Is the Random Forest Algorithm Suitable for Predicting Parkinson’s Disease with Mild Cognitive Impairment out of Parkinson’s Disease with Normal Cognition?


Abstract
:1. Introduction
2. Methods
2.1. Data Source
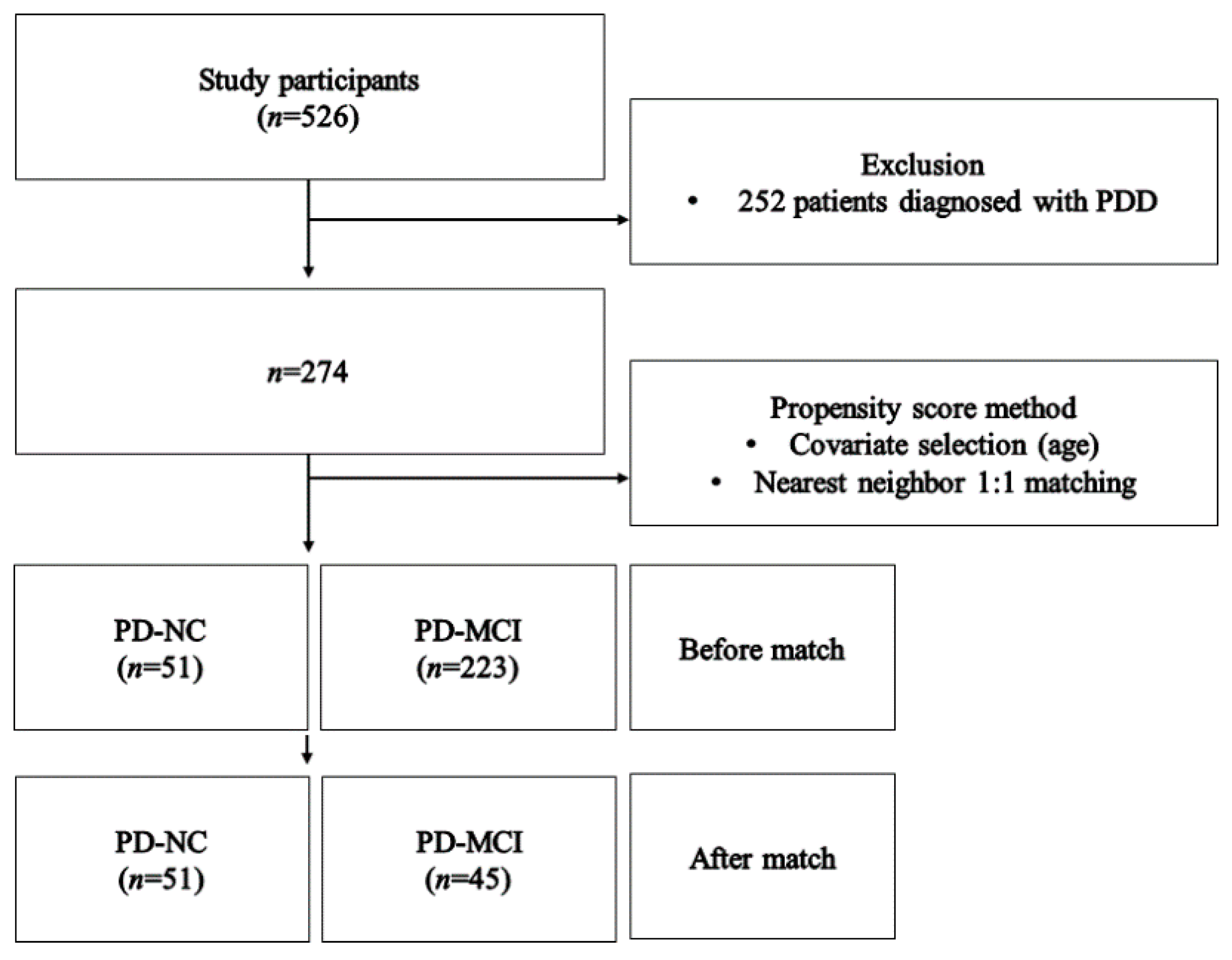
2.2. Subjects
2.3. Measurement
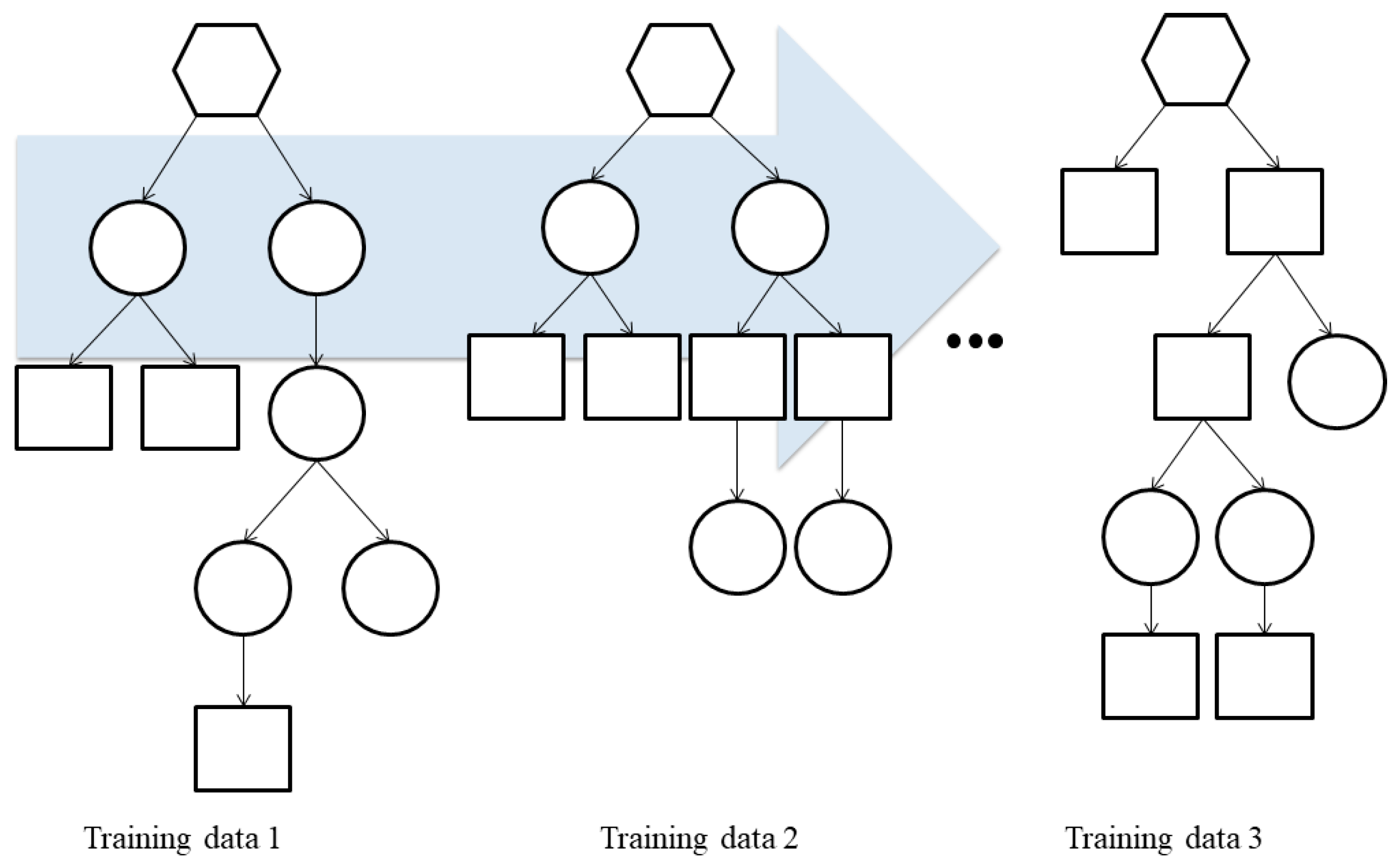
2.4. Development and Evaluation of Prediction Models
3. Results
3.1. General Characteristics of the Subjects
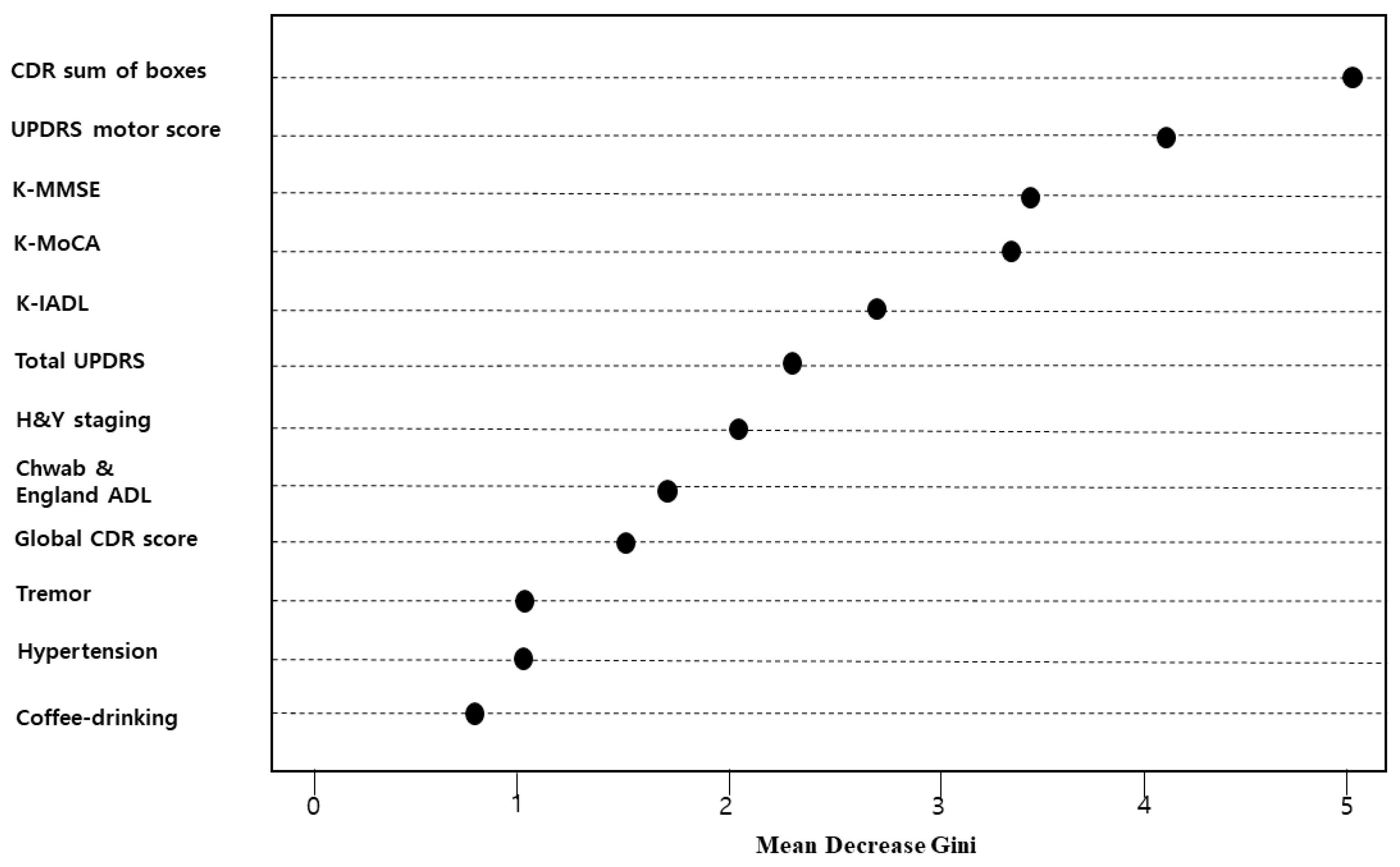
3.2. Major Risk Factors of Random Forest-Based PD-MCI Prediction Model
3.3. Comparison of the Accuracy of the Developed Prediction Models
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Broeders, M.; De Bie, R.M.A.; Velseboer, D.C.; Speelman, J.D.; Muslimovic, D.; Schmand, B. Evolution of mild cognitive impairment in Parkinson disease. Neurology 2013, 81, 346–352. [Google Scholar] [CrossRef]
- Goldman, J.G.; Aggarwal, N.T.; Schroeder, C.D. Mild cognitive impairment: An update in Parkinson’s disease and lessons learned from Alzheimer’s disease. Neurodegener. Dis. Manag. 2015, 5, 425–443. [Google Scholar] [CrossRef]
- Ciafone, J.; Little, B.; Thomas, A.J.; Gallagher, P. The Neuropsychological Profile of Mild Cognitive Impairment in Lewy Body Dementias. J. Int. Neuropsychol. Soc. 2020, 26, 210–225. [Google Scholar] [CrossRef]
- Nicoletti, A.; Luca, A.; Baschi, R.; Cicero, C.E.; Mostile, G.; Davì, M.; Pilati, L.; Restivo, V.; Zappia, M.; Monastero, R. Incidence of Mild Cognitive Impairment and Dementia in Parkinson’s Disease: The Parkinson’s Disease Cognitive Impairment Study. Front. Aging. Neurosci. 2019, 11, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hely, M.A.; Reid, W.G.; Adena, M.A.; Halliday, G.M.; Morris, J.G. The Sydney multicenter study of Parkinson’s disease: The inevitability of dementia at 20 years. Mov. Disord. 2008, 23, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Byeon, H. A prediction model for mild cognitive impairment using random forests. IJACSA 2015, 6, 8–12. [Google Scholar] [CrossRef]
