Development of the Nurses’ Occupational Stressor Scale

 , ,
, ,
Abstract
:1. Introduction
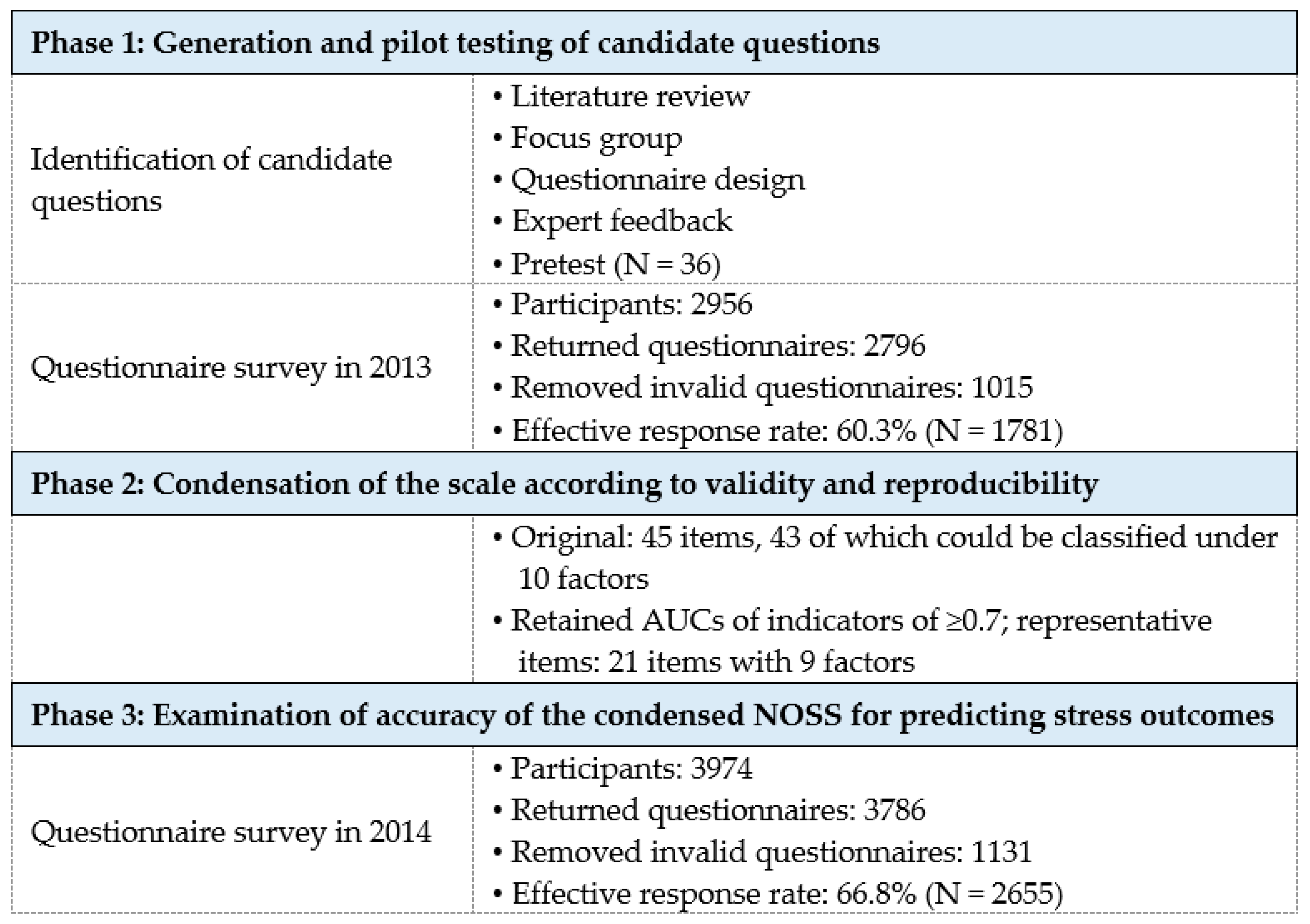
2. Materials and Methods
2.1. Study Design
2.2. Participants and Ethical Considerations
2.3. Data Collection
2.3.1. Personal Burnout and Client-Related Burnout
2.3.2. Job Dissatisfaction and Intention to Leave
2.4. Data Analysis
3. Results
3.1. Phase 1: Generation and Pilot Testing of Candidate Questions
3.1.1. Methods of Constructing Questions
3.1.2. Content Validity Index
3.1.3. Phase 1 Questionnaire Survey
3.1.4. Construct Validity
3.1.5. Test-Retest Reliability
3.1.6. Internal Consistency Reliability
3.2. Phase 2: Condensation of the NOSS According to Validity and Reproducibility
3.3. Phase 3: Examination of Accuracy of the Condensed NOSS for Predicting Stress Outcomes
3.3.1. Phase 3 Questionnaire Survey
3.3.2. Test-Retest Reliability of the 21-Item Condensed NOSS
3.3.3. Internal Consistency Reliability of the 21-Item Condensed NOSS
3.3.4. Comparison of the prediction accuracy of the original NOSS and condensed NOSS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Labour Organization. Occupational Stress and Stress Prevention in Specific Occupations. Available online: https://www.ilo.org/safework/areasofwork/workplace-health-promotion-and-well-being/WCMS_250122/lang--en/index.htm (accessed on 3 January 2020).
- Bobbio, A.; Manganelli, A.M. Antecedents of hospital nurses’ intention to leave the organization: A cross sectional survey. Int. J. Nurs. Stud. 2015, 52, 1180–1192. [Google Scholar] [CrossRef]
- Wang, J.; Okoli, C.T.C.; He, H.; Feng, F.; Li, J.; Zhuang, L.; Lin, M. Factors associated with compassion satisfaction, burnout, and secondary traumatic stress among Chinese nurses in tertiary hospitals: A cross-sectional study. Int. J. Nurs. Stud. 2020, 102, 103472. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Jóźwik, M. Positive orientation and strategies for coping with stress as predictors of professional burnout among Polish nurses. Int. J. Environ. Res. Public Health 2019, 16, 4264. [Google Scholar] [CrossRef] [Green Version]
