City of Hope Quality of Life-Ostomy Questionnaire Validity and Reliability Assessment on a Croatian Sample


Abstract
:1. Introduction
2. Patients and Methods
2.1. Methods Translation
2.2. Patients/Material
2.3. Instrument CoH-QoL-OQ
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Reliability
3.2. Age Differences in Average CoH-QoL-OQ Scales
3.3. Content Validity
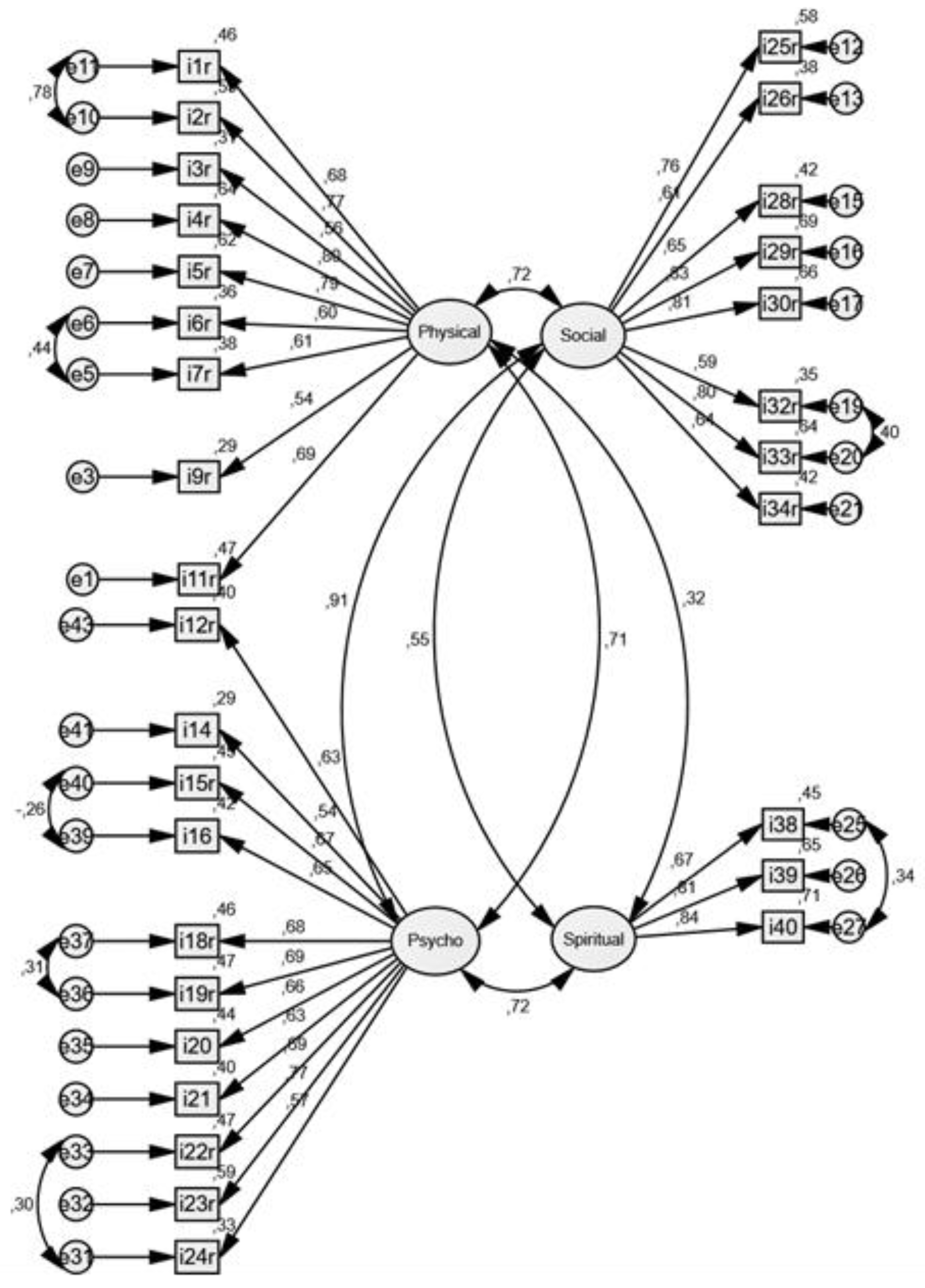
3.4. Confirmatory Factor Analysis (CFA)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nafees, B.; Storling, Z.M.; Hindsberger, C.; Lloyd, A. The ostomy leak impact tool: Development and validation of a new patient—Reported tool to measure the burden of leakage in ostomy device users. Health Qual. Life Outcomes 2018, 16, 231. [Google Scholar] [CrossRef] [PubMed]
- Croatian Institute of Public Health. Cancer Incidence in Croatia; Bulletin No 39; Croatian Institute of Public Health: Zagreb, Croatia, 2016. [Google Scholar]
- Hrvatski Zdravstveno–Statistički Ljetopis za 2017 Godinu. Available online: https://www.hzjz.hr/hrvatski-zdravstveno-statisticki-ljetopis/hrvatski-zdravstveno-statisticki-ljetopis-za-2017 (accessed on 18 October 2018).
