann, N.; Hubbell, B.; Pope, C.; Apte, J.; Brauer, M.; Cohen, A.; Weichenthal, S.; et al. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc. Natl. Acad. Sci. USA 2018, 115, 9592–9597. [Google Scholar] [CrossRef] [Green Version]
- Limaye, V.S.; Schöpp, W.; Amann, M. Applying integrated exposure-response functions to PM 2.5 pollution in India. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Xu, X.; Chu, M.; Guo, Y.; Wang, J. Air particulate matter and cardiovascular disease: The epidemiological, biomedical and clinical evidence. J. Thorac. Dis. 2016, 8, E8–E19. [Google Scholar] [CrossRef]
- Cao, J.; Yang, C.; Li, J.; Chen, R.; Chen, B.; Gu, D.; Kan, H. Association between long-term exposure to outdoor air pollution and mortality in China: A cohort study. J. Hazard. Mater. 2011, 186, 1594–1600. [Google Scholar] [CrossRef]
- Simkhovich, B.Z.; Kleinman, M.T.; Kloner, R.A. Air pollution and cardiovascular injury: Epidemiology, toxicology, and mechanisms. J. Am. Coll. Cardiol. 2008, 52, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Krewski, D.; Pope, C.A.; Thurston, G.D.; Thun, M.J. Extended Follow-Up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality; HEI Research Report 140; Health Effects Institute: Boston, MA, USA, 2009. [Google Scholar]
- National Statistical Office Thailand. Executive Summary: The 2010 Population and Housing Census; National Statistical Office Thailand: Bangkok, Thailand, 2010. [Google Scholar]
- Sarnat, J.A.; Schwartz, J.; Suh, H.H.; Samet, J.M.; Dominici, F.; Zeger, S.L. Fine particulate air pollution and mortality in 20 U.S. Cities. N. Engl. J. Med. 2001, 344, 1253–1254. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Shi, M.; Gao, S.; Li, S.; Mao, J.; Zhang, H.; Sun, Y.; Bai, Z.; Wang, Z. Assessment of population exposure to PM2.5 for mortality in China and its public health benefit based on BenMAP. Environ. Pollut. 2017, 221, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Qu, Z.; Wang, X.; Li, F.; Li, Y.; Chen, X.; Chen, M. PM2.5-related health economic benefits evaluation based on air improvement action plan in Wuhan city, middle China. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef] [Green Version]
- Ngo, T.H.; Tsai, P.C.; Ueng, Y.F.; Chi, K.H. Cytotoxicity assessment of PM2.5 collected from specific anthropogenic activities in Taiwan. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Hu, H. Combining data from multiple sources to evaluate spatial variations in the economic costs of PM2.5-related health conditions in the Beijing–Tianjin–Hebei region. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piscitelli, P.; Valenzano, B.; Rizzo, E.; Maggiotto, G.; Rivezzi, M.; Corcione, F.E.; Miani, A. Air pollution and estimated health costs related to road transportations of goods in Italy: A first healthcare burden assessment. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, R.; Hu, Y.; Russell, A.G.; Mulholland, J.A.; Odman, M.T. The impacts of prescribed fire on PM2.5 air quality and human health: Application to asthma-related emergency room visits in Georgia, USA. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [Green Version]
- Yu, G.; Wang, F.; Hu, J.; Liao, Y.; Liu, X. Value assessment of health losses caused by PM2.5 in Changsha city, China. Int. J. Environ. Res. Public Health 2019, 16, 2063. [Google Scholar] [CrossRef] [Green Version]
- Kihal-Talantikite, W.; Legendre, P.; Le Nouveau, P.; Deguen, S. Premature adult death and equity impact of a reduction of NO2, PM10, and PM2.5 levels in paris—A health impact assessment study conducted at the census block level. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, J. The effects of particulate air pollution on daily deaths: A multi-city case crossover analysis. Occup. Environ. Med. 2004, 61, 956–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vajanapoom, N.; Shy, C.M.; Neas, L.M.; Loomis, D. Associations of particulate matter and daily mortality in Bangkok, Thailand. Southeast Asian J. Trop. Med. Public Health 2002, 33, 389–399. [Google Scholar] [PubMed]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. J. Am. Med. Assoc. 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, J.; Dockery, D.W.; Neas, L.M. Is daily mortality associated specifically with fine particles? J. Air Waste Manag. Assoc. 1996, 46, 927–939. [Google Scholar] [CrossRef]
