High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
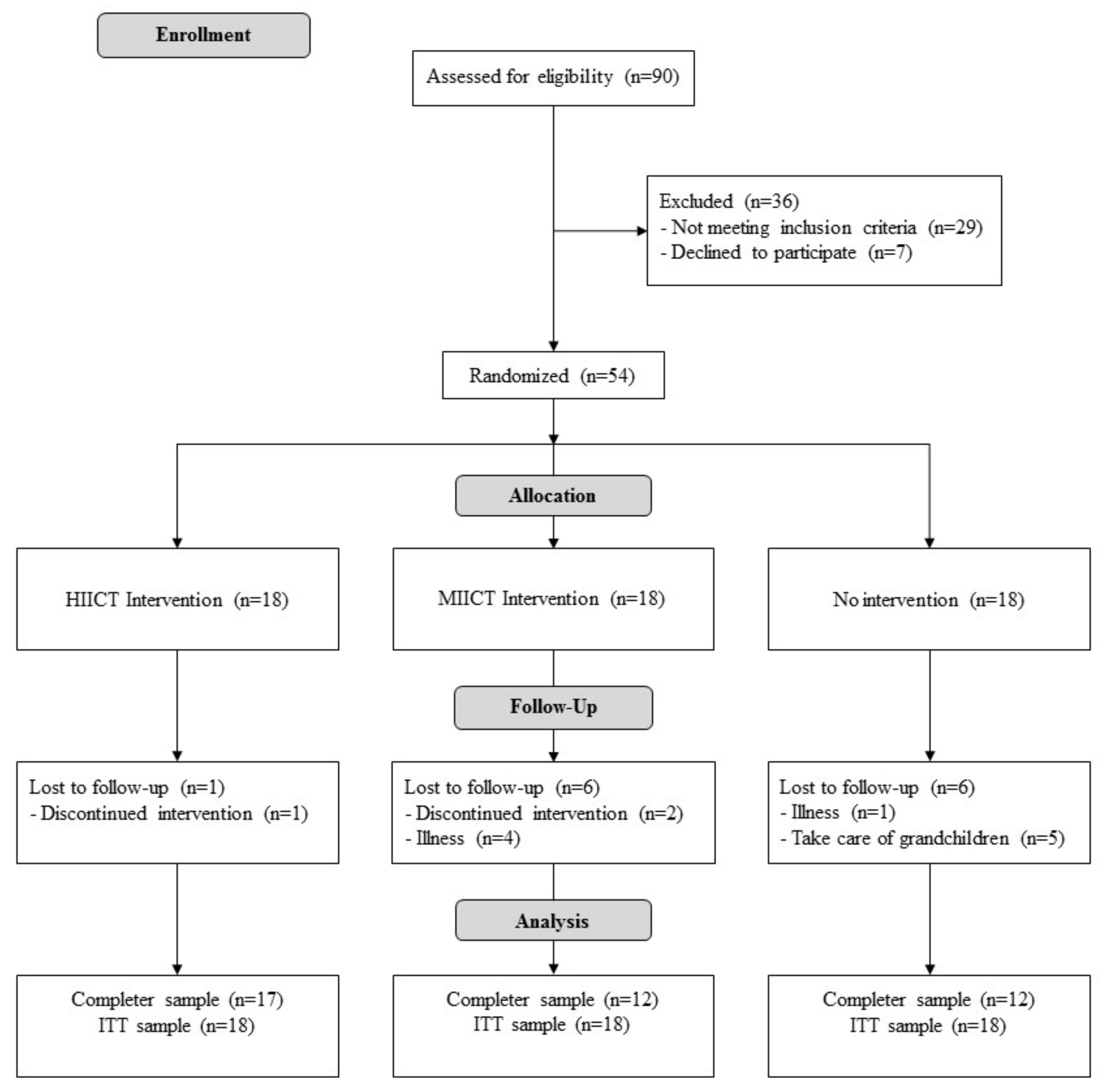
2.1. Design
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.5. Sample size and Power
2.6. Randomization and Blinding
2.7. Statistical Analysis
3. Results
3.1. Inter-group Results
- For VO2max-ES, HIICT was statistically superior to the CG (dif = 3.4 ml/kg/min, t = −3.73) and MICT was also statistically superior to the CG (dif = 1.9 ml/kg/min, t = −2.65).
