Sleep Disordered Breathing: An Epidemiological Study among Albanian Children and Adolescents



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
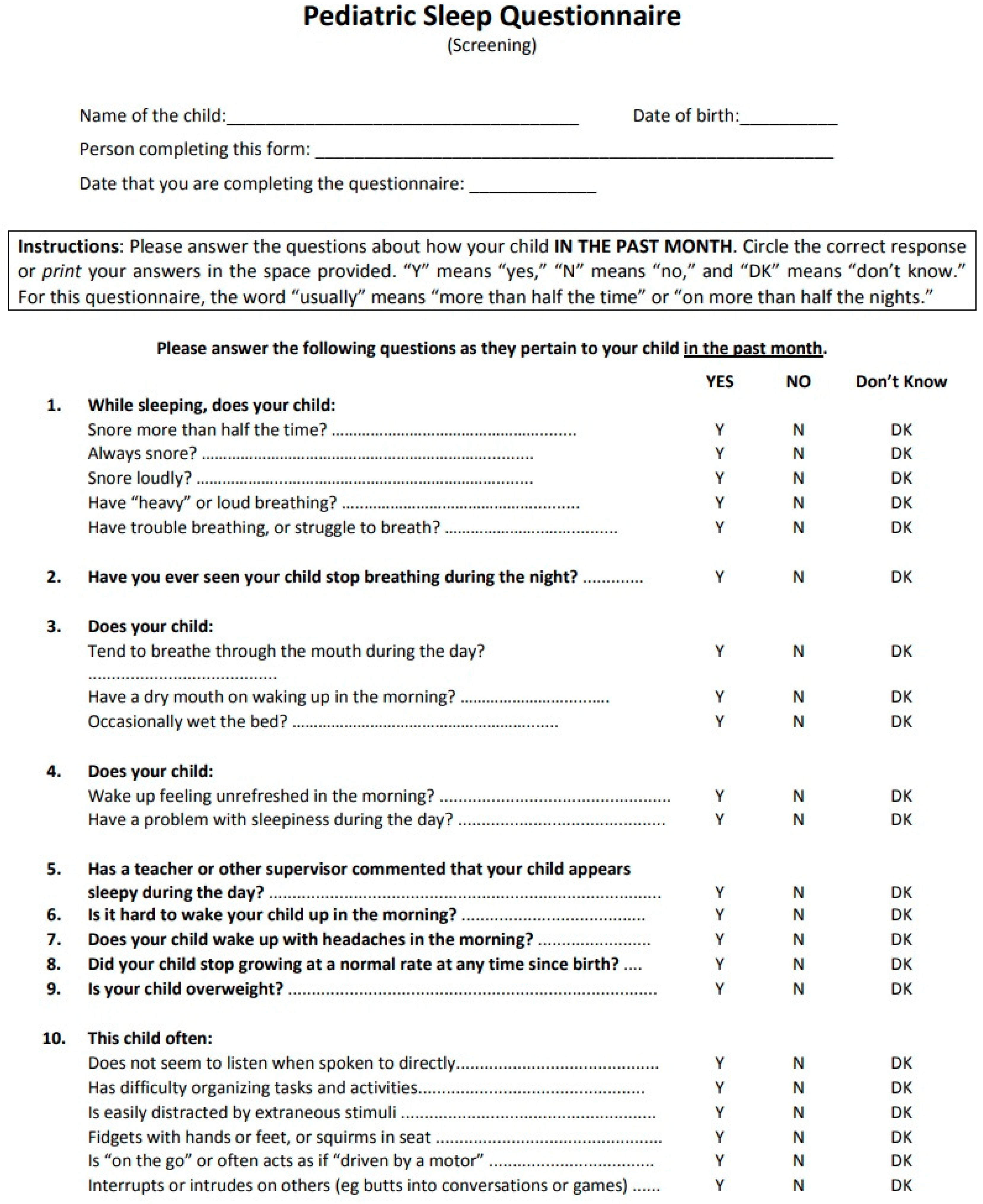
2.2. The Definition of PSQ-SDRB Scale
- 1-
- Forward translation of the questionnaire from English into Albanian by two translators;
- 2-
- Synthesis of the two translations;
- 3-
- Back-translation;
- 4-
- Evaluation by an expert committee;
- 5-
- Pretesting of the penultimate version.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lumeng, J.C.; Chervin, R.D. Epidemiology of pediatric obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 242–252. [Google Scholar] [CrossRef] [Green Version]
- Beebe, D.W.; Gozal, D. Obstructive Sleep Apnea and the prefrontal cortex: Towards a comprehensive model linking nocturnal upper airway obstruction to daytime cognitive and behavioral deficits. J. Sleep Res. 2002, 11, 1–16. [Google Scholar] [CrossRef]
- Smith, D.L.; Gozal, D.; Hunter, S.J.; Philby, M.F.; Kaylegian, J.; Kheirandish-Gozal, L. Impact of sleep disordered breathing on behavior among elementary school-aged children: A cross-sectional analysis of a large community-based sample. Eur. Respir. J. 2016, 48, 1631–1639. [Google Scholar] [CrossRef]
- Chervin, R.D.; Hedger, K.; Dillon, J.E.; Pituch, K.J. Pediatric sleep questionnaire (PSQ): Validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000, 1, 21–32. [Google Scholar] [CrossRef]
- Ischander, M.M.; Lloyd, R.D.L., Jr. Severe paediatric obesity and sleep: A mutual interactive relationship! J. Sleep Res. 2020, e13162. [Google Scholar] [CrossRef]
- Zaffanello, M.; Piacentini, G.; La Grutta, S. The cardiovascular risk in paediatrics: The paradigm of the obstructive sleep apnoea syndrome. Blood Transfus. 2020, 18, 217–225. [Google Scholar]
- Bonuck, K.; Parikh, S.; Bassila, M. Growth failure and sleep disordered breathing: A review of the literature. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 769–778. [Google Scholar] [CrossRef]
