Ischemia–Reperfusion Intervention: From Enhancements in Exercise Performance to Accelerated Performance Recovery—A Systematic Review and Meta-Analysis

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
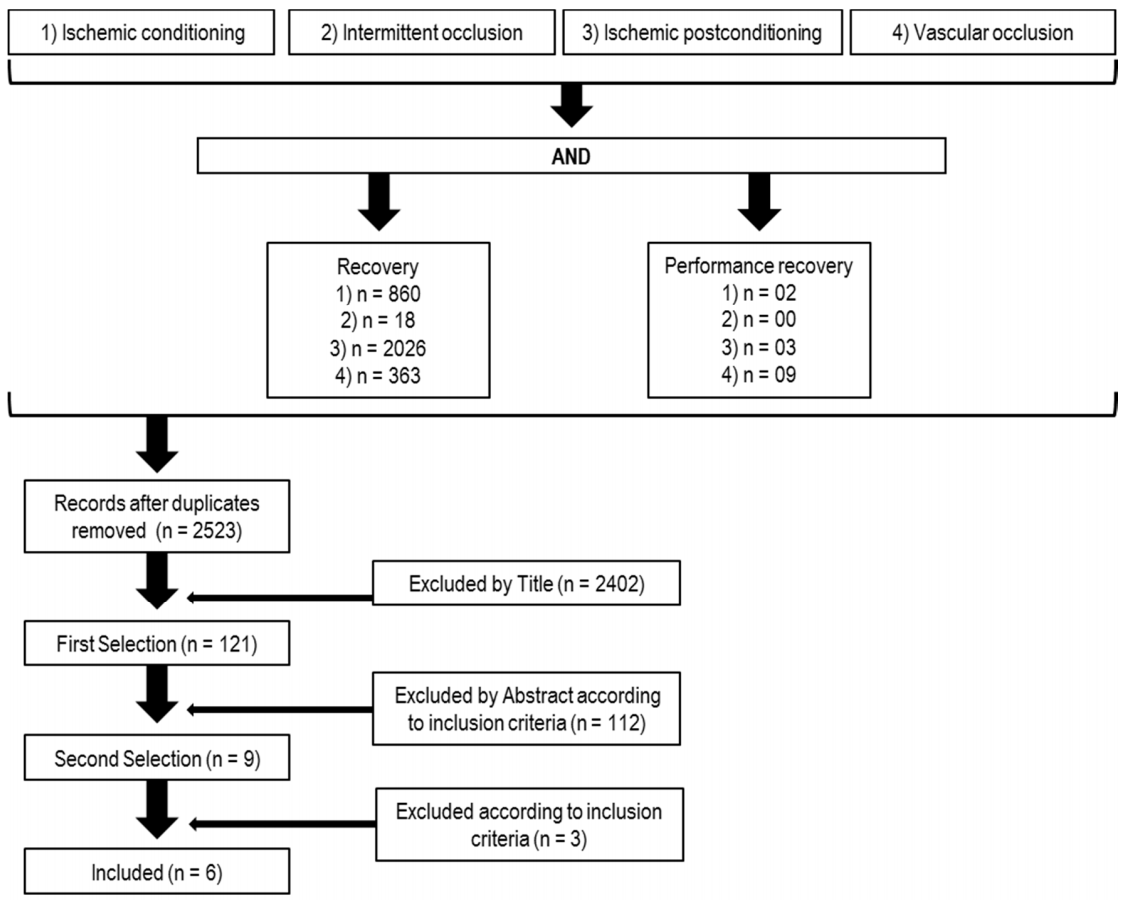
2.1. Database Search
2.2. Study Selection and Quality Assessment
2.3. Data Analysis
3. Results
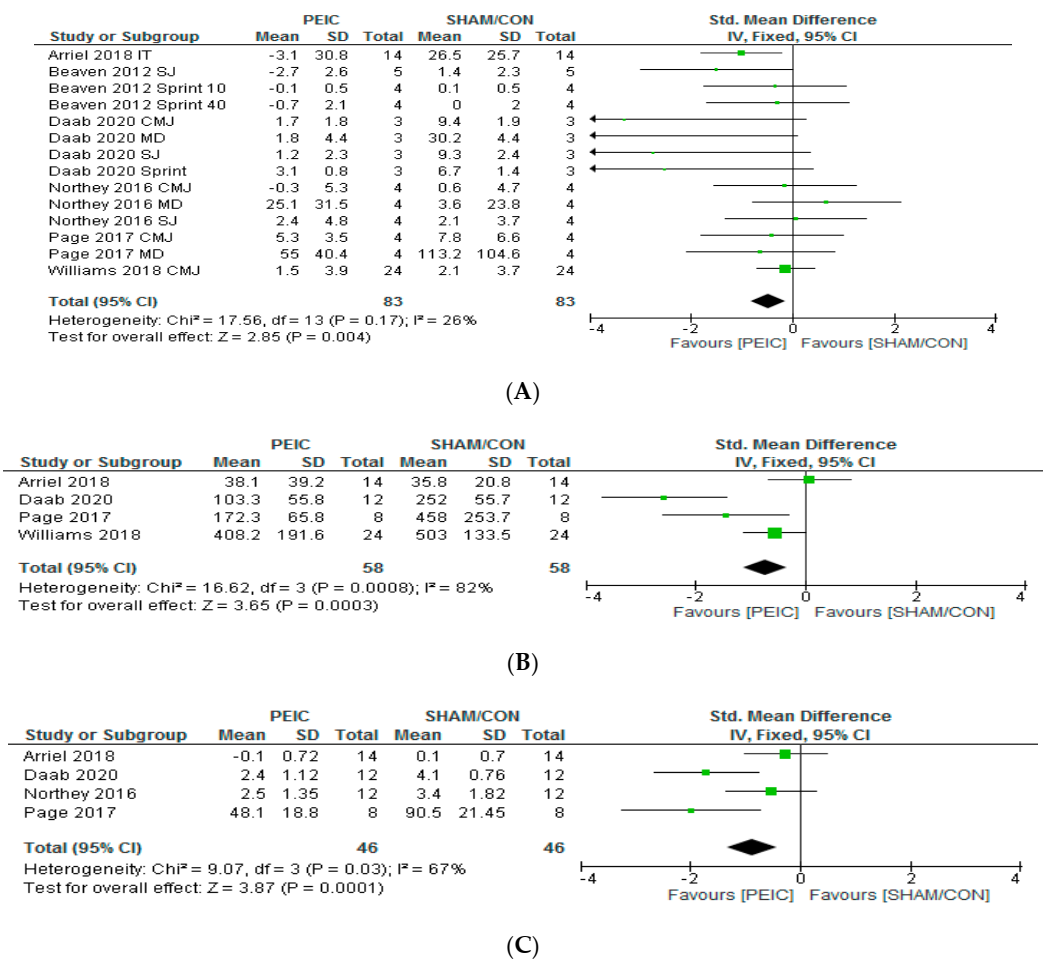
Performance Recovery, Muscle Injury Markers and MS Analysis
4. Discussion
4.1. Quality of the Papers
4.2. Participants Involved
4.3. Exercise Protocols to Induce Fatigue and Assess Performance
4.4. PEIC Effects on Performance Recovery, CK and MS
4.5. PEIC Protocols and Possible Mechanism
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chapman, A.; Vicenzino, B.; Blanch, P.; Hodges, P. Do differences in muscle recruitment between novice and elite cyclists reflect different movement patterns or less skilled muscle recruitment? J. Sci. Med. Sport 2009, 12, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Marroyo, J.A.; Pernía, R.; Villa, J.G.; Foster, C. Reliability and Seasonal Changes of Submaximal Variables to Evaluate Professional Cyclists. Int. J. Sports Physiol. Perform. 2017, 12, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, D.S.; Pearce, E.; Aboud, A.; Gillen, J.B.; Gibala, M.J.; Donato, S.; Waddington, J.M.; Green, J.G.; Tarnopolsky, M.A. Oxidative stress, inflammation, and muscle soreness in an 894-km relay trail run. Eur. J. Appl. Physiol. 2012, 112, 1839–1848. [Google Scholar] [CrossRef] [PubMed]
- Filho, E.; Di Fronso, S.; Forzini, F.; Murgia, M.; Agostini, T.; Bortoli, L.; Robazza, C.; Bertollo, M. Athletic performance and recovery-stress factors in cycling: An ever changing balance. Eur. J. Sport Sci. 2015, 15, 671–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, A. Using recovery modalities between training sessions in elite athletes: Does it help? Sports Med. 2006, 36, 781–796. [Google Scholar] [CrossRef]
- Arriel, R.A.; De Souza, H.L.R.; Da Mota, G.R.; Marocolo, M. Declines in exercise performance are prevented 24 hours after post-exercise ischemic conditioning in amateur cyclists. PLoS ONE 2018, 13, e0207053. [Google Scholar] [CrossRef]
- Page, W.; Swan, R.; Patterson, S.D. The effect of intermittent lower limb occlusion on recovery following exercise-induced muscle damage: A randomized controlled trial. J. Sci. Med. Sport 2017, 20, 729–733. [Google Scholar] [CrossRef]
