A Cohort Study of Exposure to Antihyperglycemic Therapy and Survival in Patients with Lung Cancer


Abstract
:1. Introduction
2. Methods
2.1. Data Sources & Study Design
2.2. Exposure Definition
2.3. Outcomes
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Cohort
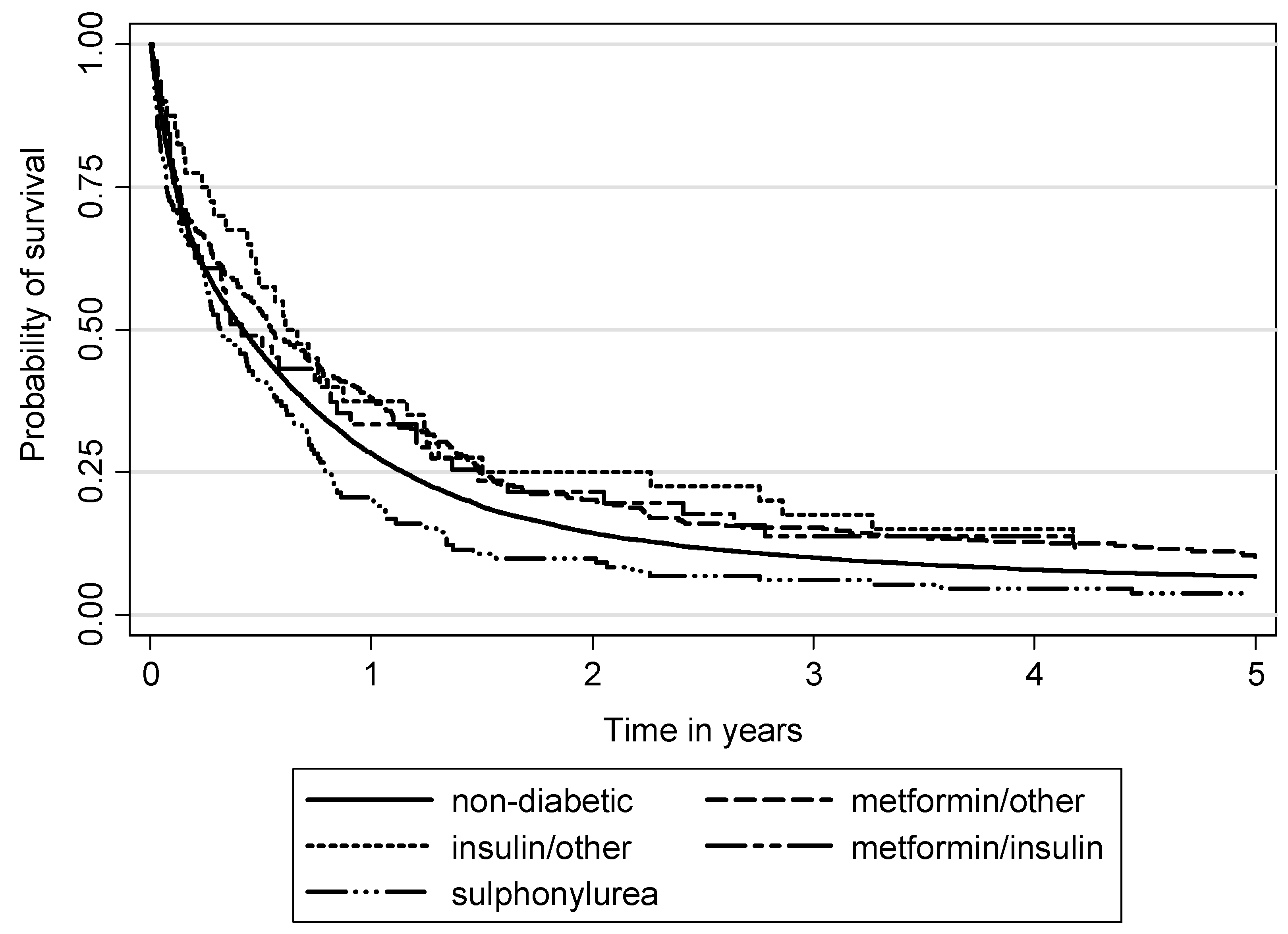
3.2. Survival Analyses: Lung Cancer-Specific and Overall Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethics Statement
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Kozielski, J.; Kaczmarczyk, G.; Porębska, I.; Szmygin-Milanowska, K.; Gołecki, M. Lung cancer in patients under the age of 40 years. Contemp. Oncol. 2012, 16, 413–415. [Google Scholar] [CrossRef]
- Leduc, C.; Antoni, D.; Charloux, A.; Falcoz, P.E.; Quoix, E. Comorbidities in the management of patients with lung cancer. Eur. Respir. J. 2017, 49, 1601721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandfeld-Paulsen, B.; Meldgaard, P.; Aggerholm-Pedersen, N. Comorbidity in lung cancer: A prospective cohort study of self-reported versus register-based comorbidity. J. Thorac. Oncol. 2017, 13, 54–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, G.; Rui, W.; Grouse, L. Diabetes mellitus increases postoperative mortality in non-small cell lung cancer. Thorac. Cancer 2014, 5, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciacca, L.; Vigneri, R.; Tumminia, A.; Frasca, F.; Squatrito, S.; Frittitta, L.; Vigneri, P. Clinical and molecular mechanisms favoring cancer initiation and progression in diabetic patients. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 808–815. [Google Scholar] [CrossRef]
- Melkonian, S.C.; Daniel, C.R.; Ye, Y.; Pierzynski, J.A.; Roth, J.A.; Wu, X. Glycemic index, glycemic load, and lung cancer risk in non-hispanic whites. Cancer Epidemiol. Biomark. Prev. 2016, 25, 532–539. [Google Scholar] [CrossRef] [Green Version]
- Ding, C.-Z.; Guo, X.-F.; Wang, G.-L.; Wang, H.T.; Xu, G.H.; Liu, Y.Y.; Wu, Z.J.; Chen, Y.H.; Wang, J.; Wang, W.G. High glucose contributes to the proliferation and migration of non-small-cell lung cancer cells via GAS5-TRIB3 axis. Biosci. Rep. 2018, 38, BSR20171014. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Chlebowski, R.; Wactawski-Wende, J.; Schlecht, N.F.; Tinker, L.; Margolis, K.L. Diabetes and lung cancer among postmenopausal women. Diabetes Care 2012, 35, 1485–1491. [Google Scholar] [CrossRef] [Green Version]