- Geda, Y.E.; Roberts, R.O.; Knopman, D.S.; Petersen, R.C.; Christianson, T.J.; Pankratz, V.S.; Smith, G.E.; Boeve, B.F.; Ivnik, R.J.; Tangalos, E.G.; et al. Prevalence of neuropsychiatric symptoms in mild cognitive impairment and normal cognitive aging: Population-based study. Arch. Gen. Psychiatry 2008, 65, 1193–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langa, K.M.; Levine, D.A. The diagnosis and management of mild cognitive impairment: A clinical review. JAMA 2014, 312, 2551–2561. [Google Scholar] [CrossRef]
- Bott, N.T.; Johnson, E.T.; Schuff, N.; Galifianakis, N.; Subas, T.; Pollock, J.; Pressman, P.; Kramer, J.H.; Possin, K.L. Sensitive measures of executive dysfunction in non-demented Parkinson’s disease. Parkinsonism Relat. Disord. 2014, 20, 1430–1433. [Google Scholar] [CrossRef] [Green Version]
- Sudo, F.K.; Alves, C.E.O.; Alves, G.S.; Ericeira-Valente, L.; Tiel, C.; Moreira, D.M.; Laks, J.; Engelhardt, E. White matter hyperintensities, executive function and global cognitive performance in vascular mild cognitive impairment. Arq. Neuropsiquiatr. 2013, 71, 431–436. [Google Scholar] [CrossRef]
- Petersen, R.C. Early diagnosis of Alzheimer’s disease: Is MCI too late? Curr. Alzheimer. Res. 2009, 6, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Gabryelewicz, T.; Styczynska, M.; Luczywek, E.; Barczak, A.; Pfeffer, A.; Androsiuk, W.; Chodakowska-Zebrowska, M.; Wasiak, B.; Peplonska, B.; Barcikowska, M. The rate of conversion of mild cognitive impairment to dementia: Predictive role of depression. Int. J. Geriatr. Psychiatry 2007, 22, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Lang, M.; Rosselli, M.; Greig, M.T.; Torres, V.L.; Vélez-Uribe, I.; Arruda, F.; Barker, W.W.; Garcia, P.; Loewenstein, D.A.; Curiel, R.E.; et al. Depression and the Diagnosis of MCI in a Culturally Diverse Sample in the United States. Arch. Clin. Neuropsychol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.B.; Kwon, D.Y.; Lee, J.M.; Han, J.K.; Kim, B.J.; Park, M.K.; Park, K.W.; Lee, D.H. Prevalence of Parkinsonism in Ansan-city. J. Korean Neurol. Assoc. 2003, 21, 498–501. [Google Scholar]
- Kim, H.M.; Nazor, C.; Zabetian, C.P.; Quinn, J.F.; Chung, K.A.; Hiller, A.L.; Shu, CH.; Leverenz, J.B.; Montine, T.J.; Edwards, K.L.; et al. Prediction of cognitive progression in Parkinson’s disease using three cognitive screening measures. Clin. Parkinsonism Relat. Disord. 2019, 1, 91–97. [Google Scholar] [CrossRef]