- Li, A.M.; So, H.K.; Au, C.T.; Ho, C.; Lau, J.; Ng, S.K.; Abdullah, V.J.; Fok, T.F.; Wing, Y.K. Epidemiology of obstructive sleep apnoea syndrome in Chinese children: A two-phase community study. Thorax 2010, 65, 991–997. [Google Scholar] [CrossRef] [Green Version]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.M.; Liao, D.; Calhoun, S.; Vela-Bueno, A. Sleep disordered breathing in children in a general population sample: Prevalence and risk factors. Sleep 2009, 32, 731–736. [Google Scholar] [CrossRef] [Green Version]
- Spruyt, K.; O’Brien, L.M.; Macmillan Coxon, A.P.; Cluydts, R.; Verleye, G.; Ferri, R. Multidimensional scaling of pediatric sleep breathing problems and bio-behavioral correlates. Sleep Med. 2006, 7, 269–280. [Google Scholar] [CrossRef]
- Archbold, K.H.; Pituch, K.J.; Panahi, P.; Chervin, R.D. Symptoms of sleep disturbances among children at two general pediatric clinics. J. Pediatr. 2002, 140, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Patakaa, A.; Daskalopouloub, E.; Kalamarasa, G.; Passaa, K.F.; Argyropouloua, P. Evaluation of five different questionnaires for assessing sleep Apnea syndrome in a sleep clinic. Sleep Med. 2014, 15, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1246. [Google Scholar] [CrossRef] [Green Version]
- Chervin, R.D.; Weatherly, R.A.; Garetz, S.L.; Ruzicka, D.L.; Giordani, D.L.; Hodges, E.K.; Dillon, J.E.; Guire, K.E. Pediatric Sleep Questionnaire: Prediction of Sleep Apnea and Outcomes. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Abazi, Y.; Tafa, G.J.; Nastasi, E.; Pashaj, E.; Cozza, P. Linguistic validation of Pediatric Sleep Questionnaire (PSQ) for diagnosis of sleep breathing disorders in children. Rev. Stomatol. Shqip. 2018, 17, 48–59. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Institute of Statistics (INSTAT). Available online: http://www.instat.gov.al/al/temat/treguesit-demografikë-dhe-socialë/popullsia/publikimet/2019/popullsia-e-shqipërisë-1-janar-2019 (accessed on 24 September 2019).