- Garcia, C.A.; Da Mota, G.R.; Marocolo, M. Cold Water Immersion is Acutely Detrimental but Increases Performance Post-12 h in Rugby Players. Int. J. Sports Med. 2016, 37, 619–624. [Google Scholar] [CrossRef]
- Lanferdini, F.J.; Bini, R.R.; Baroni, B.M.; Klein, K.D.; Carpes, F.P.; Vaz, M.A. Low-Level Laser Therapy Improves Performance and Reduces Fatigue in Competitive Cyclists. Int. J. Sports Physiol. Perform. 2017, 1–27. [Google Scholar] [CrossRef]
- Marocolo, M.; Billaut, F.; Da Mota, G.R. Ischemic Preconditioning and Exercise Performance: An Ergogenic Aid for Whom? Front. Physiol. 2018, 9, 1874. [Google Scholar] [CrossRef] [Green Version]
- Incognito, A.V.; Burr, J.F.; Millar, P.J. The Effects of Ischemic Preconditioning on Human Exercise Performance. Sports Med. Auckl. N. Z. 2016, 46, 531–544. [Google Scholar] [CrossRef] [PubMed]
- Marocolo, M.; Da Mota, G.R.; Simim, M.M.; Appell Coriolano, H.-J. Myths and Facts about the Effects of Ischemic Preconditioning on Performance. Int. J. Sports Med. 2016, 37, 87–96. [Google Scholar] [CrossRef] [Green Version]
- Murry, C.E.; Jennings, R.B.; Reimer, K.A. Preconditioning with ischemia: A delay of lethal cell injury in ischemic myocardium. Circulation 1986, 74, 1124–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.-Q.; Corvera, J.S.; Halkos, M.E.; Kerendi, F.; Wang, N.-P.; Guyton, R.A.; Vinten-Johansen, J. Inhibition of myocardial injury by ischemic postconditioning during reperfusion: Comparison with ischemic preconditioning. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H579–H588. [Google Scholar] [CrossRef]
- Crisafulli, A.; Melis, F.; Tocco, F.; Santoboni, U.M.; Lai, C.; Angioy, G.; Lorrai, L.; Pittau, G.; Concu, A.; Pagliaro, P. Exercise-induced and nitroglycerin-induced myocardial preconditioning improves hemodynamics in patients with angina. Am. J. Physiol. Heart Circ. Physiol. 2004, 287, H235–H242. [Google Scholar] [CrossRef]
- Marongiu, E.; Crisafulli, A. Cardioprotection acquired through exercise: The role of ischemic preconditioning. Curr. Cardiol. Rev. 2014, 10, 336–348. [Google Scholar] [CrossRef] [Green Version]
- Jin, C.; Wu, J.; Watanabe, M.; Okada, T.; Iesaki, T. Mitochondrial K+ channels are involved in ischemic postconditioning in rat hearts. J. Physiol. Sci. 2012, 62, 325–332. [Google Scholar] [CrossRef]
