Residential Radon Exposure and Cigarette Smoking in Association with Lung Cancer: A Matched Case-Control Study in Korea

 , , ,
, , ,  , ,
, , 
Abstract
:1. Introduction
2. Methods
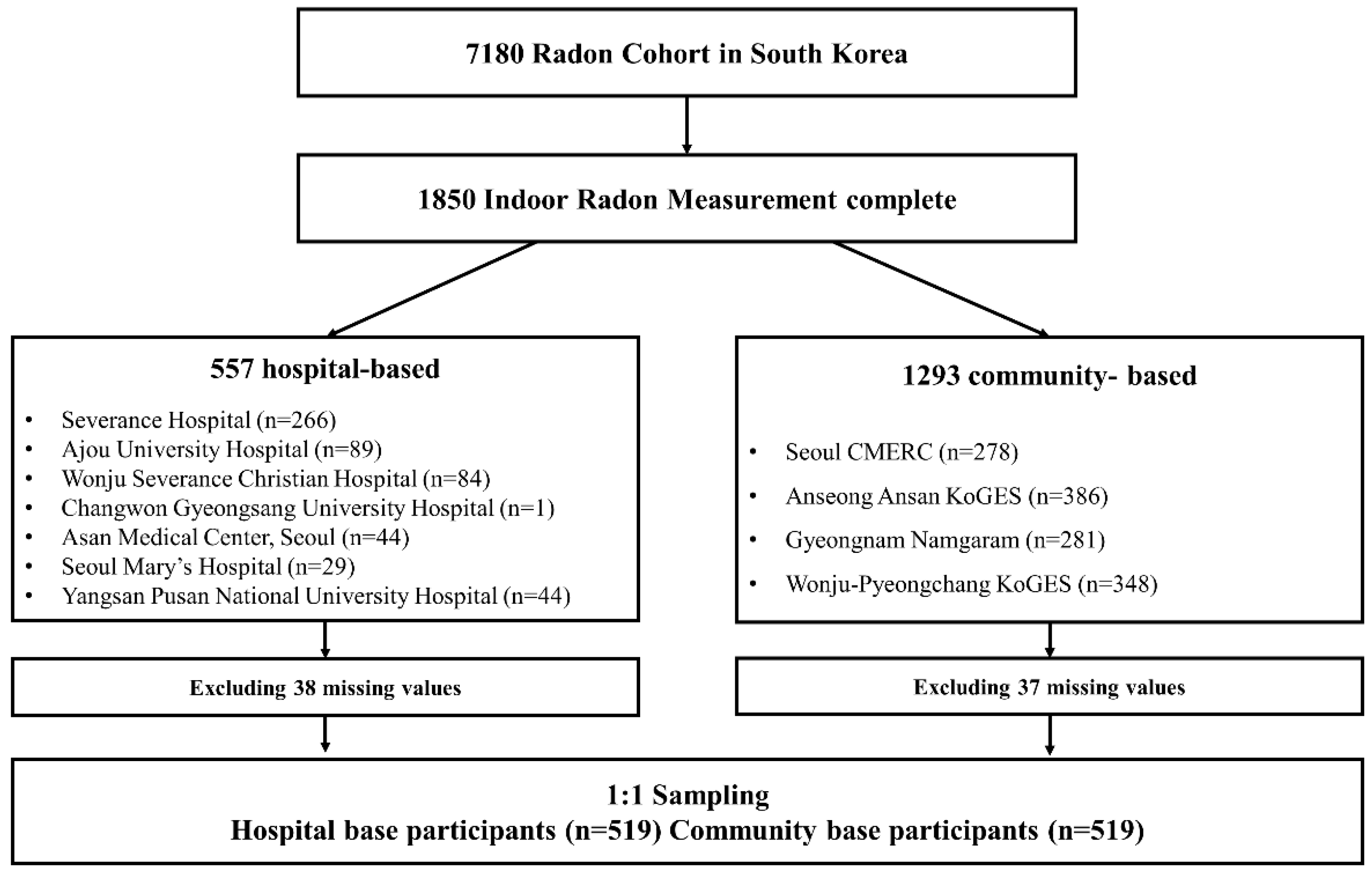
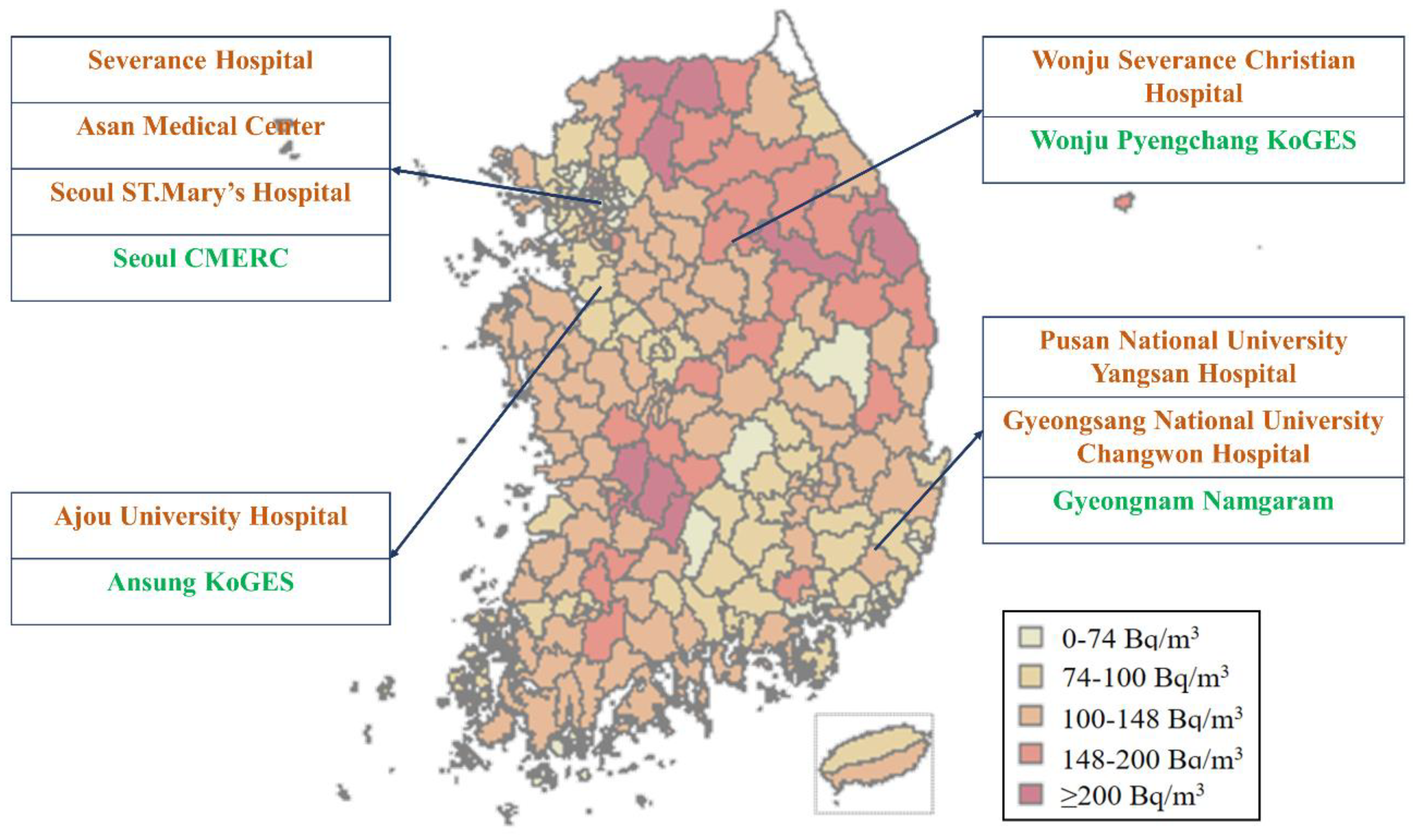
2.1. Study Design and Participants
2.2. Measurement of Residential Radon Levels
2.3. Smoking History and Covariables
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Residential Radon and Cigarette Smoking on Lung Cancer
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V. The IASLC lung cancer staging project: Proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Early Lung Cancer Action Program Investigators; Henschke, C.I.; Yankelevitz, D.F.; Libby, D.M.; Pasmantier, M.W.; Smith, J.P.; Miettinen, O.S. Survival of patients with stage I lung cancer detected on CT screening. N. Engl. J. Med. 2006, 355, 1763–1771. [Google Scholar] [PubMed] [Green Version]
- McKee, B.J.; Hashim, J.A.; French, R.J.; McKee, A.B.; Hesketh, P.J.; Lamb, C.R.; Williamson, C.; Flacke, S.; Wald, C. Experience with a CT screening program for individuals at high risk for developing lung cancer. J. Am. Coll. Radiol. 2015, 12, 192–197. [Google Scholar] [CrossRef] [Green Version]
- International Agency for Research on Cancer. Monographs on the Evaluation of Carcinogenic Risk to Humans: Man-Made Mineral Fibres and Radon; International Agency for Research on Cancer: Lyon, France, 1988. [Google Scholar]
- Alavanja, M.C.; Brownson, R.C.; Lubin, J.H.; Berger, E.; Chang, J.; Boice, J.D., Jr. Residential radon exposure and lung cancer among nonsmoking women. J. Natl. Cancer Inst. 1994, 86, 1829–1837. [Google Scholar] [CrossRef]