- Khamisa, N.; Peltzer, K.; Ilic, D.; Oldenburg, B. Work related stress, burnout, job satisfaction and general health of nurses: A follow-up study. Int. J. Nurs. Pract. 2016, 22, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, G.; Mancuso, S.; Fiz Perez, F.; Castiello D’Antonio, A.; Mucci, N.; Cupelli, V.; Arcangeli, G. Bullying among nurses and its relationship with burnout and organizational climate. Int. J. Nurs. Pract. 2016, 22, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Chin, W.S.; Chen, Y.C.; Ho, J.J.; Cheng, N.Y.; Wu, H.C.; Shiao, J.S.C. Psychological work environment and suicidal ideation among nurses in Taiwan. J. Nurs. Scholarsh. 2019, 51, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Sochalski, J.; Silber, J.H. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA 2002, 288, 1987–1993. [Google Scholar] [CrossRef] [Green Version]
- Petit Dit Dariel, O.; Regnaux, J.P. Do Magnet®-accredited hospitals show improvements in nurse and patient outcomes compared to non-Magnet hospitals: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 168–219. [Google Scholar] [CrossRef]
- Ying, L.; Aungsuroch, Y. Factors influencing nurse-assessed quality nursing care: A cross-sectional study in hospitals. J. Adv. Nurs. 2018, 74, 935–945. [Google Scholar]
- Chin, W.; Guo, Y.L.; Hung, Y.J.; Hsieh, Y.T.; Wang, L.J.; Shiao, J.S. Workplace justice and intention to leave the nursing profession. Nurs. Ethics 2019, 26, 307–319. [Google Scholar] [CrossRef]
- Liu, W.; Zhao, S.; Shi, L.; Zhang, Z.; Liu, X.; Li, L.; Duan, X.; Li, G.; Lou, F.; Jia, X.; et al. Workplace violence, job satisfaction, burnout, perceived organisational support and their effects on turnover intention among Chinese nurses in tertiary hospitals: A cross-sectional study. BMJ Open 2018, 8, e019525. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Union of Nurses Association (TUNA). Statistics of Nurses in Taiwan and Fujian Provinces: From 2013 to 2019. (In Chinese). Available online: http://www.nurse.org.tw/publicUI/H/H102.aspx (accessed on 3 January 2020).