- Libonati, J.R.; Cox, M.; Incanno, N.; Melville, S.K.; Musante, F.C.; Glassberg, H.L.; Guazzi, M. Brief periods of occlusion and reperfusion increase skeletal muscle force output in humans. Cardiologia 1998, 43, 1355–1360. [Google Scholar] [PubMed]
- Jean-St-Michel, E.; Manlhiot, C.; Li, J.; Tropak, M.; Michelsen, M.M.; Schmidt, M.R.; McCrindle, B.W.; Wells, G.D.; Redington, A.N. Remote preconditioning improves maximal performance in highly trained athletes. Med. Sci. Sports Exerc. 2011, 43, 1280–1286. [Google Scholar] [CrossRef] [Green Version]
- Bailey, T.G.; Jones, H.; Gregson, W.; Atkinson, G.; Cable, N.T.; Thijssen, D.H.J. Effect of ischemic preconditioning on lactate accumulation and running performance. Med. Sci. Sports Exerc. 2012, 44, 2084–2089. [Google Scholar] [CrossRef] [Green Version]
- Arriel, R.A.; Meireles, A.; Hohl, R.; Marocolo, M. Ischemic preconditioning improves performance and accelerates the heart rate recovery. J. Sports Med. Phys. Fitness 2020. [CrossRef]
- Burt, D.G.; Twist, C. The effects of exercise-induced muscle damage on cycling time-trial performance. J. Strength Cond. Res. 2011, 25, 2185–2192. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.B. Reactive Oxygen Species as Agents of Fatigue. Med. Sci. Sports Exerc. 2016, 48, 2239–2246. [Google Scholar] [CrossRef]
- Beaven, C.M.; Cook, C.J.; Kilduff, L.; Drawer, S.; Gill, N. Intermittent lower-limb occlusion enhances recovery after strenuous exercise. Appl. Physiol. Nutr. Metab. 2012, 37, 1132–1139. [Google Scholar] [CrossRef] [Green Version]
- De Souza, H.L.R.; Arriel, R.A.; Hohl, R.; Da Mota, G.R.; Marocolo, M. Is Ischemic Preconditioning Intervention Occlusion-Dependent to Enhance Resistance Exercise Performance? Strength Cond. Res. 2019. [CrossRef]
- Tocco, F.; Marongiu, E.; Ghiani, G.; Sanna, I.; Palazzolo, G.; Olla, S.; Pusceddu, M.; Sanna, P.; Corona, F.; Concu, A.; et al. Muscle ischemic preconditioning does not improve performance during self-paced exercise. Int. J. Sports Med. 2015, 36, 9–15. [Google Scholar] [CrossRef]
- Northey, J.M.; Rattray, B.; Argus, C.K.; Etxebarria, N.; Driller, M.W. Vascular Occlusion and Sequential Compression for Recovery After Resistance Exercise. J. Strength Cond. Res. 2016, 30, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.; Russell, M.; Cook, C.J.; Kilduff, L.P. The effect of lower limb occlusion on recovery following sprint exercise in academy rugby players. J. Sci. Med. Sport 2018, 21, 1095–1099. [Google Scholar] [CrossRef] [Green Version]
