Regular Moderate- to Vigorous-Intensity Physical Activity Rather Than Walking Is Associated with Enhanced Cognitive Functions and Mental Health in Young Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Demographic Information
2.2.2. PA
2.2.3. Cognitive Functions
2.2.4. Mental Health
2.3. Data Analysis
3. Results
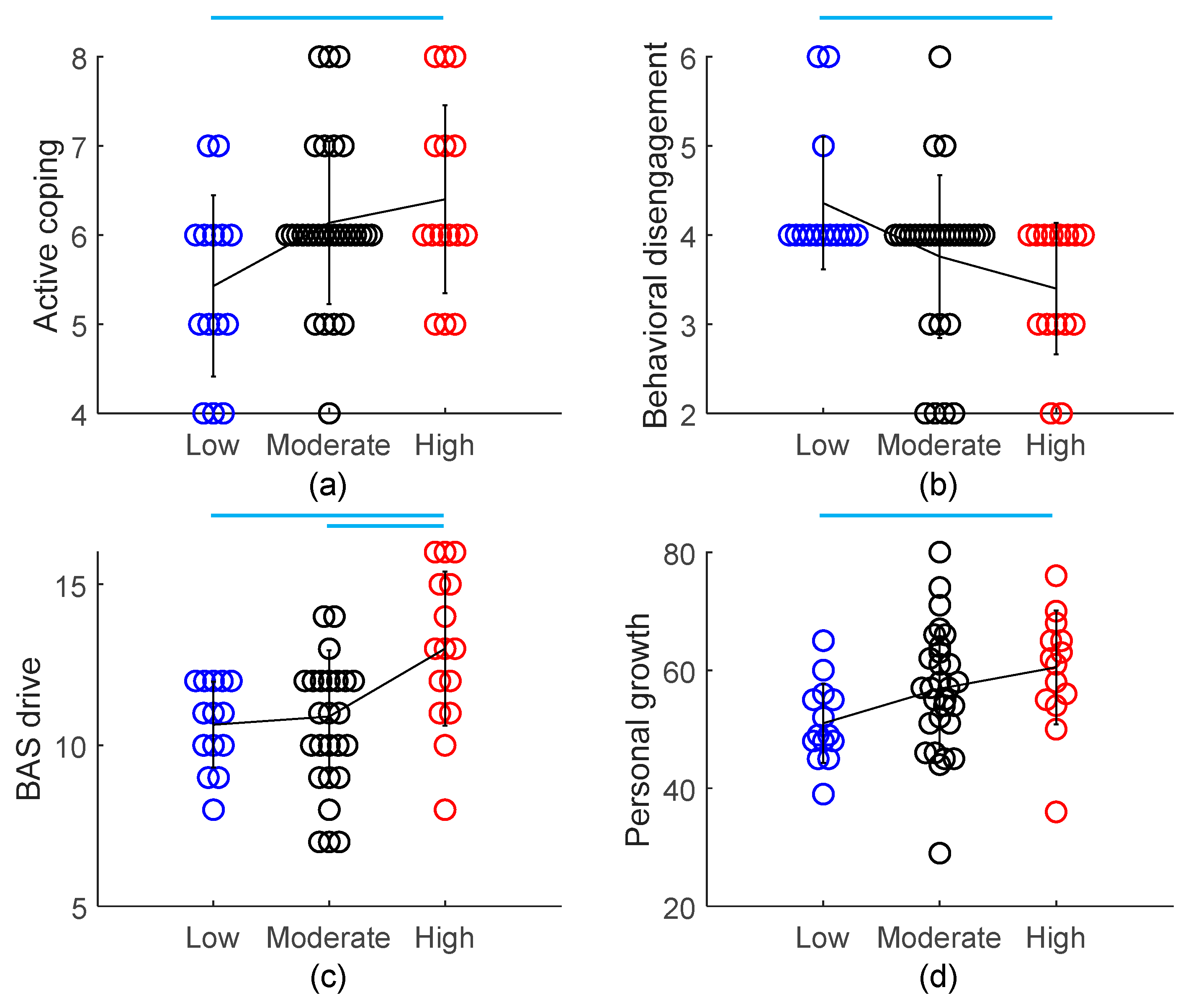
3.1. PA Level
Comparison of Cognitive Functions and Mental Health across Different PA Levels
3.2. Intensity-Specific Frequency
3.2.1. Correlations among Intensity-Specific Frequencies
3.2.2. Linear Regression: Which Frequency Predicts Outcome Variables?
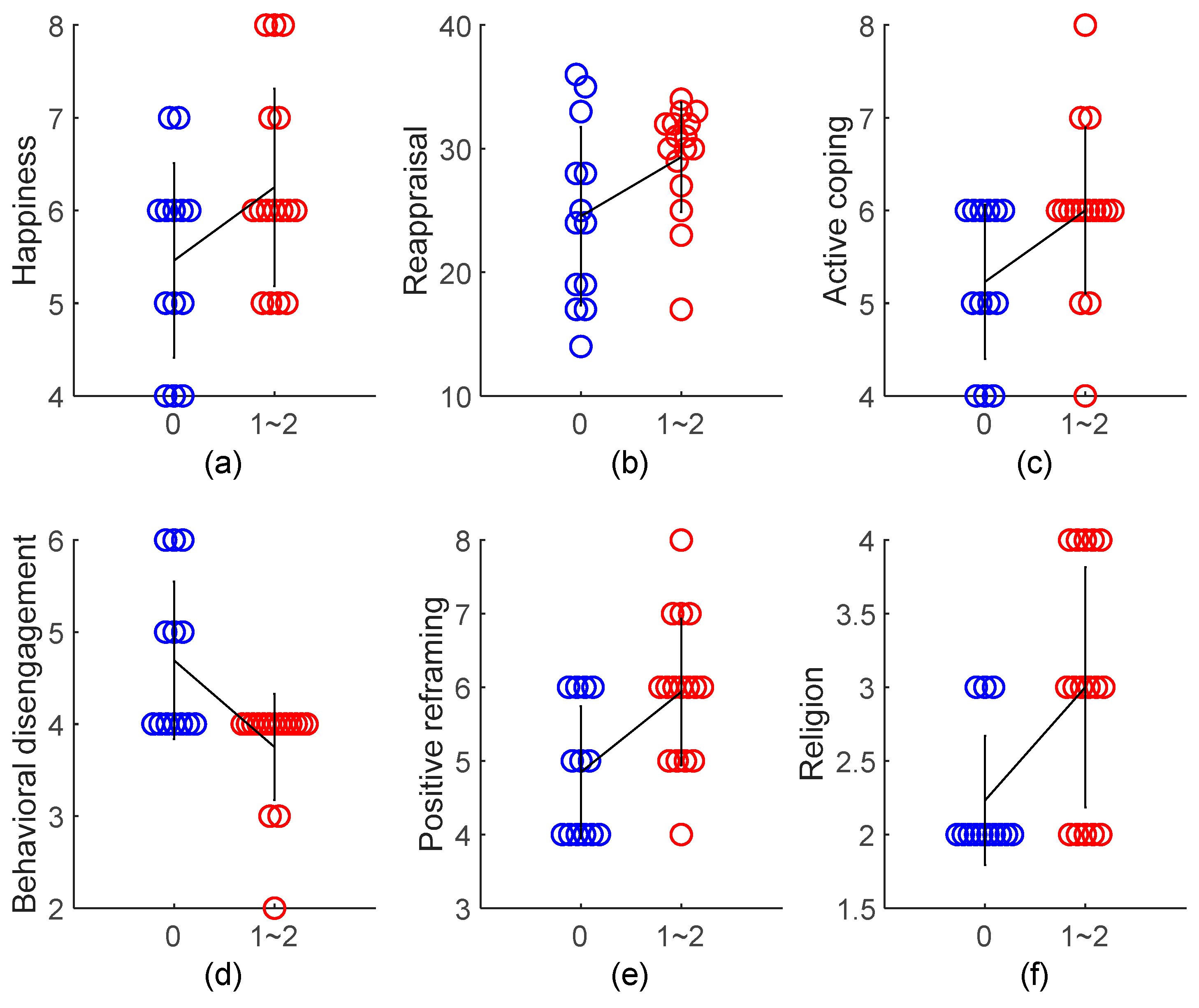
3.2.3. Combining the Frequency of Moderate- and Vigorous-Intensity PA: The Frequency of MVPA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58. [Google Scholar] [CrossRef] [PubMed]
- Basso, J.C.; Suzuki, W.A. The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: A review. Brain Plast. 2017, 2, 127–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Nakagawa, S.; An, Y.; Ito, K.; Kitaichi, Y.; Kusumi, I. The exercise-glucocorticoid paradox: How exercise is beneficial to cognition, mood, and the brain while increasing glucocorticoid levels. Front. Neuroendocrinol. 2017, 44, 83–102. [Google Scholar] [CrossRef] [PubMed]
- Chen, C. Fitness Powered Brains: Optimize Your Productivity, Leadership and Performance; Brain & Life Publishing: London, UK, 2017. [Google Scholar]
- Stimpson, N.J.; Davison, G.; Javadi, A.H. Joggin’the noggin: Towards a physiological understanding of exercise-induced cognitive benefits. Neurosci. Biobehav. Rev. 2018, 88, 177–186. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Hillman, C.H.; Fernhall, B.O.; Thompson, K.M.; Valentini, T.A. The effect of acute aerobic and resistance exercise on working memory. Med. Sci. Sports Exerc. 2009, 41, 927–934. [Google Scholar] [CrossRef] [Green Version]