- Garcia, J.; Wical, B.; Wical, W.; Schaffer, L.; Wical, T.; Wendorf, H.; Roiko, S. Obstructive sleep apnea in children with cerebral palsy and epilepsy. Dev. Med. Child. Neurol. 2016, 58, 1057–1062. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.F.; Dalesio, N.M.; Benke, J.R.; Petrone, J.A.; Vigilar, V.; Cohen, A.P.; Ishman, S.L. Anthropometric and dental measurements in children with osbtructive sleep apnea. J. Clin. Sleep Med. 2016, 12, 1279–1284. [Google Scholar] [CrossRef] [Green Version]
- Alhammad, N.S.; Hakeem, L.A.; Salama, F.S. Orofacial findings associated with obstructive sleep apnea in a group of Saudi Children. Pak. J. Med Sci. 2015, 31, 388–392. [Google Scholar] [CrossRef]
- Yüksel, H.; Söğüt, A.; Yılmaz, Ö.; Kutluay, E. Reliability and validity of the Turkish version of the pediatric sleep questionnaire: A tool for prediction of sleep related breathing disorder. Tüberküloz Ve Toraks Dergisi. 2011, 59, 236–241. [Google Scholar] [CrossRef]
- Sánchez, T.; Rojas, C.; Casalsb, M.; Bennett, J.T.; Gálvez, C.; Betancur, C.; Mesa, J.T.; Brockmann, P.E. Prevalence and risk factors for sleep-disordered breathing in chilean schoolchildren. Rev. Chilpediatr. 2018, 89, 718–725. [Google Scholar]
- Baidas, L.; Al-Jobair, A.; Al-Kawari, H.; AlShehri, A.; Al-Madani, A.; Al-Balbeesi, H. Prevalence of sleep-disordered breathing and associations with orofacial symptoms among Saudi primary school children. BMC Oral Health 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Brunetti, L.; Rana, S.; Lospalluti, M.L.; Pietrafesa, A.; Francavilla, R.; Fanelli, M.; Armenio, L. Prevalence of obstructive sleep apnea syndrome in a cohort of 1,207 children of southern Italy. Chest 2001, 120, 1930–1935. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.J.; Chae, K.Y. Obstructive sleep apnea syndrome in children: Epidemiology, pathophysiology, diagnosis and sequelae. Korean J. Pediatr. 2010, 53, 863–871. [Google Scholar] [CrossRef]
- Sauer, C.; Schlüter, B.; Hinz, R.; Gesch, D. Childhood obstructive sleep apnea syndrome: An interdisciplinary approach: A prospective epidemiological study of 4,318 five-and-a-half-year-old children. J. Orofacorthop. 2012, 73, 342–358. [Google Scholar] [CrossRef]
- Brockmann, P.E.; Koren, D.; KheirandishGozal, L.; Gozal, D. Gender dimorphism in pediatric OSA: Is it for real? Respir. Physiolneurobiol. 2017, 245, 83–88. [Google Scholar] [CrossRef]
- Redline, S.; Tishler, P.V.; Schluchter, M.; Aylor, J.; Clark, K.; Graham, G. Risk factors for sleep-disordered breathing in children. Associations with obesity, race, and respiratory problems. Am. J. Respir. Crit. Care Med. 1999, 159, 1527–1532. [Google Scholar] [CrossRef]
- Gaines, J.; Vgontzas, A.N.; Fernandez-Mendoza, J.; He, F.; Susan, L.; Liao, D.; Bixler, E.O. Increased inflammation from childhood to adolescence predicts sleep apnea in boys: A preliminary study. BrainBehav. Immun. 2017, 64, 259–265. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Emami, M.; Sadeghi, B.D.; Brand, S. Serum and Plasma Tumor Necrosis Factor Alpha Levels in Individuals with Obstructive Sleep Apnea Syndrome: A Meta-Analysis and Meta-Regression. Life 2020, 10, 87. [Google Scholar] [CrossRef]