- Barnish, M.; Daley, D.J.; Deane, K.H.; Clark, A.B.; Gray, R.J.; Horton, S.M.; Butterfint, Z.R.; Myint, P.K. Cognitive profile and determinants of poor cognition in people without dementia in Parkinson’s disease. Med. J. Islam. Repub. Iran 2019, 33, 1. [Google Scholar]
- Byeon, H. Predicting the Swallow-Related Quality of Life of the Elderly Living in a Local Community Using Support Vector Machine. Int. J. Environ. Res. Public Health 2019, 16, 4269. [Google Scholar] [CrossRef] [Green Version]
- Joloudari, J.H.; Hassannataj Joloudari, E.; Saadatfar, H.; GhasemiGol, M.; Razavi, S.M.; Mosavi, A.; Nabipour, N.; Shamshirband, S.; Nadai, L. Coronary Artery Disease Diagnosis; Ranking the Significant Features Using a Random Trees Model. Int. J. Environ. Res. Public Health 2020, 17, 731. [Google Scholar] [CrossRef] [Green Version]
- Byeon, H. Development of Depression Prediction Models for Caregivers of Patients with Dementia Using Decision Tree Learning Algorithm. Int. J. Gerontol. 2019, 13, 314–319. [Google Scholar]
- Chen, J.; Li, Q.; Wang, H.; Deng, M. A machine learning ensemble approach based on random forest and radial basis function neural network for risk evaluation of regional flood disaster: A case study of the Yangtze River Delta, China. Int. J. Environ. Res. Public Health 2020, 17, 49. [Google Scholar] [CrossRef] [Green Version]
- Byeon, H. Developing a random forest classifier for predicting the depression and managing the health of caregivers supporting patients with Alzheimer’s Disease. Technol. Health Care 2019, 27, 531–544. [Google Scholar] [CrossRef] [PubMed]
- Byeon, H.; Jin, H.; Cho, S. Development of Parkinson’s disease dementia prediction model based on verbal memory, visuospatial memory, and executive function. J. Med. Imaging Health Inform. 2017, 7, 1517–1521. [Google Scholar] [CrossRef]