- Hueso-Montoro, C.; Bonill de las Nieves, C.; Celdran-Manas, M.; Hernandes-Zambrano, S.M.; Amezcua-Martinez, M.; Morales-Asencio, J.M. Experiences and coping with alter bodi image in digestive stoma patients. Rev. Lat. Am. Enfermagem. 2016, 24, e2840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, S.; Njaj, R.; Barker, L.; Siegel, P.Z.; Liao, Y. Summarizing health-related quality of life (HRQOL): Development and testing of a one-factor model. Popul. Health Metr. 2016, 14, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vonk-Klaassen, S.M.; de Vocht, H.M.; den Ouden, M.E.; Eddes, E.H.; Schuurmans, M.J. Ostomy—Related problems and their impact on quality of life of colorectal cancer ostomates: A systematic review. Qual. Life Res. 2016, 25, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Maydick, D. A Descriptive Study Assessing quality of Life for Adults with a Permanent Ostomy and the Influence of Preoperative Stoma Site Marking. Ostomy Wound Menage. 2016, 62, 14–24. [Google Scholar]
- Alegre Salles VJ, Penteado Becker CP, Rossi Faria GM. The influence of time on the quality of life of patients with intestinal stoma.J. Coloproctol. 2014, 34, 73–75.
- Akiko Kimura, C.; Bellezi Guilhem, D.; Kamada, I.; Silva de Abreu, B.; Costa Fortes, R. Oncology ostomized patients’ perception regarding relationship as an important dimension in quality of life. J. Coloproctol. 2017, 37, 199–204. [Google Scholar] [CrossRef]
- Ang, S.G.; Chen, H.C.; Siah, R.J.; He, H.G.; Klainin-Yobas, P. Stressors relating to patient psychological health following stoma surgery: An integrated literature review. Oncol. Nurs. Forum 2013, 40, 587–594. [Google Scholar] [CrossRef]
- Bray, L.; Sanders, C. Preparing children and young people for stoma surgery. Paediatric Nurs. 2006, 18, 33–37. [Google Scholar] [CrossRef]
- Ayaz, S. Overview of psychosocial problems in individuals with stoma: A review of literature. Int. Wound J. 2019, 16, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Fingren, J.; Lindholm, E.; Petersén, C.; Hallén, A.M.; Carlsson, E. A Prospective, Explorative Study to Assess Adjustment 1 Year After Ostomy Surgery Among Swedish Patients. Ostomy Wound Manage. 2018, 64, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Wafaa Gameel, M.A.; Ahmed Hassanin, A.; Abd Elatif, Z. Developemet and validation of a Stoma—Quality of Life Scale in Arabic for Egiptian Patients with permanent colostomy. J. Med. Biomed. Sci. 2010, 3, 2073–2078. [Google Scholar]
- Gao, W.; Yuan, C.; Wang, J.; Du, J.; Wu, H.; Qian, X.; Hinds, P.S. A Chinese version of the City of Hope Quality of Life-Ostomy Questionnaire: Validity and reliability assessment. Cancer Nurs. 2013, 36, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.L.; Augusto Fda, S.; Gomboski, G. Health-related Quality of Life in persons with Ostomies managed in an Outpatient Care Setting. J. Wound Ostomy Cont. Nurs. 2016, 43, 158–164. [Google Scholar] [CrossRef]
- Anaraki, F.; Vafaie, M.; Behboo, R.; Esmaeilpour, S.; Maghsoodi, N.; Safaee, A.; Grant, M. The city of hope-quality of life-ostomy questionnaire: Persian translation and validation. Ann. Med. Health Sci. Res. 2014, 4, 634–637. [Google Scholar]
- Cakir, S.K.; Ozbayir, T. The effect of periperative stoma site marking on quality of life. Pak. J Med. Sci. 2018, 34, 149–153. [Google Scholar]
- Plazibat, V.; Prlić, N.; Kovačević, A. The quality of life of a patient with colostomy. SEEMEDJ 2017, 1, 81–89. [Google Scholar]