- Auvinen, A.; Makelainen, I.; Hakama, M.; Castren, O.; Pukkala, E.; Reisbacka, H.; Rytomaa, T. Indoor radon exposure and risk of lung cancer: A nested case-control study in Finland. J. Natl. Cancer Inst. 1996, 88, 966–972. [Google Scholar] [CrossRef] [Green Version]
- National Research Council. Health Effects of Exposure to Radon: BEIR VI; National Academies Press: Washington, DC, USA, 1999; Volume 6. [Google Scholar]
- Tomasek, L. Lung cancer risk from occupational and environmental radon and role of smoking in two Czech nested case-control studies. Int. J. Environ. Res. Public Health 2013, 10, 963–979. [Google Scholar] [CrossRef] [Green Version]
- Bohm, R.; Sedlak, A.; Bulko, M.; Holy, K. Use of threshold-specific energy model for the prediction of effects of smoking and radon exposure on the risk of lung cancer. Radiat. Prot. Dosim. 2014, 160, 100–103. [Google Scholar] [CrossRef]
- Saccomanno, G.; Huth, G.C.; Auerbach, O.; Kuschner, M. Relationship of radioactive radon daughters and cigarette smoking in the genesis of lung cancer in uranium miners. Cancer 1988, 62, 1402–1408. [Google Scholar] [CrossRef]
- Leuraud, K.; Billon, S.; Bergot, D.; Tirmarche, M.; Caer, S.; Quesne, B.; Laurier, D. Lung cancer risk associated to exposure to radon and smoking in a case-control study of French uranium miners. Health Phys. 2007, 92, 371–378. [Google Scholar] [CrossRef]
- Amabile, J.C.; Leuraud, K.; Vacquier, B.; Caer-Lorho, S.; Acker, A.; Laurier, D. Multifactorial study of the risk of lung cancer among French uranium miners: Radon, smoking and silicosis. Health Phys. 2009, 97, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Song, B.M.; Lee, J.H.; Lee, S.W.; Park, J.H.; Choi, D.P.; Lee, M.H.; Ha, K.H.; Kim, D.J.; Park, S.; et al. Cardiovascular and Metabolic Diseases Etiology Research Center (CMERC) cohort: Study protocol and results of the first 3 years of enrollment. Epidemiol. Health 2017, 39, e2017016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Han, B.G.; KoGES Group. