Meta-Analysis on the Effects of Transcranial Direct Current Stimulation on Naming of Elderly with Primary Progressive Aphasia


Abstract
:1. Introduction
2. Methods
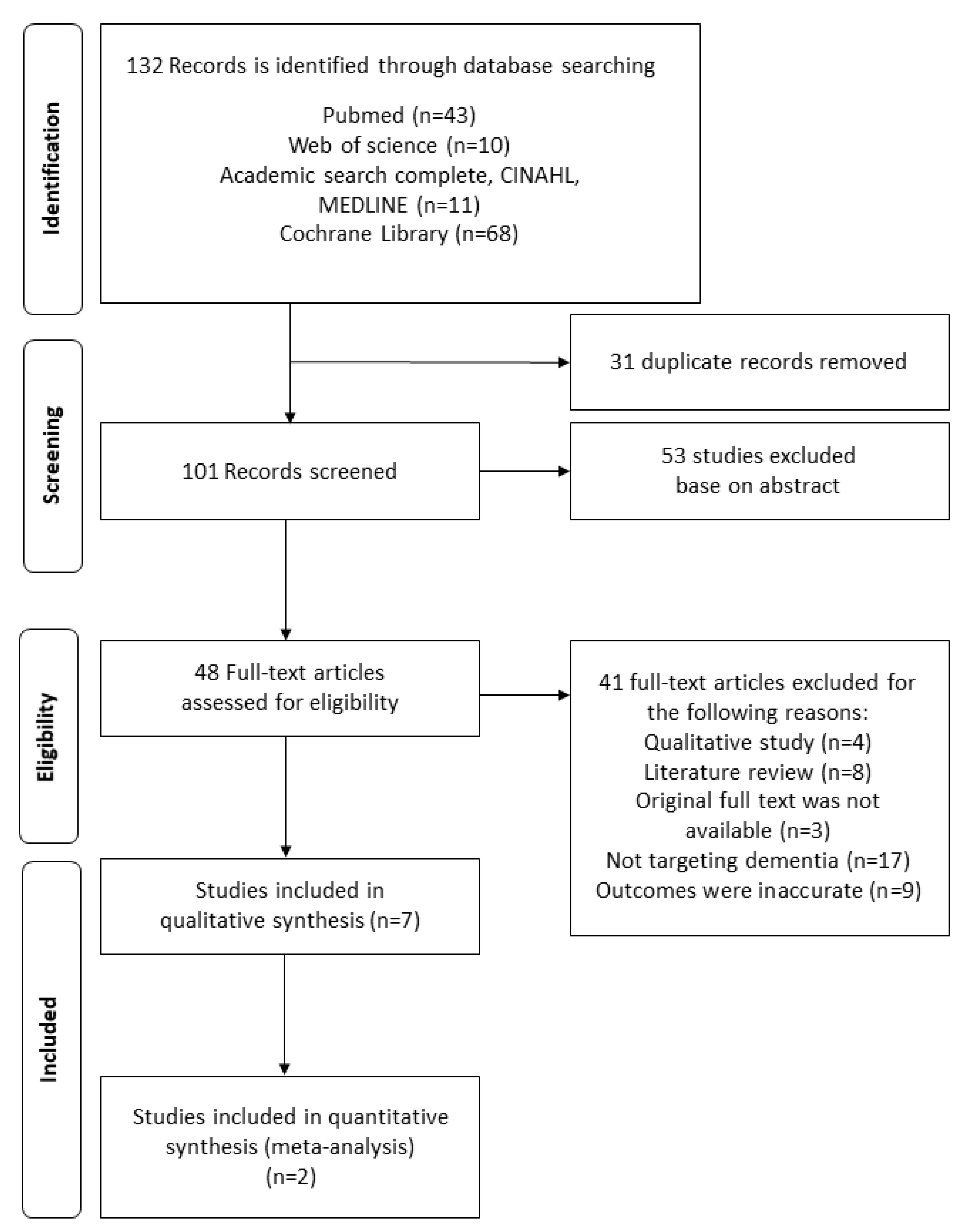
2.1. Literature Search
2.2. Literature Selection
2.3. Quality Assessment
2.4. Meta-Analysis
3. Results
3.1. Quality Assessment Results
3.2. Effects of tDCS on Improving the Naming Ability for PPA
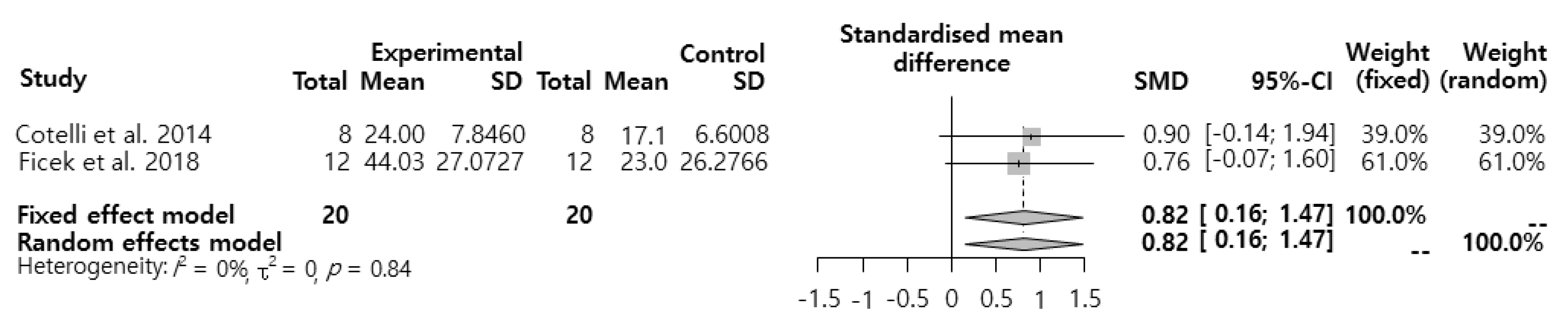
3.3. Meta-analysis for the Effects of tDCS Intervention on the Naming Performance of Patients with PPA
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Laine, M.; Martin, N. Anomia: Theoretical and Clinical Aspects; Psychology Press: Hove, UK, 2006. [Google Scholar]
- Manning, L.; Warrington, E.K. Two routes to naming: A case study. Neuropsychologia 1996, 34, 809–817. [Google Scholar] [CrossRef]
- Glosser, G.; Donofrio, N. Differences between nouns and verbs after anterior temporal lobectomy. Neuropsychology 2001, 15, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Ross, T.P. The reliability of cluster and switch scores for the Controlled Oral Word Association Test. Arch. Clin. Neuropsychol. 2003, 18, 153–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laws, K.R.; Adlington, R.L.; Gale, T.M.; Moreno-Martínez, F.J.; Sartori, G. A meta-analytic review of category naming in Alzheimer’s disease. Neuropsychologia 2007, 45, 2674–2682. [Google Scholar] [CrossRef] [PubMed]
- Klumpp, H.; Deldin, P. Review of brain functioning in depression for semantic processing and verbal fluency. Int. J. Psychophysiol. 2010, 75, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Coppens, P. Aphasia and Related Neurogenic Communication Disorders; Jones & Bartlett Publishers: Burlington, VT, USA, 2016. [Google Scholar]
- Jokel, R.; Graham, N.L.; Rochon, E.; Leonard, C. Word retrieval therapies in primary progressive aphasia. Aphasiology 2014, 28, 1038–1068. [Google Scholar] [CrossRef]
- Tak, S.; Hong, S.H. Face-name memory in Alzheimer’s disease. Geriatr. Nurs. 2014, 35, 290–394. [Google Scholar] [CrossRef]
- Hodges, J.R.; Erzinçlioğlu, S.; Patterson, K. Evolution of cognitive deficits and conversion to dementia in patients with mild cognitive impairment: A very-long-term follow-up study. Dement. Geriatr. Cogn. Disord. 2006, 21, 380–391. [Google Scholar] [CrossRef]
- Vogel, A.; Gade, A.; Stokholm, J.; Waldemar, G. Semantic memory impairment in the earliest phases of Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2005, 19, 75–81. [Google Scholar] [CrossRef]
- Crinion, J.T. Transcranial direct current stimulation as a novel method for enhancing aphasia treatment effects. Eur. Psychol. 2016, 21, 65–77. [Google Scholar] [CrossRef]
