Effects of 2-Week Exercise Training in Hypobaric Hypoxic Conditions on Exercise Performance and Immune Function in Korean National Cycling Athletes with Disabilities: A Case Report

 ,
, 

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Blood Pressure
2.4. Body Composition
2.5. Exercise Performance
2.6. Oxygen-Transporting Capacity and Immune Function
2.7. Statistical Analysis
3. Results
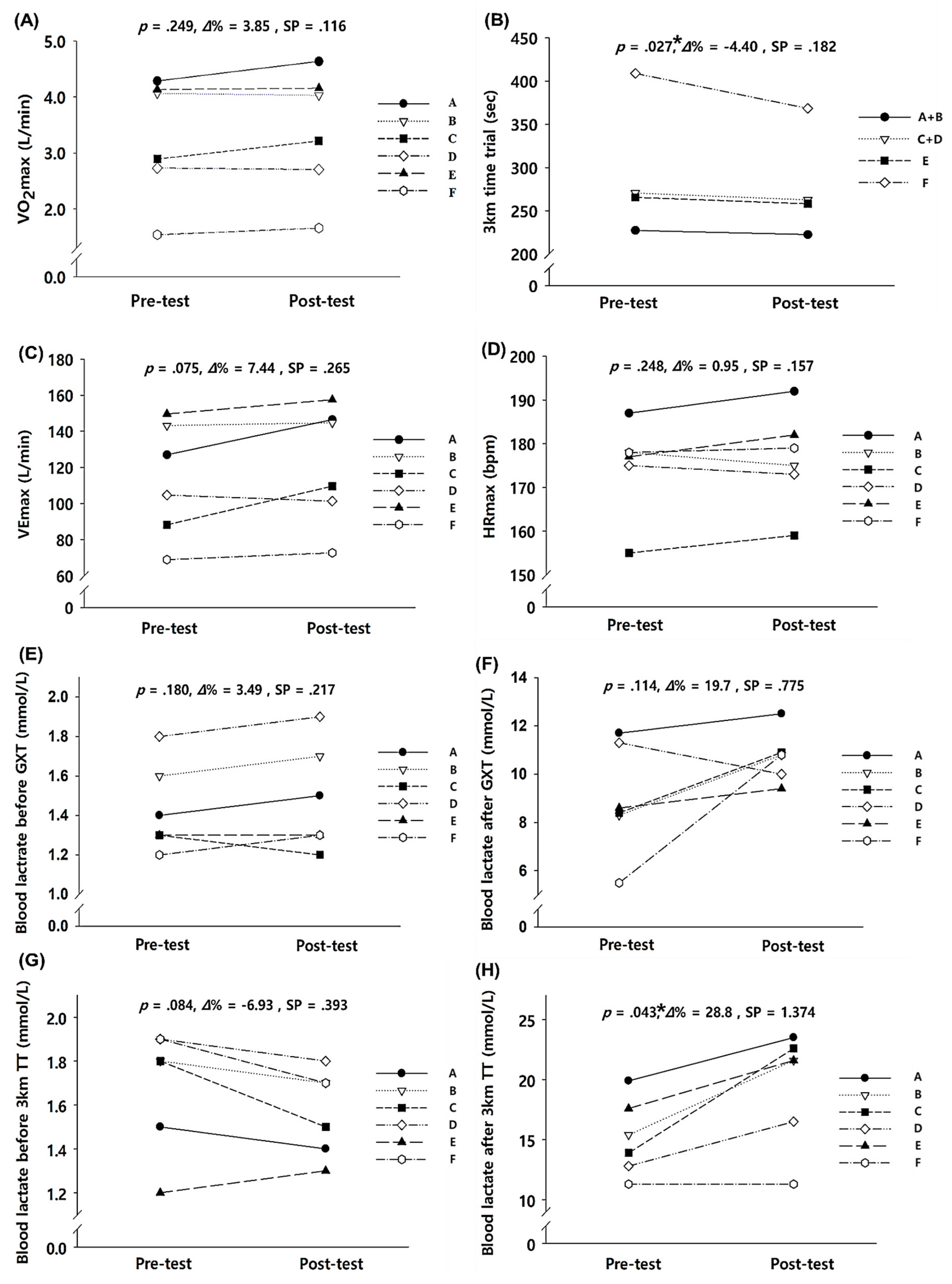
3.1. Exercise Performance
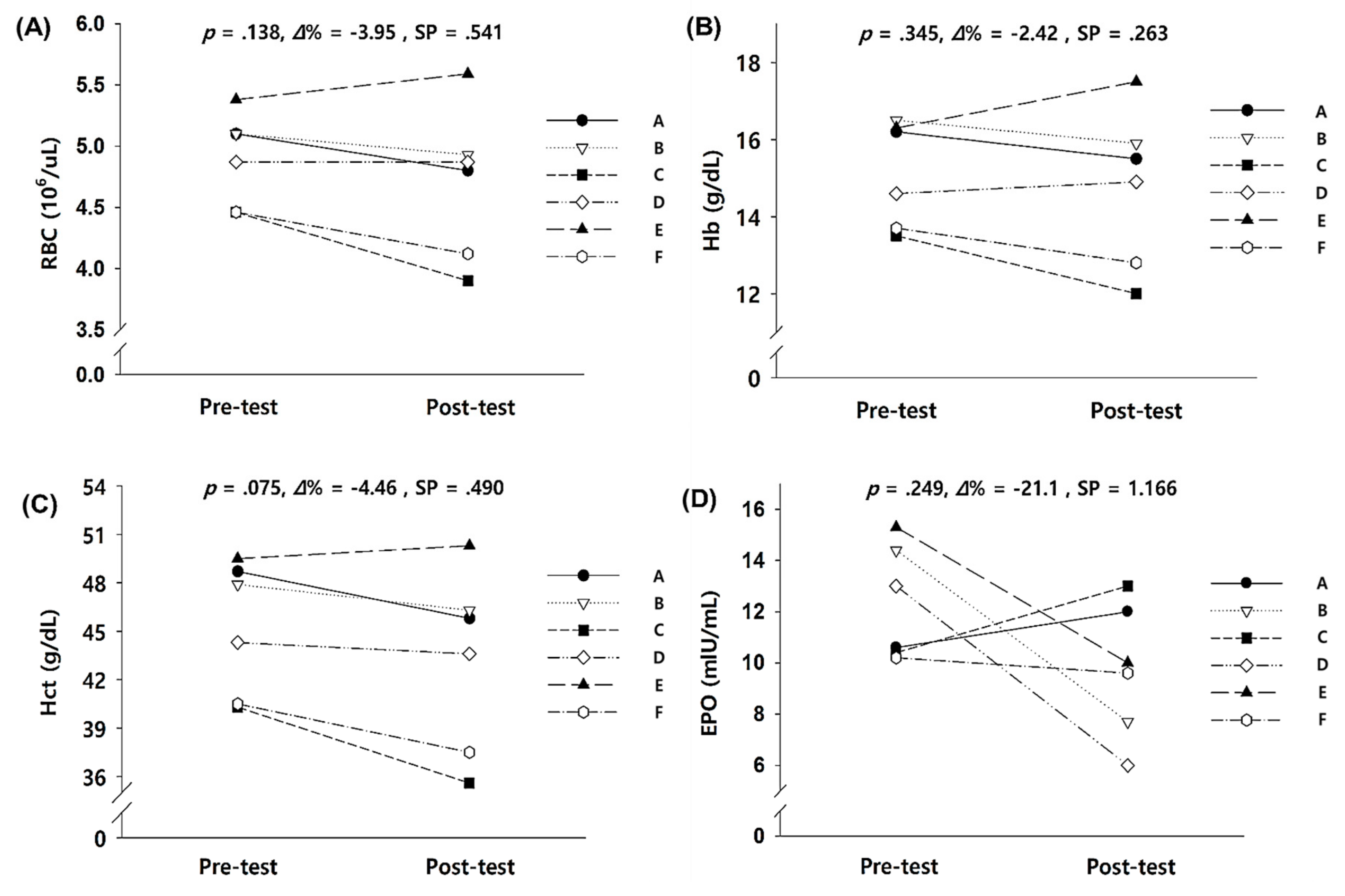
3.2. Oxygen-Transporting Capacity in the Blood
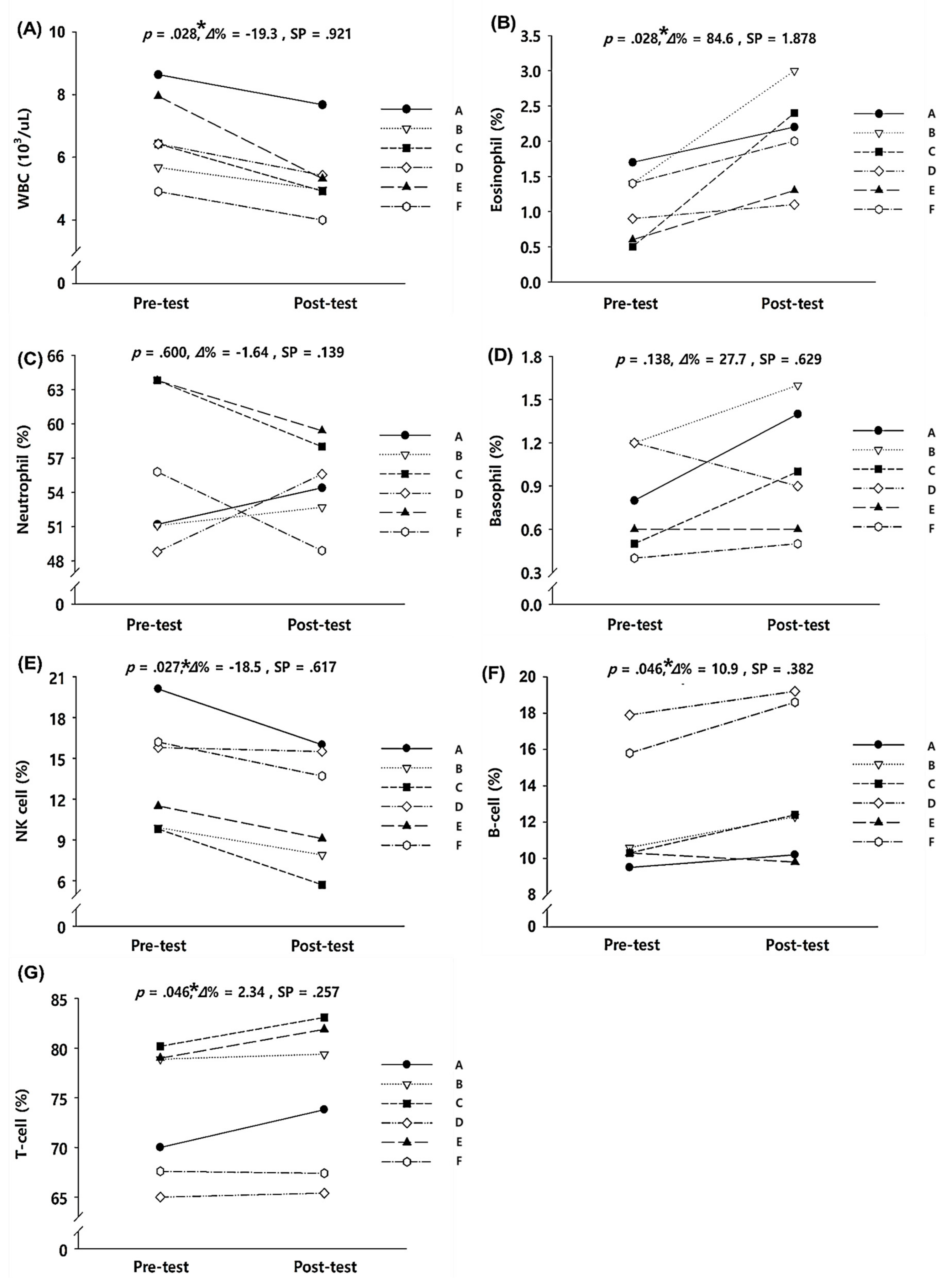
3.3. Immune Function
4. Discussion
4.1. Exercise Performance
4.2. Oxygen-Transporting Capacity of the Blood
4.3. Immune Function
5. Limitations
6. Conclusions and Suggestions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brocherie, F.; Girard, O.; Faiss, R.; Millet, G.P. Effects of Repeated-Sprint Training in Hypoxia on Sea-Level Performance: A Meta-Analysis. Sports Med. 2017, 47, 1651–1660. [Google Scholar] [CrossRef] [PubMed]
- Girard, O.; Amann, M.; Aughey, R.; Billaut, F.; Bishop, D.J.; Bourdon, P.; Buchheit, M.; Chapman, R.; D’Hooghe, M.; Garvican-Lewis, L.A.; et al. Position statement—Altitude training for improving team-sport players’ performance: Current knowledge and unresolved issues. Br. J. Sports Med. 2013, 47 (Suppl. 1), i8–i16. [Google Scholar] [CrossRef] [PubMed]
- McLean, B.D.; Gore, C.J.; Kemp, J. Application of ’live low-train high’ for enhancing normoxic exercise performance in team sport athletes. Sports Med. 2014, 44, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Lim, K. Effects of Hypoxic Training versus Normoxic Training on Exercise Performance in Competitive Swimmers. J. Sports Sci. Med. 2017, 16, 480–488. [Google Scholar] [PubMed]
- Millet, G.P.; Faiss, R.; Brocherie, F.; Girard, O. Hypoxic training and team sports: A challenge to traditional methods? Br. J. Sports Med. 2013, 47 (Suppl. 1), i6–i7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.Y.; Hwang, H.; Park, J.; Lee, S.; Lim, K. The effects of altitude/hypoxic training on oxygen delivery capacity of the blood and aerobic exercise capacity in elite athletes—A meta-analysis. J. Exerc. Nutr. Biochem. 2016, 20, 15–22. [Google Scholar] [CrossRef]