- Yanagisawa, H.; Dan, I.; Tsuzuki, D.; Kato, M.; Okamoto, M.; Kyutoku, Y.; Soya, H. Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with Stroop test. Neuroimage 2010, 50, 1702–1710. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Parks, A.C.; Henning, D.A.; Kamijo, K. Single bouts of exercise selectively sustain attentional processes. Psychophysiology 2015, 52, 618–625. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, H.; Sykes, E.A.; Moss, T.; Lowery, S.; LeBoutillier, N.; Dewey, A. Exercise enhances creativity independently of mood. Br. J. Sports Med. 1997, 31, 240–245. [Google Scholar] [CrossRef]
- Reed, J.; Ones, D.S. The effect of acute aerobic exercise on positive activated affect: A meta-analysis. Psychol. Sport Exerc. 2006, 7, 477–514. [Google Scholar] [CrossRef]
- Chaddock-Heyman, L.; Erickson, K.I.; Voss, M.; Knecht, A.; Pontifex, M.B.; Castelli, D.; Hillman, C.; Kramer, A. The effects of physical activity on functional MRI activation associated with cognitive control in children: A randomized controlled intervention. Front. Hum. Neurosci. 2013, 7, 72. [Google Scholar] [CrossRef] [Green Version]
- Ishihara, T.; Mizuno, M. Effects of tennis play on executive function in 6–11-year-old children: A 12-month longitudinal study. Eur. J. Sport Sci. 2018, 18, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlager, N.T.; Cox, K.L.; Flicker, L.; Foster, J.K.; van Bockxmeer, F.M.; Xiao, J.; Greenop, K.R.; Almeida, O.P. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. JAMA 2008, 300, 1027–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Childs, E.; de Wit, H. Regular exercise is associated with emotional resilience to acute stress in healthy adults. Front. Physiol. 2014, 5, 161. [Google Scholar] [CrossRef] [PubMed]
- Lucas, M.; Mekary, R.; Pan, A.; Mirzaei, F.; O’Reilly, É.J.; Willett, W.C.; Koenen, K.; Okereke, O.I.; Ascherio, A. Relation between clinical depression risk and physical activity and time spent watching television in older women: A 10-year prospective follow-up study. Am. J. Epidemiol. 2011, 174, 1017–1027. [Google Scholar] [CrossRef] [Green Version]