- Ministry of Health, Singapore. Health Manpower. Available online: https://www.moh.gov.sg/content/moh_web/home/statistics/Health_Facts_Singapore/Health_Manpower.html (accessed on 3 January 2020).
- Nursing and Midwifery Board of Australia. NMBA Quarterly Registration Data. Available online: http://www.nursingmidwiferyboard.gov.au/News/Newsletters/September-2015.aspx#quarterlydata (accessed on 3 January 2020).
- Taiwan Union of Nurses Association (TUNA). The survey of the nursing workforce. TUNA Nurs. Newsl. 2010, 76, 2–3. (In Chinese) [Google Scholar]
- Leineweber, C.; Chungkham, H.S.; Lindqvist, R.; Westerlund, H.; Runesdotter, S.; Smeds Alenius, L.; Tishelman, C. Nurses’ practice environment and satisfaction with schedule flexibility is related to intention to leave due to dissatisfaction: A multi-country, multilevel study. Int. J. Nurs. Stud. 2016, 58, 47–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aqeel Alkhawaldeh, J.F.M.; Soh, K.L.; Mukhtar, F.B.M.; Ooi, C.P. Effectiveness of stress management interventional program on occupational stress for nurses: A systematic review. J. Nurs. Manag. 2019. [Google Scholar] [CrossRef] [PubMed]
- Happell, B.; Dwyer, T.; Reid-Searl, K.; Burke, K.J.; Caperchione, C.M.; Gaskin, C.J. Nurses and stress: Recognizing causes and seeking solutions. J. Nurs. Manag. 2013, 21, 638–647. [Google Scholar] [CrossRef]
- Rainbow, J.G.; Steege, L.M. Transition to practice experiences of first- and second-career nurses: A mixed-methods study. J. Clin. Nurs. 2019, 28, 1193–1204. [Google Scholar] [CrossRef]
- French, S.E.; Lenton, R.; Walters, V.; Eyles, J. An empirical evaluation of an expanded Nursing Stress Scale. J. Nurs. Manag. 2000, 8, 161–178. [Google Scholar] [CrossRef]
- Lake, E.T. Development of the practice environment scale of the Nursing Work Index. Res. Nurs. Health 2002, 25, 176–188. [Google Scholar] [CrossRef]
- Yeh, W.Y.; Cheng, Y.W.; Chen, M.J.; Chiu, A.W.H. Development and validation of an occupational burnout inventory. Taiwan J. Public Health 2008, 27, 349–364. [Google Scholar]
- Chin, W.; Guo, Y.L.; Hung, Y.J.; Yang, C.Y.; Shiao, J.S. Short sleep duration is dose-dependently related to job strain and burnout in nurses: A cross sectional survey. Int. J. Nurs. Stud. 2015, 52, 297–306. [Google Scholar] [CrossRef]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Tobias, S.; Carlson, J.E. Brief report: Bartlett’s test of sphericity and chance findings in factor analysis. Multivar. Behav. Res. 1969, 4, 375–377. [Google Scholar] [CrossRef]
- Lin, M.H.; Kuo, C.Y. Survey of Perceptions of Safety and Health in the Work Environment in 2013 Taiwan (IOSH102-M306); Institute of Labor, Occupational Safety and Health, Ministry of Labor: New Taipei City, Taiwan, 2014; (In Chinese, English Abstract).