- Zhang, J.; Sokal, I.; Peskind, E.R.; Quinn, J.F.; Jankovic, J.; Kenney, C.; Chung, K.A.; Millard, S.P.; Nutt, J.G.; Montine, T.J. CSF multianalyte profile distinguishes Alzheimer and Parkinson diseases. Am. J. Clin. Pathol. 2008, 129, 526–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, M.; Hatz, F.; Gschwandtner, U.; Bogaarts, J.G.; Meyer, A.; Fuhr, P.; Roth, V. Quantitative EEG (QEEG) measures differentiate Parkinson’s disease (PD) patients from healthy controls (HC). Front. Aging Neurosci. 2017, 9, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, M.; Bogaarts, J.; Hatz, F.; Gschwandtner, U.; Cozac, V.; Meyer, A.; Liepelt, I.; Babiloni, C.; Fuhr, P.; Roth, V. Distinguishing Parkinson’s Disease Dementia (PDD) patients from Parkinson’s Disease (PD) patients using EEG frequency and connectivity measures. Clin. Neurophysiol. 2018, 129, e92. [Google Scholar] [CrossRef]
- Lee, J.E.; Kim, J.H.; Hong, E.J.; Yoo, H.S.; Nam, H.Y.; Park, O. National Biobank of Korea: Quality control programs of collected-human biospecimens. Osong. Public Health Res. Perspect. 2012, 3, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment--beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Byeon, H. The risk factors of laryngeal pathology in Korean adults using a decision tree model. J. Voice 2015, 29, 59–64. [Google Scholar] [CrossRef]
- Ghavami, P. Big Data Analytics Methods: Analytics Techniques in Data Mining, Deep Learning and Natural Language Processing; Walter de Gruyter: Berlin, Germany, 2019. [Google Scholar]
- Zhang, Z.; Kim, H.J.; Lonjon, G.; Zhu, Y. Balance diagnostics after propensity score matching. Ann. Transl. Med. 2019, 7, 16. [Google Scholar] [CrossRef]
- Kang, Y.; Na, D.L.; Hahn, S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300. [Google Scholar]
- Kang, Y.; Park, J.; Yu, K.H.; Lee, B.C. The validity of the Korean-Montreal Cognitive Assessment (K-MoCA) as a screening test for both MCI and VCI. In Proceedings of the 20th Annual Rotman Research Institute Conference, Toronto, ON, Canada, 22–26 March 2010. [Google Scholar] [CrossRef]
- Cho, M.J.; Bae, J.N.; Suh, G.H.; Hahm, B.J.; Kim, J.K.; Lee, D.W.; Kang, M.H. Validation of geriatric depression scale, Korean version (GDS) in the assessment of DSM-III-R major depression. J. Korean Neuropsychiatr. Assoc. 1999, 38, 48–63. [Google Scholar]