- Kuopio Sleep Apnea Group. Sustained improvement in mild obstructive sleep apnea after a diet- and physical activityebased lifestyle intervention: Postinterventional follow-up. Am. J. Clin. Nutr. 2010, 92, 688–696. [Google Scholar] [CrossRef]
- Hakim, F.; Wang, Y.; Carreras, A.; Hirotsu, C.; Zhang, J.; Peris, E.; Gozal, D. Chronic sleep fragmentation during the sleep period induces hypothalamic endoplasmic reticulum stress and PTP1bmediated leptin resistance in male mice. Sleep 2015, 38, 31–40. [Google Scholar] [CrossRef]
- Spiegel, K.; Tasali, E.; Penev, P.; Cauter, E.V. Brief communication: Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Lo Bue, A.; Salvaggio, A.; Insalaco, G. Obstructive sleep apnea in developmental age. A narrative review. Eur. J. Pediatr. 2020, 179, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Kohler, M.J.; Thormaehlen, S.; Kennedy, J.D.; Pamula, Y.; Van den Heuvel, C.J.; Lushington, K.; Martin, A.J. Differences in the Association Between Obesity and Obstructive Sleep Apnea Among Children and Adolescents. J. Clin. Sleep Med. 2009, 5, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Andersen, I.G.; Holm, J.C.; Homøe, P. Establishing a standard definition for child overweight and obesity worldwide: International survey. Int. J. Pediatr. Otorhinolaryngol. 2016, 87, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Laganà, G.; Fabi, F.; Abazi, Y.; Nastasi, E.B.; Vinjolli, F.; Cozza, P. Oral habits in a population of Albanian growing subjects. Eur. J. Paediatr. Dent. 2013, 14, 309–313. [Google Scholar]


{kind=link}
| Internal Consistency of the PSQ | |
|---|---|
| Domain | Cronbach’s Alpha |
| Snoring domain | 0.63 |
| Sleepiness domain | 0.38 |
| Inattention domain | 0.53 |
| Type of Symptom | PSQ Scores | ||||
|---|---|---|---|---|---|
| Total | Snoring | Sleepiness | Inattention | ||
| Symptom Severity | None | 0.13 ± 0.11 | 0.02 ± 0.09 | 0.2 ± 0.25 | 0.23 ± 0.25 |
| Loud snore | 0.35 ± 0.17 | 0.7 ± 0.23 | 0.29 ± 0.27 | 0.33 ± 0.30 | |
| Difficulty breathing | 0.33 ± 0.16 | 0.27 ± 0.34 | 0.29 ± 0.28 | 0.38 ± 0.29 | |
| Apnea during sleep | 0.4 ± 0.18 | 0.32 ± 0.38 | 0.32 ± 0.27 | 0.47 ± 0.31 | |
| p value | <0.00 | <0.00 | <0.00 | <0.00 | |
| Symptom duration | Never | 0.13 ± 0.11 | 0.01 ± 0.07 | 0.2 ± 0.25 | 0.23 ± 0.25 |
| Snore > half of sleep | 0.31 ± 0.15 | 0.57 ± 0.26 | 0.3 ± 0.27 | 0.31 ± 0.27 | |
| Snore throughout sleep | 0.32 ± 0.17 | 0.68 ± 0.26 | 0.26 ± 0.27 | 0.32 ± 0.29 | |
| p value | <0.00 | <0.00 | <0.00 | <0.00 | |
| District | Total Sample | Residence | Sex | Age (in years) | ||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Male | Female | 6–9 | 10–12 | 13–15 | ||
| Elbasani | 24 | 24 | 0 | 5 | 19 | 6 | 5 | 13 |
| Tirana | 1869 | 1388 | 481 | 880 | 989 | 810 | 695 | 364 |
| Durrësi | 829 | 548 | 281 | 392 | 437 | 286 | 350 | 193 |
