
The Effect of Dietary Intake and Nutritional Status on Anthropometric Development and Systemic Inflammation: An Observational Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
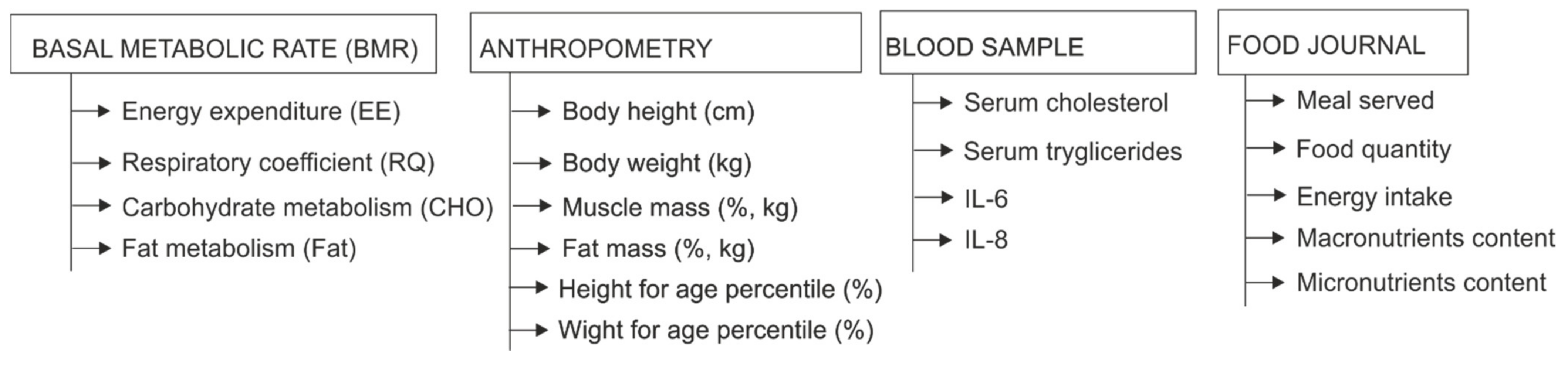
2.3. Test Applied
2.4. Basal Metabolic Rate (BMR)
2.5. Anthropometric Measurements
2.6. Blood Samples
2.7. Daily Food Intake
2.8. Statistical Evaluation
3. Results
3.1. Demographic Analysis
3.2. Basal Metabolic Rate—Energy Expenditure
3.3. Nutritional Intake
3.4. Daily Food Intake: Calories, Nutrients and Influence over the Blood Samples
4. Discussion
4.1. Basal Metabolic Rate vs. Daily Food Intake
4.2. Food Intake, Anthropometric Differences and Changes in Blood Samples
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Camacho, S.; Ruppel, A. Is the calorie concept a real solution to the obesity epidemic? Glob. Health Action 2017, 10. [Google Scholar] [CrossRef] [Green Version]
- Cordellat, A.; Padilla, B.; Grattarola, P.; García-Lucerga, C.; Crehuá-Gaudiza, E.; Núñez, F.; Martínez-Costa, C.; Blasco-Lafarga, C. Multicomponent Exercise Trainin Combined with Nutritional Counselling Improves Physical Function, Biochemical and Anthropometric Profiles in Obese Children: A Pilot Study. Nutrients 2020, 12, 2723. [Google Scholar] [CrossRef]
- Mager, D.R.; Yap, J.; Rodriguez-Dimitrescu, C.; Mazurak, V.; Ball, G.; Gilmour, S. Anthropometric measures of visceral and subcutaneous fat are important in the determination of metabolic dysregulation in boys and girls at risk for nonalcoholic fatty liver disease. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parent. Enter Nutr. 2013, 28, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Martínez Valverde, A. Effects of childhood nutrition on adult health. Allergol. Immunopathol. (Madr.) 2003, 31, 166–172. [Google Scholar] [CrossRef]
- Hoffman, D.J. Early nutrition and adult health: Perspectives for international and community nutrition programs and policies. Nutr. Res. Pract. 2010, 4, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Kaikkonen, J.E.; Mikkilä, V.; Magnussen, C.G.; Juonala, M.; Viikari, J.S.A.; Raitakari, O.T. Does childhood nutrition influence adult cardiovascular disease risk?—insights from the Young Finns Study. Ann. Med. 2013, 45, 120–128. [Google Scholar] [CrossRef]
- Nutrition and Cardiovascular Health. 2018. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6320919/ (accessed on 15 April 2021).