- Sinex, J.A.; Chapman, R.F. Hypoxic training methods for improving endurance exercise performance. J. Sport Health Sci. 2015, 4, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Czuba, M.; Waskiewicz, Z.; Zajac, A.; Poprzecki, S.; Cholewa, J.; Roczniok, R. The effects of intermittent hypoxic training on aerobic capacity and endurance performance in cyclists. J. Sports Sci. Med. 2011, 10, 175–183. [Google Scholar]
- Park, H.-Y.; Kim, S.; Nam, S.-S. Four-week “living high training low” program enhances 3000-m and 5000-m time trials by improving energy metabolism during submaximal exercise in athletes. J. Exerc. Nutr. Biochem. 2017, 21, 1. [Google Scholar] [CrossRef]
- Park, H.-Y.; Nam, S.-S. Application of “living high-training low” enhances cardiac function and skeletal muscle oxygenation during submaximal exercises in athletes. J. Exerc. Nutr. Biochem. 2017, 21, 13. [Google Scholar] [CrossRef]
- Faiss, R.; Léger, B.; Vesin, J.-M.; Fournier, P.-E.; Eggel, Y.; Dériaz, O.; Millet, G.P. Significant molecular and systemic adaptations after repeated sprint training in hypoxia. PLoS ONE 2013, 8, e56522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvin, H.M.; Cooke, K.; Sumners, D.P.; Mileva, K.N.; Bowtell, J.L. Repeated sprint training in normobaric hypoxia. Br. J. Sports Med. 2013, 47, i74–i79. [Google Scholar] [CrossRef] [PubMed]
- Hamlin, M.J.; Olsen, P.D.; Marshall, H.C.; Lizamore, C.A.; Elliot, C.A. Hypoxic repeat sprint training improves rugby player’s repeated sprint but not endurance performance. Front. Physiol. 2017, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-H.; An, H.-J.; Choi, J.-H.; Kim, Y.-Y. Effects of 2-week intermittent training in hypobaric hypoxia on the aerobic energy metabolism and performance of cycling athletes with disabilities. J. Phys. Ther. Sci. 2017, 29, 1116–1120. [Google Scholar] [CrossRef] [Green Version]
