Comparison of Bioelectrical Impedance Analysis and Dual Energy X-ray Absorptiometry for Total and Segmental Bone Mineral Content with a Three-Compartment Model


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Body Composition Measurement
2.4. Statistical Analysis
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| LOA | limit of agreement; |
| FM | fat mass; |
| BF% | percentage body fat. |
References
- Bouchard, C.; Perusse, L. Heredity and body fat. Annu. Rev. Nutr. 1988, 8, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Zemel, B.S.; Reley, E.M.; Stallings, V.A. Evaluation of methodology for nutritional assessment in children: Anthropometry, body composition, and energy expenditure. Annu. Rev. Nutr. 1997, 17, 211–235. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Katzmarzyk, P.T.; Ross, R.; Leon, A.S.; Skinner, J.S.; Rao, D.C.; Wilmore, J.H.; Rankinen, T.; Bouchard, C. Fitness alters the associations of BMI and waist circumference with total and abdominal fat. Obes. Res. 2004, 12, 525–537. [Google Scholar] [CrossRef] [PubMed]
- Despres, J.P. The insulin resistance-dyslipidemic syndrome of visceral obesity: Effect on patients’ risk. Obes. Res. 1998, 6, 8S–17S. [Google Scholar] [CrossRef] [PubMed]
- Ellis, K.J. Human body composition: In Vivo method. Physiol. Rev. 2000, 80, 649–680. [Google Scholar] [CrossRef] [Green Version]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Pietroelli, A.; Formica, C.; Wang, Z.; Heymsfield, S.B. Dual-energy X-ray absorptiometry body composition model: Review of physical concepts. Am. J. Physiol. 1996, 271, E941–E951. [Google Scholar]
- Kohrt, W.M. Body composition by DXA: Tried and true? Med. Sci. Sports Exerc. 1995, 28, 1349–1353. [Google Scholar] [CrossRef]
- Tothill, P.; Fenner, J.A.; Reid, D.M. Comparisons between three dual-energy X-ray absorptiometers used for measuring spine and femur. Br. J. Radiol. 1995, 68, 621–629. [Google Scholar] [CrossRef]
- Maw, G.J.; Mackenzie, I.L.; Taylor, N.A. Redistribution of body fluids during postural manipulations. Acta Physiol. Scand. 1995, 155, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Oshima, Y.; Shiga, T. Within-day variability of whole-body and segmental bioelectrical impedance in a standing position. Eur. J. Clin. Nutr. 2006, 60, 938–941. [Google Scholar] [CrossRef] [Green Version]