- For SBPex, HIICT was statistically better than the CG (dif = −6,39 mmHg, t = −0.122).
- For DBPex, HIICT was statistically better than the CG (dif = −5,00 mmHg, t = −3.933) and MICT was also statistically better than the CG (dif = −7,50 mmHg, t = 3.989).
- Finally, for maximal speed reached during treadmill test, HIICT was statistically superior to the CG (dif = 0.2 m/s, t = −1.96) and MICT was also statistically superior to the CG (dif = 0.57 m/s, t = −2.96).
3.2. Intra-group Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blain, H.; Masud, T.; Dargent-Molina, P.; Martin, F.C.; Rosendahl, E.; van der Velde, N.; Bousquet, J.; Benetos, A.; Cooper, C.; Kanis, J.A.; et al. A comprehensive fracture prevention strategy in older adults: The European Union Geriatric Medicine Society (EUGMS) statement. Aging Clin. Exp. Res. 2016, 28, 797–803. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health. Available online: https://population.un.org/wpp/ (accessed on 13 September 2019).
- Murias, J.M.; Paterson, D.H. Slower VO2 Kinetics in Older Individuals: Is It Inevitable? Med. Sci. Sports Exerc. 2015, 47, 2308–2318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amundsen, B.H.; Rognmo, Ø.; Hatlen-Rebhan, G.; Slørdahl, S.A. High-intensity aerobic exercise improves diastolic function in coronary artery disease. Scand. Cardiovasc. J. SCJ. 2008, 42, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Cardozo, G.G.; Oliveira, R.B.; Farinatti, P.T.V. Effects of high intensity interval versus moderate continuous training on markers of ventilatory and cardiac efficiency in coronary heart disease patients. Sci. World J. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guiraud, T.; Juneau, M.; Nigam, A.; Gayda, M.; Meyer, P.; Mehary, S.; Paillard, F.; Bosquet, L. Optimization of high intensity interval exercise in coronary heart disease. Eur. J. Appl. Physiol. 2010, 108, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Madssen, E.; Arbo, I.; Granøien, I.; Walderhaug, L.; Moholdt, T. Peak oxygen uptake after cardiac rehabilitation: A randomized controlled trial of a 12-month maintenance program versus usual care. PLoS ONE 2014, 9, 733–740. [Google Scholar] [CrossRef] [Green Version]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, S.; Wiswell, R. Rate and mechanism of maximal oxygen consumption decline with aging: Implications for exercise training. Sports Med. Auckl. NZ. 2003, 33, 877–888. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet Lond. Engl. 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Vellas, B.; Hsu, F.-C.; Newman, A.B.; Doss, H.; King, A.C.; Manini, T.M.; Church, T.; Gill, T.M.; Miller, M.E.; et al. A physical activity intervention to treat the frailty syndrome in older persons-results from the LIFE-P study. J. Gerontol. A. Biol. Sci. Med. Sci. 2015, 70, 216–222. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A. Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Laddu, D.R.; Wertheim, B.C.; Garcia, D.O.; Brunner, R.; Groessl, E.; Shadyab, A.H.; Going, S.B.; LaMonte, M.J.; Cannell, B.; LeBroff, M.S.; et al. Associations between self-reported physical activity and physical performance measures over time in postmenopausal women: The women’s health initiative. J. Am. Geriatr. Soc. 2017, 65, 2176–2181. [Google Scholar] [CrossRef] [PubMed]
