A Predictive Model for Height Tracking in an Adult Male Population in Bangladesh to Reduce Input Errors

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Continuous data collection mechanism: Data is not continuously collected. Recent eHealth data can collect data from remote clinics and or individual.
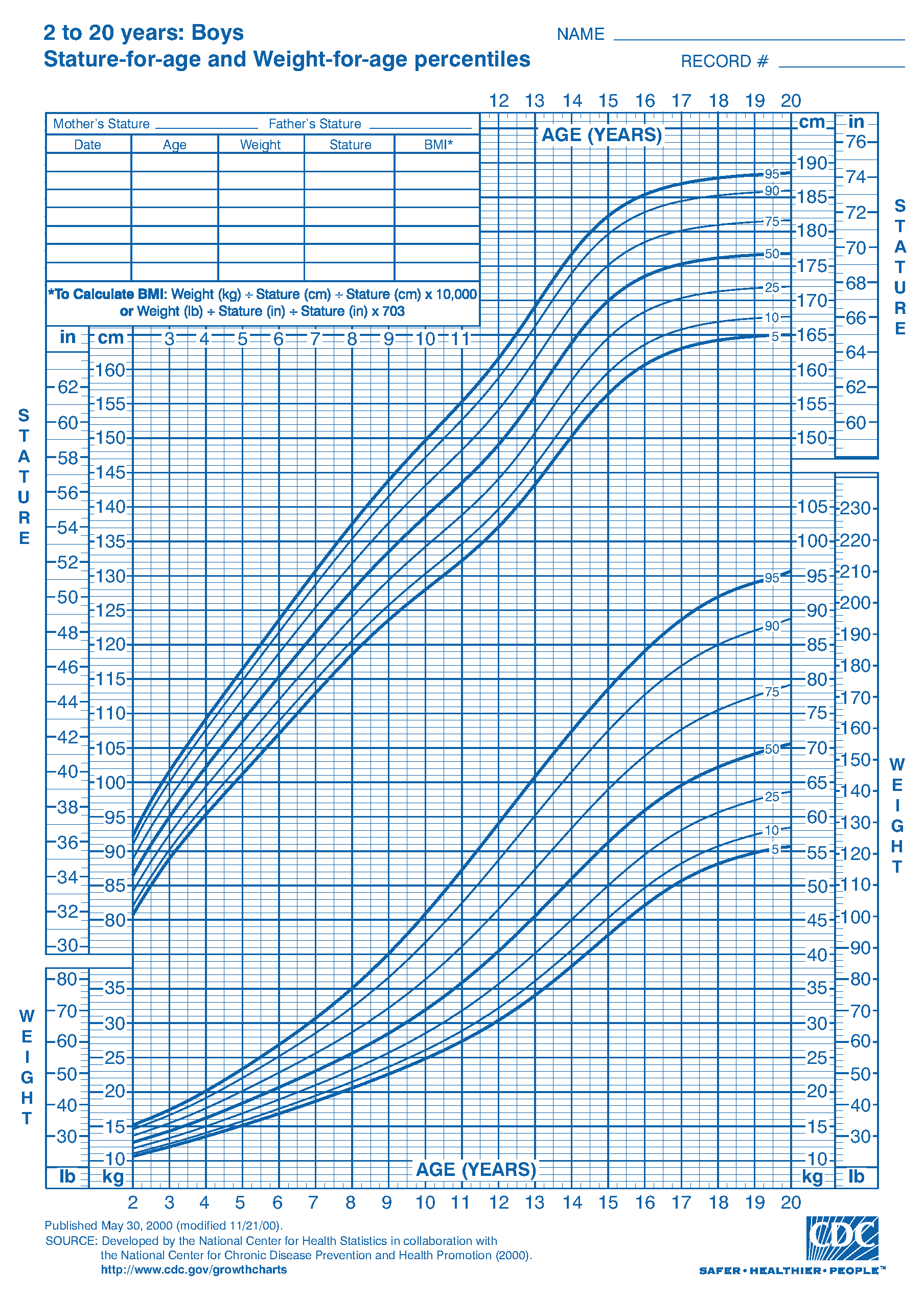
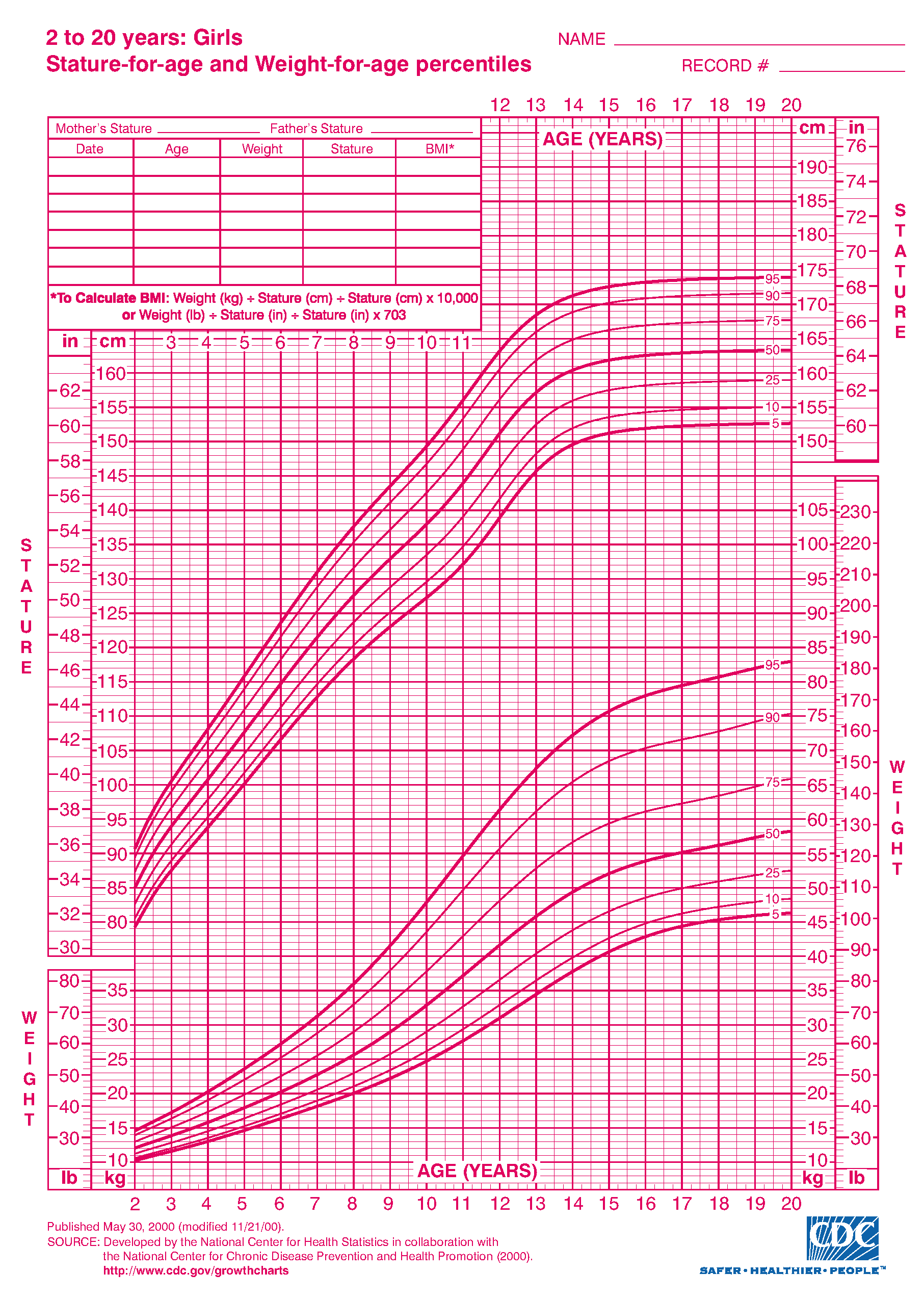
- Age level: CDC only reports clinical growth pattern of boys and girls until the age of 20. Growth pattern after the age of 20 is not available. This was due to the fact that there was no