- Mazess, R.B.; Peppler, W.W.; Chesney, R.W.; Lange, T.A.; Lindgren, U.; Smith, E., Jr. Total body and regional bone mineral by dual-photon absorptiometry in metabolic bone disease. Calcif. Tissue Int. 1984, 36, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Rico, H.; Revilla, M.; Villa, L.F.; Alvarez de Buergo, M. Age-related differences in total and regional bone mass: A cross-sectional study with DXA in 429 normal women. Osteoporos. Int. 1993, 3, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Malcolm, S.A.; Khan, K.M.; Thomas, S.A.; Reid, S.J.; Brukner, P.D.; Ebeling, P.R.; Wark, J.D. Bone mass and bone turnover in power athletes, endurance athletes, and controls: A 12-month longitudinal study. Bone 1997, 20, 477–484. [Google Scholar] [CrossRef]
- Calbet, J.A.; Moysi, J.S.; Dorado, C.; Rodríguez, L.P. Bone mineral content and density in professional tennis players. Calcif. Tissue Int. 1998, 62, 491–496. [Google Scholar] [CrossRef]
- Sinaki, M.; Wahner, H.W.; Offord, K.P. Relationship between grip strength and related regional bone mineral content. Arch. Phys. Med. Rehabil. 1989, 70, 823–826. [Google Scholar]
- Chen, K.T.; Chen, Y.Y.; Wang, C.W.; Chuang, C.L.; Chiang, L.M.; Lai, C.L.; Lu, H.K.; Dwyer, G.B.; Chao, S.P.; Shih, M.K.; et al. Comparison of standing posture bioelectrical impedance analysis with DXA for body composition in a large, healthy Chinese population. PLoS ONE 2016, 11, e0160105. [Google Scholar] [CrossRef]
- Karelis, A.D.; Chamberland, G.; Aubertin-Leheudre, M.; Duval, C. Validation of a portable bioelectrical impedance analyzer for the assessment of body composition. Appl. Physiol. Nutr. Metab. 2013, 38, 27–32. [Google Scholar] [CrossRef]
- Lee, L.W.; Liao, Y.S.; Lu, H.K.; Hsiao, P.L.; Chen, Y.Y.; Chi, C.C.; Hsieh, K.C. Validation of two portable bioelectrical impedance analyses for the assessment of body composition in school age children. PLoS ONE 2017, 12, e0171568. [Google Scholar] [CrossRef]
- Esco, M.R.; Snarr, R.L.; Leatherwood, M.D.; Chamberlain, N.A.; Redding, M.L.; Flatt, A.A.; Moon, J.R.; Williford, H.N. Comparison of total and segmental body composition using DXA and multifrequency bioimpedance in collegiate female athletes. J. Strength Cond. Res. 2015, 29, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.L.; Holmes, J.C.; Desautels, R.L.; Edmonds, L.B.; Nuudi, L. Ability of new octapolar bioimpedance spectroscopy analyzers to predict 4-component-model percentage body fat in Hispanic, black, and white adults. Am. J. Clin. Nutr. 2008, 87, 332–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Castro, J.A.C.; de Lima, T.R.; Silva, D.A.S. Body composition estimation in children and adolescents by bioelectrical impedance analysis: A systematic review. J. Bodyw. Mov. Ther. 2017, 22, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Stone, T.M.; Wingo, J.E.; Nickerson, B.S.; Esco, M.R. Comparison of bioelectrical impedance analysis and dual-energy x-ray absorptiometry for estimating bone mineral content. Int. J. Sport. Nutr. Exerc. Metab. 2018, 28, 542–546. [Google Scholar] [CrossRef]