- Daab, W.; Bouzid, M.A.; Lajri, M.; Bouchiba, M.; Rebai, H. Brief cycles of lower-limb occlusion accelerate recovery kinetics in soccer players. Phys. Sports Med. 2020, 1–8. [Google Scholar] [CrossRef]
- Marocolo, M.; Simim, M.A.M.; Bernardino, A.; Monteiro, I.R.; Patterson, S.D.; Da Mota, G.R. Ischemic preconditioning and exercise performance: Shedding light through smallest worthwhile change. Eur. J. Appl. Physiol. 2019. [CrossRef] [PubMed]
- Batterham, A.M.; Hopkins, W.G. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef]
- Androulakis-Korakakis, P.; Fisher, J.P.; Steele, J. The Minimum Effective Training Dose Required to Increase 1RM Strength in Resistance-Trained Men: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 751–765. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Thompson, D.; Nicholas, C.W.; Williams, C. Muscular soreness following prolonged intermittent high-intensity shuttle running. J. Sports Sci. 1999, 17, 387–395. [Google Scholar] [CrossRef]
- Arriel, R.A.; De Souza, H.L.R.; Da Silva, B.V.C.; Marocolo, M. Ischemic preconditioning delays the time of exhaustion in cycling performance during the early but not in the late phase. Mot. Rev. Educ. Fís. 2019, 25. [Google Scholar] [CrossRef] [Green Version]
- Richard, P.; Billaut, F. Time-Trial Performance in Elite Speed Skaters after Remote Ischemic Preconditioning. Int. J. Sports Physiol. Perform. 2018, 1–9. [Google Scholar] [CrossRef]
- Gathercole, R.J.; Sporer, B.C.; Stellingwerff, T.; Sleivert, G.G. Comparison of the Capacity of Different Jump and Sprint Field Tests to Detect Neuromuscular Fatigue. J. Strength Cond. Res. 2015, 29, 2522–2531. [Google Scholar] [CrossRef]
- Córdova, A.; Sureda, A.; Albina, M.L.; Linares, V.; Bellés, M.; Sánchez, D.J. Oxidative stress markers after a race in professional cyclists. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 171–178. [Google Scholar] [CrossRef]
- Córdova Martínez, A.; Martorell Pons, M.; Sureda Gomila, A.; Tur Marí, J.A.; Pons Biescas, A. Changes in circulating cytokines and markers of muscle damage in elite cyclists during a multi-stage competition. Clin. Physiol. Funct. Imaging 2015, 35, 351–358. [Google Scholar] [CrossRef]
- Halson, S.L.; Bridge, M.W.; Meeusen, R.; Busschaert, B.; Gleeson, M.; Jones, D.A.; Jeukendrup, A.E. Time course of performance changes and fatigue markers during intensified training in trained cyclists. J. Appl. Physiol. 2002, 93, 947–956. [Google Scholar] [CrossRef] [Green Version]