- Xin, W.X.; Fang, L.; Fang, Q.L.; Zheng, X.W.; Ding, H.Y.; Huang, P. Effect of hypoglycemic agents on survival outcomes of lung cancer patients with diabetes mellitus. A meta-analysis. Medicine 2018, 97, e0035. [Google Scholar] [CrossRef]
- Hatlen, P.; Grønberg, B.H.; Langhammer, A.; Carlsen, S.M.; Amundsen, T. Prolonged survival in patients with lung cancer with diabetes mellitus. J. Thorac. Oncol. 2011, 6, 1810–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.-S.; Yang, Y.; Yang, G.; Chow, W.-H.; Li, H.-L.; Gao, Y.-T.; Ji, B.-T.; Rothman, N.; Zheng, W.; Shu, X.-O.; et al. Pre-existing type 2 diabetes and risk of lung cancer: A report from two prospective cohort studies of 133 024 Chinese adults in urban Shanghai. BMJ Open 2014, 4, e004875. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Cao, H.; Zhang, T.; Shen, H.; Dong, W.; Wang, L.; Du, J. The effect of diabetes mellitus on lung cancer prognosis: A PRISMA-compliant meta-analysis of cohort studies. Medicine 2016, 95, e3528. [Google Scholar] [CrossRef] [PubMed]
- Karlin, N.J.; Amin, S.B.; Buras, M.R.; Kosiorek, H.E.; Verona, P.M.; Cook, C.B. Patient outcomes from lung cancer and diabetes mellitus: A matched case-control study. Future Sci. OA 2017, 4, FSO248. [Google Scholar] [CrossRef] [Green Version]
- Kinaan, M.; Ding, H.; Triggle, C.R. Metformin: An old drug for the treatment of diabetes but a new drug for the protection of the endothelium. Med. Princ. Pract. 2015, 24, 401–415. [Google Scholar] [CrossRef]
- Xu, T.; Li, D.; He, Y.; Zhang, F.; Qiao, M.; Chen, Y. Prognostic value of metformin for non-small cell lung cancer patients with diabetes. World J. Surg. Oncol. 2018, 16, 60. [Google Scholar] [CrossRef] [Green Version]