- Silva, J.O.; Gomes, P.; Gonalves, D.; Viana, C.; Nogueira, F.; Goulart, A.; Leao, P.; Mota, M.J.; Peixoto, P.; Rodrigues, A.M.; et al. Quality of Life (QoL) Among Ostomy Patients—A cross—Sectional study using Stoma—Care QoL questionnaire about the influence of some clinical and demographic dana on patients QoL. J. Coloproct. 2018, 39, 48–55. [Google Scholar]
- Magela Salome, G.; Aguinaldo de Almeida, S.; Moura Silvera, M. Quality of life and self—Esteem of patients with intestinal stoma. J. Coloproct. 2014, 34, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Grant, J.S.; Davis, L.L. Selection and use of content experts for instrument development. Res. Nurs. Health 1997, 20, 269–274. [Google Scholar] [CrossRef]
- Grant, M.; Ferrel, B.; Dean, G.; Uman, G. Revision and psychometric testing of the city of hope quality of life—Ostomy questionnaire. Qual. Life Res. 2004, 13, 1445–1447. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, J.L. Amos (Version 22.0); IBM SPSS: Chicago, IL, USA, 2006. [Google Scholar]
- Weston, R.; Gore PAWeston, R.; Gore, P.A. A brief guide to structural equation modeling. Counseling Psychol. 2006, 34, 719–751. [Google Scholar] [CrossRef]
- Krouse, R.S.; Grant, M.; Wendel, C.S.; Mohler, M.J.; Rawl, S.M.; Baldwin, C.M.; Schmidt, C.M. A mixed-methods evaluation of health-related quality of life for male veterans with and without intestinal stomas. Dis. Colon Rectum 2007, 50, 2054–2066. [Google Scholar] [CrossRef] [PubMed]
- Krouse, R.S.; Jane Mohler, M.; Wendel, C.S.; Grant, M.; Baldwin, C.M.; Rawl, S.M.; Joel Coons, S. The VA ostomy health-related quality of life study: Objectives, methods, and patient sample. Curr. Med. Res. Opin. 2006, 22, 781–791. [Google Scholar] [CrossRef]
- Krouse, R.; Grant, M.; Ferrell, B.; Dean, G.; Nelson, R.; Chu, D. Quality of Life Outcomes in 599 Cancer and Non-Cancer Patients with Colostomies. J. Surg. Res. 2007, 138, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Nunnally, J.C.; Bernstein, I.H. The Assessment of Reliability. Psychom. Theory 1994, 3, 248–292. [Google Scholar]
- Nikjoo, A.; Jafari, H.; Saba, M.A.; Ebrahimi, N.; Mirzaei, R. Patient Assessment of Constipation Quality of life Questionnaire: Translation, Cultural Adaptation, Reliability, and Validity of the Persian Version. IJMS 2018, 43, 261–268. [Google Scholar]



{kind=link}
{kind=link}
| n | (%) | ||
|---|---|---|---|
| Sex | Male | 182 | (60.3) |
| Female | 120 | (39.7) | |
| Total | 302 | (100.0) | |
| Age groups | 19–30 yrs | 18 | (6.0) |
| 31–50 yrs | 68 | (22.5) | |
| 51–70 yrs | 138 | (45.7) | |
| 70+ yrs | 78 | (25.8) | |
| Total | 302 | (100.0) | |
| Age (years) | 59.28 ± 15.26 | ||
| Type of ostomy you have | Ileostomy | 75 | (24.8) |
| Colostomy | 221 | (73.2) | |
| Urostomy | 6 | (2.0) | |
| Total | 302 | (100.0) | |
| If you have colostomy, is it permanent? | Permanent | 212 | (74.6) |
| Temporary | 72 | (25.4) | |
| Total | 284 | (100.0) | |
| Do you wear the pouch all the time? | Yes | 5 | (25.0) |
| No | 15 | (75.0) | |
| Total | 20 | (100.0) | |
| Duration of ostomy | Up to 6 months | 60 | (19.9) |
| 6–12 months | 68 | (22.5) | |
| 1.1–2 years | 26 | (8.6) | |
| 2.1–4 years | 44 | (14.6) | |
| 4.1 + 8 years | 38 | (12.6) | |
| > 8 years | 66 | (21.9) | |
| Total | 302 | (100.0) | |
| Duration of ostomy (months) | 55.23 ± 72.15 | ||
| What is your marital status | Single | 45 | (14.9) |
| Married | 198 | (65.6) | |
| Divorced | 27 | (8.9) | |