- Cooney, G.M.; Dwan, K.; Greig, C.A.; Lawlor, D.A.; Rimer, J.; Waugh, F.R.; McMurdo, M.; Mead, G.E. Exercise for depression. Cochrane Database Syst. Rev. 2013, 9. [Google Scholar] [CrossRef]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.K.; Etnier, J.L. Exploring the dose-response relationship between resistance exercise intensity and cognitive function. J. Sport Exerc. Psychol. 2009, 31, 640–656. [Google Scholar] [CrossRef] [Green Version]
- Holmes, M.M.; Galea, L.A.; Mistlberger, R.E.; Kempermann, G. Adult hippocampal neurogenesis and voluntary running activity: Circadian and dose-dependent effects. J. Neurosci. Res. 2004, 76, 216–222. [Google Scholar] [CrossRef]
- Larson, E.B.; Wang, L.; Bowen, J.D.; McCormick, W.C.; Teri, L.; Crane, P.; Kukull, W. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann. Intern. Med. 2006, 144, 73–81. [Google Scholar] [CrossRef]
- Harvey, S.B.; Øverland, S.; Hatch, S.L.; Wessely, S.; Mykletun, A.; Hotopf, M. Exercise and the prevention of depression: Results of the HUNT Cohort Study. Am. J. Psychiatry 2017, 175, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1· 2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Wise, L.A.; Adams-Campbell, L.L.; Palmer, J.R.; Rosenberg, L. Leisure time physical activity in relation to depressive symptoms in the Black Women’s Health Study. Ann. Behav. Med. 2006, 32, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamer, M.; Molloy, G.J.; de Oliveira, C.; Demakakos, P. Leisure time physical activity, risk of depressive symptoms, and inflammatory mediators: The English Longitudinal Study of Ageing. Psychoneuroendocrinology 2009, 34, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Hötting, K.; Schickert, N.; Kaiser, J.; Röder, B.; Schmidt-Kassow, M. The effects of acute physical exercise on memory, peripheral BDNF, and cortisol in young adults. Neural Plast. 2016, 2016, 12. [Google Scholar] [CrossRef] [Green Version]