- Lee, L.W.; Liao, Y.S.; Lu, H.K.; Hsieh, K.C.; Chi, C.C. Performance of bioelectrical impedance analysis in the estimation of bone mineral content in healthy children aged 6–12 years. J. Clin. Densitom. 2019. [Google Scholar] [CrossRef]
- Segal, K.R.; Burastero, S.; Chum, A.; Coronel, P.; Pierson, R.; Wang, J. Estimation of extracellular and total body water by multiple-frequency bioelectrical-impedance measurement. Am. J. Clin. Nutr. 1991, 54, 26–29. [Google Scholar] [CrossRef]
- Segal, K.R.; Van Loan, M.; Fitzgerald, P.I.; Hodgdon, J.A.; Van Itallie, T.B. Lean body mass estimation by bioelectrical impedance analysis: A four-site cross-validation study. Am. J. Clin. Nutr. 1988, 47, 7–14. [Google Scholar] [CrossRef]
- Cha, K.; Chertow, G.M.; Gonzalez, J.; Lazarus, J.M.; Wilmore, D.W. Multifrequency bioelectrical impedance estimates the distribution of body water. J. Appl. Physiol. 1995, 79, 1316–1319. [Google Scholar] [CrossRef]
- Bedogni, G.; Malavolti, M.; Severi, S.; Poli, M.; Mussi, C.; Fantuzzi, A.L.; Battistini, N. Accuracy of an eight-point tactile-electrode impedance method in the assessment of total body water. Eur. J. Clin. Nutr. 2002, 56, 1143–1148. [Google Scholar] [CrossRef] [Green Version]
- Alkahtani, S.A. A cross-sectional study on sarcopenia using different methods: Reference values for healthy Saudi young men. BMC Musculoskelet. Disord. 2017, 18, 119. [Google Scholar] [CrossRef] [Green Version]
- Mally, K.; Trentmann, J.; Heller, M.; Dittmar, M. Reliability and accuracy of segmental bioelectrical impedance analysis for assessing muscle and fat mass in older Europeans: A comparison with dual-energy X-ray absorptiometry. Eur. J. Appl. Physiol. 2011, 111, 1879–1887. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Jensen, B.; Braun, W.; Pourhassan, M.; Gallagher, D.; Muller, M.J. Quantification of whole-body and segmental skeletal muscle mass using phase-sensitive 8-electrode medical bioelectrical impedance devices. Eur. J. Clin. Nutr. 2017, 71, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Johnson, P.E.; Bolonchuk, W.W.; Lykken, G.I. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am. J. Clin. Nutr. 1985, 41, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Bracco, D.; Thiebaud, D.; Chiolero, R.L.; Landry, M.; Burckhardt, P.; Schutz, Y. Segmental body composition assessed by bioelectrical impedance analysis and DEXA in humans. J. Appl. Physiol. 1985, 81, 2580–2587. [Google Scholar] [CrossRef] [Green Version]