- Masley, S.C.; Roetzheim, R.; Clayton, G.; Presby, A.; Sundberg, K.; Masley, L.V. Lifestyle markers predict cognitive function. J. Am. Coll. Nutr. 2017, 36, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Bunout, D.; Barrera, G.; Hirsch, S.; Jimenez, T.; de la Maza, M.P. Association between activity energy expenditure and peak oxygen consumption with sarcopenia. BMC Geriatr. 2018, 18, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Martínez, F.A.; Rubio-Arias, J.Á.; Ramos-Campo, D.J.; Alcaraz, P.E. Effectiveness of resistance circuit-based training for maximum oxygen uptake and upper-body one-repetition maximum improvements: A systematic review and meta-analysis. Sports Med. Auckl. NZ. 2017, 47, 2553–2568. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Campo, D.L.; Martínez-Guardado, I.; Olcina, G.; Marín-Pagán, C.; Martínez-Noguera, F.J.; Carlos-Vivas, J.; Alcaráz, P.E.; Rubio-Arias, J.Á. Effect of high-intensity resistance circuit-based training in hipoxia on aerobic performance and repeat sprint ability. Scand. J. Med. Sci. Sports 2018, 28, 2135–2143. [Google Scholar] [CrossRef]
- Villelabeitia-Jaureguizar, K.; Vicente-Campos, D.; Senen, A.B.; Jiménez, V.H.; Garrido-Lestache, M.E.B.; López Chicharro, J.L. Effects of high-intensity interval versus continuous exercise training on post-exercise heart rate recovery in coronary heart-disease patients. Int. J. Cardiol. 2017, 244, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Molisz, A.; Schmederer, Z.; Siebert, J.; Kadamani, T.; Glasner, P.; Rosłonkiewicz, K.; Nowicka-Sauer, K.; Gutknecht, P.; Trzeciak, B.; Suchanowski, A. Haemodynamic parameters in postmenopausal women–beneficial effect of moderate continuous exercise training. Ann. Agric. Envirn. Med. 2019, 26, 425–428. [Google Scholar] [CrossRef]
- Huang, G.; Shi, X.; Davis-Brezette, J.A.; Osness, W.H. Resting heart rate changes after endurance training in older adults: A meta-analysis. Med. Sci. Sports Exerc. 2005, 37, 1381–1386. [Google Scholar] [CrossRef]
- Ballesta-García, I.; Rubio Arias, J.Á.; Ramos Campo, D.J.; Martínez González-Moro, I.; Carrasco Poyatos, M. High-intensity interval training dosage for heart failure and coronary artery disease cardiac rehabilitation: A systematic review and meta-analysis. Rev. Espanola Cardiol. Engl. Ed. 2019, 72, 233–243. [Google Scholar] [CrossRef]
- López Chicharro, J.; Vicente Campos, D. HIIT de la teoría a la práctica; Exercise Physiology & Training: Madrid, Spain, 2018. [Google Scholar]