- Raichlen, D.A.; Foster, A.D.; Gerdeman, G.L.; Seillier, A.; Giuffrida, A. Wired to run: Exercise-induced endocannabinoid signaling in humans and cursorial mammals with implications for the ‘runner’s high’. J. Exp. Biol. 2012, 215, 1331–1336. [Google Scholar] [CrossRef] [Green Version]
- Fuss, J.; Steinle, J.; Bindila, L.; Auer, M.K.; Kirchherr, H.; Lutz, B.; Gass, P. A runner’s high depends on cannabinoid receptors in mice. Proc. Natl. Acad. Sci. USA 2015, 112, 13105–13108. [Google Scholar] [CrossRef] [Green Version]
- Parikh, T.; Stratton, G. Influence of intensity of physical activity on adiposity and cardiorespiratory fitness in 5–18 year olds. Sports Med. 2011, 41, 477–488. [Google Scholar] [CrossRef]
- Åberg, M.A.; Pedersen, N.L.; Torén, K.; Svartengren, M.; Bäckstrand, B.; Johnsson, T.; Cooper-Kuhn, C.M.; Åberg, N.D.; Nilsson, M.; Kuhn, H.G. Cardiovascular fitness is associated with cognition in young adulthood. Proc. Natl. Acad. Sci. USA 2009, 106, 20906–20911. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Steptoe, A. Association between physical fitness, parasympathetic control, and proinflammatory responses to mental stress. Psychosom. Med. 2007, 69, 660–666. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.F.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Knoblich, G.; Ohlsson, S.; Haider, H.; Rhenius, D. Constraint relaxation and chunk decomposition in insight problem solving. J. Exp. Psychol. Learn. Memory Cognit. 1999, 25, 1534. [Google Scholar] [CrossRef]
- Lu, J.G.; Akinola, M.; Mason, M.F. “Switching On” creativity: Task switching can increase creativity by reducing cognitive fixation. Organ. Behav. Hum. Decis. Process. 2017, 139, 63–75. [Google Scholar] [CrossRef]
- Jaeggi, S.M.; Studer-Luethi, B.; Buschkuehl, M.; Su, Y.F.; Jonides, J.; Perrig, W.J. The relationship between n-back performance and matrix reasoning—Implications for training and transfer. Intelligence 2010, 38, 625–635. [Google Scholar] [CrossRef]
- JAQuent/nBack. Available online: https://github.com/JAQuent/nBack (accessed on 4 December 2019).