- von Hurst, P.R.; Walsh, D.C.I.; Conlon, C.A.; Ingram, M.; Kruger, R.; Stonehouse, W. Validity and reliability of bioelectrical impedance analysis to estimate body fat percentage against air displacement plethysmography and dual-energy X-ray absorptiometry. Nutr. Diet. 2016, 73, 197–204. [Google Scholar] [CrossRef]
- Anderson, L.J.; Erceg, D.N.; Schroeder, E.T. Utility of multifrequency bioelectrical impedance compared with dual-energy x-ray absorptiometry for assessment of total and regional body composition varies between men and women. Nutr. Res. 2012, 32, 479–485. [Google Scholar] [CrossRef]
- Kim, J.; Shen, W.; Gallagher, D.; Jones, A.; Wang, Z., Jr.; Wang, J.; Heshka, S.; Heymsfield, S.B. Total-body skeletal muscle mass: Estimation by dual-energy X-ray absorptiometry in children and adolescents. Am. J. Clin. Nutr. 2006, 84, 1014–1020. [Google Scholar] [CrossRef]
- Kim, J.; Wang, Z.; Heymsfield, S.B.; Baumgartner, R.N.; Gallagher, D. Total-body skeletal muscle mass: Estimation by a new dual-energy X-ray absorptiometry method. Am. J. Clin. Nutr. 2002, 76, 378–383. [Google Scholar] [CrossRef] [Green Version]
- Shih, R.; Wang, Z.; Heo, M.; Wang, W.; Heymsfield, S.B. Lower limb skeletal muscle mass: Development of dual-energy X-ray absorptiometry prediction model. J. Appl. Physiol. 1985, 89, 1380–1386. [Google Scholar] [CrossRef] [Green Version]
- Furstenberg, A.; Davenport, A. Comparison of multifrequency bioelectrical impedance analysis and dual-energy X-ray absorptiometry assessments in outpatient hemodialysis patients. Am. J. Kidney Dis. 2011, 57, 123–129. [Google Scholar] [CrossRef]
- Ling, C.H.; de Craen, A.J.; Slagboom, P.E.; Gunn, D.A.; Stokkel, M.P.; Westendorp, R.G.; Maier, A.B. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin. Nutr. 2011, 30, 610–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2015, 15, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G.; Harris, M.; Teixeira, P.J.; Weiss, L. Assessing body composition and changes in body composition. Another look at dual-energy X-ray absorptiometry. Ann. N. Y. Acad. Sci. 2000, 904, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Genton, L.; Hans, D.; Kyle, U.G.; Pichard, C. Dual-energy X-ray absorptiometry and body composition: Differences between devices and comparison with reference methods. Nutrition 2002, 18, 66–70. [Google Scholar] [CrossRef]
- Toombs, R.J.; Ducher, G.; Shepherd, J.A.; De Souza, M.J. The impact of recent technological advances on the trueness and precision of DXA to assess body composition. Obesity 2011, 20, 30–39. [Google Scholar] [CrossRef]