- Hwang, C.-L.; Yoo, J.-K.; Kim, H.-K.; Hwang, M.-H.; Handberg, E.M.; Petersen, J.W.; Christou, D.D. Novel all-extremity high-intensity interval training improves aerobic fitness, cardiac function and insulin resistance in healthy older adults. Exp. Gerontol. 2016, 82, 112–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, E.C.; Hay, J.L.; Kehler, D.S.; Boreskie, K.F.; Arora, R.C.; Umpierre, D.; Szwajcer, A.; Duhamel, T.A. Effects of high-intensity interval training versus moderate-intensity continuous training on blood pressure in adults with pre- to established hypertension: A systematic review and meta-analysis of randomized trials. Sports Med. Auckl. NZ. 2018, 48, 2127–2142. [Google Scholar] [CrossRef] [PubMed]
- Olea, M.A.; Mancilla, R.; Martínez, S.; Díaz, E. Effects of high intensity interval training on blood pressure in hypertensive subjects. Rev. Med. Chil. 2017, 145, 1154–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grace, F.; Herbert, P.; Elliott, A.D.; Richards, J.; Beaumont, A.; Sculthorpe, N.F. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp. Gerontol. 2018, 109, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; García-Pinillos, F.; Latorre-Román, P.Á. Effects of a 10-week functional training programme on pain, mood state, depression, and sleep in healthy older adults. Psychogeriact. Off. J. Psychigeriatr. Soc. 2018, 18, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Aragão-Santos, J.C.; De Resende-Neto, A.G.; Nogueira, A.C.; de Feitosa-Neta, M.L.; Brandão, L.H.; Chaves, L.M.; da Silva-Grigoletto, M.E. The effects of functional and traditional strength training on different strength parameters of elderly women: A randomized and controlled trial. J. Sports Med. Phys. Fitness 2019, 59, 380–386. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standarized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Ballesta-García, I.; Martínez-González-Moro, I.; Rubio-Arias, J.Á.; Carrasco-Poyatos, M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Functional Ability and Body Mass Index in Middle-Aged and Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4205. [Google Scholar] [CrossRef] [Green Version]
- Fielding, R.A.; Frontera, W.R.; Hughes, V.A.; Fisher, E.C.; Evans, W.J. The reproducibility of the Bruce protocol exercise test for the determination of aerobic capacity in older women. Med. Sci. Sports Exerc. 1997, 29, 1109–1113. [Google Scholar] [CrossRef]
- Kenney, W.L.; Humphrey, R.H.; Bryant, C.X.; Mahler, D.A. ACSM’s Guidelines for Exercise Testing and Prescription; Williams & Wilkins: Baltimore, MD, USA, 1995. [Google Scholar]
- Nugent, S.F.; Jung, M.E.; Bourne, J.E.; Loeppky, J.; Arnold, A.; Little, J.P. The influence of high-intensity interval training and moderate-intensity continuous training on sedentary time in overweight and obese adults. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2018, 43, 747–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dünnwald, T.; Melmer, A.; Gatterer, H.; Salzmann, K.; Ebenbichler, C.; Burtscher, M.; Schobersberger, W.; Grander, W. Supervised Short-term High-intensity Training on Plasma Irisin Concentrations in Type 2 Diabetic Patients. Int. J. Sports Med. 2019, 40, 158–164. [Google Scholar] [CrossRef]
