Analysis of Imported Cases of COVID-19 in Taiwan: A Nationwide Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistics
3. Results
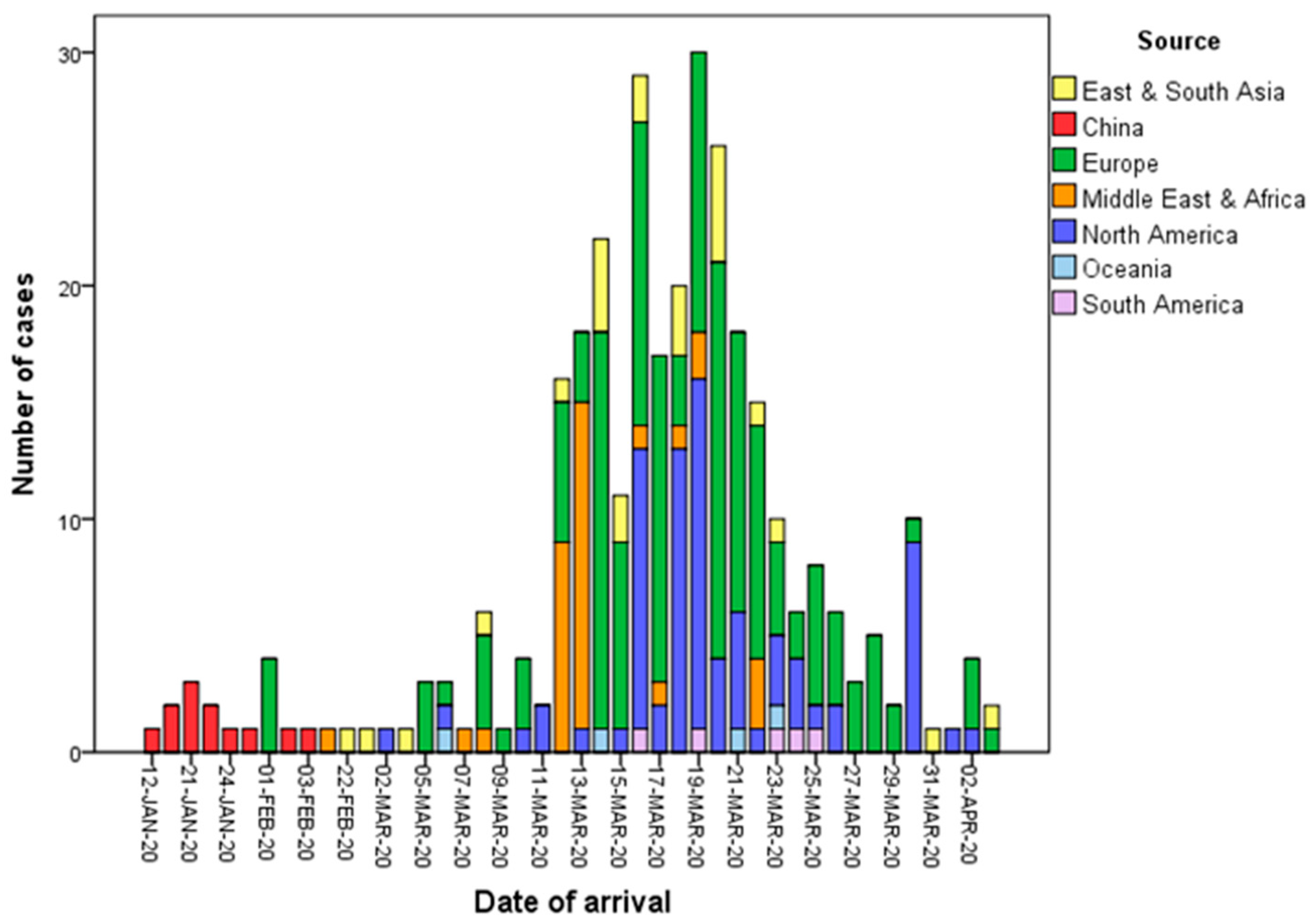
3.1. Basic Characteristics, Infection Source, and Reason for Travel
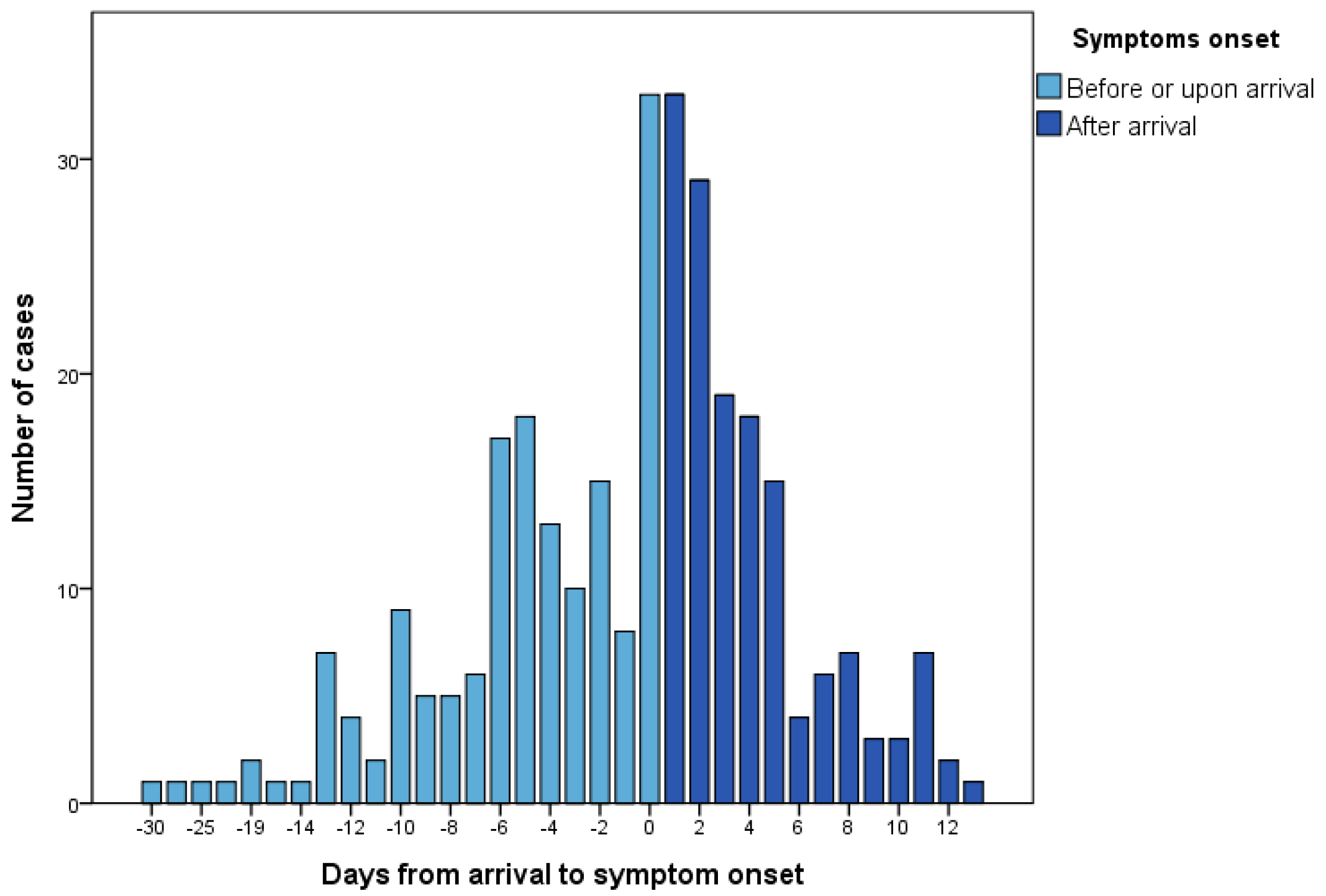
3.2. Symptom Presentation
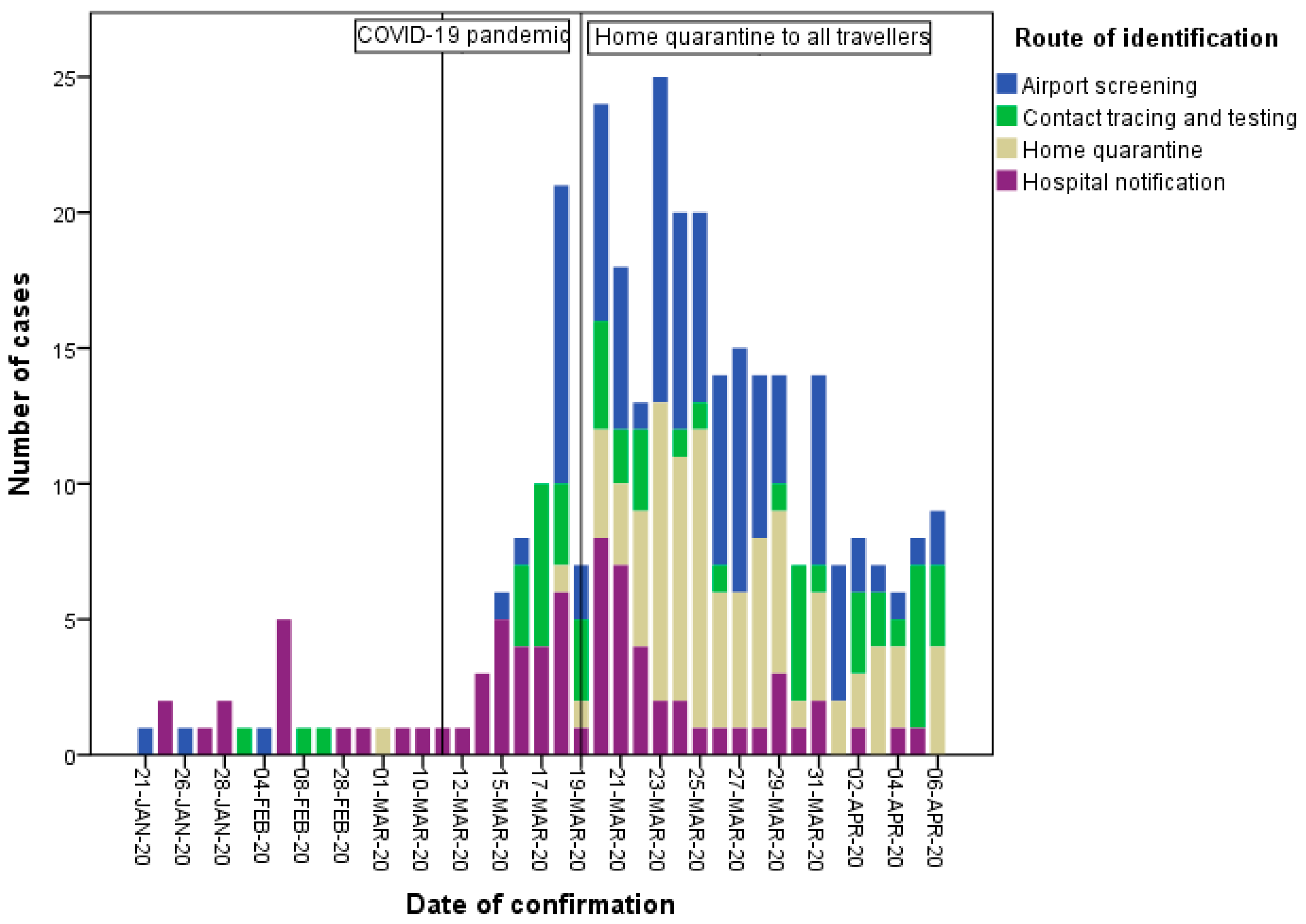
3.3. Identification Routes
3.4. Extension of Quarantine Measure after COVID-19 Declared Global Pandemic
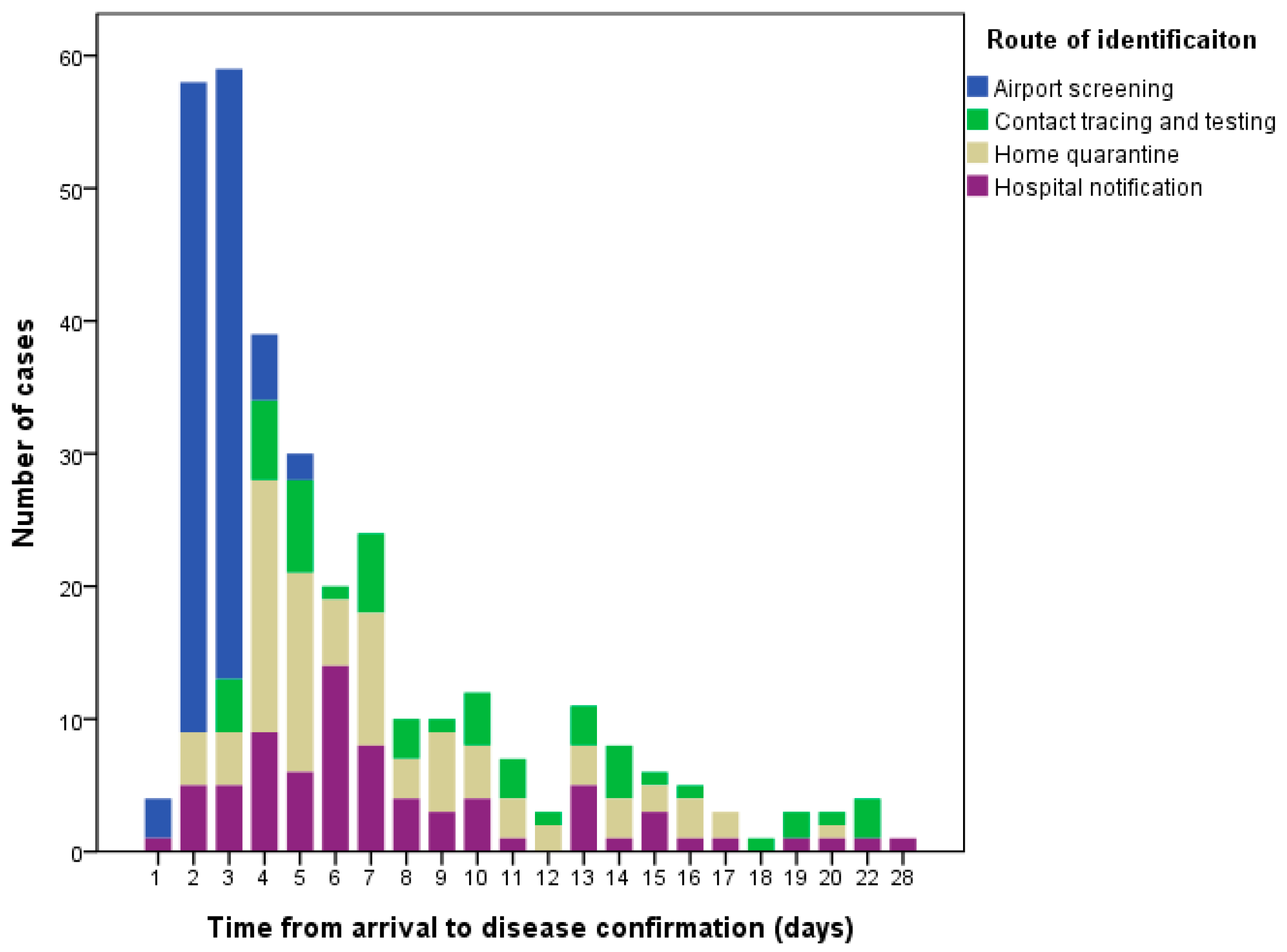
3.5. Time between Arrival and Disease Confirmation
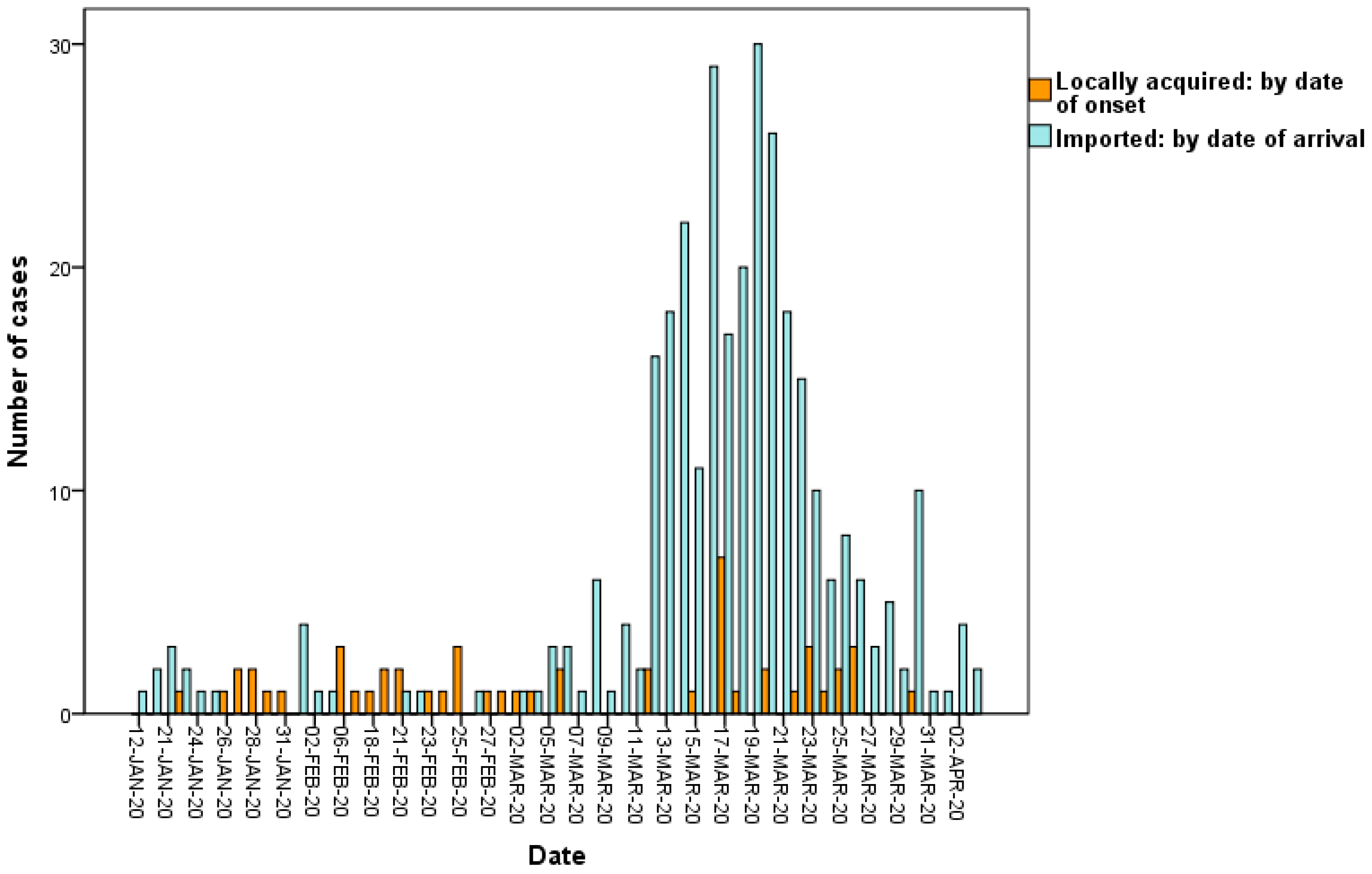