- Deurenberg, P. Limitations of the bioelectrical impedance method for the assessment of body fat in severe obesity. Am. J. Clin. Nutr. 1996, 64, 449S–452S. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | (n = 239) | Males | (n = 106) | Females | (n = 133) | |
|---|---|---|---|---|---|---|
| Age (y) | 33.8 ± 5.9 | (20.0, 45.0) | 35.1 ± 5.8 | (23.0, 45.0) | 32.7 ± 5.8 *** | (20.0–45.0) |
| Height (cm) | 166.0 ± 7.9 | (143.5, 189.0) | 172.3 ± 6.1 | (160.4, 189.0) | 161.1 ± 5.2 *** | (143.5–174.8) |
| Body weight (kg) | 64.5 ± 13.6 | (40.1, 108.5) | 74.5 ± 11.7 | (46.8, 108.5) | 56.6 ± 8.9 *** | (40.1–95.4) |
| Body mass index (kg/m2) | 23.3 ± 3.6 | (16.9, 34.0) | 25.1 ± 3.5 | (17.4, 34.0) | 21.9 ± 3.0 *** | (16.9–31.7) |
| Waist circumference (cm) | 78.2 ± 10.7 | (60.0, 111.0) | 84.9 ± 9.5 | (65.0, 111.0) | 72.9 ± 8.2 *** | (60.0–101.0) |
| Hip circumference (cm) | 94.3 ± 6.69 | (69.0, 114.0) | 96.3 ± 6.6 | (81.0–113.0) | 92.7 ± 6.4 ** | (69.0–114.0) |
| LBM, FM, BF%, and BMC Measured by DXA | All | (n = 239) | Males | (n = 106) | Females | (n = 133) |
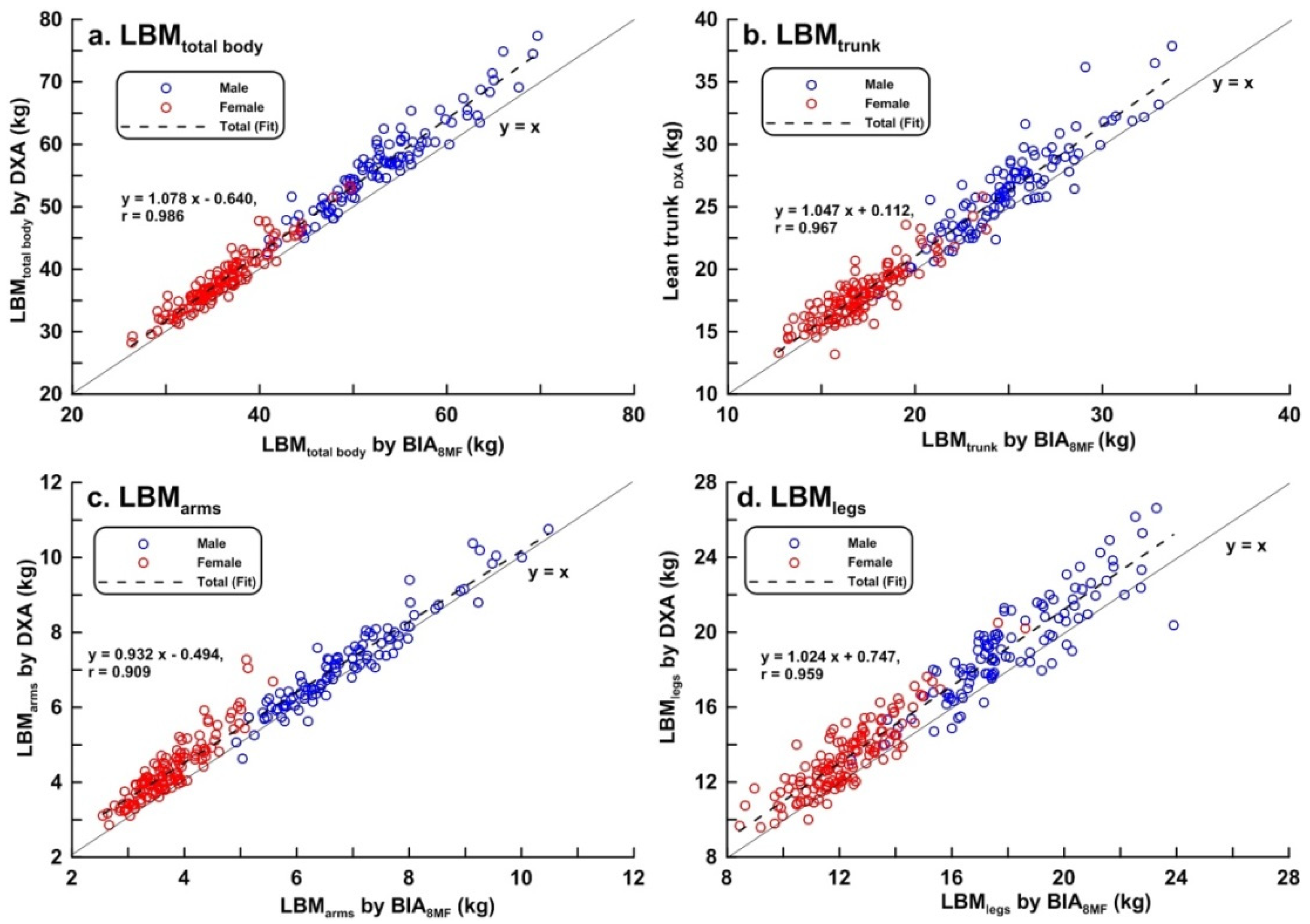
| LBMtotal_body (kg) | 46.14 ± 10.80 | (28.24, 43.36) | 56.28 ± 7.13 | (38.84, 77.36) | 38.06 ± 4.64 | (28.24, 53.37) |
| LBMtrunk (kg) | 21.72 ± 5.10 | (13.20, 37.84) | 26.44 ± 3.50 | (17.99, 37.84) | 17.96 ± 2.23 | (13.20, 25.82) |
| LBMarms (kg) | 5.12 ± 1.79 | (2.53, 10.48) | 6.86 ± 1.14 | (4.93, 10.48) | 3.72 ± 0.62 | (2.55, 5.80) |
| LBMlegs (kg) | 15.94 ± 3.73 | (9.59, 26.64) | 19.23 ± 2.65 | (13.18, 26.64) | 13.27 ± 2.05 | (9.59, 20.51) |
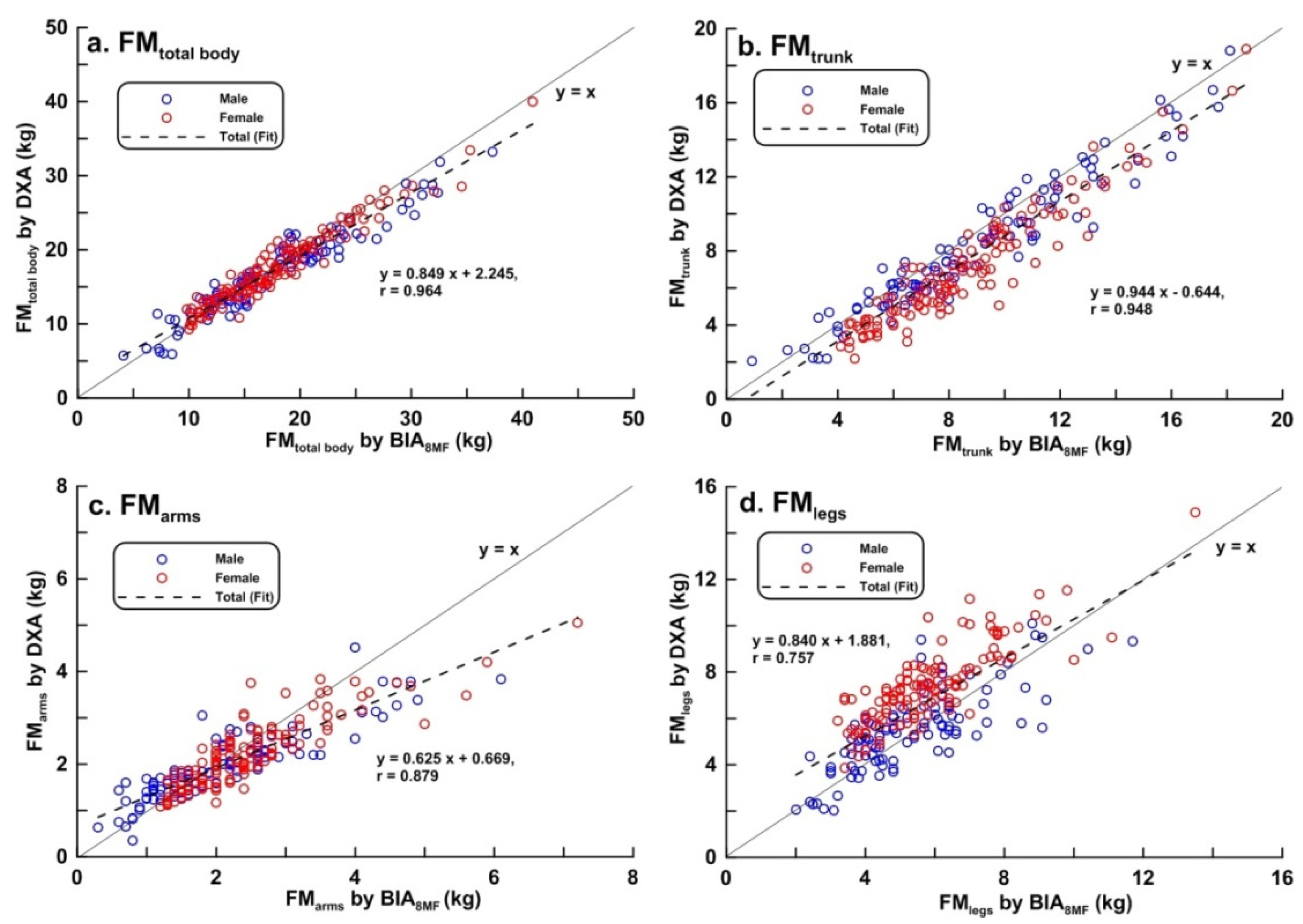
| FMtotal_body (kg) | 17.30 ± 5.40 | (5.69, 39.97) | 16.93 ± 5.67 | (5.69, 17.62) | 17.60 ± 5.18 | (9.23, 39.98) |
| FMtrunk (kg) | 7.65 ± 3.34 | (2.04, 18.90) | 8.35 ± 3.53 | (2.04, 18.82) | 7.09 ± 3.08 | (2.19, 18.90) |
| FMarms (kg) | 2.10 ± 0.75 | (0.35, 5.05) | 1.96 ± 0.74 | (0.35, 4.53) | 2.30 ± 1.30 | (1.09, 5.05) |
| FMlegs (kg) | 6.58 ± 1.93 | (2.03, 14.88) | 5.53 ± 1.70 | (2.03, 10.07) | 7.54 ± 3.23 | (3.85, 14.88) |
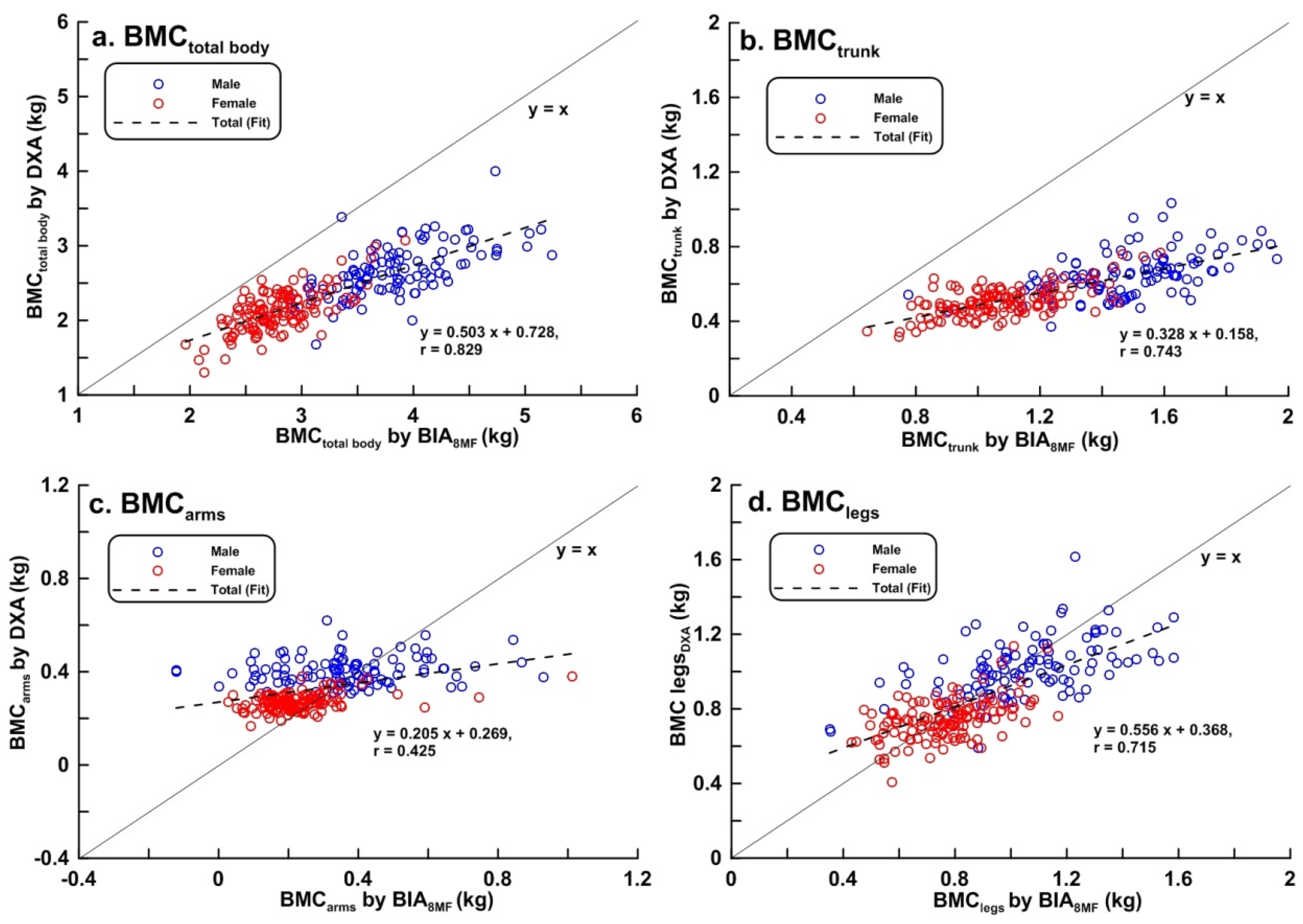
| BMCtotal_body (kg) | 2.36 ± 0.41 | (1.31, 4.00) | 2.66 ± 0.35 | (1.68, 4.00) | 2.12 ± 0.28 | (1.31, 3.07) |
| BMCtrunk (kg) | 0.57 ± 0.12 | (0.32, 1.03) | 0.65 ± 0.12 | (0.37, 1.03) | 0.51 ± 0.08 | (0.32, 0.77) |
| BMCarms (kg) | 0.33 ± 0.08 | (0.17, 0.62) | 0.40 ± 0.06 | (0.25, 0.62) | 0.27 ± 0.04 | (0.17, 0.38) |
| BMClegs (kg) | 0.87 ± 0.19 | (0.41, 1.62) | 1.02 ± 0.15 | (0.59, 1.62) | 0.74 ± 0.11 | (0.41, 1.14) |
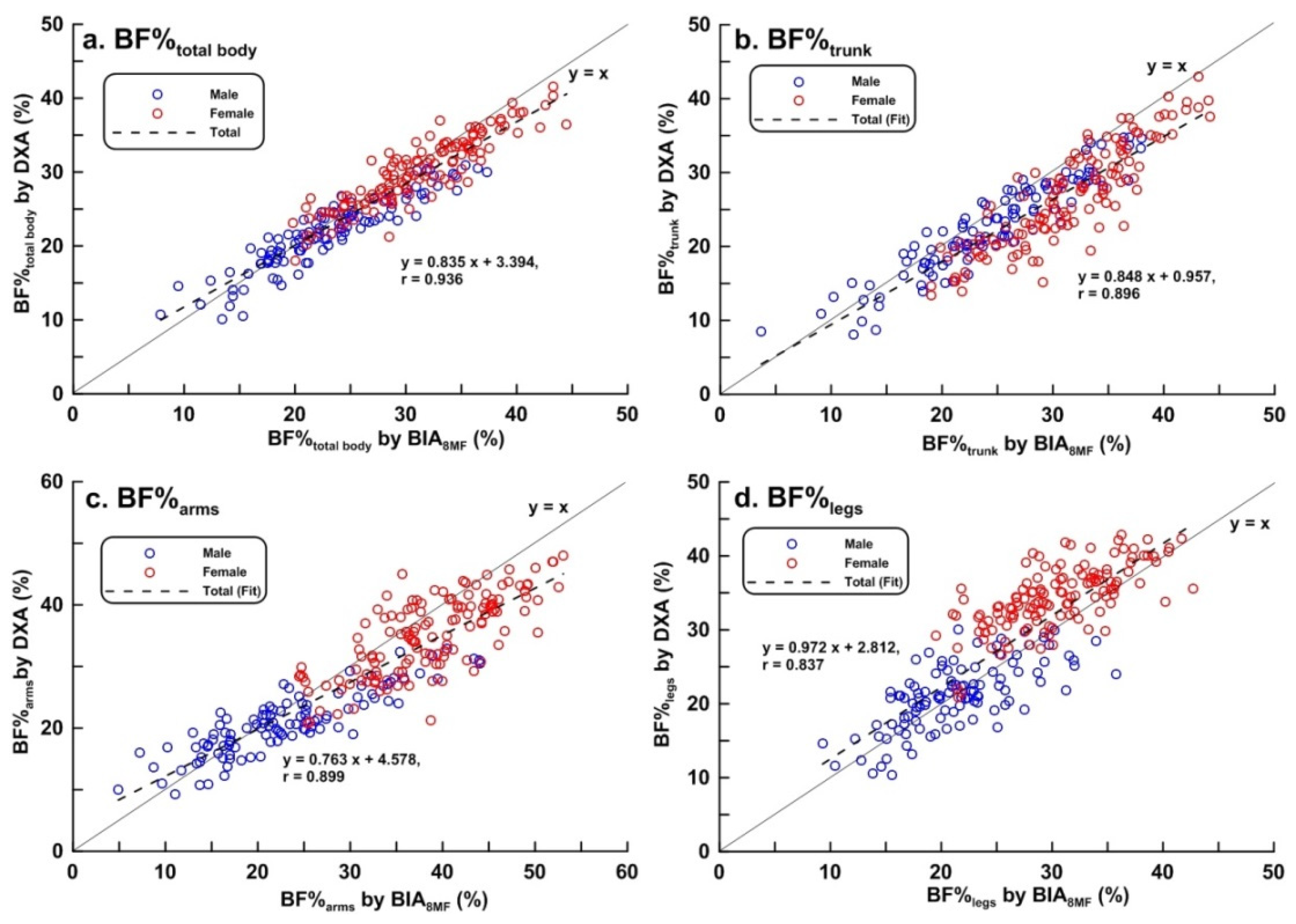
| BF%total_body (%) | 26.38 ± 6.25 | (10.10, 41.50) | 21.83 ± 4.78 | (10.10, 30.90) | 30.00 ± 4.74 | (18.00, 41.50) |