- Kim, J.; Shin, W. How to Do Random Allocation (Randomization). Clin. Orthop. Surg. 2014, 6, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boukabous, I.; Marcotte-Chénard, A.; Amamou, T.; Boulay, P.; Brochu, M.; Tessier, D.; Riesco, E. Low-Volume High-Intensity Interval Training (HIIT) versus Moderate-Intensity Continuous Training on Body Composition, Cardiometabolic Profile and Physical Capacity in Older Women. J. Aging Phys. Act. 2019, 27, 1–34. [Google Scholar]
- Su, L.; Fu, J.; Sun, S.; Zhao, G.; Cheng, W.; Dou, C.; Quan, M. Effects of HIIT and MICT on cardiovascular risk factors in adults with overweight and/or obesity: A meta-analysis. PLoS ONE 2019, 14, e0210644. [Google Scholar] [CrossRef]
- Connolly, L.J.; Bailey, S.J.; Krustrup, P.; Fulford, J.; Smietanka, C.; Jones, A.M. Effects of self-paced interval and continuous training on health markers in women. Eur. J. Appl. Physiol. 2017, 117, 2281–2293. [Google Scholar] [CrossRef] [Green Version]
- Kemi, O.J.; Ellingsen, Ø.; Ceci, M.; Grimaldi, S.; Smith, G.L.; Condorelli, G.; Wisløff, U. Aerobic interval training enhances cardiomyocyte contractility and Ca2+ cycling by phosphorylation of CaMKII and Thr-17 of phospholamban. J. Mol. Cell Cardiol. 2007, 43, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Njemanze, H.; Warren, C.; Eggett, C.; MacGowan, G.A.; Bates, M.G.D.; Siervo, M.; Ivkovic, S.; Trenell, M.I.; Jakovljevic, D.G. Age-related decline in cardiac autonomin function is not attenuated with increased physical activity. Oncotarget 2016, 7, 76390–76397. [Google Scholar] [CrossRef] [Green Version]
- Qiu, Z.; Zheng, K.; Zhang, H.; Feng, J.; Wang, L.; Zhou, H. Physical Exercise and Patients with Chronic Renal Failure: A Meta-Analysis. BioMed Res. Int. 2017, 2017, 7191826. [Google Scholar] [CrossRef] [PubMed]
- Arbit, B.; Azarbal, B.; Hayes, S.W.; Gransar, H.; Germano, G.; Friedman, J.D.; Thomson, L.; Berman, D.S. Prognostic Contribution of Exercise Capacity, Heart Rate Recovery, Chronotropic Incompetence, and Myocardial Perfusion Single-Photon Emission Computerized Tomography in the Prediction of Cardiac Death and All-Cause Mortality. Am. J. Cardiol. 2015, 116, 1678–1684. [Google Scholar] [CrossRef] [PubMed]
- Akyüz, A.; Alpsoy, S.; Akkoyun, D.Ç.; Degirmenci, H.; Güler, N. Heart rate recovery may predict the presence of coronary artery disease. Anadolu. Kardiyol. Derg. 2014, 14, 351–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Bassett, D.R.; Turner, M.J. Exaggerated blood pressure response to maximal exercise in endurance-trained individuals. Am. J. Hypertens 1996, 9, 1099–1103. [Google Scholar] [CrossRef] [Green Version]
- Martin, W.H.; Ogawa, T.; Kohrt, W.M.; Malley, M.T.; Korte, E.; Kieffer, P.S.; Schechtman, K.B. Effects of aging, gender, and physical training on peripheral vascular function. Circulation 1991, 84, 654–664. [Google Scholar] [CrossRef] [Green Version]