3.6. Locally Acquired Cases Infected by Imported Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 4 April 2020).
- The Center for Systems Science and Engineering, Johns Hopkins University. Coronavirus COVID-19 Global Cases. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6/ (accessed on 29 April 2020).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet (Lond. Engl.) 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) Pandemic. Available online: https://www.who.int/publications-detail/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 4 April 2020).
- Bogoch, I.I.; Watts, A.; Thomas-Bachli, A.; Huber, C.; Kraemer, M.U.G.; Khan, K. Potential for global spread of a novel coronavirus from China. J. Travel. Med. 2020, 27, taaa011. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.E.; Chen, L.H. Travellers give wings to novel coronavirus (2019-nCoV). J. Travel. Med. 2020, 27, taaa015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, C.R.; Sah, P.; Moghadas, S.M.; Pandey, A.; Shoukat, A.; Wang, Y.; Wang, Z.; Meyers, L.A.; Singer, B.H.; Galvani, A.P. Impact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak. Proc. Natl. Acad. Sci. USA 2020, 117, 7504–7509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Pastore, Y.P.A.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A. Wuhan novel coronavirus (COVID-19): Why global control is challenging? Public Health 2020, 179, A1–A2. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Li, S.Y.; Yang, C.H. Initial rapid and proactive response for the COVID-19 outbreak—Taiwan’s experience. J. Formos. Med. Assoc. 2020, 119, 771–773. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big Data Analytics, New Technology, and Proactive Testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel. Med. 2020, 27, taaa020. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Centers for Disease Control. Press Releases. Available online: https://www.cdc.gov.tw/En (accessed on 4 April 2020).
- Taiwan Centers for Disease Control. CECC Urges People Subject to Home Quarantine/Isolation to Follow Related Regulations to Protect Everyone’s Health. Available online: https://www.cdc.gov.tw/En/Bulletin/Detail/mhkl82LMg-mKGeltPu7JPw?typeid=158 (accessed on 4 April 2020).