| BF%trunk (%) | 24.94 ± 6.85 | (8.10, 43.00) | 22.69 ± 6.25 | (8.10, 34.70) | 26.73 ± 6.79 | (13.40, 43.00) |
| BF%arms (%) | 28.72 ± 9.17 | (9.30, 47.95) | 20.85 ± 5.16 | (9.30, 32.85) | 35.00 ± 6.39 | (20.75, 47.95) |
| BF%legs (%) | 28.49 ± 7.89 | (10.35, 42.85) | 21.14 ± 4.46 | (10.35, 30.00) | 34.35 ± 4.29 | (20.85, 42.85) |
| LBM, FM, BF%, and BMC Measured by BIA8MF | All | (n = 239) | Males | (n = 106) | Females | (n = 133) |
| LBMtotal_body (kg) | 43.36 ± 9.85 *** | (26.32, 69.66) | 52.28 ± 6.35 *** | (37.32, 69.66) | 35.93 ± 4.18 *** | (26.32, 29.74) |
| LBMtrunk (kg) | 20.65 ± 4.72 *** | (12.70, 33.70) | 25.08 ± 2.98 *** | (18.00, 33.70) | 17.11 ± 2.14 *** | (12.70, 23.80) |
| LBMarms (kg) | 6.03 ± 1.74 *** | (3.08, 11.64) | 7.43 ± 1.34 *** | (4.21, 11.64) | 4.91 ± 1.09 *** | (3.08, 9.45) |
| LBMegs (kg) | 14.84 ± 3.50 *** | (8.44, 23.89) | 18.09 ± 2.31 *** | (12.43, 23.89) | 12.25 ± 1.61 *** | (8.44, 18.62) |
| FMtotal_body (kg) | 17.76 ± 6.11 *** | (4.10, 40.90) | 17.62 ± 6.64 *** | (4.10, 37.30) | 17.86 ± 5.68 * | (9.80, 40.90) |
| FMtrunk (kg) | 2.29 ± 1.05 *** | (0.90, 18.70) | 9.05 ± 3.71 *** | (0.90, 18.10) | 8.59 ± 3.01 *** | (4.10, 18.70) |
| FMarms (kg) | 2.29 ± 1.05 *** | (0.30, 7.20) | 2.09 ± 1.11 * | (0.30, 6.10) | 2.46 ± 0.98 *** | (1.20, 7.20) |
| FMlegs (kg) | 5.59 ± 1.73 *** | (2.00, 13.50) | 5.34 ± 1.79 | (2.00, 10.70) | 5.79 ± 1.66 *** | (3.20, 13.50) |
| BMCtotal_body (kg) | 3.24 ± 0.66 *** | (1.96, 5.14) | 3.82 ± 0.49 *** | (2.67, 5.14) | 2.78 ± 0.33 *** | (1.96, 3.93) |
| BMCtrunk (kg) | 1.26 ± 0.28 *** | (0.64, 1.96) | 1.49 ± 0.21 *** | (0.78, 1.96) | 1.08 ± 0.18 *** | (0.64, 1.59) |
| BMCarms (kg) | 0.28 ± 0.17 *** | (−0.12, 1.01) | 0.35 ± 0.19 * | (−0.12, 0.93) | 0.23 ± 0.12 *** | (0.03, 1.01) |
| BMClegs (kg) | 0.90 ± 0.24 ** | (0.35, 1.58) | 1.02 ± 0.15 | (0.35, 1.58) | 0.77 ± 0.16 * | (0.43, 1.17) |
| BF%total_body (%) | 27.53 ± 6.97 *** | (7.90, 44.50) | 23.14 ± 6.03 *** | (7.90, 37.30) | 31.00 ± 5.59 *** | (19.80, 44.50) |
| BF%trunk (%) | 28.30 ± 7.18 *** | (3.70, 44.20) | 24.53 ± 6.87 *** | (3.70, 38.00) | 31.30 ± 5.92 *** | (19.00, 44.20) |
| BF%arms (%) | 31.68 ± 10.73 *** | (4.90, 53.05) | 23.09 ± 8.24 * | (4.90, 44.50) | 38.52 ± 6.87 *** | (24.50, 53.05) |
| BF%legs (%) | 26.44 ± 6.73 *** | (10.40, 42.70) | 21.46 ± 5.09 | (10.40, 35.80) | 30.41 ± 5.02 *** | (19.50, 42.70) |
| Bias a (mean ± 2 SD) | LOA% b | Regression Equation c | r2 | PE d | |
|---|---|---|---|---|---|
| Total (n = 239) | |||||
| LBMtotal_body (kg) | −2.78 ± 3.85 | 8.3 | y = −0.092x + 1.375 | 0.247 *** | 3.380 |
| LBMtrunk (kg) | −1.07 ± 2.62 | 12.1 | y = −0.080x + 0.631 | 0.089 *** | 1.694 |