- Daida, H.; Allison, T.G.; Squires, R.W.; Miller, T.D.; Gau, G.T. Peak exercise blood pressure stratified by age and gender in apparently healthy subjects. Mayo. Clin. Proc. 1996, 71, 445–452. [Google Scholar] [CrossRef]
- López Chicharro, J.L.; Vaquero, A.F. Physiology of Exercise; Editorial Médica Panamericana: Madrid, Spain, 2006. [Google Scholar]
- Bermúdez, C. Valoración de la presión arterial en la ergometría. Rev. Urug. Cardiol. 2012, 27, 399–404. [Google Scholar]
- Le, V.-V.; Mitiku, T.; Sungar, G.; Myers, J.; Froelicher, V. The blood pressure response to dynamic exercise testing: A systematic review. Prog. Cardiovasc. Dis. 2008, 51, 135–160. [Google Scholar] [CrossRef]
- Ayabe, M.; Aoki, J.; Kumahara, H.; Ishii, K.; Yonei, Y.; Tanaka, H. Effects of Age and Body Mass Index on Accuracy of Simple Moderate Vigorous Physical Activity Monitor Under Controlled Condition. Anti Aging Med. 2011, 8, 31–47. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Group | n | Mean | SD | Min | Max | p |
|---|---|---|---|---|---|---|
| Age (years) | ||||||
| CG | 18 | 67.4 | 5.71 | 59 | 75 | 0.370 |
| MICT | 18 | 70 | 8.76 | 55 | 86 | |
| HIICT | 18 | 66.3 | 5.44 | 57 | 76 | |
| Body Mass Index (kg/m2) | ||||||
| CG | 18 | 31.2 | 4.89 | 20.9 | 38.4 | 0.689 |
| MICT | 18 | 30.1 | 3.08 | 24.3 | 35.9 | |
| HIICT | 18 | 30.4 | 4.13 | 35.2 | 37.7 | |
| Maximal Oxygen Consumption estimated (ml/kg/min) | ||||||
| CG | 18 | 26.8 | 5.17 | 15.5 | 39.0 | 0.065 |
| MICT | 18 | 25.0 | 5.57 | 15.5 | 33.1 | |
| HIICT | 18 | 26.1 | 5.63 | 18.4 | 36.1 | |
| Heart Rate peak (bpm) | ||||||
| CG | 18 | 144.94 | 15.4 | 108 | 170 | 0.719 |
| MICT | 18 | 150.78 | 22.6 | 119 | 193 | |
| HIICT | 18 | 148.83 | 17.7 | 93 | 173 | |
| Heart Rate recovery (bpm) | ||||||
| CG | 18 | 79.5 | 8.1 | 68.2 | 91.3 | <0.001 |
| MICT | 18 | 85 | 14.3 | 60.5 | 121 | |
| HIICT | 18 | 100 | 53.0 | 54.8 | 296 | |
| Systolic Blood Pressure exercise (mmHg) | ||||||
| CG | 18 | 184 | 23.50 | 146 | 210 | 0.008 |
| MICT | 18 | 185 | 10.80 | 170 | 210 | |
| HIICT | 18 | 179 | 9.67 | 160 | 200 | |
| Diastolic Blood Pressure exercise (mmHg) | ||||||
| CG | 18 | 76.9 | 13.2 | 50 | 95 | 0.003 |
| MICT | 18 | 56.9 | 9.3 | 40 | 75 | |
| HIICT | 18 | 58.3 | 6.9 | 50 | 75 | |
| Systolic Blood Pressure recovery (mmHg) | ||||||
| CG | 18 | 152 | 16.2 | 120 | 175 | 0.042 |
| MICT | 18 | 156 | 13.6 | 140 | 190 | |
| HIICT | 18 | 151 | 11.7 | 135 | 180 | |
| Diastolic Blood Pressure recovery (mmHg) | ||||||
| CG | 18 | 73.3 | 7.28 | 65 | 90 | 0.001 |
| MICT | 18 | 73.9 | 7.19 | 60 | 85 | |
| HIICT | 18 | 73.9 | 5.02 | 65 | 80 | |
| Maximal speed reached during treadmill test (m/s) | ||||||
| CG | 18 | 4.94 | 0.809 | 3.2 | 6.7 | 0.054 |
| MICT | 18 | 4.66 | 0.899 | 3.2 | 5.9 | |
| HIICT | 18 | 4.86 | 0.910 | 3.7 | 6.4 | |
| Group | Increment | ANCOVA interactions (F, p, ES η²) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (ITT) | n (treated) | Mean | SD | Training x Group | Training x Baseline | Training x Age | |||||||