- Parmet, W.E.; Sinha, M.S. Covid-19—The Law and Limits of Quarantine. N. Engl. J. Med. 2020, 382, e28. [Google Scholar] [CrossRef] [PubMed]
- Salathe, M.; Althaus, C.L.; Neher, R.; Stringhini, S.; Hodcroft, E.; Fellay, J.; Zwahlen, M.; Senti, G.; Battegay, M.; Wilder-Smith, A.; et al. COVID-19 epidemic in Switzerland: On the importance of testing, contact tracing and isolation. Swiss Med. Wkly. 2020, 150, w20225. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet (Lond. Engl.) 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Nicastri, E.; D’Abramo, A.; Faggioni, G.; De Santis, R.; Mariano, A.; Lepore, L.; Molinari, F.; Petralito, G.; Fillo, S.; Munzi, D.; et al. Coronavirus disease (COVID-19) in a paucisymptomatic patient: Epidemiological and clinical challenge in settings with limited community transmission, Italy, February 2020. Euro Surveill. 2020, 25, 2000230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautier, J.F.; Ravussin, Y. A New Symptom of COVID-19: Loss of Taste and Smell. Obes. (Silver Spring) 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munster, V.J.; Koopmans, M.; van Doremalen, N.; van Riel, D.; de Wit, E. A Novel Coronavirus Emerging in China—Key Questions for Impact Assessment. N. Engl. J. Med. 2020, 382, 692–694. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | No. of Cases (N = 321) (%) | Date of Arrival | Date of Confirmation | Reasons for Travel | |
|---|---|---|---|---|---|
| Taiwanese (n = 310) | Non-Taiwanese (n = 11) | ||||
| China (Wuhan) | 11 (3.4) | 12/1–3/2 | 21/1–6/2 | business, tourism, residency | tourism |
| Macao | 1 (0.3) | 24/1 | 6/2 | tourism | |
| Italy | 7 (2.2) | 1/2–19/3 | 6/2—24/3 | tourism, study, business | |
| Egypt | 12 (3.7) | 21/2–19/3 | 29/2–30/3 | tourism | |
| Dubai | 10 (3.1) | 21/2–13/3 | 29/2–17/3 | tourism | |
| Japan | 2 (0.6) | 22/2–8/3 | 28/2–15/3 | tourism | |
| United States | 81 (25.2) | 2/3–2/4 | 18/3–6/4 | tourism, study, residency, business, family visit, conference, work | business, work |
| Philippines | 11 (3.4) | 3–23/3 | 5–31/3 | tourism, family visit, study, business, work | |
| Greece | 1 (0.3) | 5/3 | 15/3 | tourism | |
| Netherlands | 8 (2.5) | 5–20/3 | 10–25/3 | business, tourism, study | |
| Germany | 10 (3.1) | 6–21/3 | 14/3–4/4 | business, tourism, sporting event, work | |
| Mexico | 2 (0.6) | 6/3–21/3 | 20/3–26/3 | tourism | |
| Australia | 2 (0.6) | 6/3–23/3 | 27/3–28/3 | work, business | |
| United Kingdom | 73 (22.7) | 8/3–4/4 | 11/3–6/4 | tourism, study, business, sporting event, residency, work, religion | |
| Belgium | 4 (1.2) | 8–20/3 | 12–25/3 | tourism, study | |
| Switzerland | 6 (1.9) | 8–20/3 | 14–31/3 | tourism, study, business | |
| France | 21 (6.5) | 8–27/3 | 14–31/3 | tourism, business, study, work | tourism, family visit |
| Turkey | 18 (5.6) | 8–20/3 | 15–29/3 | tourism | |
| Thailand | 6 (1.9) | 8–20/3 | 15/3–3/4 | tourism, study | |
| Portugal | 2 (0.6) | 9/3–16/3 | 20/3–29/3 | tourism | |
| Ireland | 4 (1.2) | 9–20/3 | 12–28/3 | tourism, study, business | |
| Spain | 17 (5.3) | 9–27/3 | 15–29/3 | tourism, study | |
| Austria | 10 (3.1) | 10–14/3 | 14/3–5/4 | tourism | work |