- Giugliano, D.; Ceriello, A.; Esposito, K. The Effects of Diet on Inflammation: Emphasis on the Metabolic Syndrome. J. Am. Coll Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef] [Green Version]
- Minihane, A.M.; Vinoy, S.; Russell, W.R.; Baka, A.; Roche, H.M.; Tuohy, K.; Teeling, J.L.; Blaak, E.E.; Fenech, M.; Vauzour, D.; et al. Low-grade inflammation, diet composition and health: Current research evidence and its translation. Br. J. Nutr. 2015, 114, 999–1012. [Google Scholar] [CrossRef] [Green Version]
- Alwarawrah, Y.; Kiernan, K.; Maciver, N.J. Changes in Nutritional Status Impact Immune Cell Metabolism and Function. Front. Immunol. 2018, 9, 1055. [Google Scholar] [CrossRef] [Green Version]
- Makki, K.; Froguel, P.; Wolowczuk, I. Adipose Tissue in Obesity-Related Inflammation and Insulin Resistance: Cells, Cytokines, and Chemokines. Int. Sch. Res. Not. Inflamm. 2013, 2013, e139239. [Google Scholar] [CrossRef] [Green Version]
- Juncal-Ruiz, M.; Riesco-Dávila, L.; De La Foz, V.O.-G.; Ramírez-Bonilla, M.; Martínez-García, O.; Irure-Ventura, J.; Leza, J.C.; López-Hoyos, M.; Crespo-Facorro, B. The effect of excess weight on circulating inflammatory cytokines in drug-naïve first-episode psychosis individuals. J. Neuroinflamm. 2018, 15. [Google Scholar] [CrossRef] [Green Version]
- Huffman, K.M.; Slentz, C.A.; Bales, C.W.; Houmard, J.A.; Kraus, W.E. Relationships between Adipose Tissue and Cytokine Responses to a Randomized Controlled Exercise Training Intervention. Metabolism 2008, 57, 577–583. [Google Scholar] [CrossRef] [Green Version]
- Agita, A.; Alsagaff, M.T. Inflammation, Immunity, and Hypertension. Acta Med. Indones. 2017, 49, 158–165. [Google Scholar]
- Smykiewicz, P.; Segiet, A.; Keag, M.; Żera, T. Proinflammatory cytokines and ageing of the cardiovascular-renal system. Mech Ageing Dev. 2018, 175, 35–45. [Google Scholar] [CrossRef]
- Zhu, J.-Z.; Yi, H.-W.; Huang, W.; Pang, T.; Zhou, H.-P.; Wu, X.-D. Fatty liver diseases, mechanisms, and potential therapeutic plant medicines. Chin. J. Nat. Med. 2020, 18, 161–168. [Google Scholar] [CrossRef]
- Morton, G.J.; Meek, T.H.; Schwartz, M.W. Neurobiology of food intake in health and disease. Nat. Rev. Neurosci. 2014, 15, 367–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Physiological Responses to Food Intake throughout the Day. Available online: https://www.researchgate.net/publication/261102019 (accessed on 15 April 2021).
- Hopkins, M.; Blundell, J.; Halford, J.; King, N.; Finlayson, G. The Regulation of Food Intake in Humans. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Grossman, A., Hershman, J.M., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: http://www.ncbi.nlm.nih.gov/books/NBK278931/ (accessed on 15 April 2021).