interest from the research community to investigate the similar set of characteristics of human growth pattern for ages more than 20. Human height generally stops growing at the of 20–22, however, other anthropometrics parameters (, , and ) may change with age.
- Anthropometric parameters: CDC reports only , , and other growth parameters for children. However, recent NCD related diseases require hip, waist size to be measured. These parameters are not considered. Recent focus on non-communicable diseases (NCD) has influence on obesity of people, thus the growth characteristics of these parameters became important. In this paper, we investigate to understand if there are any significant clinical growth patterns, specifically regarding height for male over 20 years of age.
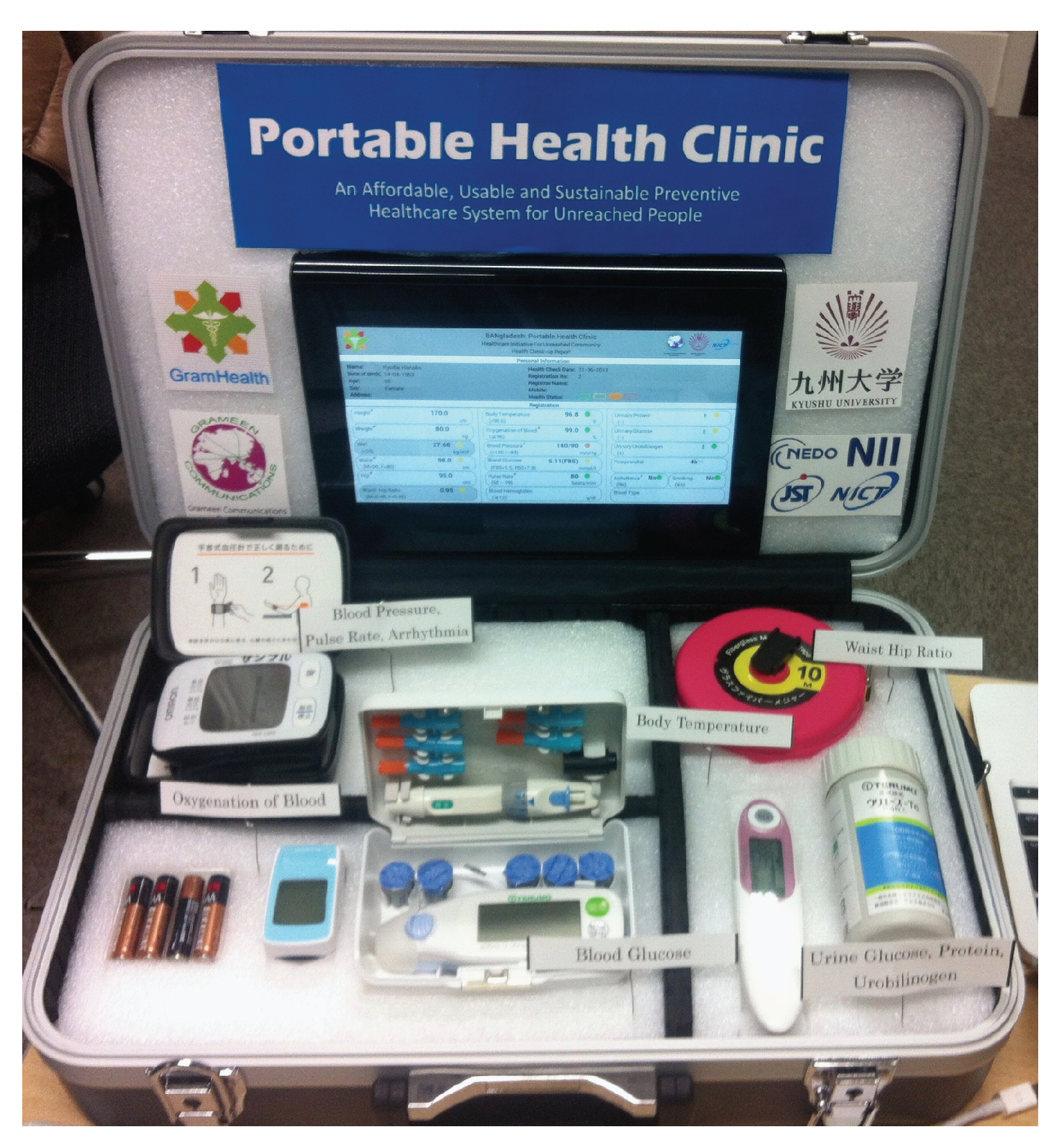
2. About Portable Health Clinic Data and our Research Motivation
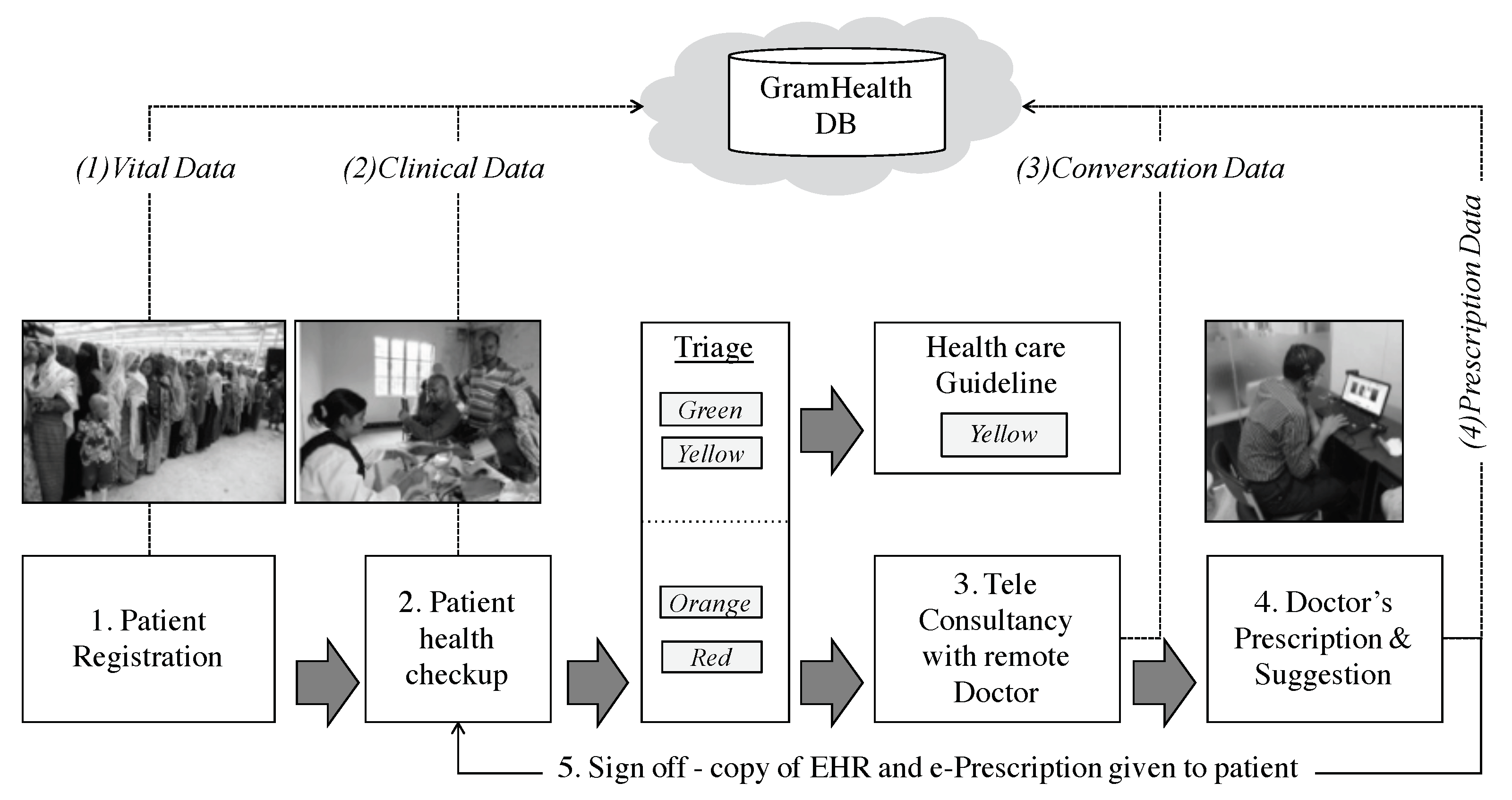
- Registration: Patients supply vital information e.g., name, age, sex, location and disease complaints etc. A data entry operator inputs data into the database (GramHealth). A patient ID is issued for follow up observations.