- Choi, S.H.; Na, D.L.; Lee, B.H.; Hahm, D.S.; Jeong, J.H.; Yoon, S.J.; Yoo, K.H.; Ha, C.K.; Han, I.W. Estimating the validity of the Korean version of expanded clinical dementia rating (CDR) scale. J. Korean Neurol. Assoc. 2001, 19, 585–591. [Google Scholar]
- Kang, S.J.; Choi, S.H.; Lee, B.H.; Kwon, J.C.; Na, D.L.; Han, S.H. The reliability and validity of the Korean Instrumental Activities of Daily Living (K-IADL). J. Korean Neurol. Assoc. 2002, 20, 8–14. [Google Scholar]
- Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. The unified Parkinson’s disease rating scale (UPDRS): Status and recommendations. Mov. Disord. 2003, 18, 738–750. [Google Scholar] [CrossRef] [PubMed]
- Richards, M.; Marder, K.; Cote, L.; Mayeux, R. Interrater reliability of the Unified Parkinson’s Disease Rating Scale motor examination. Mov. Disord. 1994, 9, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Gillingham, F.J.; Donaldson, M.C. Schwab and England Activities of Daily Living. In Third Symposium of Parkinson’s Disease; E&S Livingstone: Edinburgh, UK, 1969. [Google Scholar]
- Woods, S.P.; Tröster, A.I. Prodromal frontal/executive dysfunction predicts incident dementia in Parkinson’s disease. J. Int. Neuropsychol. Soc. 2003, 9, 17–24. [Google Scholar] [CrossRef]
- Aarsland, D.; Brønnick, K.; Ehrt, U.; De Deyn, P.P.; Tekin, S.; Emre, M.; Cummings, J.L. Neuropsychiatric symptoms in patients with Parkinson’s disease and dementia: Frequency, profile and associated care giver stress. J. Neurol. Neurosurg. Psychiatry 2007, 78, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Prell, T.; Witte, O.W.; Grosskreutz, J. Biomarkers for dementia, fatigue, and depression in Parkinson’s disease. Front. Neurol. 2019, 10, 195. [Google Scholar] [CrossRef] [Green Version]
- Byeon, H. Developing a model to predict the occurrence of the cardiocerebrovascular disease for the Korean elderly using the random forests algorithm. IJACSA 2018, 9, 494–499. [Google Scholar]
- Larose, D.T. Discovering Knowledge in Data: An Introduction to Data Mining; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Lunetta, K.L.; Hayward, L.B.; Segal, J.; Van Eerdewegh, P. Screening large-scale association study data: Exploiting interactions using random forests. BMC Genet. 2004, 5, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable. | Measurement | Characteristics |