- Dankel, S.J.; Buckner, S.L.; Jessee, M.B.; Mattocks, K.T.; Mouser, J.G.; Counts, B.R.; Laurentino, G.C.; Abe, T.; Loenneke, J.P. Post-exercise blood flow restriction attenuates muscle hypertrophy. Eur. J. Appl. Physiol. 2016, 116, 1955–1963. [Google Scholar] [CrossRef]
- Powers, S.K.; Jackson, M.J. Exercise-induced oxidative stress: Cellular mechanisms and impact on muscle force production. Physiol. Rev. 2008, 88, 1243–1276. [Google Scholar] [CrossRef] [Green Version]
- Raat, N.J.H.; Shiva, S.; Gladwin, M.T. Effects of nitrite on modulating ROS generation following ischemia and reperfusion. Adv. Drug Deliv. Rev. 2009, 61, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.-Y.; Wang, N.-P.; Kerendi, F.; Halkos, M.; Kin, H.; Guyton, R.A.; Vinten-Johansen, J.; Zhao, Z.-Q. Hypoxic postconditioning reduces cardiomyocyte loss by inhibiting ROS generation and intracellular Ca2+ overload. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H1900–H1908. [Google Scholar] [CrossRef] [Green Version]
- Johnsen, J.; Pryds, K.; Salman, R.; Løfgren, B.; Kristiansen, S.B.; Bøtker, H.E. The remote ischemic preconditioning algorithm: Effect of number of cycles, cycle duration and effector organ mass on efficacy of protection. Basic Res. Cardiol. 2016, 111, 10. [Google Scholar] [CrossRef]
- Wang, G.; Li, X.; Wang, H.; Wang, Y.; Zhang, L.; Zhang, L.; Liu, B.; Zhang, M. Later phase cardioprotection of ischemic post-conditioning against ischemia/reperfusion injury depends on iNOS and PI3K-Akt pathway. Am. J. Transl. Res. 2015, 7, 2603–2611. [Google Scholar]
- Powers, S.K.; Ji, L.L.; Kavazis, A.N.; Jackson, M.J. Reactive oxygen species: Impact on skeletal muscle. Compr. Physiol. 2011, 1, 941–969. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Points | |||
|---|---|---|---|
| Reporting | 0 | ½ | 1 |
| 1. Is the hypothesis/aim/objective of the study clearly described? | No | Unclear | Yes |
| 2. Are the main outcomes to be measured clearly described in the Introduction? | No | Unclear | Yes |
| 3. Are the characteristics of the subjects included in the study clearly described? | No | Unclear | Yes |
| 4. Are the interventions of interest clearly described? | No | Unclear | Yes |
| 5. Are the main findings of the study clearly described? | No | Unclear | Yes |
| 6. Does the study provide estimates of the random variability in the data for the main outcomes? | No | Unclear | Yes |