- Index: A set of physical check-up is performed by the healthcare assistant, the clinical data is shared with GramHealth database. The data can be uploaded automatically if the sensor have a wireless interface and is connected with the local server (the tablet PC), or the healthcare assistant manually inserts data by using an android app attached to the PHC box.
- Criterion: Patients are classified in four groups with color-coded risk stratification: green (healthy), yellow (caution), orange (affected) and red (emergency). The ‘green‘ and ’yellow’ patients are given a healthy guidance booklet. The ‘orange‘ and ‘red‘ marked patients consults with a call center doctor.
- Causality: The patients who have been marked by ‘yellow‘ and ‘red‘ should consult with the remote doctor for further investigations of their disease and explanation of their medical records. Telehealth consultancy is performed over voice and video.
- Prescription and Suggestion: At the end, remote doctor identifies disease after checking the clinical data, discussing with the patient for their symptoms analysis and his/her past health records (if any). And the doctor fills up the prescription and uploads to the GramHealth server (The GramHealth server is maintained by Grameen Communications, Bangladesh. They are operating PHC and achieving the health records. Kyushu University has a joint research collaboration agreement with them. All the privacy data has been removed and only Age, Height, Weight, BMI, Waist and Hip data are provided. The healthcare assistant prints the prescription and handover it to the patient with necessary explanations).
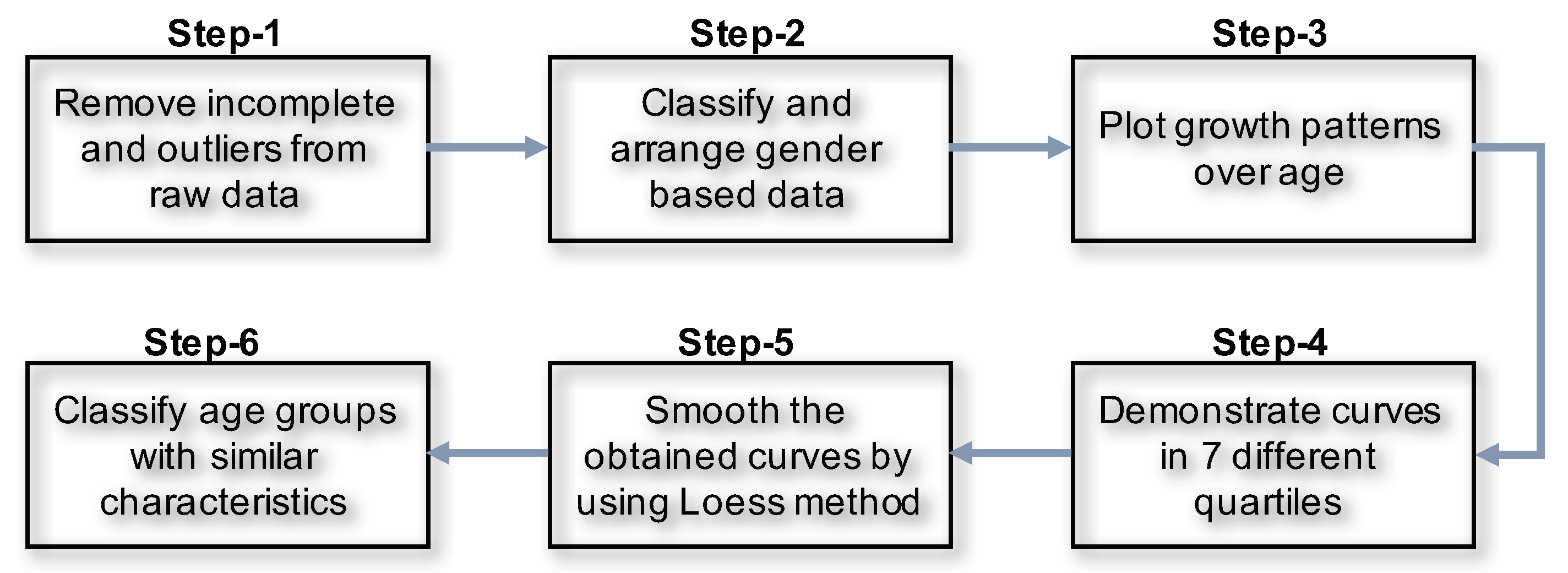
3. Steps to Demonstrate Growth Pattern from Raw Healthcare Data
- Step-1: Filtration: We run a statistical analysis to identify the outliers. We detected outliers from our eyeball measurements. Outliers are considered to be the data which are beyond the human acceptance range. We also removed the incomplete data. We had 40,391 records, from which we found N = 38,856 records belongs to 20–100 years of age.
- Step-2: Gender based records: We classified the data based on gender. Number of male was = 19,054. After remove the NA, we found = 14,085 records and finally after remove the outlier the processed records was = 13,932.