- Mazzeo, R.S.; Donovan, D.; Fleshner, M.; Butterfield, G.E.; Zamudio, S.; Wolfel, E.E.; Moore, L.G. Interleukin-6 response to exercise and high-altitude exposure: Influence of α-adrenergic blockade. J. Appl. Physiol. 2001, 91, 2143–2149. [Google Scholar] [CrossRef]
- Mazzeo, R.S. Physiological responses to exercise at altitude. Sports Med. 2008, 38, 1–8. [Google Scholar] [CrossRef]
- Mazzeo, R.S.; Child, A.; Butterfield, G.E.; Braun, B.; Rock, P.B.; Wolfel, E.E.; Zamudio, S.; Moore, L.G. Sympathoadrenal responses to submaximal exercise in women after acclimatization to 4,300 meters. Metab. Clin. Exp. 2000, 49, 1036–1042. [Google Scholar] [CrossRef]
- Van Gool, J.; van Vugt, H.; Helle, M.; Aarden, L.A. The relation among stress, adrenalin, interleukin 6 and acute phase proteins in the rat. Clin. Immunol. Immunopathol. 1990, 57, 200–210. [Google Scholar] [CrossRef]
- Cohen, T.; Nahari, D.; Cerem, L.W.; Neufeld, G.; Levi, B.-Z. Interleukin 6 induces the expression of vascular endothelial growth factor. J. Biol. Chem. 1996, 271, 736–741. [Google Scholar] [CrossRef] [Green Version]
- Faquin, W.C.; Schneider, T.J.; Goldberg, M.A. Effect of inflammatory cytokines on hypoxia-induced erythropoietin production. Blood 1992, 79, 1987–1994. [Google Scholar] [CrossRef] [Green Version]
- Park, H.-Y.; Park, W.; Lim, K. Living High-Training Low for 21 Days Enhances Exercise Economy, Hemodynamic Function, and Exercise Performance of Competitive Runners. J. Sports Sci. Med. 2019, 18, 427–437. [Google Scholar]
- Serebrovskaya, T.V.; Nikolsky, I.S.; Nikolska, V.V.; Mallet, R.T.; Ishchuk, V.A. Intermittent hypoxia mobilizes hematopoietic progenitors and augments cellular and humoral elements of innate immunity in adult men. High Alt. Med. Biol. 2011, 12, 243–252. [Google Scholar] [CrossRef]