- McCarthy, D.; Davison, M. Signal probability, reinforcement and signal detection. J. Exp. Anal. Behav. 1979, 32, 373–386. [Google Scholar] [CrossRef] [Green Version]
- Inoue, Y. The Measurement of Mindfulness: The Third Wave of Behavioral and Cognitive Therapies for Mood Disorders. Doshisha Policy Manag. Rev. 2014, 15, 141–152. [Google Scholar]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822. [Google Scholar] [CrossRef] [Green Version]
- Kimura, M.; Yogo, M.; Daibo, I. Development of Japanese version of the Emotional Contagion Scale. Jpn. J. Interpers. Soc. Psychol. 2007, 7, 31–39. [Google Scholar]
- Doherty, R.W. The emotional contagion scale: A measure of individual differences. J. Nonverbal Behav. 1997, 21, 131–154. [Google Scholar] [CrossRef]
- Yoshizu, J.; Sekiguchi, R.; Amemiya, T. Development of a Japanese version of emotion regulation questionnaire. Jpn. J. Res. Emot. 2013, 20, 56–62. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348. [Google Scholar] [CrossRef]
- Otsuka, Y. The COPE Inventory: A theoretically based coping questionnaire. Hiroshima Univ. Psychol. Res. 2008, 8, 121–128. [Google Scholar]
- Carver, C.S. You want to measure coping but your protocol’too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Yamagata, S.; Kijima, N.; Shigemasu, K.; Ono, Y.; Ando, J. Gray’s Temperament Model: Development of Japanese Version of BIS/BAS Scales and A Behavior Genetic Investigation Using the Twin Method. Jpn. J. Person. 2007, 15, 276–289. [Google Scholar] [CrossRef]
- Carver, C.S.; White, T.L. Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS scales. J. Personal. Soc. Psychol. 1994, 67, 319. [Google Scholar] [CrossRef]
- Kojima, M.; Furukawa, T. Manual for the Japanese Version of Beck Depression Inventory, 2nd ed.; Nihon Bunka Kagakusha Co., Ltd.: Tokyo, Japan, 2003. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and -II in psychiatric outpatients. J. Personal. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Hidano, T.; Fukuda, M.; Iwawaki, S.; Soga, Y.; Spielberger, C.D. State-Trait Anxiety Inventory-JYZ; Jitsumukyoiku-Shuppan Co., Ltd.: Tokyo, Japan, 2000. [Google Scholar]
- Spielberger, C.D.; Gorssuch, R.L.; Lushene, P.R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Sumi, K. Reliability and validity of the Japanese version of the Perceived Stress Scale. Jpn. J. Health Psychol. 2006, 19, 44–53. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Kitamura, T.; Kishida, Y.; Gatayama, R.; Matsuoka, T.; Miura, S.; Yamabe, K. Ryff’s psychological well-being inventory: Factorial structure and life history correlates among Japanese university students. Psychol. Rep. 2004, 94, 83–103. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069. [Google Scholar] [CrossRef]
- Kato, T. Frequently used coping scales: A meta-analysis. Stress Health 2015, 31, 315–323. [Google Scholar] [CrossRef]
- Litman, J.A.; Lunsford, G.D. Frequency of use and impact of coping strategies assessed by the COPE Inventory and their relationships to post-event health and well-being. J. Health Psychol. 2009, 14, 982–991. [Google Scholar] [CrossRef]
- Chen, C.; Takahashi, T.; Nakagawa, S.; Inoue, T.; Kusumi, I. Reinforcement learning in depression: A review of computational research. Neurosci. Biobehav. Rev. 2015, 55, 247–267. [Google Scholar] [CrossRef] [PubMed]