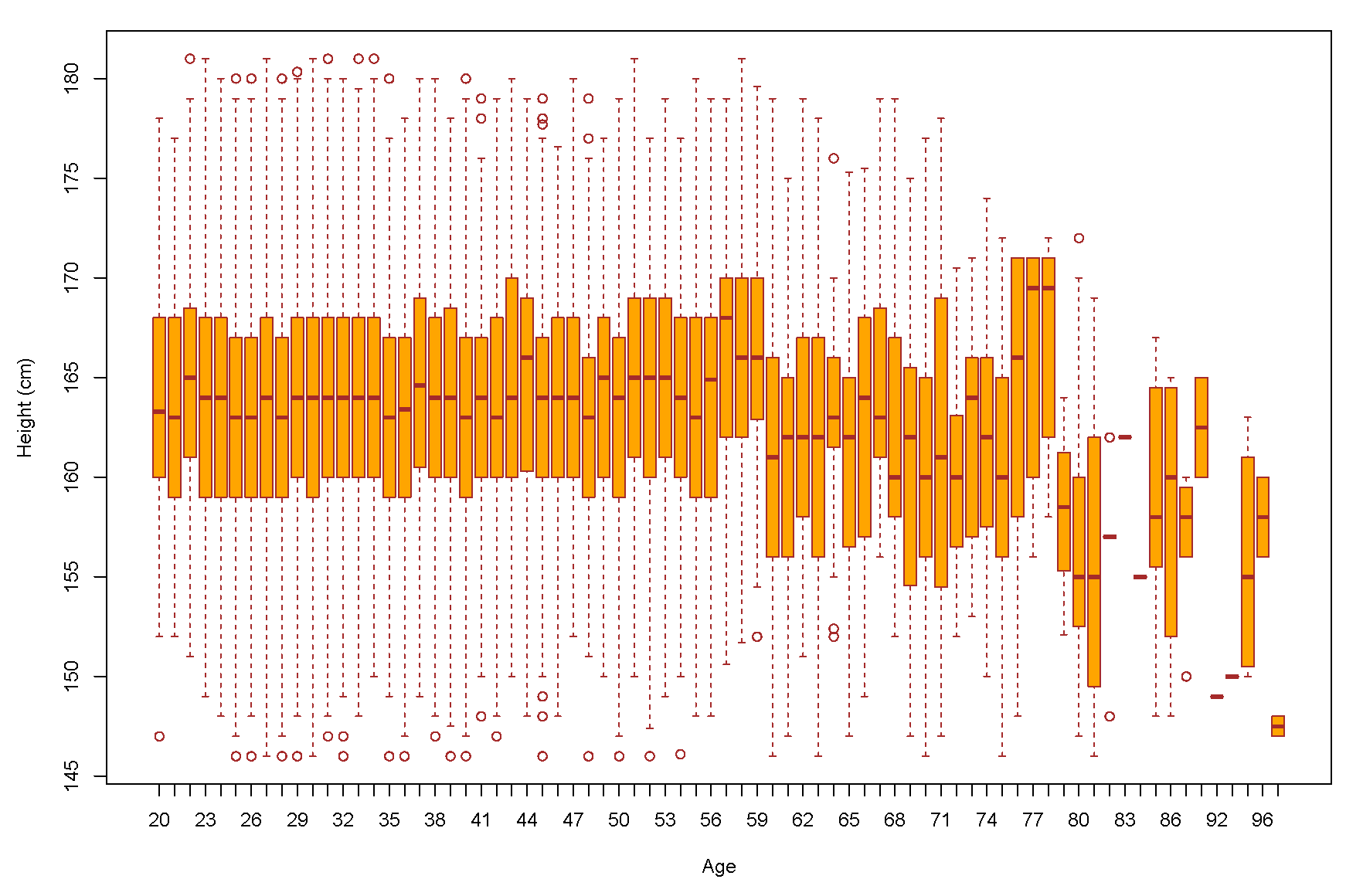
- Step-3: We demonstrated a scatter plot to check the age based height pattern for each age. In this study, we focused only on male’s height (Figure 6).
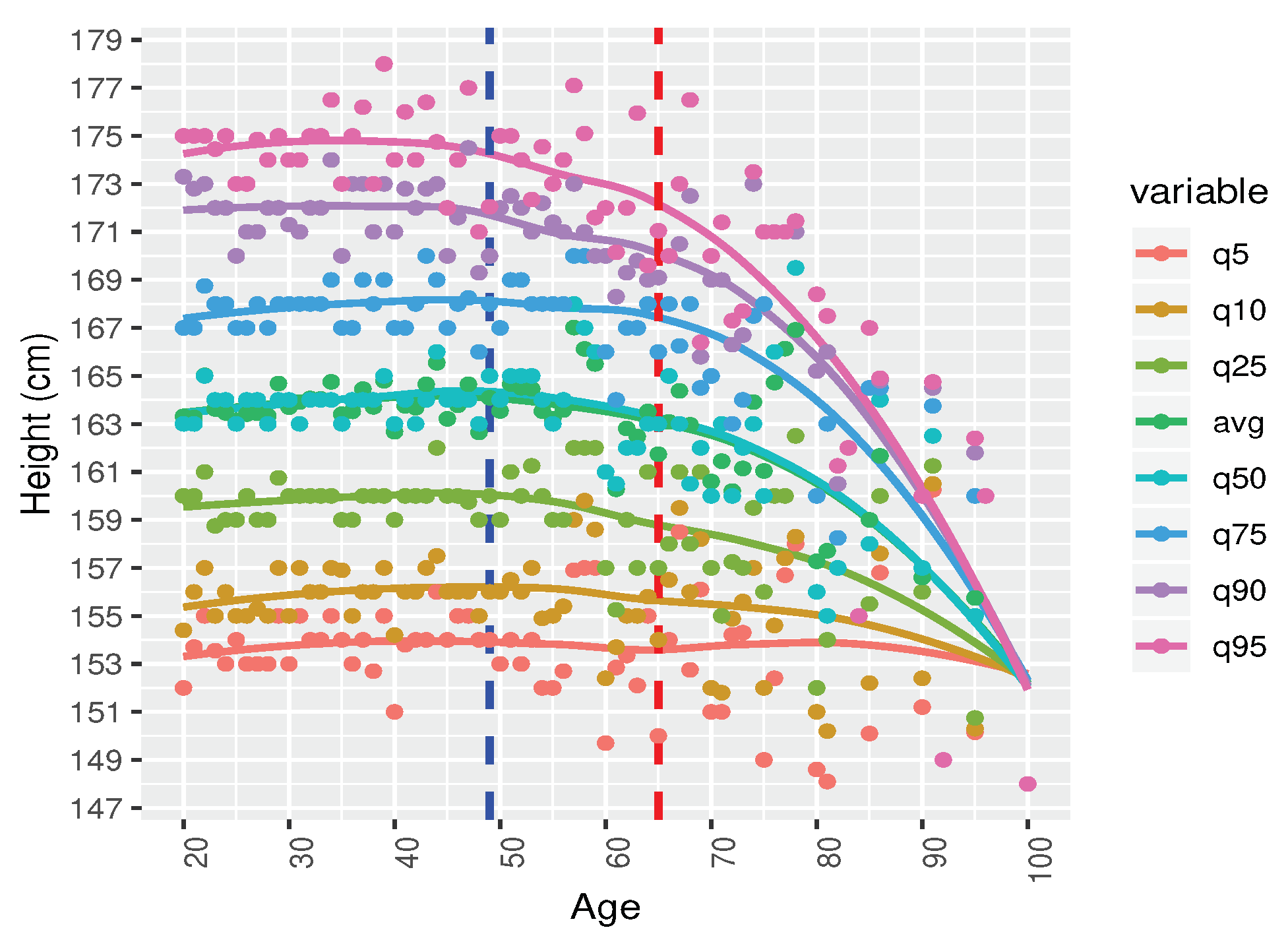
- Step-4: Male height in correspondence with age by seven difference quantiles (5th, 10th, 25th, 50th, 75th, 90th, and 95th) are plotted to understanding the distribution patterns (Figure 7).
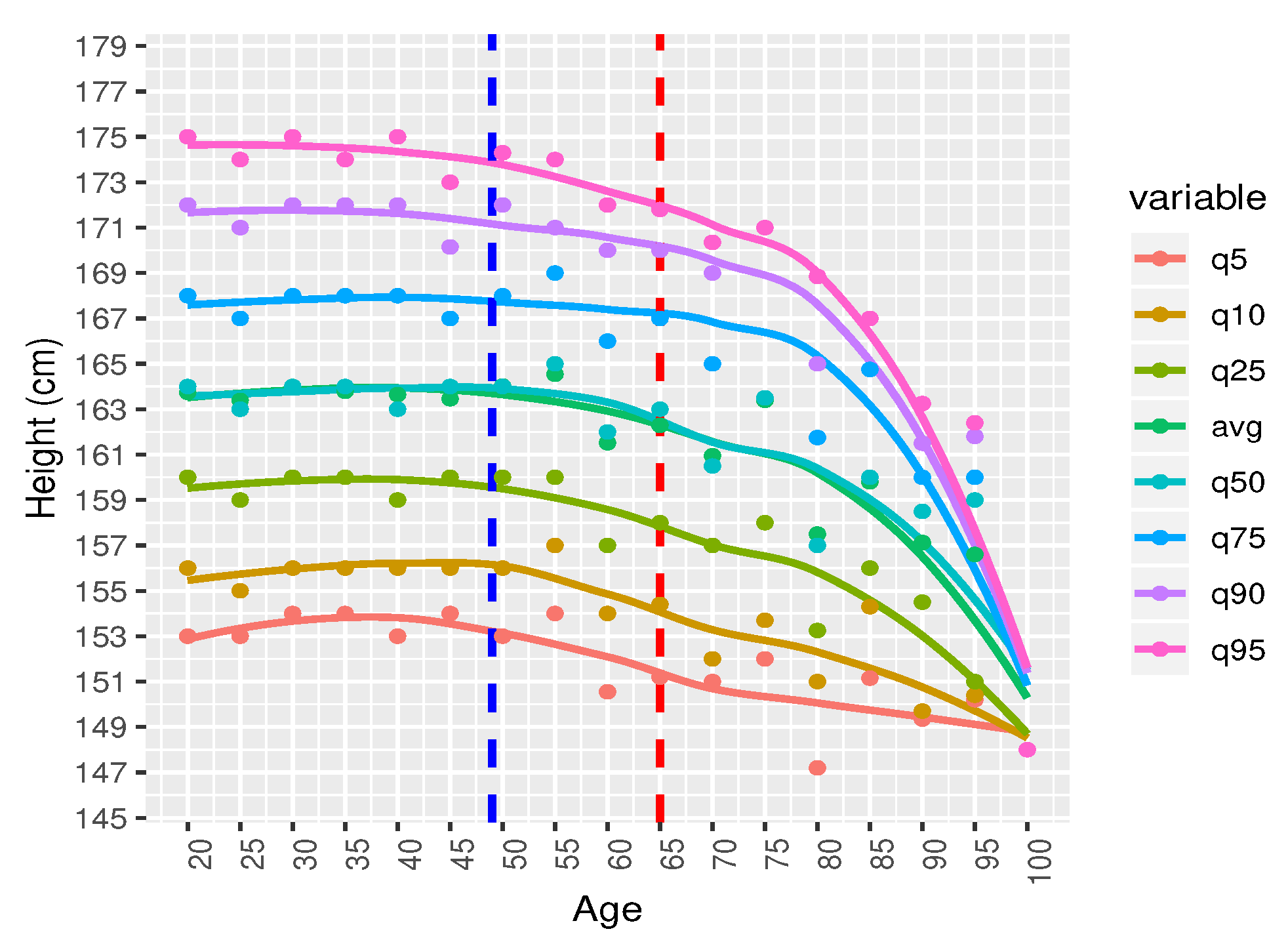
- Step-5: All the seven quantiles have been smoothened by using the popular Loess method (Figure 8). Loess represents for locally estimated scatterplot smoothing (loess stands for locally weighted scatterplot smoothing) and is one of many non-parametric regression techniques, but arguably the most flexible. A smoothing function is a function that attempts to capture general patterns in stressor-response relationships while reducing the noise and it makes minimal assumptions about the relationships among variables. The result of a loess application is a line through the moving central tendency of the stressor-response relationship. Loess is essentially used to visually assess the relationship between two variables.