- Netemeyer, R.G.; Boles, J.S.; McMurrian, R. Development and validation of work–family conflict and family–work conflict scales. J. Appl. Psychol. 1996, 81, 400–410. [Google Scholar] [CrossRef]
- Kneebone, I.I.; Dewar, S.J. Reliability and validity of the Attributional Style Questionnaire- Survey in people with multiple sclerosis. Ther. Adv. Neurol. Disord. 2017, 10, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Developing and testing self-reporting scales. In Nursing Research: Generating and Assessing Evidence for Nursing Practice, 9th ed.; Polit, D.F., Beck, C.T., Eds.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 351–378. [Google Scholar]
- Peltzer, K.; Mashego, T.A.; Mabeba, M. Short communication: Occupational stress and burnout among South African medical practitioners. Stress Health 2003, 19, 275–280. [Google Scholar] [CrossRef]
- Chen, L.; Liu, J.; Yang, H.; Ma, H.; Wang, H.; Huang, Y.; Cheng, H.; Tang, D.; Liu, M.; Luo, H.; et al. Work-family conflict and job burn-out among Chinese doctors: The mediating role of coping styles. BMJ Open 2018, 31, e000004. [Google Scholar] [CrossRef]
- Brauchli, R.; Bauer, G.F.; Hämmig, O. Relationship between time-based work-life conflict and burnout: A cross-sectional study among employees in four large Swiss enterprises. Swiss J. Psychol. 2011, 70, 165–173. [Google Scholar] [CrossRef]
- World Health Organization. Occupational Health: A Manual for Primary Health Care Workers. Available online: https://www.who.int/occupational_health/publications/emhealthcarework/en/ (accessed on 26 December 2019).
- Yip, Y. A study of work stress, patient handling activities and the risk of low back pain among nurses in Hong Kong. J. Adv. Nurs. 2001, 36, 794–804. [Google Scholar] [CrossRef]
- Smith, D.R.; Mihashi, M.; Adachi, Y.; Koga, H.; Ishitake, T. A detailed analysis of musculoskeletal disorder risk factors among Japanese nurses. J. Saf. Res. 2006, 37, 195–200. [Google Scholar] [CrossRef]
- Kozak, A.; Schedlbauer, G.; Peters, C.; Nienhaus, A. Self-reported musculoskeletal disorders of the distal upper extremities and the neck in German veterinarians: A cross-sectional study. PLoS ONE 2014, 9, e89362. [Google Scholar] [CrossRef]
- Mizuno-Lewis, S.; McAllister, M. Taking leave from work: The impact of culture on Japanese female nurses. J. Clin. Nurs. 2008, 17, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Brindley, P.G. Psychological burnout and the intensive care practitioner: A practical and candid review for those who care. J. Intensive Care Soc. 2017, 18, 270–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilcoyne, M.; Dowling, M. Working in an overcrowded accident and emergency department: Nurses’ narratives. Aust. J. Adv. Nurs. 2008, 25, 21–27. [Google Scholar]
- Bekker, M.; Coetzee, S.K.; Klopper, H.C.; Ellis, S.M. Non-nursing tasks, nursing tasks left undone and job satisfaction among professional nurses in South African hospitals. J. Nurs. Manag. 2015, 23, 1115–1125. [Google Scholar] [CrossRef]
- Tschannen, D.; Kalisch, B.J.; Lee, K.H. Missed nursing care: The impact on intention to leave and turnover. Can. J. Nurs. Res. 2010, 42, 22–39. [Google Scholar]
- Hinz, C. How to Deal with Difficult Family Members of Patients. Available online: https://dailynurse.com/how-to-deal-with-difficult-family-members-of-patients/ (accessed on 26 December 2019).