- Takahashi, H.; Asano, K.; Nakayama, H. Effect of endurance training under hypoxic condition on oxidative enzyme activity in rat skeletal muscle. Appl. Hum. Sci. 1996, 15, 111–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Miranda, M.A.; Schlater, A.E.; Green, T.L.; Kanatous, S.B. In the face of hypoxia: Myoglobin increases in response to hypoxic conditions and lipid supplementation in cultured Weddell seal skeletal muscle cells. J. Exp. Biol. 2012, 215, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Hoppeler, H.; Vogt, M.; Weibel, E.R.; Flück, M. Response of skeletal muscle mitochondria to hypoxia. Exp. Physiol. 2003, 88, 109–119. [Google Scholar] [CrossRef]
- Jaspers, R.T.; Testerink, J.; Della Gaspera, B.; Chanoine, C.; Bagowski, C.P.; van der Laarse, W.J. Increased oxidative metabolism and myoglobin expression in zebrafish muscle during chronic hypoxia. Biol. Open 2014, 3, 718–727. [Google Scholar] [CrossRef] [Green Version]
- Kurhaluk, N.; Tkachenko, H.; Nosar, V. The effects of intermittent hypoxia training on mitochondrial oxygen consumption in rats exposed to skeletal unloading. Ann. Clin. Lab. Sci. 2013, 43, 54–63. [Google Scholar]
- Brooks, G.; Wolfel, E.; Groves, B.; Bender, P.R.; Butterfield, G.; Cymerman, A.; Mazzeo, R.; Sutton, J.; Wolfe, R.; Reeves, J. Muscle accounts for glucose disposal but not blood lactate appearance during exercise after acclimatization to 4300 m. J. Appl. Physiol. 1992, 72, 2435–2445. [Google Scholar] [CrossRef]
- Park, H.-Y.; Shin, C.; Lim, K. Intermittent hypoxic training for 6 weeks in 3000 m hypobaric hypoxia conditions enhances exercise economy and aerobic exercise performance in moderately trained swimmers. Biol. Sport 2018, 35, 49. [Google Scholar] [CrossRef]
- Lühker, O.; Berger, M.M.; Pohlmann, A.; Hotz, L.; Gruhlke, T.; Hochreiter, M. Changes in acid–base and ion balance during exercise in normoxia and normobaric hypoxia. Eur. J. Appl. Physiol. 2017, 117, 2251–2261. [Google Scholar] [CrossRef]
- Moon, H.-W.; Shin, S.-H.; Lee, C.-H.; Park, H.-Y.; Sunoo, S.; Nam, S.-S. Effects of various acute hypoxic conditions on the hemorheological response during exercise and recovery 1. Clin. Hemorheol. Microcirc. 2016, 63, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Płoszczyca, K.; Langfort, J.; Czuba, M. The effects of altitude training on erythropoietic response and hematological variables in adult athletes: A narrative review. Front. Physiol. 