- Vichit-Vadakan, N.; Vajanapoom, N.; Ostro, B. The Public Health and Air Pollution in Asia (PAPA) Project: Estimating the mortality effects of particulate matter in Bangkok, Thailand. Environ. Health Perspect. 2008, 116, 1179–1182. [Google Scholar] [CrossRef] [PubMed]
- Vichit-Vadakan, N.; Vajanapoom, N. Health impact from air pollution in Thailand: Current and future challenges. Environ. Health Perspect. 2011, 119, 2–5. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.M.; Vichit-Vadakan, N.; Kan, H.; Qian, Z. Public Health and Air Pollution in Asia (PAPA): A multicity study of short-term effects of air pollution on mortality. Environ. Health Perspect. 2008, 116, 1195–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Li, S.; Tawatsupa, B.; Punnasiri, K.; Jaakkola, J.J.K.; Williams, G. The association between air pollution and mortality in Thailand. Sci. Rep. 2014, 4, 5509. [Google Scholar] [CrossRef] [Green Version]
- Fann, N.; Baker, K.R.; Fulcher, C.M. Characterizing the PM2.5-related health benefits of emission reductions for 17 industrial, area and mobile emission sectors across the U.S. Environ. Int. 2012, 49, 141–151. [Google Scholar] [CrossRef]
- US EPA. Review of the National Ambient Air Quality Standards for Particulate Matter: Policy Assessment of Scientific and Technical Information; Environmental Protection Agency: Research Triangle Park, NC, USA, 1996. [Google Scholar]
- Chuersuwan, N.; Nimrat, S.; Lekphet, S.; Kerdkumrai, T. Levels and major sources of PM2.5 and PM10 in Bangkok Metropolitan Region. Environ. Int. 2008, 34, 671–677. [Google Scholar] [CrossRef]
- Vichit-Vadakan, N.; Ostro, B.D.; Chestnut, L.G.; Mills, D.M.; Aekplakorn, W.; Wangwongwatana, S.; Panich, N. Air pollution and respiratory symptoms: Results from three panel studies in Bangkok, Thailand. Environ. Health Perspect. 2001, 109, 381–387. [Google Scholar] [CrossRef]
- Pinichka, C.; Makka, N.; Sukkumnoed, D.; Chariyalertsak, S.; Inchai, P.; Bundhamcharoen, K. Burden of disease attributed to ambient air pollution in Thailand: A GIS-based approach. PLoS ONE 2017, 12, e0189909. [Google Scholar] [CrossRef] [PubMed]
- WHO International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Available online: https://icd.who.int/browse10/2016/en# (accessed on 10 July 2019).
- US EPA. Environmental Benefits Mapping and Analysis Program—Community Edition User’s Manual; 2017. Available online: https://www.epa.gov/sites/production/files/2015-04/documents/benmap-ce_user_manual_march_2015.pdf (accessed on 1 June 2019).
- Nodzu, M.I.; Ogino, S.Y.; Tachibana, Y.; Yamanaka, M.D. Climatological description of seasonal variations in lower-tropospheric temperature inversion layers over the Indochina Peninsula. J. Clim. 2006, 19, 3307–3319. [Google Scholar] [CrossRef]
- Al-Hemoud, A.; Al-Sudairawi, M.; Al-Rashidi, M.; Behbehani, W.; Al-Khayat, A. Temperature inversion and mixing height: Critical indicators for air pollution in hot arid climate. Nat. Hazards 2019, 97, 139–155. [Google Scholar] [CrossRef]
- Kwak, H.Y.; Ko, J.; Lee, S.; Joh, C.H. Identifying the correlation between rainfall, traffic flow performance and air pollution concentration in Seoul using a path analysis. Transp. Res. Procedia 2017, 25, 3552–3563. [Google Scholar] [CrossRef]
- Jacob, D.J.; Winner, D.A. Effect of climate change on air quality. Atmos. Environ. 2009, 43, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Lambert, S.J.; Fyfe, J.C. Changes in winter cyclone frequencies and strengths simulated in enhanced greenhouse warming experiments: Results from the models participating in the IPCC diagnostic exercise. Clim. Dyn. 2006, 26, 713–728. [Google Scholar] [CrossRef]
- Newell, K.; Kartsonaki, C.; Lam, K.B.H.; Kurmi, O.P. Cardiorespiratory health effects of particulate ambient air pollution exposure in low-income and middle-income countries: A systematic review and meta-analysis. Lancet Planet. Health 2017, 1, e360–e367. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | No. of Station | Missing Data (%) | Statistical Values (µg/m3) | |