| Widower/Widow | 32 | (10.6) | |
| Total | 302 | (100.0) | |
| Mean | SD | Median | 1st Quartile | 3rd Quartile | Minimum | Maximum | Valid N | N of Items | Cronbach Alpha | Test- Retest (n = 50) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical | 6.85 | 1.82 | 7.00 | 5.54 | 7.00 | 1.82 | 10.00 | N = 299 | 11 | 0.89 | 0.99 |
| Psychological | 6.24 | 2.03 | 6.15 | 4.92 | 6.15 | 0.31 | 10.00 | N = 295 | 13 | 0.89 | 0.99 |
| Social | 6.03 | 1.89 | 6.00 | 4.75 | 6.00 | 0.83 | 10.00 | N = 295 | 12 | 0.83 | 0.99 |
| Spiritual | 6.27 | 1.94 | 6.14 | 5.00 | 6.14 | 0.00 | 10.00 | N = 298 | 7 | 0.73 | 0.99 |
| COH Total | 6.37 | 1.66 | 6.35 | 5.21 | 6.34 | 1.51 | 9.65 | N = 284 | 43 | 0.95 | 0.99 |
| Convergent Validity * | Discriminant Validity † | ||||
|---|---|---|---|---|---|
| Physical | Psychological | Social | Spiritual | ||
| Physical | 0.44–0.72 | -- | 0.35–0.56 | 0.33–0.57 | 0.14–0.34 |
| Psychological | 0.33–0.69 | 0.22–0.60 | -- | 0.30–0.66 | 0.28–0.62 |
| Social | 0.11–0.78 | 0.07–0.59 | 0.14–0.70 | -- | 0.04–0.49 |
| Spiritual | 0.22–0.63 | 0.09–0.46 | 0.11–0.57 | 0.15–0.64 | -- |
| Corrected Item-Total Correlation Total COH | Cronbach’s Alpha if Item Deleted Total COH | Physical | Psychological | Social | Spiritual | |
|---|---|---|---|---|---|---|
| Physical strength (r) | 0.542 | 0.945 | 0.437 ** | 0.493 ** | 0.208 ** | |
| Fatigue (r) | 0.611 | 0.945 | 0.506 ** | 0.541 ** | 0.272 ** | |
| Skin surrounding the ostomy (r) | 0.445 | 0.946 | 0.347 ** | 0.376 ** | 0.280 ** | |
| Sleep disorders (r) | 0.656 | 0.944 | 0.562 ** | 0.574 ** | 0.342 ** | |
| Aches or pains (r) | 0.614 | 0.945 | 0.525 ** | 0.483 ** | 0.273 ** | |
| Gas (r) | 0.473 | 0.945 | 0.359 ** | 0.373 ** | 0.185 ** | |
| Odor (r) | 0.537 | 0.945 | 0.472 ** | 0.441 ** | 0.259 ** | |
| Constipation (r) | 0.429 | 0.946 | 0.360 ** | 0.330 ** | 0.221 ** | |
| Diarrhea (r) | 0.509 | 0.945 | 0.451 ** | 0.413 ** | 0.251 ** | |
| Leaking from the pouch (or around the appliance) (r) | 0.491 | 0.945 | 0.422 ** | 0.391 ** | 0.313 ** | |
| Overall physical well-being (r) | 0.583 | 0.945 | 0.499 ** | 0.486 ** | 0.336 ** | |
| How difficult has it been for you to adjust to your ostomy? (r) | 0.638 | 0.944 | 0.437 ** | 0.493 ** | 0.208 ** | |
| How useful do you feel? | 0.414 | 0.946 | 0.592 ** | 0.602 ** | 0.402 ** | |
| How much satisfaction or enjoyment in life do you feel? | 0.489 | 0.945 | 0.220 ** | 0.331 ** | 0.381 ** | |
| How much are you embarrassed by your ostomy? (r) | 0.617 | 0.944 | 0.255 ** | 0.381 ** | 0.447 ** | |
| How good is your overall quality of life? | 0.626 | 0.944 | 0.442 ** | 0.615 ** | 0.387 ** | |
| How is your ability to remember things? | 0.339 | 0.946 | 0.413 ** | 0.539 ** | 0.468 ** | |
| How difficult is it to look at your ostomy? (r) | 0.640 | 0.944 | 0.258 ** | 0.304 ** | 0.280 ** | |
| How difficult is it for you to care for your ostomy? (r) | 0.669 | 0.944 | 0.439 ** | 0.588 ** | 0.416 ** | |
| Do you feel like you are in control of things in your life? | 0.636 | 0.944 | 0.513 ** | 0.614 ** | 0.423 ** | |
| How satisfied are you with your appearance? | 0.619 | 0.944 | 0.408 ** | 0.540 ** | 0.619 ** | |
| How much anxiety do you have? (r) | 0.687 | 0.944 | 0.379 ** | 0.510 ** | 0.517 ** | |
| How much depression do you have? (r) | 0.730 | 0.944 | 0.600 ** | 0.604 ** | 0.417 ** | |
| Are you fearful that your disease will come back? (r) | 0.585 | 0.945 | 0.486 ** | 0.664 ** | 0.564 ** | |