2018, 9, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Povea, C.; Schmitt, L.; Brugniaux, J.; Nicolet, G.; Richalet, J.-P.; Fouillot, J.-P. Effects of intermittent hypoxia on heart rate variability during rest and exercise. High Alt. Med. Biol. 2005, 6, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Taralov, Z.; Terziyski, K.; Dimov, P.; Marinov, B.; Tarvainen, M.P.; Perini, R.; Kostianev, S. Assessment of the acute impact of normobaric hypoxia as a part of an intermittent hypoxic training on heart rate variability. Cor et Vasa 2015, 57, e251–e256. [Google Scholar] [CrossRef] [Green Version]
- Kjaer, M.; Bangsbo, J.; Lortie, G.; Galbo, H. Hormonal response to exercise in humans: Influence of hypoxia and physical training. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1988, 254, R197–R203. [Google Scholar] [CrossRef]
- Madanecki, P.; Kapoor, N.; Bebok, Z.; Ochocka, R.; Collawn, J.; Bartoszewski, R. Regulation of angiogenesis by hypoxia: The role of microRNA. Cell. Mol. Biol. Lett. 2013, 18, 47–57. [Google Scholar] [CrossRef] [Green Version]
- Nunomiya, A.; Shin, J.; Kitajima, Y.; Dan, T.; Miyata, T.; Nagatomi, R. Activation of the hypoxia-inducible factor pathway induced by prolyl hydroxylase domain 2 deficiency enhances the effect of running training in mice. Acta Physiol. 2017, 220, 99–112. [Google Scholar] [CrossRef]
- Park, H.; Lim, K. The effect of high-intensity aerobic continuous and anaerobic interval training at 3,000 m hypobaric hypoxic condition for six-weeks on aerobic and anaerobic exercise capacity in competitive swimmers. Korean J. Sport Sci. 2017, 28, 241–249. [Google Scholar] [CrossRef]
- Park, H.-Y.; Sunoo, S.; Nam, S.-S. The effect of 4 weeks fixed and mixed intermittent hypoxic training (IHT) on respiratory metabolic and acid-base response of capillary blood during submaximal bicycle exercise in male elite taekwondo players. J. Exerc. Nutr. Biochem. 2016, 20, 35. [Google Scholar] [CrossRef]