- Lu, Y.; Hu, X.M.; Huang, X.L.; Zhuang, X.D.; Guo, P.; Feng, L.F.; Hu, W.; Chen, L.; Zou, H.; Hao, Y.T. The relationship between job satisfaction, work stress, work–family conflict, and turnover intention among physicians in Guangdong, China: A cross-sectional study. BMJ Open 2017, 7, e014894. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.L.; Chen, K.L.; Lee, L.H.; Yang, C.I. Working in a danger zone: A qualitative study of Taiwanese nurses’ work experiences in a negative pressure isolation ward. Am. J. Infect. Control 2016, 44, 809–814. [Google Scholar] [CrossRef]
- Butts, M.M.; Casper, W.J.; Yang, T.S. How important are work-family support policies? A meta-analytic investigation of their effects on employee outcomes. J. Appl. Psychol. 2013, 98, 1–25. [Google Scholar] [CrossRef]
- Wendsche, J.; Ghadiri, A.; Bengsch, A.; Wegge, J. Antecedents and outcomes of nurses’ rest break organization: A scoping review. Int. J. Nurs. Stud. 2017, 75, 65–80. [Google Scholar] [CrossRef]
- Xu, D.; Chen, L.; Wan, X.; Zhang, Y.; Liu, N.; Wang, K. Toileting behaviour and related health beliefs among Chinese female nurses. Int. J. Clin. Pract. 2016, 70, 416–423. [Google Scholar] [CrossRef]
- Chao, S.Y.; Roth, P. The experiences of Taiwanese women caring for parents-in-law. J. Adv. Nurs. 2000, 31, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Lash, T.L. (Eds.) Validity in Epidemiologic Studies. In Modern Epidemiology, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 129–146. [Google Scholar]
- Carpenter, S. Ten steps in scale development and reporting: A guide for researchers. Commun. Methods Meas. 2018, 12, 25–44. [Google Scholar] [CrossRef]
- Mucci, N.; Giorgi, G.; Roncaioli, M.; Fiz Perez, J.; Arcangeli, G.; Mucci, N. The correlation between stress and economic crisis: A systematic review. Neuropsychiatr. Dis. Treat. 2016, 12, 983–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charos, D.; Kolypera, V.; Lazaridou, E.; Andriopoulou, M.; Vivilaki, V.; Livanis, E. The impact of occupational stress on health care professionals during the financial crisis. Arch. Hell. Med. 2017, 34, 467–475. [Google Scholar]


{kind=link}
| Variable | Eligible Participants in 1st Year (N = 1781) | Eligible Participants in 2nd Year (N = 2655) | ||||||
|---|---|---|---|---|---|---|---|---|
| n | % | Mean | SD | n | % | Mean | SD | |
| Age (years) | 30.3 | 6.6 | 32.5 | 7.3 | ||||
| ≤30 | 1022 | 57.4 | 1152 | 43.4 | ||||
| 31–40 | 619 | 34.8 | 1097 | 41.3 | ||||
| ≥40 | 135 | 7.6 | 365 | 13.7 | ||||
| Missing | 5 | 0.3 | 41 | 1.5 | ||||
| Marital status | ||||||||
| Single | 1145 | 64.3 | 1439 | 54.2 | ||||
| Married | 606 | 34.0 | 1145 | 43.1 | ||||
| Divorce or widow | 27 | 1.5 | 53 | 2.0 | ||||
| Missing | 3 | 0.2 | 18 | 0.7 | ||||
| Educational level | ||||||||
| Professional school | 20 | 1.1 | 93 | 3.5 | ||||
| Junior college | 634 | 35.6 | 921 | 34.7 | ||||
| College or above | 1124 | 63.1 | 1631 | 61.4 | ||||
| Missing | 3 | 0.2 | 10 | 0.4 | ||||
| Total work tenure (years) | 8.6 | 6.8 | 10.1 | 7.3 | ||||
| <5 | 729 | 40.9 | 877 | 33.0 | ||||
| 5–10 | 508 | 28.5 | 694 | 26.1 | ||||
| 11–15 | 259 | 14.5 | 516 | 19.4 | ||||
| 16–20 | 183 | 10.3 | 310 | 11.7 | ||||
| ≥20 | 101 | 5.7 | 236 | 8.9 | ||||
| Missing | 1 | 0.1 | 22 | 0.8 | ||||
| Working hours/day | 9.3 | 1.1 | 9.2 | 1.2 | ||||
| Working hours/week | 49.9 | 8.1 | 47.8 | 7.7 | ||||