- Chuang, M.C.; Yang, Y.H.; Tsai, Y.H.; Hsieh, M.J.; Lin, Y.C.; Lin, C.K.; Chen, P.C.; Yang, T.M. Survival benefit associated with metformin use in inoperable non-small cell lung cancer patients with diabetes: A population-based retrospective cohort study. PLoS ONE 2018, 13, e0191129. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Hendryx, M.; Qi, L.; Ho, G.Y.; Margolis, K.L. Pre-existing diabetes and lung cancer prognosis. Br. J. Cancer 2016, 115, 76–79. [Google Scholar] [CrossRef] [Green Version]
- Menamin, Ú.C.; Cardwell, C.R.; Hughes, C.M.; Murray, L.M. Metformin use and survival from lung cancer: A population-based cohort study. Lung Cancer 2016, 94, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.J.; Gallagher, E.J.; Sigel, K.; Mhango, G.; Galsky, M.D.; Smith, C.B.; LeRoith, D.; Wisnivesky, J.P. Survival of patients with stage IV lung cancer with diabetes treated with metformin. Am. J. Respir. Crit. Care Med. 2015, 191, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.C.-H. Changing advanced lung cancer into chronic disease. Lung Cancer Manag. 2014, 3, 23–28. [Google Scholar] [CrossRef]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, K.M.; Jiang, X.; Anggondowati, T.; Lin, G.; Ganti, A.K. Comorbidity and survival in lung cancer patients. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1079–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.J.; Yu, D.; Wen, W.; Saito, E.; Rahman, S.; Shu, X.O.; Chen, Y.; Gupta, P.C.; Gu, D.; Tsugane, S.; et al. Association of diabetes with all-cause and cause-specific mortality in Asia. A pooled analysis of more than 1 million participants. JAMA Network Open 2019, 2, e192696. [Google Scholar] [CrossRef]
- Gomes, M.B.; Rathmann, W.; Charbonnel, B.; Khunti, K.; Kosiborod, M.; Nicolucci, A.; Pocock, S.J.; Shestakova, M.V.; Shimomura, I.; Tang, F.; et al. Treatment of type 2 diabetes mellitus worldwide: Baseline patient characteristics in the global DISCOVER study. Diabetes Res. Clin. Pract. 2019, 151, 20–32. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Colombet, M.; Bray, F. Cancer Incidence in Five Continents, CI5plus: IARC Cancer Base No. 9; International Agency for Research on Cancer: Lyon, France, 2018; Available online: http://ci5.iarc.fr (accessed on 3 March 2020).