| LBMarms (kg) | 0.91 ± 1.51 | 29.5 | y = −0.027x + 1.056 | 0.003 | 1.178 |
| LBMlegs (kg) | −1.09 ± 2.17 | 13.4 | y = −0.063x − 0.111 | 0.045 *** | 1.528 |
| FMtotal_body (kg) | 0.45 ± 3.37 | 19.5 | y = 0.125x − 1.752 | 0.181 *** | 1.743 |
| FMtrunk (kg) | 1.14 ± 2.14 | 27.9 | y = 0.000x + 1.137 | 0.000 | 1.562 |
| FMarms (kg) | 0.19 ± 9.43 | 32.8 | y = 0.355x − 0.588 | 0.343 *** | 0.563 |
| FMlegs (kg) | −2.05 ± 8.74 | 30.7 | y = −0.123x − 0.237 | 0.026 * | 1.624 |
| BMCtotal_body (kg) | 0.88 ± 0.80 | 33.9 | y = 0.505x − 0.534 | 0.422 *** | 0.969 |
| BMCtrunk (kg) | 0.69 ± 0.41 | 71.6 | y = 0.051x − 0.104 | 0.647 *** | 0.717 |
| BMCarms (kg) | −0.05 ± 0.31 | 93.0 | y = 0.925x − 0.327 | 0.425 *** | 0.159 |
| BMClegs (kg) | 0.03 ± 0.34 | 39.4 | y = 0.290x − 0.226 | 0.116 *** | 0.173 |
| BF%total_body (%) | 1.15 ± 4.93 | 18.7 | y = 0.111x − 1.849 | 0.086 *** | 2.712 |
| BF%trunk (%) | 3.36 ± 6.45 | 25.9 | y = 0.051x + 2.003 | 0.010 | 4.652 |
| BF%arms (%) | 2.96 ± 9.43 | 32.8 | y = 0.165x + 2.042 | 0.116 *** | 5.559 |
| BF%legs (%) | −2.05 ± 8.74 | 30.7 | y = −0.172x + 2.699 | 0.076 *** | 4.819 |
| Males (n = 109) | |||||
| LBMtotal_body (kg) | −3.07 ± 4.16 | 7.4 | y = −0.117x + 2.808 | 0.142 *** | 2.768 |
| LBMtrunk (kg) | −1.36 ± 3.03 | 11.5 | y = −0.169x + 2.998 | 0.124 *** | 1.352 |
| LBMarms (kg) | 0.57 ± 1.36 | 19.8 | y = 0.179x − 0.711 | 0.099 *** | 0.589 |
| LBMlegs (kg) | −1.14 ± 2.46 | 12.8 | y = −0.145x + 1.583 | 0.080 ** | 1.113 |
| FMtotal_body (kg) | 0.69 ± 3.84 | 22.7 | y = 0.159x − 2.060 | 0.256 *** | 1.354 |
| FMtrunk (kg) | 0.70 ± 2.05 | 24.6 | y = 0.050x + 0.259 | 0.031 | 0.825 |
| FMarms (kg) | 0.13 ± 1.14 | 58.0 | y = 0.422x − 0.724 | 0.447 *** | 0.386 |
| FMlegs (kg) | −0.20 ± 2.35 | 42.4 | y = 0.058x − 0.514 | 0.006 | 0.789 |
| BMCtotal_body (kg) | 1.16 ± 0.76 | 28.7 | y = 0.412x − 0.176 | 0.170 *** | 0.813 |
| BMCtrunk (kg) | 0.83 ± 0.35 | 53.8 | y = 0.685x + 0.100 | 0.314 *** | 0.567 |
| BMCarms (kg) | −0.05 ± 0.39 | 109.9 | y = 1.478x − 0.604 | 0.658 *** | 0.132 |
| BMClegs (kg) | 0.04 ± 0.41 | 40.3 | y = 0.572x − 0.588 | 0.233 *** | 0.138 |
| BF%total_body (%) | 1.35 ± 4.96 | 22.7 | y = 0.240x − 0.407 | 0.264 *** | 1.873 |
| BF%trunk (%) | 1.84 ± 4.98 | 22.0 | y = 0.097x − 0.471 | 0.064 ** | 2.056 |
| BF%arms (%) | 2.25 ± 9.06 | 43.5 | y = 0.490x − 8.519 | 0.493 *** | 3.355 |
| BF%legs (%) | 0.32 ± 7.75 | 36.7 | y = 0.157x − 3.032 | 0.233 *** | 2.578 |
| Females (n = 130) | |||||
| LBMtotal_body (kg) | −2.13 ± 3.00 | 7.9 | y = −0.106x + 1.804 | 0.095 *** | 1.939 |
| LBMtrunk (kg) | −0.85 ± 0.35 | 12.0 | y = −0.047x − 0.023 | 0.009 | 1.021 |