- Gore, C.J.; Sharpe, K.; Garvican-Lewis, L.A.; Saunders, P.U.; Humberstone, C.E.; Robertson, E.Y.; Wachsmuth, N.B.; Clark, S.A.; McLean, B.D.; Friedmann-Bette, B. Altitude training and haemoglobin mass from the optimised carbon monoxide rebreathing method determined by a meta-analysis. Br. J. Sports Med. 2013, 47, i31–i39. [Google Scholar] [CrossRef]
- Gore, C.J.; Rodríguez, F.A.; Truijens, M.J.; Townsend, N.E.; Stray-Gundersen, J.; Levine, B.D. Increased serum erythropoietin but not red cell production after 4 wk of intermittent hypobaric hypoxia (4000–5500 m). J. Appl. Physiol. 2006, 101, 1386–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, R.-L.; Witkowski, S.; Zhang, Y.; Alfrey, C.; Sivieri, M.; Karlsen, T.; Resaland, G.K.; Harber, M.; Stray-Gundersen, J.; Levine, B. Determinants of erythropoietin release in response to short-term hypobaric hypoxia. J. Appl. Phys. 2002, 92, 2361–2367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, G.; Tschöp, M.; Fischer, R.; Bidlingmaier, C.; Riepl, R.; Tschöp, K.; Hautmann, H.; Endres, S.; Toepfer, M. High altitude increases circulating interleukin-6, interleukin-1 receptor antagonist and C-reactive protein. Cytokine 2000, 12, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Steensberg, A. Exercise and hypoxia: Effects on leukocytes and interleukin-6—shared mechanisms? Med. Sci. Sports Exerc. 2002, 34, 2004–2012. [Google Scholar] [CrossRef]
- Pyne, D.B.; McDonald, W.A.; Morton, D.S.; Swiggett, J.P.; Foster, M.; Sonnenfeld, G.; Smith, J.A. Inhibition of interferon, cytokine, and lymphocyte proliferative responses in elite swimmers with altitude exposure. J. Interferon Cytokine Res. 2000, 20, 411–418. [Google Scholar] [CrossRef]
- Tiollier, E.; Schmitt, L.; Burnat, P.; Fouillot, J.P.; Robach, P.; Filaire, E.; Guezennec, C.; Richalet, J.P. Living high-training low altitude training: Effects on mucosal immunity. Eur. J. Appl. Physiol. 2005, 94, 298–304. [Google Scholar] [CrossRef]
- Brugniaux, J.V.; Schmitt, L.; Robach, P.; Jeanvoine, H.; Zimmermann, H.; Nicolet, G.; Duvallet, A.; Fouillot, J.P.; Richalet, J.P. Living high-training low: Tolerance and acclimatization in elite endurance athletes. Eur. J. Appl. Physiol. 2006, 96, 66–77. [Google Scholar] [CrossRef]