- Inzucchi, S.E.; Bergensta, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycemia in type 2 diabetes, 2015: A patient-centered approach: Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015, 38, 140. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.D.; Park, K.G.; Lee, Y.S.; Park, Y.Y.; Kim, D.K.; Nedumaran, B.; Jang, W.G.; Cho, W.J.; Ha, J.; Lee, I.K.; et al. Metformin inhibits hepatic gluconeogenesis through AMP activated protein kinase-dependent regulation of the orphan nuclear receptor SHP. Diabetes 2008, 57, 306–314. [Google Scholar] [CrossRef] [Green Version]
- Rena, G.; Pearson, E.R.; Sakamoto, K. Molecular mechanism of action of metformin: Old or new insights? Diabetologia 2013, 56, 1898–1906. [Google Scholar] [CrossRef] [Green Version]
- Bulcao, C.; Ribeiro-Filho, F.F.; Sanudo, A.; Roberta Ferreira, SG. Effects of simvastatin and metformin on inflammation and insulin resistance in individuals with mild metabolic syndrome. Am. J. Cardiovasc. Drugs 2007, 7, 219–224. [Google Scholar] [CrossRef]
- Memmott, R.M.; Mercado, J.R.; Maier, C.R.; Kawabata, S.; Fox, S.D.; Dennis, P.A. Metformin prevents tobacco carcinogen-induced lung tumorigenesis. Cancer Prev. Res. 2010, 3, 1066–1076. [Google Scholar] [CrossRef] [Green Version]
- Arrieta, O.; Varela-Santoyo, E.; Soto-Perez-de-Celis, E.; Sánchez-Reyes, R.; De la Torre-Vallejo, M.; Muñiz-Hernández, S.; Cardona, A.F. Metformin use and its effect on survival in diabetic patients with advanced non-small cell lung cancer. BMC Cancer 2016, 16, 633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Liang, G.; Yang, L.; Zhang, F. Prognosis of small cell lung cancer patients with diabetes treated with metformin. Clin. Transl. Oncol. 2015, 17, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-H. Metformin and lung cancer risk in patients with type 2 diabetes mellitus. Oncotarget 2017, 8, 41132–41142. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.X.; Yao, W.X.; Ge, J.; Peng, X.C.; Du, X.B.; Zhang, R.; Yao, B.; Xie, K.; Li, L.H.; Dong, H.; et al. Prognostic influence of metformin as first-line chemotherapy for advanced nonsmall cell lung cancer in patients with type 2 diabetes. Cancer 2011, 117, 5103–5111. [Google Scholar] [CrossRef]
- Wan, G.; Yu, X.; Chen, P.; Wang, X.; Pan, D.; Wang, X.; Li, L.; Cai, X.; Cao, F. Metformin therapy associated with survival benefit in lung cancer patients with diabetes. Oncotarget 2016, 7, 35437–35445. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Yao, W.; Chu, Q.; Han, R.; Wang, Y.; Sun, J.; Wang, D.; Wang, Y.; Cao, M.; He, Y. Synergistic effects of metformin in combination with EGFR-TKI in the treatment of patients with advanced non-small cell lung cancer and type 2 diabetes. Cancer Lett. 2015, 369, 97–102. [Google Scholar] [CrossRef]
- Kong, F.; Gao, F.; Liu, H.; Chen, L.; Zheng, R.; Yu, J.; Li, X.; Liu, G.; Jia, Y. Metformin use improves the survival of diabetic combined small-cell lung cancer patients. Tumour Biol. 2015, 36, 8101–8106. [Google Scholar] [CrossRef]