| 7. Were the instruments of testing reliable? | No | Unclear | Yes |
| 8. Was a follow-up duration sufficiently described and consistent within the study? | No | Unclear | Yes |
| 9. Number of participants included in study findings | <5 | 6–15 | >16 |
| Analysis and presentation | |||
| 10. Have actual probability values been reported (e.g., 0.035 rather than <0.05) for the main outcomes except, where the probability value is less than 0.001? | No | Unclear | Yes |
| 11. Was there a statement adequately describing or referencing all statistical procedures used? | No | Unclear | Yes |
| 12. Were the statistical analyses used appropriate? | No | Unclear | Yes |
| 13. Was the presentation of results satisfactory? | No | Unclear | Yes |
| 14. Were confidence intervals given for the main results? | No | Unclear | Yes |
| 15. Was the conclusion drawn from the statistical analysis justified? | No | Unclear | Yes |
| N | Male | Female | Samples | Subjects | (Exercise) Fatigue Protocol | Exercise/Test to Assess Performance | Is PEIC Favorable to Performance? | Other Variables Analyzed | |
|---|---|---|---|---|---|---|---|---|---|
| Beaven et al. (2012) [24] | 14 | 10 | 4 | Paired | Healthy Recreationally trained | Jumps/sprints/leg press test | Jumps/sprints/leg press test | Yes | # |
| Northey et al. (2016) [27] | 12 | 12 | 0 | Paired | Healthy well trained (resistance exercise) | Back Squat (10 sets × 10 repetitions (70% 1RM)) | MVC/Jumps | No | MS and PRS |
| Page et al. (2017) [7] | 16 | 16 | 0 | No Paired | Healthy Recreationally active | Jumps (5 sets × 20 repetitions own body weight (box 0.6 m height)) | MIVC/Jumps | Yes | MS *, CK *, TC |
| Williams et al. (2018) [28] | 24 | 24 | 0 | Paired | Rugby Player (college level) | 6 sets × 50 m sprints | Jumps | No | MS, PRS, CK, lactate, cortisol and testosterone |
| Arriel et al. (2018) [6] | 28 | 28 | 0 | No Paired | Trained cyclists | Maximal Incremental | Maximal Incremental | Yes | MS, PRS, RPE, CK, HR |
| Daab et al. (2020) [29] | 12 | 12 | 0 | Paired | Semi-professional soccer players | Loughborough intermittent shuttle test & | Jumps/Sprint/MVC | Yes | MS *, CK *, LDH *, CRP |
| PEIC Sets | Total PEIC and SHAM Time (min) | Ischemia Pressure (mm Hg) PEIC/SHAM/Limb | Time to Test | Groups | Were Subjects Informed about Effects of PEIC? | |
|---|---|---|---|---|---|---|