- Hogan, S.P.; Rosenberg, H.F.; Moqbel, R.; Phipps, S.; Foster, P.S.; Lacy, P.; Kay, A.B.; Rothenberg, M.E. Eosinophils: Biological properties and role in health and disease. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2008, 38, 709–750. [Google Scholar] [CrossRef]
- Horiuchi, T.; Weller, P.F. Expression of vascular endothelial growth factor by human eosinophils: Upregulation by granulocyte macrophage colony-stimulating factor and interleukin-5. Am. J. Respir. Cell mol. biol. 1997, 17, 70–77. [Google Scholar] [CrossRef]
- Rothenberg, M.E.; Hogan, S.P. The eosinophil. Ann. Rev. Immunol. 2006, 24, 147–174. [Google Scholar] [CrossRef]
- Iannello, A.; Debbeche, O.; Samarani, S.; Ahmad, A. Antiviral NK cell responses in HIV infection: I. NK cell receptor genes as determinants of HIV resistance and progression to AIDS. J. Leukocyte Biol. 2008, 84, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.; Weaver, C. Janeway’s Immunobiology; Garland Science: New York, NY, USA, 2016. [Google Scholar]
- Yanaba, K.; Bouaziz, J.D.; Matsushita, T.; Magro, C.M.; St Clair, E.W.; Tedder, T.F. B-lymphocyte contributions to human autoimmune disease. Immunol. Rev. 2008, 223, 284–299. [Google Scholar] [CrossRef] [PubMed]
- Alberts, B.; Johnson, A.; Lewis, J.; Raff, M.; Roberts, K.; Walter, P. Molecular Biology of the Cell 4th edn (New York: Garland Science). Ann. Bot. 2002, 91, 401. [Google Scholar]
- Koch, S.; Larbi, A.; Derhovanessian, E.; Özcelik, D.; Naumova, E.; Pawelec, G. Multiparameter flow cytometric analysis of CD4 and CD8 T cell subsets in young and old people. Immun. Ageing 2008, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Before Training | After Training | p-Value |
|---|---|---|---|
| Number (n) | 6 (two blind athletes, one male and one female; two blind pilots, one male and one female; one cognitively-impaired male athlete; and one male athlete with a spinal cord disability) | ||