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.I.; Park, J.S.; Kim, R.B.; Seo, A.R.; Park, Y.J.; Kim, M.J.; Park, K.S. WHO disability assessment schedule 2.0 is related to upper and lower extremity disease-specific quality of life. Qual. Life Res. 2018, 27, 2243–2250. [Google Scholar] [CrossRef]
- Park, J.H.; Lee, C.M.; Lee, H.Y.; Kang, D.R. Estimation of Seasonal Correction Factors for Indoor Radon Concentrations in Korea. Int. J. Environ. Res. Public Health 2018, 15, 2251. [Google Scholar] [CrossRef] [Green Version]
- Angell, W.J.; Zeeb, H.; Shannon, F. WHO Handbook on Indoor Radon: A Public Health Perspective; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Marsh, J.; Birchall, A. Sensitivity analysis of the weighted equivalent lung dose per unit exposure from radon progeny. Radiat. Prot. Dosim. 2000, 87, 167–178. [Google Scholar] [CrossRef]
- Gundersen, D.A.; Delnevo, C.D.; Wackowski, O. Exploring the relationship between race/ethnicity, menthol smoking, and cessation, in a nationally representative sample of adults. Prev. Med. 2009, 49, 553–557. [Google Scholar] [CrossRef]
- Sulsky, S.I.; Fuller, W.G.; Van Landingham, C.; Ogden, M.W.; Swauger, J.E.; Curtin, G.M. Evaluating the association between menthol cigarette use and the likelihood of being a former versus current smoker. Regul. Toxicol. Pharmacol. 2014, 70, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.Y.; Park, J.H.; Lee, C.-M.; Kang, D.R. Affected model of indoor radon concentrations based on lifestyle, greenery ratio, and radon levels in groundwater. J. Health Inform. Stat. 2017, 42, 309–316. [Google Scholar] [CrossRef]