- Whitton, A.E.; Treadway, M.T.; Pizzagalli, D.A. Reward processing dysfunction in major depression, bipolar disorder and schizophrenia. Curr. Opin. Psychiatry 2015, 28, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Ann. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.L.; Miles, E.; Sheeran, P. Dealing with feeling: A meta-analysis of the effectiveness of strategies derived from the process model of emotion regulation. Psychol. Bull. 2012, 138, 775. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Cerin, E.; Leslie, E.; Sugiyama, T.; Owen, N. Associations of multiple physical activity domains with mental well-being. Mental Health Phys. Act. 2009, 2, 55–64. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Measure | Mean ± SD | Measure | Mean ± SD |
|---|---|---|---|
| PA | Cognitive functions | ||
| PA level | Low = 14, Moderate = 29, High = 15 | Creativity (Quiz) | 1.00 ± 0.82 |
| Working memory | |||
| Intensity-specific frequency (days/week) | 1-back d | 2.77 ± 0.34 | |
| Walking | 3.64 ± 2.40 | 1-back response time (ms) | 668.2 ± 170.0 |
| Moderate | 1.50 ± 1.74 | 2-back d | 2.55 ± 0.39 |
| Vigorous | 1.26 ± 1.62 | 2-back response time (ms) | 800.1 ± 203.2 |
| Mindful attention (MAAS) | 44.1 ± 8.98 | ||
| Mental health | |||
| Emotional contagion (ECS) | Substance use | 2.66 ± 1.12 | |
| Love | 9.53 ± 1.58 | Behavioral disengagement | 3.81 ± 0.89 |
| Happiness | 5.86 ± 1.34 | Self-blame | 5.19 ± 1.53 |
| Anger | 8.57 ± 1.73 | BIS/BAS | |
| Sadness | 8.40 ± 1.61 | BIS | 20.9 ± 4.57 |
| Emotion regulation (ERQ) | Drive | 11.4 ± 2.20 | |
| Reappraisal | 27.8 ± 6.47 | Fun seeking | 12.1 ± 4.52 |
| Suppression | 13.2 ± 4.34 | Reward responsiveness | 16.7 ± 2.35 |
| Coping (COPE) | Depression (BDI-II) | 7.29 ± 6.45 | |
| Active coping | 6.03 ± 1.03 | State anxiety (STAI-Y1) | 37.2 ± 7.98 |
| Planning | 6.12 ± 1.06 | Trait anxiety (STAI-Y2) | 43.3 ± 9.59 |
| Positive reframing | 5.50 ± 1.47 | Perceived stress (PSS) | 18.2 ± 4.80 |
| Acceptance | 6.24 ± 1.07 | Psychological wellbeing (PWI) | |
| Humor | 4.31 ± 1.66 | Autonomy | 49.5 ± 8.33 |
| Religion | 2.81 ± 1.10 | Environmental mastery | 54.7 ± 8.24 |
| Using emotional support | 5.64 ± 1.44 | Personal growth | 56.4 ± 9.89 |
| Using instrumental support | 5.97 ± 1.31 | Positive relations with others | 58.6 ± 9.18 |
| Self-distraction | 5.60 ± 1.20 | Purpose in life | 56.2 ± 10.0 |
| Denial | 2.76 ± 1.07 | Self-acceptance | 51.0 ± 10.8 |
| Venting | 5.34 ± 1.37 | ||
| Independent Variables | Working Memory | Coping (COPE) | Psychological Wellbeing (PWI) | ||||
|---|---|---|---|---|---|---|---|
| 2-back d | Active Coping | Denial | Behavioral Disengagement | Autonomy | Personal Growth | ||
| Model 1 | Walking (days/week) | −0.026 | 0.001 | 0.124 * | −0.006 | 0.352 | 0.357 |
| Moderate (days/week) | 0.068 * | 0.085 | −0.084 | −0.134 * (−0.263) 1 | −0.616 | 1.27 | |
| Vigorous (days/week) | 0.034 | 0.251 ** | −0.123 | −0.245 ** (−0.447) | 2.08 ** | 2.32 ** | |
| F(3,54) | 3.122 | 3.460 | 3.439 | 5.409 | 4.025 | 3.319 | |
| R2 | 0.148 | 0.161 | 0.160 | 0.231 | 0.183 | 0.156 | |
| p | 0.033 | 0.023 | 0.023 | 0.003 | 0.012 | 0.026 | |
| Model 2 | Walking (days/week) | −0.023 | −0.005 | 0.118 + | −0.003 | 0.354 | 0.226 |
| Moderate (days/week) | 0.071 * | 0.087 | −0.089 | −0.131 * (−0.257) | −0.627 | 1.16 | |
| Vigorous (days/week) | 0.035 | 0.298 ** | −0.119 | −0.248 ** (−0.452) | 1.885 * | 2.467 ** (0.404) | |