- Step-6: Group wise characteristics: We observed the characteristics by classifying the participants into 17 different groups considering 5 year’s age intervals i.e., 20–24, 25–29, ⋯, 95–99, 100-).
4. Data Analysis and Results Discussion
- Age group 20–49: There is no significant change in the growth at this age level. The reason could be the following: there is no significance change because generally male stop growing at the age of 18–20. Therefore, our findings comply with the natural growth of human being.
- Age group 50–64: A slowly decremented pattern is observed at this age zone. There could be two reasons for the height decreases with age: (a) biologically, our bone starts shrinking after this age level (b) a person of 79 years old now, was at 20 years of old in 1960s. At that period, the average height of male was 162 cm–164 cm [24]. Their growth height stopped at the age of 20. That is why the growth pattern shows a decremental characteristics.
- Age group 65–100: There is a drastic height loss in this age zone. Height of people may not decrease so drastically. This is quite surprising. We assume that this pattern is not representative. In fact, there are only 37 data samples. Also, it can be assumed that the people were short at when their growth level stopped at their age of twenty which happened sixty to eighty years ago. People at that time, were generally short.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ahmed, A.; Inoue, S.; Kai, E.; Nakashima, N.; Yasunobu, N. Portable Health Clinic: A Pervasive Way to Serve the Unreached Community for Preventive Healthcare; Springer: Berlin/Heidelberg, Germany, 2013; pp. 265–274. [Google Scholar]
- Kai, E.; Ahmed, A. Technical Challenges in Providing Remote Health Consultancy Services for the Unreached Community. In Proceedings of the 27th International Conference on Advanced Information Networking and Applications Workshops, Barcelona, Spain, 25–28 March 2013; pp. 1016–1020. [Google Scholar]
- Ahmed, A.; Ishida, K.; Okada, M.; Yasuura, H. Poor-friendly technology initiative in Japan. J. Soc. Bus. 2010, 1, 92–104. [Google Scholar]
- Ahmed, A.; Hargrave, A.; Nohara, Y.; Islam, R.; Ghosh, P.; Nakashima, N.; Hiroto, Y. Smart Sensors and Systems; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Ben-Gal, I. Outlier detection. In Data Mining and Knowledge Discovery Handbook; Springer: Berlin/Heidelberg, Germany, 2005; pp. 131–146. [Google Scholar]
- Goldberg, S.I.; Niemierko, A.; Turchin, A. Analysis of data errors in clinical research databases. AMIA Annu. Symp. Proc. 2008, 2008, 242–246. [Google Scholar]
- Kumar, V.; Kumar, D.; Singh, R.K. Outlier mining in medical databases: An application of data mining in health care management to detect abnormal values presented in medical databases. IJCSNS Int. J. Comput. Sci. Netw. Secur. 2008, 8, 272–277. [Google Scholar]
- Jacobs, B. Electronic medical record, error detection, and error reduction: A pediatric critical care perspective. Pediatr. Crit. Care Med. 2007, 8, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Johnson, C.L. CDC Growth Charts: United States Advance Data from Vital and Health Statistics; National Center for Health Statistics: Hyattsville, MD, USA, 2000; pp. 1–27.