- Tian, R.H.; Zhang, Y.G.; Wu, Z.; Liu, X.; Yang, J.W.; Ji, H.L. Effects of metformin on survival outcomes of lung cancer patients with type 2 diabetes mellitus: A meta-analysis. Clin. Transl. Oncol. 2016, 18, 641–649. [Google Scholar] [CrossRef]
- Wink, K.C.; Belderbos, J.S.; Dieleman, E.M.; Rossi, M.; Rasch, C.R.; Damhuis, R.A.; Houben, R.M.; Troost, E.G. Improved progression free survival for patients with diabetes and locally advanced non-small cell lung cancer (NSCLC) using metformin during concurrent chemoradiotherapy. Radiother. Oncol. 2016, 118, 453–459. [Google Scholar] [CrossRef]
- Storozhuk, Y.; Hopmans, S.N.; Sanli, T.; Barron, C.; Tsiani, E.; Cutz, J.C.; Pond, G.; Wright, J.; Singh, G.; Tsakiridis, T. Metformin inhibits growth and enhances radiation response of non-small cell lung cancer (NSCLC) through ATM and AMPK. Br. J. Cancer 2013, 108, 2021–2032. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Li, G.; Wang, Y.; Tang, S.; Sun, X.; Feng, X.; Li, Y.; Bao, G.; Li, P.; Mao, X.; et al. Suppression of tumor angiogenesis by metformin treatment via a mechanism linked to targeting of HER2/HIF-1α/VEGF secretion axis. Oncotarget 2015, 6, 44579–44592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Han, R.; Xiao, H.; Lin, C.; Wang, Y.; Liu, H.; Li, K.; Chen, H.; Sun, F.; Yang, Z.; et al. Metformin sensitizes EGFR-TKI-resistant human lung cancer cells in vitro and in vivo through inhibition of IL-6 signaling and EMT reversal. Clin. Cancer Res. 2014, 20, 2714–2726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, S.F.; Guimarães Idos, S.; Madeira, K.P.; Daltoé, R.D.; Silva, I.V.; Rangel, L.B. Metformin synergistically enhances antiproliferative effects of cisplatin and etoposide in NCI-H460 human lung cancer cells. J. Bras. Pneumol. 2013, 39, 644–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgillo, F.; Sasso, F.C.; Della Corte, C.M.; Vitagliano, D.; D’Aiuto, E.; Troiani, T.; Martinelli, E.; De Vita, F.; Orditura, M.; De Palma, R.; et al. Synergistic effects of metformin treatment in combination with gefitinib, a selective EGFR tyrosine kinase inhibitor, in LKB1 wild-type NSCLC cell lines. Clin. Cancer Res. 2013, 19, 3508–3519. [Google Scholar] [CrossRef] [Green Version]
- Uehara, T.; Mitsuhashi, A.; Tsuruoka, N.; Shozu, M. Metformin potentiates the anticancer effects of cisplatin under normoxic conditions in vitro. Oncol. Rep. 2015, 33, 744–750. [Google Scholar] [CrossRef] [Green Version]
- Landman, G.W.D.; Kleefstra, N.; van Hateren, K.J.J.; Groenier, K.H.; Gans, R.O.; Bilo, H.J. Metformin associated with lower cancer mortality in type 2 diabetes: ZODIAC-16. Diabetes Care 2010, 33, 322–326. [Google Scholar] [CrossRef] [Green Version]
- Medairos, R.A.; Clark, J.; Holoubek, S.; Kubasiak, J.C.; Pithadia, R.; Hamid, F.; Chmielewski, G.W.; Warren, W.H.; Basu, S.; Borgia, J.A.; et al. Metformin exposure is associated with improved progression-free survival in diabetic patients after resection for early-stage non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2016, 152, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Owen, M.R.; Doran, E.; Halestrap, A.P. Evidence that metformin exerts its antidiabetic effects through inhibition of complex I of the mitochon- drial respiratory chain. Biochem. J. 2000, 348, 607–614. [Google Scholar] [CrossRef]