| Sleeping hours/day | 6.8 | 1.3 | 6.8 | 1.2 | ||||
| Personal burnout (standardized score: 0–100) | 63.9 | 21.0 | 59.9 | 20.5 | ||||
| Personal burnout ≥ 95 | 230 | 12.9 | 241 | 9.1 | ||||
| Client-related Burnout (standardized score: 0–100) | 47.9 | 18.7 | 46.8 | 19.8 | ||||
| Client-related burnout ≥ 75 | 190 | 10.7 | 290 | 10.9 | ||||
| Score of intention to leave (score: 0–10) | 5.6 | 2.8 | 5.4 | 2.7 | ||||
| Had intention to leave | 255 | 15.5 | 255 | 10.4 | ||||
| Subscales and Component Items | Factor Loading |
|---|---|
| 1. Work Demands | |
| I am worried about receiving complaints from patients or their relatives for not meeting their demands. | 0.68 |
| I have to bear the negative sentiment of patients or their relatives. | 0.76 |
| I do not have sufficient time to meet patients’ and their relatives’ demands. | 0.74 |
| I am unsure of the extent of patients’ conditions or treatments that I should reveal to them. | 0.59 |
| Excessive duties in the workplace prevent me from attending to patients. | 0.61 |
| I have to maintain professional units other than my own. | 0.49 |
| 2. Work–Family Conflict | |
| The burden of work affects my domestic life. | 0.75 |
| The amount of time my job occupies makes it difficult for me to fulfill family responsibilities. | 0.83 |
| The burden of work makes it difficult for me to undertake my personal chores and/or engage in hobbies. | 0.83 |
| My job produces strain that makes it difficult for me to fulfill my family duties. | 0.83 |
| I have to adapt my schedule for family activities/outings to accommodate my work responsibilities. | 0.74 |
| 3. Insufficient Support from Coworkers or Caregivers | |
| The professional evaluation of care of mine is opposite to that of the doctors. | 0.62 |
| Doctors’ temperamental nature agitates me. | 0.56 |
| I cannot instantaneously obtain patient-related information because of inadequate communication within the team. | 0.68 |
| Team members do not appear to help in a timely manner under urgent circumstances. | 0.65 |
| Lack of support from the team affects patients’ trust in me. | 0.63 |
| 4. Workplace Violence and Bullying | |
| Verbal abuse such as insults and sarcastic comments. | 0.66 |
| Psychological abuse such as threats, discrimination, bullying, and harassment. | 0.83 |
| Physical abuse such as hitting, kicking, pushing, pinching, pulling, and dragging. | 0.71 |
| Sexual harassment such as inappropriate implications and behaviors. | 0.68 |
| 5. Organizational Issues | |
| The on-call system affects my life. | 0.66 |
| My working hours include on-call hours. | −0.48 |
| I was informed of a change to my schedule at less than 24 hours’ notice. | 0.54 |
| The organization usually remunerates my overtime work at a low rate of pay. | 0.40 |
| Not achieving a promotion (e.g., level 1 or 2) within the expected period affects my income. | 0.45 |
| 6. Occupational Hazards | |
| Exposure to chemicals such as chemotherapy drugs, alcohol, and Cidex. | 0.63 |
| Exposure to radiation or strong light such as X-ray, ultraviolet light, and lasers. | 0.67 |
| I feel stressed considering that my patients might be have contagious diseases such as SARS or AIDS a. | 0.38 |
| Transporting patients or equipment. | 0.61 |
| The workplace offers sufficient protective equipment such as masks and gowns. | −0.35 |
| 7. Difficulty Taking Leave | |