- Helm-Estabrooks, N.; Albert, M.L. Manual of Aphasia and Aphasia Therapy; Pro-Ed Publishing: Austin, TX, USA, 2004. [Google Scholar]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of transcranial direct current stimulation: Evidence based update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, M.T.; Kasschau, M.; Dobbs, B.; Pawlak, N.; Pau, W.; Sherman, K.; Bikson, M.; Datta, A.; Charvet, L.E. Remotely supervised transcranial direct current stimulation: An update on safety and tolerability. J. Vis. Exp. 2017, 128, e56211. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L.; Koslowsky, M.; Lavidor, M. tDCS polarity effects in motor and cognitive domains: A meta-analytical review. Exp. Brain. Res. 2012, 216, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Shiozawa, P.; Fregni, F.; Benseñor, I.M.; Lotufo, P.A.; Berlim, M.T.; Daskalakis, J.Z.; Cordeiro, Q.; Brunoni, A.R. Transcranial direct current stimulation for major depression: An updated systematic review and meta-analysis. Int. J. Neuropsychopharmacol. 2014, 17, 1443–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsner, B.; Kugler, J.; Pohl, M.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving aphasia in patients with aphasia after stroke. Cochrane Database Syst. Rev. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Horvath, J.C.; Forte, J.D.; Carter, O. Quantitative review finds no evidence of cognitive effects in healthy populations from single-session transcranial direct current stimulation (tDCS). Brain Stimul. 2015, 8, 535–550. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Kmet, L.M.; Lee, R.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2004. [Google Scholar]
- Lee, L.; Packer, T.L.; Tang, S.H.; Girdler, S. Self-management education programs for age-related macular degeneration: A systematic review. Australas. J. Ageing 2008, 27, 170–176. [Google Scholar] [CrossRef]
- Hung, J.; Bauer, A.; Grossman, M.; Hamilton, R.H.; Coslett, H.B.; Reilly, J. Semantic feature training in combination with transcranial direct current stimulation (tDCS) for progressive anomia. Front. Hum. Neurosci. 2017, 11, 253. [Google Scholar] [CrossRef] [Green Version]
- Cotelli, M.; Manenti, R.; Petesi, M.; Brambilla, M.; Cosseddu, M.; Zanetti, O.; Miniussi, C.; Padovani, A.; Borroni, B. Treatment of primary progressive aphasias by transcranial direct current stimulation combined with language training. J. Alzheimers Dis. 2014, 39, 799–808. [Google Scholar] [CrossRef]
- Ficek, B.N.; Wang, Z.; Zhao, Y.; Webster, K.T.; Desmond, J.E.; Hillis, A.E.; Frangakis, C.; Vasconcellos Faria, A.; Caffo, B.; Tsapkini, K. The effect of tDCS on functional connectivity in primary progressive aphasia. Neuroimage Clin. 2018, 19, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Tsapkini, K.; Webster, K.T.; Ficek, B.N.; Desmond, J.E.; Onyike, C.U.; Rapp, B.; Frangakis, C.E.; Hillis, A.E. Electrical brain stimulation in different variants of primary progressive aphasia: A randomized clinical trial. Alzheimers Dement. 2018, 4, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Tsapkini, K.; Frangakis, C.; Gomez, Y.; Davis, C.; Hillis, A.E. Augmentation of spelling therapy with transcranial direct current stimulation in primary progressive aphasia: Preliminary results and challenges. Aphasiology 2014, 28, 1112–1130. [Google Scholar] [CrossRef] [Green Version]