- Levy, A.; Doyen, J. Metformin for non-small cell lung cancer patients: Opportunities and pitfalls. Crit. Rev. Oncol. Hematol. 2018, 125, 41–47. [Google Scholar] [CrossRef]
- Ioacara, S.; Guja, C.; Ionescu-Tirgoviste, C.; Fica, S.; Roden, M. Cancer specific mortality in insulin-treated type 2 diabetes patients. PLoS ONE 2014, 9, e93132. [Google Scholar] [CrossRef]
- Tseng, C.H. Higher risk of mortality from lung cancer in Taiwanese people with diabetes. Diabetes Res. Clin. Pract. 2013, 102, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, C.M.; Emanuelli, B.; Kahn, C.R. Critical nodes in signalling pathways: Insights into insulin action. Nat. Rev. Mol. Cell Biol. 2006, 7, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Sciacca, L.; Le Moli, R.; Vigneri, R. Insulin analogs and cancer. Front. Endocrinol. 2012, 3, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronsveld, H.K.; Ter Braak, B.; Karlstad, O.; Vestergaard, P.; Starup-Linde, J.; Bazelier, M.T.; De Bruin, M.L.; de Boer, A.; Siezen, C.L.; van de Water, B.; et al. Treatment with insulin (analogues) and breast cancer risk in diabetics; a systematic review and meta-analysis of in vitro, animal and human evidence. Breast Cancer Res. 2015, 17, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.W.; Filion, K.B.; Azoulay, L.; Doll, M.K.; Suissa, S. Effect of Long-Acting Insulin Analogs on the Risk of Cancer: A Systematic Review of Observational Studies. Diabetes Care 2016, 39, 486–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordeleau, L.; Yakubovich, N.; Dagenais, G.R.; Rosenstock, J.; Probstfield, J.; Chang Yu, P.; Ryden, L.E.; Pirags, V.; Spinas, G.A.; Birkeland, K.I.; et al. The association of basal insulin glargine and/or n-3 fatty acids with incident cancers in patients with dysglycemia. Diabetes Care 2014, 37, 1360–1366. [Google Scholar] [CrossRef] [Green Version]
- Investigators, O.R.I.G.I.N.T. Basal insulin and cardiovascular and other outcomes in dysglycemia. N. Engl. J. Med. 2012, 367, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Yeo, C.D.; Park, K.H.; Park, C.K.; Lee, S.H.; Kim, S.J.; Yoon, H.K.; Lee, Y.S.; Lee, E.J.; Lee, K.Y.; Kim, T.J. Expression of insulin-like growth factor 1 receptor (IGF-1R) predicts poor responses to epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors in non-small cell lung cancer patients harboring activating EGFR mutations. Lung Cancer 2015, 87, 311–317. [Google Scholar] [CrossRef]
- Kim, J.S.; Kim, E.S.; Liu, D.; Lee, J.J.; Solis, L.; Behrens, C.; Lippman, S.M.; Hong, W.K.; Wistuba, I.I.; Lee, H.Y. Prognostic impact of insulin receptor expression on survival of patients with nonsmall cell lung cancer. Cancer 2012, 118, 2454–2465. [Google Scholar] [CrossRef] [Green Version]
- Mathieu, M.C.; Clark, G.M.; Allred, D.C.; Goldfine, I.D.; Vigneri, R. Insulin receptor expression and clinical outcome in node-negative breast cancer. Proc. Assoc. Am. Phys. 1997, 109, 565–571. [Google Scholar]