| Gender2 | −0.011 | 0.424 | 0.079 | −0.045 | −1.605 | 2.147 | |
| Age | −0.022 | 0.035 | 0.051 | −0.029 | 0.061 | 1.111 * (0.270) | |
| F(5,52) | 2.089 | 2.670 | 2.201 | 3.247 | 2.452 | 3.262 | |
| R2 | 0.167 | 0.204 | 0.175 | 0.238 | 0.191 | 0.239 | |
| p | 0.082 | 0.032 | 0.068 | 0.013 | 0.045 | 0.012 | |
| Measure | Correlation Coefficient | Measure | Correlation Coefficient |
|---|---|---|---|
| Cognitive functions | |||
| Creativity (Quiz) | 0.275 | ||
| Working memory | 2-back d | 0.343 ** | |
| 1-back d | −0.046 | 2-back response time | −0.087 |
| 1-back response time | −0.101 | Mindful attention (MAAS) | −0.165 |
| Mental health | |||
| Emotional contagion (ECS) | Substance use | −0.034 | |
| Love | 0.199 | Behavioral disengagement | −0.454 ** |
| Happiness | −0.047 | Self-blame | 0.076 |
| Anger | −0.125 | BIS/BAS | |
| Sadness | 0.107 | BIS | −0.024 |
| Emotion regulation (ERQ) | Drive | 0.291 * | |
| Reappraisal | 0.159 | Fun seeking | −0.027 |
| Suppression | 0.013 | Reward responsiveness | 0.269 * |
| Coping (COPE) | Depression (BDI-II) | 0.014 | |
| Active coping | 0.345 ** | State anxiety (STAI-Y1) | −0.268 * |
| Planning | 0.193 | Trait anxiety (STAI-Y2) | −0.150 |
| Positive reframing | 0.136 | Perceived stress (PSS) | −0.008 |
| Acceptance | 0.280 * | Psychological wellbeing (PWI) | |
| Humor | −0.099 | Autonomy | 0.136 |
| Religion | 0.162 | Environmental mastery | 0.189 |
| Using emotional support | 0.222 | Personal growth | 0.367 * |
| Using instrumental support | −0.015 | Positive relations with others | 0.157 |
| Self-distraction | −0.210 | Purpose in life | 0.236 |
| Denial | −0.287 * | Self-acceptance | 0.204 |
| Venting | −0.228 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakagawa, T.; Koan, I.; Chen, C.; Matsubara, T.; Hagiwara, K.; Lei, H.; Hirotsu, M.; Yamagata, H.; Nakagawa, S. Regular Moderate- to Vigorous-Intensity Physical Activity Rather Than Walking Is Associated with Enhanced Cognitive Functions and Mental Health in Young Adults. Int. J. Environ. Res. Public Health 2020, 17, 614. https://doi.org/10.3390/ijerph17020614
Nakagawa T, Koan I, Chen C, Matsubara T, Hagiwara K, Lei H, Hirotsu M, Yamagata H, Nakagawa S. Regular Moderate- to Vigorous-Intensity Physical Activity Rather Than Walking Is Associated with Enhanced Cognitive Functions and Mental Health in Young Adults. International Journal of Environmental Research and Public Health. 2020; 17(2):614. https://doi.org/10.3390/ijerph17020614
Chicago/Turabian StyleNakagawa, Takumi, Ibuki Koan, Chong Chen, Toshio Matsubara, Kosuke Hagiwara, Huijie Lei, Masako Hirotsu, Hirotaka Yamagata, and Shin Nakagawa. 2020. "Regular Moderate- to Vigorous-Intensity Physical Activity Rather Than Walking Is Associated with Enhanced Cognitive Functions and Mental Health in Young Adults" International Journal of Environmental Research and Public Health 17, no. 2: 614. https://doi.org/10.3390/ijerph17020614
APA StyleNakagawa, T., Koan, I., Chen, C., Matsubara, T., Hagiwara, K., Lei, H., Hirotsu, M., Yamagata, H., & Nakagawa, S. (2020). Regular Moderate- to Vigorous-Intensity Physical Activity Rather Than Walking Is Associated with Enhanced Cognitive Functions and Mental Health in Young Adults. International Journal of Environmental Research and Public Health, 17(2), 614. https://doi.org/10.3390/ijerph17020614