| F | p | ES η² | F | p | ES η² | F | p | ES η² | |||||
| Maximal Oxygen Consumption estimated (ml/kg/min) | |||||||||||||
| CG | 18 | 12 | −0.80 | −0.31 | 7.36 | 0.002 1,2 | 0.224 | 13.60 | <0.001 | 0.171 | 0.11 | 0.742 | 0.002 |
| MICT | 18 | 12 | 1.90 | −0.85 | |||||||||
| HIICT | 18 | 17 | 3.40 | 0.12 | |||||||||
| Heart Rate peak (bpm) | |||||||||||||
| CG | 18 | 12 | −4.33 | −0.06 | 3.26 | 0.474 | 0.002 | 2.56 | 0.115 | 0.043 | 8.18 | 0.006 | 0.070 |
| MICT | 18 | 12 | −0.72 | −4.70 | |||||||||
| HIICT | 18 | 17 | −4.72 | 2.61 | |||||||||
| Heart Rate recovery (bpm) | |||||||||||||
| CG | 18 | 12 | 0.81 | 0.00 | 1.92 | 0.156 | 0.070 | 37.844 | <0.001 | 0.426 | 0.039 | 0.844 | 0.001 |
| MICT | 18 | 12 | −0.34 | −3.65 | |||||||||
| HIICT | 18 | 17 | −19.85 | −40.18 | |||||||||
| Systolic Blood Pressure exercise (mmHg) | |||||||||||||
| CG | 18 | 12 | −15.40 | −7.75 | 3.48 | 0.038 2 | 0.120 | 37.66 | <0.001 | 0.394 | 6.24 | 0.016 | 0.098 |
| MICT | 18 | 12 | −6.39 | 0.24 | |||||||||
| HIICT | 18 | 17 | −3.06 | −3.52 | |||||||||
| Diastolic Blood Pressure exercise (mmHg) | |||||||||||||
| CG | 18 | 12 | −12.78 | −5.10 | 17.4 | <0.001 1,2 | 0.405 | 8.37 | <0.001 | 0.086 | 1.19 | 0.281 | 0.014 |
| MICT | 18 | 12 | 7.50 | 0.28 | |||||||||
| HIICT | 18 | 17 | 5.00 | −0.68 | |||||||||
| Systolic Blood Pressure recovery (mmHg) | |||||||||||||
| CG | 18 | 12 | −6.39 | −4.70 | 0.0587 | 0.943 | 0.002 | 76.01 | <0.001 | 0.589 | 13.332 | <0.001 | 0.207 |
| MICT | 18 | 12 | −5.84 | −6.86 | |||||||||
| HIICT | 18 | 17 | −6.95 | −6.21 | |||||||||
| Diastolic Blood Pressure recovery (mmHg) | |||||||||||||
| CG | 18 | 12 | 1.39 | −2.00 | 0.0540 | 0.947 | 0.002 | 73.137 | <0.001 | 0.592 | 5.3698 | 0.025 | 0.097 |
| MICT | 18 | 12 | 1.11 | −2.04 | |||||||||
| HIICT | 18 | 17 | 2.22 | −0.30 | |||||||||
| Maximal speed reached during treadmill test (m/s) | |||||||||||||
| CG | 18 | 12 | −0.08 | −0.01 | 7.68 | 0.001 1,2 | 0.231 | 10.28 | 0.023 | 0.134 | 0.317 | 0.575 | 0.005 |
| MICT | 18 | 12 | 0.51 | −0.14 | |||||||||
| HIICT | 18 | 17 | 0.20 | 0.07 | |||||||||
| Body Mass Index (kg/m2) | |||||||||||||
| CG | 18 | 12 | 0.30 | −0.05 | 6.99 | 0.002 2 | 0.215 | 3.02 | 0.088 | 0.046 | 0.217 | 0.643 | 0.003 |
| MICT | 18 | 12 | −0.10 | 1.47 | |||||||||
| HIICT | 18 | 17 | −0.30 | 0.47 | |||||||||
| Variables | Pre-training | Post-Training | p | 95% CI for MD | Cohen’s d | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | Lower | Upper | |||
| Maximal Oxygen Consumption estimated (mL/kg/min) | ||||||||||
| CG | 18 | 26.8 | 5.17 | 12 | 26.00 | 4.86 | 0.288 | −0.753 | 2.386 | 0.14 |
| MICT | 18 | 25.0 | 5.57 | 12 | 26.90 | 4.72 | 0.010 | −3.378 | −0.541 | 0.32 |
| HIICT | 18 | 26.1 | 5.63 | 17 | 29.50 | 5.75 | <0.001 | −3.968 | −0.441 | 0.58 |
| Heart Rate peak (bpm) | ||||||||||
| CG | 18 | 144.94 | 15.41 | 12 | 140.61 | 15.35 | 0.066 | −0.316 | 8.983 | 0.26 |
| MICT | 18 | 150.78 | 22.64 | 12 | 150.06 | 17.94 | 0.770 | −4.408 | 5.853 | 0.03 |