- Law, J.H.; Habibi, G.; Hu, K.; Masoudi, H.; Wang, M.Y.; Stratford, A.L.; Park, E.; Gee, J.M.; Finlay, P.; Jones, H.E.; et al. Phosphorylated insulin-like growth factor-i/insulin receptor is present in all breast cancer subtypes and is related to poor survival. Cancer Res. 2008, 68, 10238–10246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciacca, L.; Cassarino, M.F.; Genua, M.; Vigneri, P.; Giovanna Pennisi, M.; Malandrino, P.; Squatrito, S.; Pezzino, V.; Vigneri, R. Biological effects of insulin and its analogs on cancer cells with different insulin family receptor expression. J. Cell. Physiol. 2014, 229, 1817–1821. [Google Scholar] [CrossRef] [PubMed]
- Vigneri, R.; Goldfine, I.D.; Frittitta, L. Insulin, insulin receptors, and cancer. J. Endocrinol. Investig. 2016, 39, 1365–1376. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non Diabetic | Metformin and Other Medication Users | Insulin and Other Medication Users | Metformin and Insulin Users | Sulphonylurea Users | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | |
| Total | 15,394 | 100.0 | 313 | 100.0 | 40 | 100.0 | 51 | 100.0 | 131 | 100.0 |
| Sex | ||||||||||
| Male | 12,943 | 84.1 | 222 | 70.9 | 34 | 85.0 | 35 | 68.6 | 95 | 72.5 |
| Female | 2451 | 15.9 | 91 | 29.1 | 6 | 15.0 | 16 | 31.4 | 36 | 27.5 |
| Age at diagnosis | ||||||||||
| <60 | 4010 | 26.0 | 53 | 16.9 | 6 | 15.0 | 3 | 5.9 | 13 | 9.9 |
| 60–69 | 5315 | 34.5 | 123 | 39.3 | 18 | 45.0 | 17 | 33.3 | 39 | 29.8 |
| 70–79 | 4663 | 30.3 | 103 | 32.9 | 15 | 37.5 | 26 | 51.0 | 58 | 44.3 |
| 80+ | 1406 | 9.2 | 34 | 10.9 | 1 | 2.5 | 5 | 9.8 | 21 | 16.0 |
| TNM stage | ||||||||||
| I | 1136 | 7.4 | 22 | 7.0 | 4 | 10.0 | 3 | 5.9 | 9 | 6.9 |
| II | 2004 | 13.0 | 37 | 11.8 | 8 | 20.0 | 8 | 15.7 | 23 | 17.6 |
| III | 4876 | 31.7 | 91 | 29.1 | 11 | 27.5 | 13 | 25.5 | 37 | 28.2 |
| IV | 5591 | 36.3 | 113 | 36.1 | 11 | 27.5 | 13 | 25.5 | 40 | 30.5 |
| Missing | 1787 | 11.6 | 50 | 16.0 | 6 | 15.0 | 14 | 27.5 | 22 | 16.8 |
| Histological group | ||||||||||
| Squamous cell Ca | 1837 | 11.9 | 36 | 11.5 | 4 | 10.0 | 3 | 5.9 | 13 | 9.9 |
| Adenocarcinoma | 4576 | 29.7 | 76 | 24.3 | 11 | 27.5 | 16 | 31.4 | 31 | 23.7 |
| Small cell Ca | 2411 | 15.7 | 57 | 18.2 | 8 | 20.0 | 7 | 13.7 | 25 | 19.1 |
| Other | 1902 | 12.4 | 34 | 10.9 | 4 | 10.0 | 6 | 11.8 | 10 | 7.6 |
| Unspecified | 4668 | 30.3 | 110 | 35.1 | 13 | 32.5 | 19 | 37.2 | 52 | 39.7 |
| Variable | Multivariate-Adjusted HR † (95% CI) | p-Value |
|---|---|---|
| Sex | ||
| Male | 1.00 | ref. |
| Female | 0.75 (0.71-0.78) | <0.001 |
| Age at diagnosis | ||
| <60 | 1.00 | ref. |
| 60–69 | 1.20 (0.14–1.25) | <0.001 |
| 70–79 | 1.34 (1.28–1.40) | <0.001 |
| 80+ | 1.35 (1.26–1.45) | <0.001 |
| TNM stage | ||
| I | 1.00 | ref. |
| II | 1.61 (1.47–1.76) | <0.001 |
| III | 2.82 (2.61–3.06) | <0.001 |
| IV | 4.68 (4.32–5.07) | <0.001 |
| Missing | 2.67 (2.44–2.93) | <0.001 |
| Histological group | ||
| Squamous cell Ca | 1.00 | ref. |
| Adenocarcinoma | 0.94 (0.88–0.99) | 0.024 |
| Small cell Ca | 0.88 (0.83–0.94) | <0.001 |