|---|---|---|
| Sociodemographic factors | Gender | Male or female |
| Education | Middle school graduate and below or high school graduate and above | |
| Mainly used hand | Left hand, right hand, or both hands | |
| Family dementia history | Yes or no | |
| Family PD history | Yes or no | |
| Pack-years | Non-smoking, 1–20, 21–40, or ≥41 pack-years | |
| Health behaviors | Coffee-drinking | Yes or no |
| Mean coffee intake per day (cups/day) | No, ≤1, 2–3, or ≥4 cups | |
| Coffee drinking period (year) | No, ≤5, 6–9, or ≥10 years | |
| Exposure to pesticide | Never, currently not exposed but exposed previously, or currently exposed to pesticide | |
| Environmental factors | Carbon monoxide poisoning | Yes or no |
| Disease history | Manganese poisoning | Yes or no |
| Traumatic brain injury | Yes or no | |
| Stroke | Yes or no | |
| Diabetes | Yes or no | |
| Hypertension | Yes or no | |
| Hyperlipidemia | Yes or no | |
| Atrial fibrillation | Yes or no | |
| Tremor | Yes or no | |
| Exercise characteristics related to PD (PD related motor signs) | Rigidity | Yes or no |
| Bradykinesia | Yes or no | |
| Postural instability | Yes or no | |
| Rapid eye movement (REM) and sleep behavior disorders (RBD) | Yes or no | |
| Sleep behavior disorders | Total score of K-MMSE | Continuous variable |
| Neuropsychological characteristics | Total score of K-MoCA | Continuous variable |
| CDR global score | ||
| CDR sum of boxes | ||
| K-IADL | ||
| Total score of UPDRS | ||
| Motor score of UPDRS | ||
| H&Y staging (Hoehn and Yahr staging) | ||
| Schwab and England ADL |
| Characteristics | After Match | ||
|---|---|---|---|
| PD-MCI (n = 45) | PD-NC (n = 51) | Total (n = 96) | |
| Gender | |||
| Male | 24 (53.3) | 22 (43.1) | 46 (47.9) |
| Female | 21 (46.7) | 29 (56.9) | 50 (52.1) |
| Education | |||
| Middle school graduate and below | 27 (60.0) | 32 (62.7) | 59 (61.5) |
| High school graduate and above | 18 (40.0) | 19 (37.3) | 37 (38.5) |
| Mainly used hand | |||