| Iceland | 4 (1.2) | 10–28/3 | 17/3–6/4 | tourism | |
| Indonesia | 8 (2.5) | 12/3–4/4 | 18/3–6/4 | tourism, work | wedding, work |
| Czech Republic | 15 (4.7) | 14–20/3 | 16/3–5/4 | tourism, work, study, business | |
| New Zealand | 2 (0.6) | 14/3–21/3 | 22/3–26/3 | tourism | |
| Poland | 1 (0.3) | 15/3 | 20/3 | study tour | |
| Denmark | 2 (0.6) | 15/3 | 22/3–2/4 | family visit | |
| Qatar | 2 (0.6) | 16/3–19/3 | 18/3–25/3 | business | |
| Countries in South America | 5 (1.6) | 16–25/3 | 23/3–4/4 | tourism | |
| Canada | 2 (0.6) | 16/3–26/3 | 20/3–28/3 | tourism, study | |
| Malaysia | 1 (0.3) | 16/3 | 26/3 | business | |
| Luxembourg | 1 (0.3) | 17/3 | 20/3 | tourism | |
| Singapore | 1 (0.3) | 18/3 | 20/3 | business | |
| South Africa | 1 (0.3) | 18/3 | 21/3 | business | |
| Monaco | 3 (0.9) | 22/3 | 26/3–5/4 | tourism | |
| Tunisia | 1 (0.3) | 27/3 | 29/3 | study tour | |
| Category and Presentation | n | % |
|---|---|---|
| Generalised symptoms | ||
| Fever | 144 | 44.9 |
| Chills | 9 | 2.8 |
| Malaise | 52 | 16.2 |
| Myalgia or arthralgia | 40 | 12.5 |
| Respiratory symptoms | 233 | 72.6 |
| Cough | 146 | 45.5 |
| Sore throat | 100 | 31.2 |
| Rhinorrhoea, sneezing, nasal stuffiness | 96 | 29.9 |
| Chest tightness or pain | 18 | 5.6 |
| Dyspnea | 11 | 3.4 |
| Neurological symptoms | 76 | 23.7 |
| Loss of smell or taste | 42 | 13.1 |
| Headache | 34 | 10.6 |
| Dizziness | 6 | 1.9 |
| Gastrointestinal symptoms | 26 | 8.1 |
| Diarrhoea | 23 | 7.2 |
| Abdominal pain | 3 | 0.9 |
| Nausea or vomiting | 3 | 0.9 |
| Ophthalmic symptoms | ||
| Itching, congestion, or pain in the eyes | 6 | 1.9 |
| No symptoms | 11 | 3.4 |
| Route of Identification | n (%) | No. of Locally Acquired Cases as Their Infectees | R * (95% CI) | Days from Arrival to Disease Confirmation Mean (95% CI) |
|---|---|---|---|---|
| Airport screening | 105 (32.7) | 0 | 0 (0–0) ** | 2.6 (2.4–2.7) *** |
| Home quarantine | 89 (27.7) | 4 | 0.04 (0.00–0.09) | 7.4 (6.5–8.3) |
| Contact tracing | 52 (16.2) | 8 | 0.15 (0.00–0.30) | 9.7 (8.2–11.3) |
| Hospital notification | 75 (23.4) | 7 | 0.09 (0.02–0.17) | 7.8 (6.7–9.0) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.-Y.; Chen, T.-J.; Hwang, S.-J. Analysis of Imported Cases of COVID-19 in Taiwan: A Nationwide Study. Int. J. Environ. Res. Public Health 2020, 17, 3311. https://doi.org/10.3390/ijerph17093311
Liu J-Y, Chen T-J, Hwang S-J. Analysis of Imported Cases of COVID-19 in Taiwan: A Nationwide Study. International Journal of Environmental Research and Public Health. 2020; 17(9):3311. https://doi.org/10.3390/ijerph17093311
Chicago/Turabian StyleLiu, Jui-Yao, Tzeng-Ji Chen, and Shinn-Jang Hwang. 2020. "Analysis of Imported Cases of COVID-19 in Taiwan: A Nationwide Study" International Journal of Environmental Research and Public Health 17, no. 9: 3311. https://doi.org/10.3390/ijerph17093311
APA StyleLiu, J. -Y., Chen, T. -J., & Hwang, S. -J. (2020). Analysis of Imported Cases of COVID-19 in Taiwan: A Nationwide Study. International Journal of Environmental Research and Public Health, 17(9), 3311. https://doi.org/10.3390/ijerph17093311