| Other | 1.00 (0.93–1.07) | 0.923 |
| Unspecified | 1.27 (1.19–1.34) | <0.001 |
| Diabetes | ||
| Non diabetic | 1.00 | ref. |
| Metformin and other medication users | 0.82 (0.72–0.92) | 0.001 |
| Insulin and other medication users | 0.65 (0.44–0.95) | 0.026 |
| Metformin and insulin users | 0.84 (0.61–1.16) | 0.283 |
| Sulphonylurea users | 1.19 (0.99–1.43) | 0.060 |
| Variable | Multivariate-Adjusted HR † (95% CI) | p-Value |
|---|---|---|
| Sex | ||
| Male | 1.00 | ref. |
| Female | 0.75 (0.72–0.78) | <0.001 |
| Age at diagnosis | ||
| <60 | 1.00 | ref. |
| 60–69 | 1.22 (1.17–1.27) | <0.001 |
| 70–79 | 1.39 (1.33–1.45) | <0.001 |
| 80+ | 1.49 (1.39–1.59) | <0.001 |
| TNM stage | ||
| I | 1.00 | ref. |
| II | 1.52 (1.41–1.65) | <0.001 |
| III | 2.52 (2.34–2.70) | <0.001 |
| IV | 4.09 (3.80–4.39) | <0.001 |
| Missing | 2.42 (2.23–2.63) | <0.001 |
| Histological group | ||
| Squamous cell Ca | 1.00 | ref. |
| Adenocarcinoma | 0.92 (0.88–0.98) | 0.006 |
| Small cell Ca | 0.89 (0.83–0.94) | <0.001 |
| Other | 0.98 (0.92–1.05) | 0.556 |
| Unspecified | 1.32 (1.24–1.39) | <0.001 |
| Diabetes | ||
| Non diabetic | 1.00 | ref. |
| Metformin and other medication users | 0.82 (0.73–0.92) | 0.001 |
| Insulin and other medication users | 0.85 (0.62–1.16) | 0.299 |
| Metformin and insulin users | 0.93 (0.70–1.16) | 0.614 |
| Sulphonylurea users | 1.22 (1.03–1.45) | 0.023 |
| Cumulative Dose (mg) | Lung Cancer Specific Mortality HR † (95% CI) | p-Value | Overall Mortality HR † (95% CI) | p-Value |
|---|---|---|---|---|
| <360,000 | 1.00 | ref. | 1.00 | ref. |
| 360,000–1,300,000 | 0.61 (0.44–0.84) | 0.003 | 0.74 (0.54–1.02) | 0.07 |
| >1,300,000 | 1.05 (0.66–1.71) | 0.82 | 1.03 (0.64–1.66) | 0.91 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danila, E.; Linkevičiūtė-Ulinskienė, D.; Zablockis, R.; Gruslys, V.; Cicėnas, S.; Smailytė, G. A Cohort Study of Exposure to Antihyperglycemic Therapy and Survival in Patients with Lung Cancer. Int. J. Environ. Res. Public Health 2020, 17, 1747. https://doi.org/10.3390/ijerph17051747
Danila E, Linkevičiūtė-Ulinskienė D, Zablockis R, Gruslys V, Cicėnas S, Smailytė G. A Cohort Study of Exposure to Antihyperglycemic Therapy and Survival in Patients with Lung Cancer. International Journal of Environmental Research and Public Health. 2020; 17(5):1747. https://doi.org/10.3390/ijerph17051747
Chicago/Turabian StyleDanila, Edvardas, Donata Linkevičiūtė-Ulinskienė, Rolandas Zablockis, Vygantas Gruslys, Saulius Cicėnas, and Giedrė Smailytė. 2020. "A Cohort Study of Exposure to Antihyperglycemic Therapy and Survival in Patients with Lung Cancer" International Journal of Environmental Research and Public Health 17, no. 5: 1747. https://doi.org/10.3390/ijerph17051747
APA StyleDanila, E., Linkevičiūtė-Ulinskienė, D., Zablockis, R., Gruslys, V., Cicėnas, S., & Smailytė, G. (2020). A Cohort Study of Exposure to Antihyperglycemic Therapy and Survival in Patients with Lung Cancer. International Journal of Environmental Research and Public Health, 17(5), 1747. https://doi.org/10.3390/ijerph17051747