| The level of difficulty in asking for leaves for household emergencies is_______% (0% = very difficult, 100% = very smooth) b. | 0.87 |
| The level of difficulty in excusing myself for feeling strong discomfort is_______% (0% = very difficult, 100% = very smooth) b. | 0.80 |
| 8. Powerlessness | |
| Patients’ conditions do not improve. | 0.66 |
| Encountering the death of a patient. | 0.70 |
| I have insufficient time to offer mental health care to patients during working hours. | 0.45 |
| 9. Interpersonal Relationships | |
| Relationships among colleagues within the unit are generally good. | −0.34 |
| I should teach student nurses and newcomers while caring for patients. | 0.55 |
| I worry that my colleagues’ incompetence will affect patient safety. | 0.45 |
| The manager or head nurse supports me in the event of a conflict between me and a patient. | −0.38 |
| Primary caregivers do not execute their tasks appropriately. | 0.38 |
| 10. Unmet Basic Physiological Needs | |
| I have no time to fulfill my personal needs (e.g., water consumption and toilet breaks). | 0.61 |
| I cannot take an uninterrupted 30-minute mealtime break. | 0.80 |
| I can receive deserved compensation such as premiums and compensatory leave for overtime of more than 1 h. | −0.47 |
| Factor | Personal Burnout a | Client-Related Burnout b | Job Dissatisfaction c | Intention to Leave d | ||||
|---|---|---|---|---|---|---|---|---|
| OR | AUC | OR | AUC | OR | AUC | OR | AUC | |
| 1 | 1.04 *** | 0.68 | 1.05 *** | 0.73 | 1.06 *** | 0.77 | 1.06 *** | 0.78 |
| 2 | 1.04 *** | 0.68 | 1.06 *** | 0.75 | 1.04 *** | 0.69 | 1.04 *** | 0.67 |
| 3 | 1.03 *** | 0.64 | 1.04 *** | 0.70 | 1.05 *** | 0.71 | 1.05 *** | 0.73 |
| 4 | 1.02 *** | 0.64 | 1.03 *** | 0.70 | 1.03 *** | 0.70 | 1.04 *** | 0.71 |
| 5 | 1.02 *** | 0.64 | 1.02 *** | 0.64 | 1.02 *** | 0.63 | 1.02 *** | 0.63 |
| 6 | 1.02 *** | 0.60 | 1.03 *** | 0.69 | 1.03 *** | 0.67 | 1.03 *** | 0.68 |
| 7 | 1.02 *** | 0.66 | 1.01 *** | 0.62 | 1.01 *** | 0.63 | 1.01 *** | 0.61 |
| 8 | 1.02 *** | 0.59 | 1.03 *** | 0.64 | 1.02 *** | 0.61 | 1.02 *** | 0.62 |
| 9 | 1.02 *** | 0.63 | 1.04 *** | 0.69 | 1.04 *** | 0.68 | 1.04 *** | 0.70 |
| 10 | 1.00 | 0.51 | 0.99 | 0.53 | 0.99 | 0.53 | 0.99 * | 0.53 |
| Item | Mean | SD | Cronbach’s α if the Item is Deleted | |
|---|---|---|---|---|
| Subscale 1: Work Demands (Cronbach’s α: 0.61) | ||||
| 1 | I have to bear negative sentiment from patients or their relatives. | 3.16 | 0.66 | 0.44 |
| 2 | Excessive duties in the workplace prevent me from attending to patients. | 3.01 | 0.73 | 0.58 |
| 3 | I have to maintain professional units other than my own. | 3.24 | 0.72 | 0.50 |
| Subscale 2: Work–Family Conflict (Cronbach’s α: 0.70) | ||||
| 4 | The burden of work affects my domestic life. | 2.89 | 0.69 | 0.79 |
| 5 | The burden of work makes it difficult for me to undertake my personal chores and/or engage in hobbies. | 2.82 | 0.73 | 0.53 |
| 6 | I have to adapt my schedule for family activities/outings to accommodate my work responsibilities. | 3.11 | 0.65 | 0.52 |
| Subscale 3: Insufficient Support from Coworkers or Caregivers (Cronbach’s α: 0.62) | ||||
| 7 | Doctors’ temperamental nature agitates me. | 3.14 | 0.69 | 0.48 |
| 8 | I worry that my colleagues’ incompetence will affect patient safety. | 2.85 | 0.68 | 0.56 |
| 9 | I feel stressed because primary caregivers do not execute their tasks appropriately. | 2.96 | 0.65 | 0.53 |