- Kim, S.H.; Koh, S.B.; Lee, C.M.; Kim, C.; Kang, D.R. Indoor Radon and Lung Cancer: Estimation of Attributable Risk, Disease Burden, and Effects of Mitigation. Yonsei Med. J. 2018, 59, 1123–1130. [Google Scholar] [CrossRef]
- Barros-Dios, J.M.; Barreiro, M.A.; Ruano-Ravina, A.; Figueiras, A. Exposure to residential radon and lung cancer in Spain: A population-based case-control study. Am. J. Epidemiol. 2002, 156, 548–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barros-Dios, J.M.; Ruano-Ravina, A.; Perez-Rios, M.; Castro-Bernardez, M.; Abal-Arca, J.; Tojo-Castro, M. Residential radon exposure, histologic types, and lung cancer risk. A case-control study in Galicia, Spain. Cancer Epidemiol. Biomark. Prev. 2012, 21, 951–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alavanja, M.C. Biologic damage resulting from exposure to tobacco smoke and from radon: Implication for preventive interventions. Oncogene 2002, 21, 7365–7375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, A.; Allen, J.; Laney, R.; Curnow, A. The cellular and molecular carcinogenic effects of radon exposure: A review. Int. J. Mol. Sci. 2013, 14, 14024–14063. [Google Scholar] [CrossRef] [Green Version]
- Mohanku, M.N.; Meenakshi, C. Radon-induced Chromosome Damage in Blood Lymphocytes of Smokers. Res. J. Environ. Toxicol. 2012, 6, 51–58. [Google Scholar] [CrossRef]
- Meenakshi, C.; Mohankumar, M.N. Synergistic effect of radon in blood cells of smokers—An in vitro study. Mutat. Res. 2013, 757, 79–82. [Google Scholar] [CrossRef]
- Morawska, L.; Phillips, C.R. Attachment of Radon Progeny to Cigarette-Smoke Aerosol. Aerosol Sci. Technol. 1992, 17, 149–158. [Google Scholar] [CrossRef]
- Biermann, A.H.; Sawyer, S.R. Attachment of Radon Progeny to Cigarette-Smoke Aerosol (No. UCRL-CR--120647.)s; Lawrence Livermore National Laboratory: Livermore, CA, USA, 1995.