- McConathey, E.M.; White, N.C.; Gervits, F.; Ash, S.; Coslett, H.; Grossman, M.; Hamilton, R.H. Baseline performance predicts tDCS-mediated improvements in language symptoms in primary progressive aphasia. Front. Hum. Neurosci. 2017, 11, 347. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wu, D.; Chen, Y.; Yuan, Y.; Zhang, M. Effects of transcranial direct current stimulation on language improvement and cortical activation in nonfluent variant primary progressive aphasia. Neurosci. Lett. 2013, 549, 29–33. [Google Scholar] [CrossRef]
- Rohrer, J.D.; Knight, W.D.; Warren, J.E.; Fox, N.C.; Rossor, M.N.; Warren, J.D. Word-finding difficulty: A clinical analysis of the progressive aphasias. Brain 2008, 131, 8–38. [Google Scholar] [CrossRef] [Green Version]
- Hardiman, O.; Doherty, C.P.; Elamin, M.; Bede, P. Neurodegenerative Disorders; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Budd, M.A.; Kortte, K.; Cloutman, L.; Newhart, M.; Gottesman, R.F.; Davis, C.; Heidler-Gary, J.; Seay, M.W.; Hillis, A.E. The nature of naming errors in primary progressive aphasia versus acute post-stroke aphasia. Neuropsychology 2010, 24, 581–589. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, L.F.; de Souza, I.C.; Vidor, L.P.; de Souza, A.; Deitos, A.; Volz, M.S.; Fregni, F.; Caumo, W.; Torres, I.L. Neurobiological effects of transcranial direct current stimulation: A review. Front. Psychiatry 2012, 3, 110. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Lee, J. Application of transcranial direct current stimulation in psychiatry. J. Korean Neuropsychiatr. Assoc. 2016, 55, 158–167. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Criteria | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | ||||||||||||||||
| Wang, et al. 2013 [29] | + | + | ± | + | N/A | N/A | N/A | + | − | − | + | ± | ± | + | 15 | |
| Cotelli, et al. 2014b [24] | + | + | + | + | ± | + | + | + | ± | + | + | + | + | + | 26 | |
| Tsapkini, et al. 2014 [27] | + | + | ± | + | ± | − | + | + | ± | + | + | ± | + | + | 22 | |
| Hung, et al. 2017 [23] | + | + | ± | + | − | N/A | N/A | + | ± | + | ± | ± | + | + | 18 | |
| McConathey, et al. 2017 [28] | + | + | + | + | ± | − | + | + | ± | + | + | + | + | + | 24 | |
| Ficek, et al. 2018 [25] | + | + | ± | + | ± | + | + | + | + | + | + | ± | + | + | 25 | |
| Tsapkini, et al. 2018 [26] | + | + | ± | ± | ± | + | + | + | ± | ± | + | ± | + | + | 22 | |
| Study and Design | Participants | Intervention | Assessment | Outcomes | |||
|---|---|---|---|---|---|---|---|
| Stimulated Region | tDCS | Sham tDCS | Session | ||||
| Ficek et al. (2018) [25] Blinding & Crossover & RCT Design | PPA (n = 24) tDCS (n = 12) : age = 65.2 ± 7.0 Sham (n = 12) : age = 69.1 ± 5.6 | Left inferior frontal gyrus | Anodal 2 mA 20 min | 30 s | 15 sessions (daily) | Letter accuracy (Written naming) | Both tDCS and sham groups improved the letter accuracy of trained words |
| Hung et al. (2017) [23] pre-post design | PPA (n = 4) & AD (n = 1) : age = 66.6±8.56) | Left temporoparietal region | Anodal 1.5 mA 20 min | 30 s | 10 sessions (2 weeks) | Naming : six semantic items (trained and untrained items) | After tDCS intervention, trained items were maintain longer than untrained items. |