| Right hand | 44 (97.8) | 47 (92.2) | 91 (94.8) |
| Left hand | 1 (2.2) | 1 (2.0) | 2 (2.1) |
| Both hands | 0 | 3 (5.9) | 3 (3.1) |
| Family PD history | |||
| No | 36 (92.3) | 33 (91.7) | 69 (92.0) |
| Yes | 3 (7.7) | 3 (8.3) | 6 (8.0) |
| Family dementia history | |||
| No | 36 (94.7) | 32 (91.4) | 68 (93.2) |
| Yes | 2 (5.3) | 3 (8.6) | 5 (6.8) |
| Pack year (Smoking) | |||
| 1–20 | 6 (13.3) | 3 (5.9) | 9 (9.4) |
| 21–40 | 3 (6.7) | 2 (3.9) | 5 (5.2) |
| 41+ | 36 (80.0) | 46 (90.2) | 82 (85.4) |
| Coffee-drinking | |||
| No | 15 (33.3) | 19 (37.3) | 34 (35.4) |
| Yes | 30 (66.7) | 32 (62.7) | 57 (64.6) |
| Carbon monoxide poisoning | |||
| No | 42 (97.7) | 38 (86.4) | 80 (92.0) |
| Yes | 1 (2.3) | 6 (13.6) | 7 (8.0) |
| Traumatic brain injury | |||
| No | 40 (93.0) | 42 (95.5) | 82 (94.3) |
| Yes | 3 (7.0) | 2 (4.5) | 5 (5.7) |
| Stroke | |||
| No | 41 (95.3) | 44 (100) | 85 (97.7) |
| Yes | 2 (4.7) | 0 | 2 (2.3) |
| Diabetes | |||
| No | 36 (80.0) | 37 (74.4) | 73 (76.8) |
| Yes | 9 (20.0) | 13 (26.0) | 22 (23.2) |
| Hypertension | |||
| No | 32 (71.1) | 25 (50.0) | 57 (60.0) |
| Yes | 13 (28.9) | 25 (50.0) | 38 (40.0) |
| Hyperlipidemia | |||
| No | 41 (91.1) | 43 (86.0) | 84 (88.4) |
| Yes | 4 (8.9) | 7 (14.0) | 11 (11.6) |
| Atrial fibrillation | |||
| No | 44 (97.8) | 47 (94.0) | 91 (95.8) |
| Yes | 1 (2.2) | 3 (6.0) | 4 (4.2) |
| Tremor | |||
| No | 14 (33.3) | 8 (17.4) | 22 (25.0) |
| Yes | 28 (66.7) | 38 (82.6) | 66 (75.0) |
| Rigidity | |||
| No | 3 (7.0) | 8 (17.0) | 11 (12.2) |
| Yes | 40 (93.0) | 39 (83.0) | 79 (87.8) |
| Bradykinesia | |||
| No | 2 (4.7) | 6 (12.8) | 8 (8.9) |
| Yes | 41 (95.3) | 41 (87.2) | 82 (91.1) |
| Postural instability | |||
| No | 22 (55.0) | 28 (60.9) | 50 (58.1) |
| Yes | 18 (45.0) | 18 (39.1) | 36 (41.9) |
| REM sleep behavior disorders | |||
| No | 29 (67.4) | 27 (56.3) | 56 (61.5) |
| Yes | 14 (32.6) | 21 (43.7) | 35 (38.5) |
| Depression (GDS) | |||
| No | 22 (62.9) | 22 (75.9) | 44 (68.8) |
| Yes | 13 (37.1) | 7 (24.1) | 20 (31.3) |
| K-MMSE, mean ± SD | 25.8 ± 2.7 | 25.4 ± 4.7 | 25.6 ± 3.9 |
| K-MoCA, mean ± SD | 20.6 ± 4.0 | 20.5 ± 6.2 | 20.5 ± 5.3 |