|---|---|---|---|---|
| Mean (±SD) | Q1, Q3, and IQR | |||
| 2012 | 1 | 90.3 | 33.7 (±14.0) | 24.2, 38.5, and 14.3 |
| 2013 | 1 | 92.0 | 35.5 (±17.7) | 22.5, 41.3, and 18.9 |
| 2014 | 2 | 88.5 | 30.6 (±16.1) | 20.7, 39.4, and 18.8 |
| 2015 | 3 | 73.2 | 28.1 (±15.4) | 17.5, 35.8, and 18.4 |
| 2016 | 5 | 61.4 | 27.7 (±14.8) | 16.8, 34.3, and 17.5 |
| 2017 | 6 | 46.4 | 26.1 (±14.2) | 15.6, 33.5, and 17.9 |
| 2018 | 10 | 22.5 | 27.2 (±15.3) | 16.6, 33.7, and 17.0 |
| Season | Month | Average PM2.5 (µg/m3) | Average % Relative Humidity | Average Wind Direction (°) | Average Temperature (°C) | Average Wind Speed (m/s) | Monthly Cumulative Rainfall (mm) |
|---|---|---|---|---|---|---|---|
| Dry, Cool | January | 40.8 | 62.0 | 165 | 27.7 | 1.1 | 40.9 |
| Dry, Cool | February | 39.1 | 62.7 | 169 | 28.9 | 1.1 | 14.3 |
| Hot | March | 31.0 | 66.7 | 185 | 30.2 | 1.2 | 47.0 |
| Hot | April | 26.7 | 65.5 | 186 | 31.1 | 1.1 | 72.6 |
| Hot | May | 17.9 | 67.2 | 194 | 31.0 | 1.1 | 132.2 |
| Hot, Rainy | June | 18.0 | 69.4 | 210 | 30.0 | 1.1 | 197.4 |
| Rainy | July | 18.1 | 70.8 | 219 | 29.3 | 1.1 | 151.3 |
| Rainy | August | 17.4 | 71.3 | 220 | 29.2 | 1.1 | 185.2 |
| Rainy | September | 18.2 | 74.7 | 212 | 28.7 | 0.9 | 314.6 |
| Rainy | October | 26.6 | 73.6 | 171 | 28.7 | 0.8 | 277.6 |
| Dry, Cool | November | 28.8 | 66.0 | 156 | 29.1 | 0.9 | 70.9 |
| Dry, Cool | December | 39.8 | 58.6 | 154 | 28.0 | 1.0 | 20.5 |
| Factors | PM2.5 | PM10 | Relative Humidity | Wind Direction | Temperature | Wind Speed | Rain |
|---|---|---|---|---|---|---|---|
| PM2.5 | 1.000 | ||||||
| PM10 | 0.944 | 1.000 | |||||
| Relative Humidity | −0.451 | −0.462 | 1.000 | ||||
| Wind Direction | −0.353 | −0.370 | 0.221 | 1.000 | |||
| Temperature | −0.240 | −0.255 | −0.170 | 0.291 | 1.000 | ||
| Wind Speed | −0.208 | −0.295 | −0.174 | 0.153 | 0.218 | 1.000 | |
| Daily Rainfall | −0.201 | −0.201 | 0.485 | 0.032 | −0.261 | −0.215 | 1.000 |
| United States a | China b | |||
|---|---|---|---|---|
| Health Endpoints | β Values (Standard Deviation) | Avoided Mortality | β Values (Standard Deviation) | Avoided Mortality |
| Mortality, All-cause non-accidental | 0.00583 (±0.00096) | 2772 | 0.000896 (±0.000538) | 374 |
| Mortality, cardiopulmonary | 0.0122 (±0.00135) | 1686 | 0.002547 (±0.006250) | 316 |
| Mortality, lung cancer | 0.0131 (±0.00379) | 291 | 0.00334 (±0.001758) | 67 |
| Health Endpoint | Health Burden | Thailand Standard 25 µg/m3 | WHO Guideline 10 µg/m3 |
|---|---|---|---|
| Deaths * (95% CI) | Avoided Deaths * (95% CI) | Avoided Deaths * (95% CI) | |
| Mortality, non-accidental | 4240 (1219–6938) | 1393 (593–2691) | 3159 (893–5248) |
| Mortality, cardiopulmonary | 1317 (1065–1551) | 360 (284–434) | 959 (769–1140) |
| Mortality, lung cancer | 370 (175–530) | 102 (45–156) | 270 (125–397) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fold, N.R.; Allison, M.R.; Wood, B.C.; Thao, P.T.B.; Bonnet, S.; Garivait, S.; Kamens, R.; Pengjan, S. An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand. Int. J. Environ. Res. Public Health 2020, 17, 7298. https://doi.org/10.3390/ijerph17197298
Fold NR, Allison MR, Wood BC, Thao PTB, Bonnet S, Garivait S, Kamens R, Pengjan S. An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand. International Journal of Environmental Research and Public Health. 2020; 17(19):7298. https://doi.org/10.3390/ijerph17197298
Chicago/Turabian StyleFold, Nathaniel R., Mary R. Allison, Berkley C. Wood, Pham T. B. Thao, Sebastien Bonnet, Savitri Garivait, Richard Kamens, and Sitthipong Pengjan. 2020. "An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand" International Journal of Environmental Research and Public Health 17, no. 19: 7298. https://doi.org/10.3390/ijerph17197298
APA StyleFold, N. R., Allison, M. R., Wood, B. C., Thao, P. T. B., Bonnet, S., Garivait, S., Kamens, R., & Pengjan, S. (2020). An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand. International Journal of Environmental Research and Public Health, 17(19), 7298. https://doi.org/10.3390/ijerph17197298