| Do you have difficulty meeting new people? (r) | 0.714 | 0.944 | 0.541 ** | 0.702 ** | 0.448 ** | |
| How much financial burden resulted from your illness or treatment? (r) | 0.574 | 0.945 | 0.499 ** | 0.505 ** | 0.283 ** | |
| How distressing has your illness been for your family? (r) | 0.244 | 0.947 | 0.302 ** | 0.191 ** | 0.036 | |
| How much does your ostomy interfere with your ability to travel? (r) | 0.605 | 0.944 | 0.465 ** | 0.542 ** | 0.342 ** | |
| Has your ostomy interfered with your personal relationships? (r) | 0.762 | 0.943 | 0.593 ** | 0.695 ** | 0.455 ** | |
| How much isolation is caused by your ostomy? (r) | 0.733 | 0.943 | 0.491 ** | 0.711 ** | 0.489 ** | |
| Is support from friends and family sufficient to meet your needs? | 0.181 | 0.947 | 0.045 | 0.204 ** | 0.317 ** | |
| Has your ostomy interfered with your recreational/sports activities? (r) | 0.571 | 0.945 | 0.447 ** | 0.483 ** | 0.358 ** | |
| Has your ostomy interfered with your social activities? (r) | 0.740 | 0.943 | 0.501 ** | 0.667 ** | 0.524 ** | |
| Has your ostomy interfered with your ability to be intimate? (r) | 0.591 | 0.945 | 0.413 ** | 0.543 ** | 0.410 ** | |
| Do you have enough privacy at home for doing your ostomy care? | 0.181 | 0.947 | 0.068 | 0.186 ** | 0.341 ** | |
| Do you have enough privacy when traveling for conducting your ostomy care? | 0.180 | 0.947 | 0.107 | 0.141 * | 0.256 ** | |
| How much uncertainty do you feel about your future? (r) | 0.612 | 0.944 | 0.465 ** | 0.561 ** | 0.641 ** | |
| Do you sense a reason for being alive? | 0.425 | 0.946 | 0.206 ** | 0.440 ** | 0.378 ** | |
| Do you have a sense of inner peace? | 0.560 | 0.945 | 0.332 ** | 0.566 ** | 0.476 ** | |
| How hopeful do you feel? | 0.554 | 0.945 | 0.237 ** | 0.568 ** | 0.504 ** | |
| Is support you receive from personal spiritual activities such as prayer or mediation sufficient to meet your needs? | 0.297 | 0.947 | 0.165 ** | 0.278 ** | 0.208 ** | |
| Is support you receive from religious activities such as going to church or synagogue sufficient to meet your needs? | 0.171 | 0.948 | 0.088 | 0.110 | 0.146 * | |
| Has having an ostomy made positive changes in your lifestyle? | 0.390 | 0.946 | 0.236 ** | 0.408 ** | 0.324 ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konjevoda, V.; Zelić, M.; Munjas Samarin, R.; Petek, D. City of Hope Quality of Life-Ostomy Questionnaire Validity and Reliability Assessment on a Croatian Sample. Int. J. Environ. Res. Public Health 2020, 17, 768. https://doi.org/10.3390/ijerph17030768
Konjevoda V, Zelić M, Munjas Samarin R, Petek D. City of Hope Quality of Life-Ostomy Questionnaire Validity and Reliability Assessment on a Croatian Sample. International Journal of Environmental Research and Public Health. 2020; 17(3):768. https://doi.org/10.3390/ijerph17030768
Chicago/Turabian StyleKonjevoda, Vesna, Marko Zelić, Radenka Munjas Samarin, and Davorina Petek. 2020. "City of Hope Quality of Life-Ostomy Questionnaire Validity and Reliability Assessment on a Croatian Sample" International Journal of Environmental Research and Public Health 17, no. 3: 768. https://doi.org/10.3390/ijerph17030768
APA StyleKonjevoda, V., Zelić, M., Munjas Samarin, R., & Petek, D. (2020). City of Hope Quality of Life-Ostomy Questionnaire Validity and Reliability Assessment on a Croatian Sample. International Journal of Environmental Research and Public Health, 17(3), 768. https://doi.org/10.3390/ijerph17030768