| Beaven et al. (2012) [24] | 2 × 3 min | 6 | 220/15/thigh | 5 min–24 h | PEIC/SHAM | No |
| Northey et al. (2016) [27] | 2 × 3 min | 6 | 220/#/thigh | 1–24 h | PEIC/CON | It was not exposed by authors |
| Page et al. (2017) [7] | 3 × 5 min | 15 | 220/20/thigh | 24–48–72 h | PEIC/SHAM | No |
| Williams et al. (2018) [28] | 2 × 3 min | 6 | 171−266/15/thigh | 2–24 h | PEIC/SHAM | Yes |
| Arriel et al. (2018) [6] | 2 × 5 min and 5 × 2 min | 10 and 10 | 50 > SAP/20/thigh | 24 h | PEIC/SHAM | Yes |
| Daab et al. (2020) [29] | 3 × 5 min | 15 | 50 > SAP/20/thigh | 0–24–48–72 h | PEIC/SHAM | It was not exposed by authors |
| KERRYPNX | PEIC | SHAM/CON | |||||
|---|---|---|---|---|---|---|---|
| Exercise | Pre-Intervention | 24-h Post-Intervention | Change (%) | Pre-Intervention | 24-h Post-Intervention | Change (%) | |
| Beaven et al. (2012) [24] | SJea (m.s−2) | 20.1 ± 3.9 | 22.8 ± 4.3 | 13.4 | 18.9 ± 3.7 | 17.5 ± 3.6 | −7.4 |
| S 10 m (s) | 12.5 ± 0.8 | 12.4 ± 0.8 | 0.8 | 12.6 ± 0.7 | 12.7 ± 0.8 | −0.8 | |
| S 40 m (s) | 42.5 ± 3.4 | 41.8 ± 3.3 | 1.7 | 42.7 ± 3.1 | 42.7 ± 3.2 | 0.0 | |
| Northey et al. (2016) [27] | CMJ (cm) | 41.8 ± 8.8 | 42.1 ± 6.9 | 0.7 | 42.7 ± 7.7 | 42.1 ± 7.0 | −1.4 |
| SJ (cm) | 37.7 ± 7.8 | 35.3 ± 7.2 | −6.4 | 38.1 ± 5.6 | 36.0 ± 6.1 | −5.5 | |
| MD (30 deg.s−1) (Nm) | 281.5 ± 46.0 | 256.4 ± 52.0 | −8.9 | 273.7 ± 35.5 | 270.1 ± 39.1 | −1.3 | |
| Page et al. (2017) [7] | CMJ (cm) | 34.0 ± 4.4 | 28.7 ± 1.2 | −15.6 | 38.9 ± 8.1 | 31.1 ± 2.0 | −20.1 |
| MD (N) | 611.0 ± 51.0 | 556.0 ± 67.2 | −9.0 | 629.0 ± 136.0 | 515.8 ± 43.3 | −18.0 | |
| Williams et al. (2018) [28] | CMJ (cm) | 40.4 ± 6.0 | 38.9 ± 6.2 | −3.7 | 39.7 ± 6.0 | 37.6 ± 5.6 | −5.3 |
| Arriel et al. (2018) [6] | IT (s) | 808.3 ± 122.9 | 811.4 ± 135.1 | 0.4 | 779.9 ± 122.9 | 753.4 ± 110.0 | −3.4 |
| Daab et al. (2020) [29] | CMJ (%) | 100.0 ± 0.0 | 98.3 ± 1.8 | −1.7 | 100.0 ± 0.0 | 90.6 ± 1.9 | −9.4 |
| SJ (%) | 100.0 ± 0.0 | 98.8 ± 2.3 | −1.2 | 100.0 ± 0.0 | 90.7 ± 2.4 | −9.3 | |
| MD (%) | 100.0 ± 0.0 | 98.2 ± 4.4 | −1.8 | 100.0 ± 0.0 | 69.8 ± 4.4 | −30.2 | |
| S 20 m (%) | 100.0 ± 0.0 | 103.1 ± 0.8 | −3.1 | 100.0 ± 0.0 | 106.7 ± 1.4 | −6.7 | |
| Mean | −2.5 * | −8.5 | |||||
| PEIC | SHAM/CON | ||||||
|---|---|---|---|---|---|---|---|
| Exercise | Pre-Intervention | 24-h Post-Intervention | Change (%) | Pre-Intervention | 24-h Post-Intervention | Change (%) | |
| Northey et al. (2016) [27] | PRS (scores) | 8.1 ± 1.5 | 5.6 ± 1.6 | −30.9 | 7.9 ± 0.9 | 5.1 ± 1.9 | −35.4 |