| Environmental conditions (mmHg) | Week 1, 596 (simulated altitude: 2000 m); Week 2, 526 (simulated altitude: 3000 m). | ||
| Age (years) | 40.67 ± 8.36 | ||
| SBP (mmHg) | 131.33 ± 11.67 | 137.17 ± 18.26 | 0.553 |
| DBP (mmHg) | 77.67 ± 7.69 | 69.37 ± 11.03 | 0.427 |
| Weight (kg) | 69.37 ± 11.03 | 68.70 ± 11.61 | 0.340 |
| FFM (kg) | 46.70 ± 12.23 | 49.27 ± 13.63 | 0.104 |
| % Body fat | 29.35 ± 10.38 | 28.57 ± 9.31 | 0.505 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-Y.; Jung, W.-S.; Kim, J.; Hwang, H.; Kim, S.-W.; An, Y.; Lee, H.; Jeon, S.; Lim, K. Effects of 2-Week Exercise Training in Hypobaric Hypoxic Conditions on Exercise Performance and Immune Function in Korean National Cycling Athletes with Disabilities: A Case Report. Int. J. Environ. Res. Public Health 2020, 17, 861. https://doi.org/10.3390/ijerph17030861
Park H-Y, Jung W-S, Kim J, Hwang H, Kim S-W, An Y, Lee H, Jeon S, Lim K. Effects of 2-Week Exercise Training in Hypobaric Hypoxic Conditions on Exercise Performance and Immune Function in Korean National Cycling Athletes with Disabilities: A Case Report. International Journal of Environmental Research and Public Health. 2020; 17(3):861. https://doi.org/10.3390/ijerph17030861
Chicago/Turabian StylePark, Hun-Young, Won-Sang Jung, Jisu Kim, Hyejung Hwang, Sung-Woo Kim, Younghwan An, Haeman Lee, Seonju Jeon, and Kiwon Lim. 2020. "Effects of 2-Week Exercise Training in Hypobaric Hypoxic Conditions on Exercise Performance and Immune Function in Korean National Cycling Athletes with Disabilities: A Case Report" International Journal of Environmental Research and Public Health 17, no. 3: 861. https://doi.org/10.3390/ijerph17030861
APA StylePark, H. -Y., Jung, W. -S., Kim, J., Hwang, H., Kim, S. -W., An, Y., Lee, H., Jeon, S., & Lim, K. (2020). Effects of 2-Week Exercise Training in Hypobaric Hypoxic Conditions on Exercise Performance and Immune Function in Korean National Cycling Athletes with Disabilities: A Case Report. International Journal of Environmental Research and Public Health, 17(3), 861. https://doi.org/10.3390/ijerph17030861