- Kreuzer, M.; Walsh, L.; Schnelzer, M.; Tschense, A.; Grosche, B. Radon and risk of extrapulmonary cancers: Results of the German uranium miners′ cohort study, 1960–2003. Br. J. Cancer 2008, 99, 1946–1953. [Google Scholar] [CrossRef]
- Denman, A.R.; Rogers, S.; Ali, A.; Sinclair, J.; Phillips, P.S.; Crockett, R.G.; Groves-Kirkby, C.J. Small area mapping of domestic radon, smoking prevalence and lung cancer incidence—A case study in Northamptonshire, UK. J. Environ. Radioact. 2015, 150, 159–169. [Google Scholar] [CrossRef]
- Hornung, R.W.; Meinhardt, T.J. Quantitative risk assessment of lung cancer in U.S. uranium miners. Health Phys. 1987, 52, 417–430. [Google Scholar] [CrossRef]
- Tomasek, L.; Darby, S.C.; Swerdlow, A.J.; Placek, V.; Kunz, E. Radon exposure and cancers other than lung cancer among uranium miners in West Bohemia. Lancet 1993, 341, 919–923. [Google Scholar] [CrossRef]
- Heidenreich, W.F.; Tomasek, L.; Rogel, A.; Laurier, D.; Tirmarche, M. Studies of radon-exposed miner cohorts using a biologically based model: Comparison of current Czech and French data with historic data from China and Colorado. Radiat. Environ. Biophys. 2004, 43, 247–256. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Case (N = 519) | Control (N = 519) | p Value |
|---|---|---|---|
| Age, years | 64 [57–72] | 64 [59–72] | 0.116 |
| Sex, n (%) | N/A | ||
| Male | 253 (48.75) | 253 (48.75) | |
| Female | 266 (51.25) | 266 (51.25) | |
| Residential radon *, Bq/m3 | 65.46 ± 46.71 | 73.75 ± 60.21 | 0.013 |
| 48.32 [34.43–73.61] | 55.06 [37.71–82.78] | <0.001 | |
| High-radon dwelling †, n (%) | 71 (13.68) | 92 (17.73) | 0.007 |
| Cigarette smoking, n (%) | 222 (42.77) | 181 (34.87) | 0.009 |
| Tobacco consumption, n (%) | <0.001 | ||
| Never-smokers | 297 (57.23) | 338 (65.13) | |
| Light smokers (1–100 pack-years) | 9 (1.73) | 7 (1.35) | |
| Moderate smokers (100–365 pack-years) | 32 (6.17) | 34 (6.55) | |
| Heavy smokers (over 365 pack-years) | 178 (34.30) | 85 (16.38) | |
| Non-response | 3(0.58) | 55(10.60) | |
| Second-hand smoking, n (%) | 239 (46.05) | 110 (21.19) | <0.001 |
| Sleeping hours | 7.20 ± 1.83 | 6.76 ± 1.44 | <0.001 |
| Indoor hours | 15.88 ± 4.39 | 14.17 ± 3.69 | <0.001 |
| Housing type, n (%) | <0.001 | ||
| Single-family house | 178 (34.30) | 373 (71.87) | |
| Apartment | 180 (34.68) | 68 (13.10) | |
| Other multi-family dwelling | 161 (31.02) | 78 (15.03) | |
| Floor of residence | 4.76 ± 5.09 | 2.63 ± 3.69 | <0.001 |
| Presence of house crack, n (%) | 120 (23.12) | 145 (27.94) | 0.075 |
| Construction year | 1996 [1990–2003] | 1997 [1987–2005] | 0.638 |
| Green ratio | 48.09 ± 21.09 | 56.89 ± 18.54 | <0.001 |
| Variables | Case, n | Control, n | Conditional Logistic Regression | Conventional Logistic Regression | ||
|---|---|---|---|---|---|---|
| OR (95% CI) * | p-Value | OR (95% CI) † | p-Value | |||
| Residential radon | ||||||
| Low (< 100 Bq/m3) | 448 | 427 | 1.00 (reference) | 1.00 (reference) | ||
| High (≥ 100 Bq/m3) | 71 | 92 | 1.56 (1.03–2.37) | 0.037 | 1.52 (1.00–2.31) | 0.048 |
| Cigarette smoking | ||||||
| Non-smokers | 297 | 338 | 1.00 (reference) | 1.00 (reference) | ||