| Gjirokastra | 172 | 172 | 0 | 82 | 90 | 64 | 63 | 45 |
| Saranda | 171 | 171 | 0 | 76 | 95 | 65 | 88 | 18 |
| Dibra | 264 | 264 | 0 | 138 | 126 | 98 | 100 | 66 |
| Bulqiza | 248 | 248 | 0 | 130 | 118 | 76 | 140 | 32 |
| Shkodra | 526 | 526 | 0 | 263 | 263 | 215 | 206 | 105 |
| Vlora | 339 | 339 | 0 | 154 | 185 | 115 | 130 | 94 |
| Total | 4442 | 3680 | 762 | 2120 | 2322 | 1735 | 1777 | 930 |
| Subjects at Risk of SBD | Gender | Residence Status | ||||
|---|---|---|---|---|---|---|
| No | Yes | Male | Female | Urban | Rural | |
| Number | 4093 | 349 | 2120 | 2322 | 3680 | 762 |
| Prevalence | 92.10% | 7.90% | 8.50% | 7.20% | 7.30% | 10.40% |
| CI * (%) | 7.1 to 8.7% | 7.3 to 9.7% | 6.1 to 8.3% | 6.5 to 8.1% | 8.2 to 12.6% | |
| Age (in years) | Number | Prevalence | CI (%) |
|---|---|---|---|
| 6 | 83 | 8.40% | 2.4 to 14.4% |
| 7 | 445 | 5.60% | 3.5 to 7.7% |
| 8 | 536 | 6.00% | 4.0 to 8.0% |
| 9 | 671 | 7.90% | 5.9 to 9.9% |
| 10 | 557 | 9.00% | 6.6 to 11.4% |
| 11 | 634 | 9.00% | 6.8 to 11.2% |
| 12 | 586 | 7.50% | 5.4 to 9.6% |
| 13 | 425 | 8.50% | 5.8 to 11.2% |
| 14 | 287 | 8.40% | 5.2 to 11.6% |
| 15 | 218 | 9.60% | 5.7 to 13.5% |
| District | Number | Prevalence | CI (%) |
|---|---|---|---|
| Elbasani | 24 | 4.20% | 0 to 12.2% |
| Tirana | 1869 | 8.00% | 6.8 to 9.2% |
| Durrësi | 829 | 7.40% | 5.6 to 9.2% |
| Gjirokastra | 172 | 10.50% | 5.9 to 15.1% |
| Saranda | 171 | 7.00% | 3.2 to 10.8% |
| Dibra | 264 | 7.20% | 4.1 to 10.3% |
| Bulqiza | 248 | 10.90% | 7.0 to 14.8% |
| Shkodra | 526 | 5.90% | 3.9 to 7.9% |
| Vlora | 339 | 9.10% | 6.0 to 12.2% |
| All sample | 4442 | 7.90% | 7.1 to 8.7% |
| BMI ≥ 25 | SBD | ||||
|---|---|---|---|---|---|
| Value | YES | % | No | % | |
| Yes | 400 | 83 | 20.8 | 317 | 79.2 |
| No | 3938 | 250 | 6.3 | 3688 | 93.7 |
| Don’t know | 65 | 12 | 18.4 | 53 | 81.6 |
| No answer | 39 | 6 | 15.3 | 33 | 84.7 |
| Total | 4442 | 351 | 7.9 | 4091 | 92.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abazi, Y.; Cenko, F.; Cardella, M.; Tafa, G.; Laganà, G. Sleep Disordered Breathing: An Epidemiological Study among Albanian Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 8586. https://doi.org/10.3390/ijerph17228586
Abazi Y, Cenko F, Cardella M, Tafa G, Laganà G. Sleep Disordered Breathing: An Epidemiological Study among Albanian Children and Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(22):8586. https://doi.org/10.3390/ijerph17228586
Chicago/Turabian StyleAbazi, Yllka, Fabian Cenko, Marianna Cardella, Gjergji Tafa, and Giuseppina Laganà. 2020. "Sleep Disordered Breathing: An Epidemiological Study among Albanian Children and Adolescents" International Journal of Environmental Research and Public Health 17, no. 22: 8586. https://doi.org/10.3390/ijerph17228586
APA StyleAbazi, Y., Cenko, F., Cardella, M., Tafa, G., & Laganà, G. (2020). Sleep Disordered Breathing: An Epidemiological Study among Albanian Children and Adolescents. International Journal of Environmental Research and Public Health, 17(22), 8586. https://doi.org/10.3390/ijerph17228586