| HIICT | 18 | 148.83 | 17.76 | 17 | 144.11 | 20.37 | 0.125 | −1.444 | 10.888 | 0.25 |
| Heart Rate recovery (bpm) | ||||||||||
| CG | 18 | 79.54 | 8.13 | 12 | 80.35 | 8.13 | 0.669 | −4.737 | 3.117 | 0.09 |
| MICT | 18 | 85.01 | 14.32 | 12 | 84.67 | 10.67 | 0.916 | −6.204 | 6.871 | 0.02 |
| HIICT | 18 | 100.16 | 52.98 | 17 | 80.31 | 12.80 | 0.105 | −4.629 | 44.327 | 0.36 |
| Systolic Blood Pressure exercise (mmHg) | ||||||||||
| CG | 18 | 184.28 | 23.52 | 12 | 168.88 | 15.77 | 0.002 | 6.335 | 24.442 | 0.58 |
| MICT | 18 | 185.00 | 10.84 | 12 | 178.61 | 11.08 | 0.015 | 1.430 | 11.347 | 0.55 |
| HIICT | 18 | 178.61 | 9.67 | 17 | 175.55 | 6.15 | 0.213 | −1.927 | 8.038 | 0.30 |
| Diastolic Blood Pressure exercise (mmHg) | ||||||||||
| CG | 18 | 76.94 | 13.18 | 12 | 64.16 | 8.08 | 0.002 | 5.186 | 20.368 | 0.90 |
| MICT | 18 | 56.94 | 9.25 | 12 | 64.44 | 9.53 | 0.002 | −11.699 | −3.300 | 0.75 |
| HIICT | 18 | 58.33 | 6.86 | 17 | 63.33 | 6.18 | 0.003 | −8.075 | −1.925 | 0.69 |
| Systolic Blood Pressure recovery (mmHg) | ||||||||||
| CG | 18 | 151.94 | 16.19 | 12 | 145.55 | 11.49 | 0.020 | 1.145 | 11.632 | 0.37 |
| MICT | 18 | 155.56 | 13.60 | 12 | 149.72 | 6.74 | 0.019 | 1.065 | 10.600 | 0.40 |
| HIICT | 18 | 151.11 | 11.70 | 17 | 144.16 | 5.49 | 0.028 | 0.845 | 13.043 | 0.57 |
| Diastolic Blood Pressure recovery (mmHg) | ||||||||||
| CG | 18 | 73.33 | 7.27 | 12 | 74.72 | 5.27 | 0.462 | −5.279 | 2.501 | 0.18 |
| MICT | 18 | 73.89 | 7.18 | 12 | 75.00 | 5.14 | 0.570 | −2.258 | 2.703 | 0.14 |
| HIICT | 18 | 73.89 | 5.01 | 17 | 76.11 | 4.71 | 0.215 | −5.862 | 1.418 | 0.42 |
| Maximal speed reached during treadmill test (m/s) | ||||||||||
| CG | 18 | 4.94 | 0.80 | 12 | 4.86 | 0.79 | 0.448 | −0.143 | 0.309 | 0.09 |
| MICT | 18 | 4.47 | 0.90 | 12 | 4.98 | 0.77 | 0.015 | −0.544 | −0.067 | 0.53 |
| HIICT | 18 | 5.21 | 0.82 | 17 | 5.41 | 0.89 | 0.001 | −0.685 | −0.203 | 0.23 |
| Body Mass Index (kg/m2) | ||||||||||
| CG | 18 | 31.2 | 4.89 | 12 | 31.5 | 5.05 | 0.019 | −0.52 | −0.53 | 0.06 |
| MICT | 18 | 30.1 | 3.08 | 12 | 30.0 | 3.15 | 0.140 | −0.02 | 0.29 | 0.03 |
| HIICT | 18 | 30.4 | 4.13 | 17 | 30.1 | 4.24 | 0.035 | 0.02 | 0.60 | 0.07 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballesta-García, I.; Martínez-González-Moro, I.; Ramos-Campo, D.J.; Carrasco-Poyatos, M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 1805. https://doi.org/10.3390/ijerph17051805
Ballesta-García I, Martínez-González-Moro I, Ramos-Campo DJ, Carrasco-Poyatos M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(5):1805. https://doi.org/10.3390/ijerph17051805
Chicago/Turabian StyleBallesta-García, Ismael, Ignacio Martínez-González-Moro, Domingo J Ramos-Campo, and María Carrasco-Poyatos. 2020. "High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 5: 1805. https://doi.org/10.3390/ijerph17051805
APA StyleBallesta-García, I., Martínez-González-Moro, I., Ramos-Campo, D. J., & Carrasco-Poyatos, M. (2020). High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(5), 1805. https://doi.org/10.3390/ijerph17051805