| Smokers | 222 | 181 | 2.53 (1.60–3.99) | <0.001 | 2.50 (1.59–3.94) | <0.001 |
| Tobacco consumption | ||||||
| Never-smoker | 297 | 338 | 1.00 (reference) | 1.00 (reference) | ||
| Light smokers | 9 | 7 | 3.05 (0.81–11.43) | 0.739 | 2.47 (0.68–8.56) | 0.797 |
| Moderate smokers | 32 | 34 | 2.65 (1.32–5.30) | 0.934 | 2.03 (1.11–3.71) | 0.847 |
| Heavy smokers | 178 | 85 | 5.56 (3.31–9.35) | <0.001 | 4.24 (2.92–6.15) | <0.001 |
| Radon and smoking | ||||||
| Low-radon non-smokers | 262 | 282 | 1.00 (reference) | 1.00 (reference) | ||
| High-radon non-smokers | 35 | 56 | 1.40 (0.81–2.43) | 0.231 | 1.40 (0.81–2.44) | 0.230 |
| Low-radon smokers | 186 | 145 | 2.42 (1.49–3.92) | <0.001 | 2.42 (1.50–3.91) | <0.001 |
| High-radon smokers | 36 | 36 | 4.27 (2.14–8.52) | <0.001 | 4.02 (2.03–7.97) | <0.001 |
| Variables | Case, n | Control, n | Conditional Logistic Regression | Conventional Logistic Regression | ||
|---|---|---|---|---|---|---|
| OR (95% CI) * | p-Value | OR (95% CI) † | p-Value | |||
| Residential radon | ||||||
| Low (<100 Bq/m3) | 448 | 427 | 1.00 (reference) | 1.00 (reference) | ||
| High (≥100 Bq/m3) | 71 | 92 | 1.56 (1.03–2.37) | 0.037 | 1.52 (1.00–2.31) | 0.048 |
| Smoke exposure | ||||||
| Smoke-free | 122 | 254 | 1.00 (reference) | 1.00 (reference) | ||
| Smoke-exposed | 397 | 265 | 2.67 (1.69–4.21) | <0.001 | 2.64 (1.68–4.17) | <0.001 |
| Radon and smoke exposure | ||||||
| Low-radon smoke-free | 109 | 204 | 1.00 (reference) | 1.00 (reference) | ||
| High-radon smoke-free | 13 | 50 | 1.01 (0.49–2.07) | 0.956 | 1.04 (0.51–2.13) | 0.919 |
| Low-radon smoke-exposed | 339 | 223 | 2.39 (1.48–3.87) | <0.001 | 2.41 (1.49–3.89) | <0.001 |
| High-radon smoke-exposed | 58 | 42 | 4.93 (2.57–9.45) | <0.001 | 4.65 (2.44–8.88) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, E.J.; Lee, H.; Kim, H.C.; Sheen, S.S.; Koh, S.B.; Park, K.S.; Cho, N.H.; Lee, C.-M.; Kang, D.R. Residential Radon Exposure and Cigarette Smoking in Association with Lung Cancer: A Matched Case-Control Study in Korea. Int. J. Environ. Res. Public Health 2020, 17, 2946. https://doi.org/10.3390/ijerph17082946
Park EJ, Lee H, Kim HC, Sheen SS, Koh SB, Park KS, Cho NH, Lee C-M, Kang DR. Residential Radon Exposure and Cigarette Smoking in Association with Lung Cancer: A Matched Case-Control Study in Korea. International Journal of Environmental Research and Public Health. 2020; 17(8):2946. https://doi.org/10.3390/ijerph17082946
Chicago/Turabian StylePark, Eung Joo, Hokyou Lee, Hyeon Chang Kim, Seung Soo Sheen, Sang Baek Koh, Ki Soo Park, Nam Han Cho, Cheol-Min Lee, and Dae Ryong Kang. 2020. "Residential Radon Exposure and Cigarette Smoking in Association with Lung Cancer: A Matched Case-Control Study in Korea" International Journal of Environmental Research and Public Health 17, no. 8: 2946. https://doi.org/10.3390/ijerph17082946
APA StylePark, E. J., Lee, H., Kim, H. C., Sheen, S. S., Koh, S. B., Park, K. S., Cho, N. H., Lee, C. -M., & Kang, D. R. (2020). Residential Radon Exposure and Cigarette Smoking in Association with Lung Cancer: A Matched Case-Control Study in Korea. International Journal of Environmental Research and Public Health, 17(8), 2946. https://doi.org/10.3390/ijerph17082946