| Cotelli et al. (2014b) [24] Blinding & RCT design | PPA (n = 16) AtDCS (n = 8) : age = 63.4 ± 6.8 Placebo tDCS (n = 8) : age = 70.4 ± 6.8 | Left dorsolateral prefrontal cortex | Anodal 2 mA 25 min | 10 s | 10 sessions (2 weeks) | Languistic abilities : Aachen Aphasia Tes (AAT) | Naming accuracy of the AtDCS group increased selectively during the pre–after intervention period. |
| McConathey et al. (2017) [28] Blinding & Crossover & RCT design | PPA (n = 15) : age = 68.71 ± 6.97 tDCS (n = 7, analysis n = 4), Sham (n = 8, analysis n = 3) | Left prefrontal region | Anodal 1.5 mA 20 min | 30 s | 10 sessions (2 weeks) | Sementic process : BNT, PPT, Category Fluency tests | Those with lower base scores have improved significantly since the actual tDCS compared to those with higher base scores. |
| Wang et al. (2013) [29] A1-B1-A2-B2 | PPA (n = 1) : age = 67 | Left posterior perisylvian region, left Broca’s area | B1–B2 Anodal 1.2 mA 20 min | A1–A2 30 s | 5 days (A1–A2) 5 days (B1–B2) | Psycolinguistic Assessment in Chinese Aphasia (PACA) | After the B1 intervention, the scores of the four PACA sub items increased significantly. |
| Tsapkini et al. (2014) [27] Blinding & Crossover & RCT design | PPA(n = 6) | Left inferior frontal gyrus | 1–2 mA 20 min | 30 s | 15 sessions | Number of correctly spelled word-prompts associated with each phoneme | Significant improvement has been maintained through the follow-up period under the tDCS. |
| Tsapkini et al. (2018) [26] Blinding & Crossover & RCT | PPA (n = 36) 1. tDCS (n = 20, crossover n = 15) 2. Sham (n = 16, crossover n = 15) | Left inferior frontal gyrus | 2 mA 20 min | 30 s | 15 sessions (5 sessions per week) | Letter accuracy : trained & untrained items | Trained items were significantly improved immediately after tDCS intervention. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byeon, H. Meta-Analysis on the Effects of Transcranial Direct Current Stimulation on Naming of Elderly with Primary Progressive Aphasia. Int. J. Environ. Res. Public Health 2020, 17, 1095. https://doi.org/10.3390/ijerph17031095
Byeon H. Meta-Analysis on the Effects of Transcranial Direct Current Stimulation on Naming of Elderly with Primary Progressive Aphasia. International Journal of Environmental Research and Public Health. 2020; 17(3):1095. https://doi.org/10.3390/ijerph17031095
Chicago/Turabian StyleByeon, Haewon. 2020. "Meta-Analysis on the Effects of Transcranial Direct Current Stimulation on Naming of Elderly with Primary Progressive Aphasia" International Journal of Environmental Research and Public Health 17, no. 3: 1095. https://doi.org/10.3390/ijerph17031095
APA StyleByeon, H. (2020). Meta-Analysis on the Effects of Transcranial Direct Current Stimulation on Naming of Elderly with Primary Progressive Aphasia. International Journal of Environmental Research and Public Health, 17(3), 1095. https://doi.org/10.3390/ijerph17031095