| Global CDR score, mean ± SD | 0.5 ± 0.2 | 0.5 ± 0.6 | 0.5 ± 0.4 |
| Sum of boxes in CDR, mean ± SD | 1.4 ± 1.4 | 0.8 ± 1.3 | 1.2 ± 1.4 |
| K-IADL, mean ± SD | 1.0 ± 2.6 | 0.7 ± 1.0 | 0.8 ± 2.0 |
| Total UPDRS, mean ± SD | 34.9 ± 18.9 | 29.9 ± 13.1 | 33.0 ± 16.9 |
| Motor UPDRS, mean ± SD | 22.6 ± 11.6 | 17.9 ± 8.6 | 20.0 ± 10.3 |
| H&Y staging score, mean ± SD | 2.1 ± 0.8 | 1.8 ± 0.6 | 2.0 ± 0.7 |
| Schwab and England ADL, mean ± SD | 80.0 ± 16.0 | 87.7 ± 8.1 | 83.6 ± 13.3 |
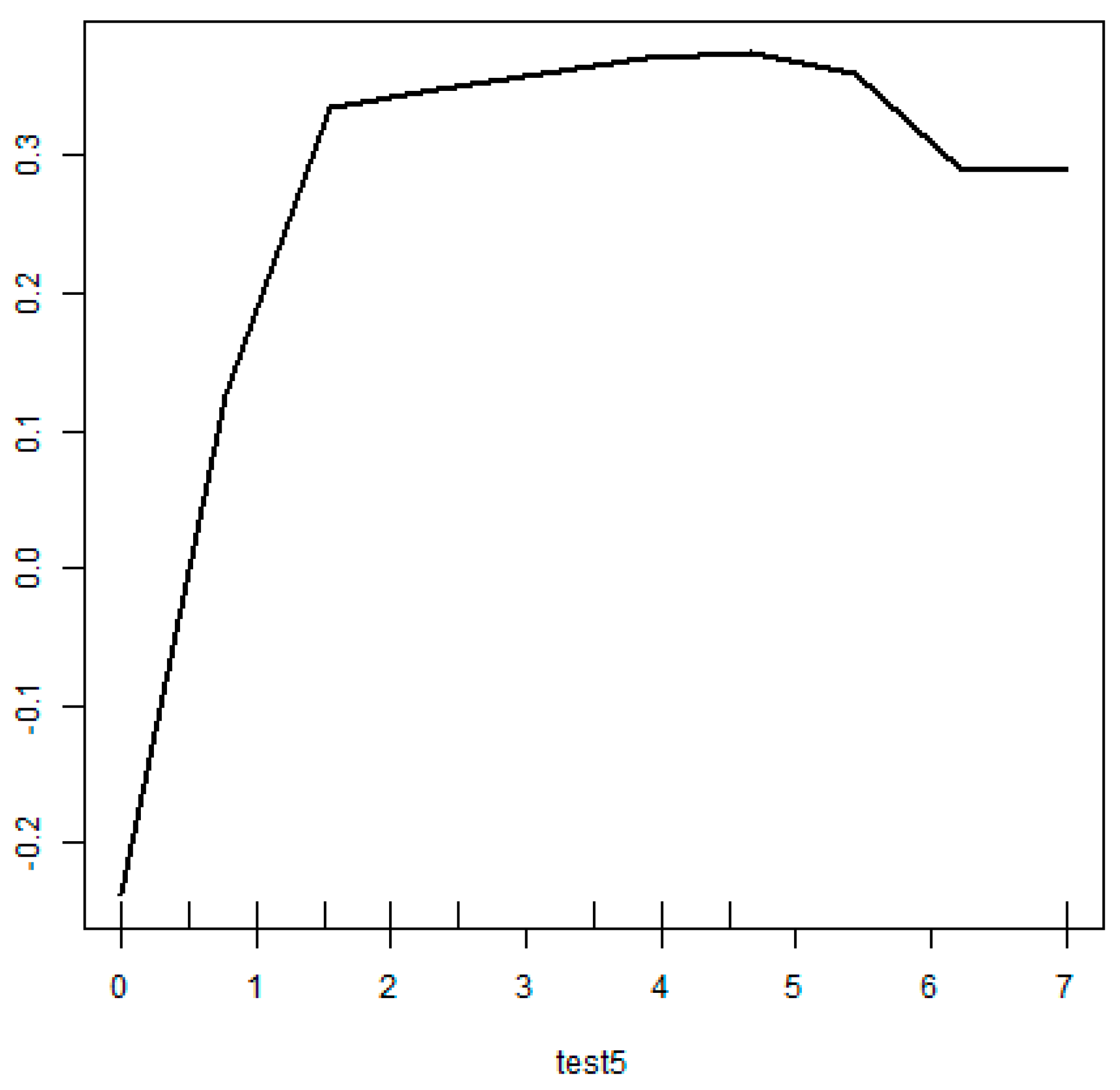
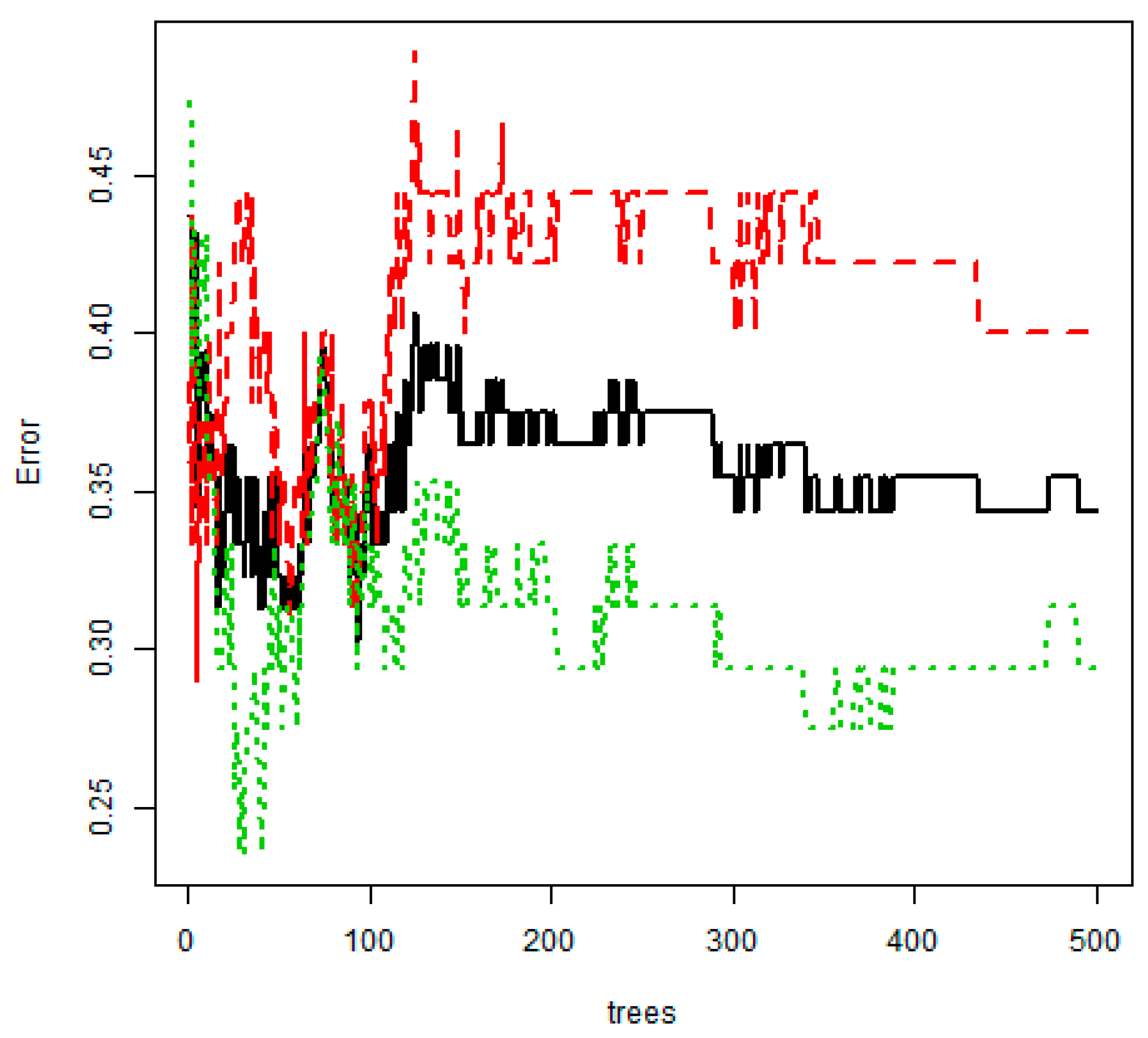
| Numbers of mtry | Error of Out-of-Bag |
|---|---|
| 5 | 0.344 |
| 6 | 0.375 |
| 7 | 0.396 |
| 8 | 0.375 |
| 9 | 0.396 |
| 10 | 0.365 |
| 11 | 0.385 |
| 12 | 0.375 |
| 13 | 0.375 |
| 14 | 0.375 |
| 15 | 0.375 |
| Model | Overall Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Multiple logistic regression | NA | NA | NA |
| Decision tree | 67.7 | 51.1 | 82.4 |
| Random Forest | 65.6 | 70.6 | 60.0 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byeon, H. Is the Random Forest Algorithm Suitable for Predicting Parkinson’s Disease with Mild Cognitive Impairment out of Parkinson’s Disease with Normal Cognition? Int. J. Environ. Res. Public Health 2020, 17, 2594. https://doi.org/10.3390/ijerph17072594
Byeon H. Is the Random Forest Algorithm Suitable for Predicting Parkinson’s Disease with Mild Cognitive Impairment out of Parkinson’s Disease with Normal Cognition? International Journal of Environmental Research and Public Health. 2020; 17(7):2594. https://doi.org/10.3390/ijerph17072594
Chicago/Turabian StyleByeon, Haewon. 2020. "Is the Random Forest Algorithm Suitable for Predicting Parkinson’s Disease with Mild Cognitive Impairment out of Parkinson’s Disease with Normal Cognition?" International Journal of Environmental Research and Public Health 17, no. 7: 2594. https://doi.org/10.3390/ijerph17072594
APA StyleByeon, H. (2020). Is the Random Forest Algorithm Suitable for Predicting Parkinson’s Disease with Mild Cognitive Impairment out of Parkinson’s Disease with Normal Cognition? International Journal of Environmental Research and Public Health, 17(7), 2594. https://doi.org/10.3390/ijerph17072594