| MS (scores) | 0.6 ± 0.8 | 3.1 ± 1.9 | 416.7 | 1.0 ± 0.8 | 4.4 ± 2.4 | 340.0 | |
| Page et al. (2017) [7] | MS (scores) | 8.9 ± 8.0 | 57.0 ± 24.6 | 540.5 | 15.6 ± 12.5 | 106.1 ± 30.1 | 580.1 |
| CK (U/L) | 163.5 ± 30.1 | 335.8 ± 87.3 | 105.4 | 178.4 ± 61.4 | 636.4 ± 300.1 | 256.7 | |
| Williams et al. (2018) [28] | CK (U/L) | 218.9 ± 81.9 | 627.1 ± 250.7 | 186.5 | 228.6 ± 81.9 | 731.6 ± 189.7 | 220.0 |
| Arriel et al. (2018) [6] | PRS (scores) | 8.2 ± 2.2 | 7.2 ± 2.0 | −12.2 | 7.5 ± 2.3 | 7.4 ± 1.7 | −1.3 |
| MS (scores) | 0.8 ± 1.2 | 0.7 ± 0.9 | −12.5 | 0.6 ± 1.1 | 0.7 ± 1.1 | 16.7 | |
| CK (U/L) | 205.9 ± 138.4 | 244.0 ± 160.2 | 18.5 | 192.5 ± 127.6 | 228.3 ± 138.5 | 18.6 | |
| Daab et al. (2020) [29] | MS (scores) | 0.5 ± 0.1 | 2.9 ± 1.2 | 480.0 | 0.6 ± 0.5 | 4.7 ± 1.1 | 683 |
| CK (%) | 100.0 ± 0.0 | 203.3 ± 55.8 | 103.3 | 100.0 ± 0.0 | 352.0 ± 55.7 | 252.0 | |
| Mean | PRS | −21.6 | −18.4 | ||||
| MS | 356.2 | 404.9 | |||||
| CK | 103.4 | 186.8 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arriel, R.A.; Rodrigues, J.F.; Souza, H.L.R.d.; Meireles, A.; Leitão, L.F.M.; Crisafulli, A.; Marocolo, M. Ischemia–Reperfusion Intervention: From Enhancements in Exercise Performance to Accelerated Performance Recovery—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8161. https://doi.org/10.3390/ijerph17218161
Arriel RA, Rodrigues JF, Souza HLRd, Meireles A, Leitão LFM, Crisafulli A, Marocolo M. Ischemia–Reperfusion Intervention: From Enhancements in Exercise Performance to Accelerated Performance Recovery—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(21):8161. https://doi.org/10.3390/ijerph17218161
Chicago/Turabian StyleArriel, Rhaí André, Jéssica Ferreira Rodrigues, Hiago Leandro Rodrigues de Souza, Anderson Meireles, Luís Filipe Moutinho Leitão, Antonio Crisafulli, and Moacir Marocolo. 2020. "Ischemia–Reperfusion Intervention: From Enhancements in Exercise Performance to Accelerated Performance Recovery—A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 21: 8161. https://doi.org/10.3390/ijerph17218161
APA StyleArriel, R. A., Rodrigues, J. F., Souza, H. L. R. d., Meireles, A., Leitão, L. F. M., Crisafulli, A., & Marocolo, M. (2020). Ischemia–Reperfusion Intervention: From Enhancements in Exercise Performance to Accelerated Performance Recovery—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(21), 8161. https://doi.org/10.3390/ijerph17218161