| Subscale 4: Workplace Violence and Bullying | ||||
| 10 | I feel stressed due to psychological abuse such as threats, discrimination, bullying, and harassment. | 2.85 | 0.76 | - |
| Subscale 5: Organizational Issues (Cronbach’s α: 0.59) | ||||
| 11 | The on-call system affects my life. | 2.97 | 0.82 | 0.45 |
| 12 | The organization usually remunerates my overtime work at a low rate of pay. | 2.77 | 0.81 | 0.47 |
| 13 | Not achieving a promotion (e.g., level 1 or 2) within the expected period affects my income. | 3.04 | 0.76 | 0.55 |
| Subscale 6: Occupational Hazards (Cronbach’s α: 0.39) | ||||
| 14 | I feel stressed considering that my patients might be have contagious diseases such as SARS or AIDS. | 3.21 | 0.65 | - |
| 15 | I need to transport patients or equipment. | 3.12 | 0.76 | - |
| Subscale 7: Difficulty Taking Leave (Cronbach’s α: 0.77) | ||||
| 16 | I cannot ask for leaves for household emergencies. | 2.87 | 0.83 | - |
| 17 | I cannot excuse myself for feeling strong discomfort. | 2.60 | 0.84 | - |
| Subscale 8: Powerlessness (Cronbach’s α: 0.35) | ||||
| 18 | It upsets me if patients’ conditions do not improve. | 2.77 | 0.65 | - |
| 19 | I have insufficient time to offer mental health care to patients during working hours. | 3.00 | 0.67 | - |
| Subscale 9: Unmet Basic Physiological Needs (Cronbach’s α: 0.69) | ||||
| 20 | I have no time to fulfill my personal needs (e.g., water consumption and toilet breaks). | 2.81 | 0.75 | - |
| 21 | I cannot take an uninterrupted 30-minute mealtime break. | 3.02 | 0.81 | - |
| Variable | Personal Burnout | Client-Related Burnout | Job Dissatisfaction | Intention to Leave | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Factors | AUC | R2 | Factors | AUC | R2 | Factors | AUC | R2 | Factors | AUC | R2 | |
| 43-item NOSS in 1st year (N = 1781) | 1 2 4 6 7 | 0.79 | 18.81% | 1 2 3 4 7 8 | 0.80 | 18.52% | 1 2 6 7 10 | 0.75 | 14.41% | 1 2 4 5 7 10 | 0.75 | 12.16% |
| 21-item NOSS in 2nd year (N = 2655) | 1 2 4 6 7 | 0.82 | 20.64% | 1 2 3 4 7 8 | 0.77 | 15.67% | 1 2 6 7 9 a | 0.73 | 11.20% | 1 2 4 5 7 9 a | 0.77 | 13.93% |
| 21-item NOSS in 1st year (N = 1781) | 0.81 | 19.93% | 0.79 | 19.13% | 0.76 | 14.73% | 0.75 | 12.87% | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Guo, Y.-L.L.; Lin, L.-C.; Lee, Y.-J.; Hu, P.-Y.; Ho, J.-J.; Shiao, J.S.-C. Development of the Nurses’ Occupational Stressor Scale. Int. J. Environ. Res. Public Health 2020, 17, 649. https://doi.org/10.3390/ijerph17020649
Chen Y-C, Guo Y-LL, Lin L-C, Lee Y-J, Hu P-Y, Ho J-J, Shiao JS-C. Development of the Nurses’ Occupational Stressor Scale. International Journal of Environmental Research and Public Health. 2020; 17(2):649. https://doi.org/10.3390/ijerph17020649
Chicago/Turabian StyleChen, Yi-Chuan, Yue-Liang Leon Guo, Li-Chan Lin, Yu-Ju Lee, Pei-Yi Hu, Jiune-Jye Ho, and Judith Shu-Chu Shiao. 2020. "Development of the Nurses’ Occupational Stressor Scale" International Journal of Environmental Research and Public Health 17, no. 2: 649. https://doi.org/10.3390/ijerph17020649
APA StyleChen, Y. -C., Guo, Y. -L. L., Lin, L. -C., Lee, Y. -J., Hu, P. -Y., Ho, J. -J., & Shiao, J. S. -C. (2020). Development of the Nurses’ Occupational Stressor Scale. International Journal of Environmental Research and Public Health, 17(2), 649. https://doi.org/10.3390/ijerph17020649