| LBMarms (kg) | 1.19 ± 1.47 | 39.5 | y = 0.638x − 1.587 | 0.525 *** | 1.021 |
| LBMlegs (kg) | −1.02 ± 1.97 | 14.8 | y = −0.202x + 1.525 | 0.144 *** | 1.046 |
| FMtotal_body (kg) | 0.26 ± 2.91 | 16.5 | y = 0.095x − 1.424 | 0.124 *** | 1.098 |
| FMtrunk (kg) | 1.49 ± 1.94 | 27.4 | y = −0.022x + 1.668 | 0.005 | 1.327 |
| FMarms (kg) | 0.15 ± 2.32 | 100.6 | y = 0.293x − 0.443 | 0.244 *** | 0.410 |
| FMlegs (kg) | −1.86 ± 6.15 | 80.4 | y = −0.017x − 1.503 | 0.001 | 1.419 |
| BMCtotal_body (kg) | 0.66 ± 0.49 | 23.2 | y = 0.197x + 0.177 | 0.051 *** | 0.526 |
| BMCtrunk (kg) | 0.57 ± 0.28 | 56.0 | y = 0.884x − 0.128 | 0.547 *** | 0.438 |
| BMCarms (kg) | −0.04 ± 0.22 | 81.5 | y = 1.354x − 0.379 | 0.720 *** | 0.087 |
| BMClegs (kg) | 0.03 ± 0.27 | 36.8 | y = 0.457x − 0.321 | 0.149 *** | 0.104 |
| BF%total_body (%) | 0.99 ± 4.89 | 16.3 | y = 0.173x − 4.283 | 0.127 *** | 1.961 |
| BF%trunk (%) | 4.57 ± 6.47 | 24.2 | y = −0.146x + 8.816 | 0.078 ** | 4.173 |
| BF%arms (%) | 3.53 ± 4.80 | 13.7 | y = 0.084x + 0.443 | 0.012 | 4.433 |
| BF%legs (%) | −3.93 ± 7.59 | 22.1 | y = 0.186x − 9.949 | 0.044 * | 4.071 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, Y.-S.; Li, H.-C.; Lu, H.-K.; Lai, C.-L.; Wang, Y.-S.; Hsieh, K.-C. Comparison of Bioelectrical Impedance Analysis and Dual Energy X-ray Absorptiometry for Total and Segmental Bone Mineral Content with a Three-Compartment Model. Int. J. Environ. Res. Public Health 2020, 17, 2595. https://doi.org/10.3390/ijerph17072595
Liao Y-S, Li H-C, Lu H-K, Lai C-L, Wang Y-S, Hsieh K-C. Comparison of Bioelectrical Impedance Analysis and Dual Energy X-ray Absorptiometry for Total and Segmental Bone Mineral Content with a Three-Compartment Model. International Journal of Environmental Research and Public Health. 2020; 17(7):2595. https://doi.org/10.3390/ijerph17072595
Chicago/Turabian StyleLiao, Yu-San, Hung-Chou Li, Hsueh-Kuan Lu, Chung-Liang Lai, Yue-Sheng Wang, and Kuen-Chang Hsieh. 2020. "Comparison of Bioelectrical Impedance Analysis and Dual Energy X-ray Absorptiometry for Total and Segmental Bone Mineral Content with a Three-Compartment Model" International Journal of Environmental Research and Public Health 17, no. 7: 2595. https://doi.org/10.3390/ijerph17072595
APA StyleLiao, Y. -S., Li, H. -C., Lu, H. -K., Lai, C. -L., Wang, Y. -S., & Hsieh, K. -C. (2020). Comparison of Bioelectrical Impedance Analysis and Dual Energy X-ray Absorptiometry for Total and Segmental Bone Mineral Content with a Three-Compartment Model. International Journal of Environmental Research and Public Health, 17(7), 2595. https://doi.org/10.3390/ijerph17072595