- Hasan, M.; Fukuda, A.; Maruf, R.I.; Yokota, F.; Ahmed, A. Errors in remote healthcare system: Where, how and by whom? In Proceedings of the TENCON-IEEE Region 10 Conference, Penang, Malaysia, 8–10 November 2017. [Google Scholar]
- Rebeiro-Hargrave, A.; Ahmed, A.; Nakashima, N.; Ghosh, P.P. Telehealth for low resource unreached communities. In Proceedings of the Third International Japan-Egypt Conference on Electronics, Communications and Computers, Kyushu, Japan, 16–18 March 2015. [Google Scholar]
- Hossain, M.N.; Kazi, M.H.; Chakrabarty, R.; Okajima, H.; Kitaoka, H.; Ahmed, A. Social Adoption of ICT Based Healthcare Delivery Systems in Rural Bangladesh (A Case Study on Portable Health Clinic). In Proceedings of the 1st International Conference on Advanced Information and Communication Technology, Chittagong, Bangladesh, 16–17 May 2016. [Google Scholar]
- Hossain, M.N.; Okajima, H.; Kitaoka, H.; Ahmed, A. Consumer acceptance of eHealth among rural inhabitants in developing countries (A Study on Portable Health Clinic in Bangladesh). Procedia Comput. Sci. 2017, 111, 471–478. [Google Scholar] [CrossRef]
- Hossain, M.N.; Sampa, M.B.; Yokota, F.; Fukuda, A.; Ahmed, A. Factors Affecting Rural Patients’ Primary Compliance with e-Prescription: A Developing Country Perspective. Telemed. e-Health 2019, 25, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Nohara, Y.; Kai, E.; Ghosh, P.P.; Islam, R.; Ahmed, A.; Kuroda, M.; Kobayashi, K. Health checkup and telemedical intervention program for preventive medicine in developing countries: Verification study. J. Med. Internet Res. 2015, 17, e2. [Google Scholar] [CrossRef]
- Alabbasi, S.; Rebeiro-Hargrave, A.; Kaneko, K.; Ahmed, A.; Fukuda, A. Personal Health Book Application for Developing Countries. Int. J. Ad. Comput. Sci. Appl. (IJACSA) 2015, 6, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Hasan, M.; Yokota, F.; Fukuda, A.; Sultana, N.; Ahmed, A. Concept of an Acceptance Range to Detect of Errors in Human Assisted Remote Healthcare Systems A Study on Portable Health Clinic System in Bangladesh. In Proceedings of the 2nd International Conference on Healthcare, SDG’s and Social Business, Fukuoka, Japan, 26–27 April 2018. [Google Scholar]
- Eiko, K.; Ahmed, A.; Inoue, S.; Taniguchi, A.; Nohara, Y.; Nakashima, N.; Kitsuregawa, M. Evolving health consultancy by predictive caravan health sensing in developing countries. In Proceedings of the 2014 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Washington, DC, USA, 13–16 September 2014. [Google Scholar]
- Galiano, A.; Massaro, A.; Boussahel, B.; Barbuzzi, D.; Tarulli, F.; Pellicani, L.; Renna, L.; Guarini, A.; De Tullio, G.; Nardelli, G.; et al. Improvements in haematology for home health assistance and monitoring by a web based communication system. In Proceedings of the IEEE International Symposium on Medical Measurements and Applications, Benevento, Italy, 15–18 May 2016. [Google Scholar]
- Matlani, P.; Londhe, N.D. A cloud computing based telemedicine service. In Proceedings of the 22 Point-of-Care Healthcare Technologies (PHT), Bangalore, India, 16–18 January 2013. [Google Scholar]
- Hsieh, J.; Hsu, M.W. A cloud computing based 12—Lead ECG telemedicine service. BMC Med. Inf. Dec. Mak. 2012, 12, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Massaro, A.; Maritati, V.; Savino, N.; Galiano, A.; Convertini, D.; De Fonte, E.; Di Muro, M. A Study of a health resources management platform integrating neural networks and DSS telemedicine for homecare assistance. Information 2018, 9, 176. [Google Scholar] [CrossRef] [Green Version]
- Rahman, T.K.; Kazi, M.H.; Islam, R.M.; Fukuda, A.; Ahmed, A. Measurement of illness and wellness score of non-communicable disease patients. In Proceedings of the TENCON-IEEE Region 10 Conference, Penang, Malaysia, 8–10 November 2017. [Google Scholar]
- Ahmed, A.; Rebeiro-Hargrave, A.; Nohara, Y.; Eiko, K.; Ripon, Z.H.; Nakashima, N. Targeting morbidity in unreached communities using portable health clinic system. In Proceedings of the Institute of Electronics, Information and Communication Engineers, Fukuoka-shi, Japan, 17–19 August 2014. [Google Scholar]
- Subramaniam, S.V.; Ozaltin, E.; Finley, J.E. Height of Nations: A Sociaeconomic Analysis of Cohort Differences and Patterns among Woman in 54 Low-to-Middle-Income Countries. PLoS ONE 2011, 6, e18962. [Google Scholar]
- Max, R.; Cameron, A.; Hannah, R. Human Height. Available online: https://www.ourworldindata.org/human-height (accessed on 12 July 2019).











© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasan, M.; Yokota, F.; Islam, R.; Hisazumi, K.; Fukuda, A.; Ahmed, A. A Predictive Model for Height Tracking in an Adult Male Population in Bangladesh to Reduce Input Errors. Int. J. Environ. Res. Public Health 2020, 17, 1806. https://doi.org/10.3390/ijerph17051806
Hasan M, Yokota F, Islam R, Hisazumi K, Fukuda A, Ahmed A. A Predictive Model for Height Tracking in an Adult Male Population in Bangladesh to Reduce Input Errors. International Journal of Environmental Research and Public Health. 2020; 17(5):1806. https://doi.org/10.3390/ijerph17051806
Chicago/Turabian StyleHasan, Mehdi, Fumihiko Yokota, Rafiqul Islam, Kenji Hisazumi, Akira Fukuda, and Ashir Ahmed. 2020. "A Predictive Model for Height Tracking in an Adult Male Population in Bangladesh to Reduce Input Errors" International Journal of Environmental Research and Public Health 17, no. 5: 1806. https://doi.org/10.3390/ijerph17051806
APA StyleHasan, M., Yokota, F., Islam, R., Hisazumi, K., Fukuda, A., & Ahmed, A. (2020). A Predictive Model for Height Tracking in an Adult Male Population in Bangladesh to Reduce Input Errors. International Journal of Environmental Research and Public Health, 17(5), 1806. https://doi.org/10.3390/ijerph17051806