- Balliett, M.; Burke, J.R. Changes in anthropometric measurements, body composition, blood pressure, lipid profile, and testosterone in patients participating in a low-energy dietary intervention. J. Chiropr. Med. 2013, 12, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Alam, I.; Larbi, A.; Pawelec, G.; Paracha, P.I. Relationship between anthropometric variables and nutrient intake in apparently healthy male elderly individuals: A study from Pakistan. Nutr. J. 2011, 10, 111. [Google Scholar] [CrossRef] [Green Version]
- Peckmezian, T.; Hay, P. A systematic review and narrative synthesis of interventions for uncomplicated obesity: Weight loss, well-being and impact on eating disorders. J. Eat. Disord. 2017, 5, 15. [Google Scholar] [CrossRef] [Green Version]
- De la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Zazpe, I.; Vazquez-Ruiz, Z.; Benito-Corchon, S.; Bes-Rastrollo, M. Glycemic load, glycemic index, bread and incidence of overweight/obesity in a Mediterranean cohort: The SUN project. BMC Public Health 2014, 14, 1091. [Google Scholar] [CrossRef] [Green Version]
- Rautiainen, S.; Wang, L.; Lee, I.-M.; Manson, J.E.; Buring, J.E.; Sesso, H.D. Higher Intake of Fruit, but Not Vegetables or Fiber, at Baseline Is Associated with Lower Risk of Becoming Overweight or Obese in Middle-Aged and Older Women of Normal BMI at Baseline. J. Nutr. 2015, 145, 960–968. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Hu, F.B.; Colditz, G.A.; Manson, J.E.; Willett, W.C.; Liu, S. Changes in intake of fruits and vegetables in relation to risk of obesity and weight gain among middle-aged women. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2004, 28, 1569–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlesinger, S.; Neuenschwander, M.; Schwedhelm, C.; Hoffmann, G.; Bechthold, A.; Boeing, H.; Schwingshackl, L. Food Groups and Risk of Overweight, Obesity, and Weight Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2019, 10, 205–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ability of the Harris Benedict Formula to Predict Energy Requirements Differs with Weight History and Ethnicity. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2598419/ (accessed on 12 April 2021).
- Davidson, L.E.; Wang, J.; Thornton, J.C.; Kaleem, Z.; Silva-Palacios, F.; Pierson, R.N.; Heymsfield, S.B.; Gallagher, D. Predicting Fat Percent by Skinfolds in Racial Groups: Durnin and Womersley Revisited. Med. Sci. Sports Exerc. 2011, 43, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Defining Childhood Obesity. Overweight & Obesity. CDC. Published . 24 July 2019. Available online: https://www.cdc.gov/obesity/childhood/defining.html (accessed on 15 April 2021).
- FoodData Central. Available online: https://fdc.nal.usda.gov/ (accessed on 21 April 2021).
- Stubelj, M.; Teraž, K.; Vatovec, T.P. Predicting Equations and Resting Energy Expenditure Changes in Overweight Adults. Zdr. Varst. 2020, 59, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Anderegg, B.A.; Worrall, C.; Barbour, E.; Simpson, K.N.; DeLegge, M. Comparison of resting energy expenditure prediction methods with measured resting energy expenditure in obese, hospitalized adults. J. Parenter. Enteral Nutr. 2009, 33, 168–175. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; Jurado-Fasoli, L.; De-la-O, A.; Gutierrez, Á.; Castillo, M.J.; Ruiz, J.R. Accuracy and Validity of Resting Energy Expenditure Predictive Equations in Middle-Aged Adults. Nutrients 2018, 10, 1635. [Google Scholar] [CrossRef] [Green Version]
- Periasamy, M.; Herrera, J.L.; Reis, F.C.G. Skeletal Muscle Thermogenesis and Its Role in Whole Body Energy Metabolism. Diabetes Metab. J. 2017, 41, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Gavini, C.K.; Mukherjee, S.; Shukla, C.; Britton, S.L.; Koch, L.G.; Shi, H.; Novak, C.M. Leanness and heightened nonresting energy expenditure: Role of skeletal muscle activity thermogenesis. Am. J. Physiol. Endocrinol. Metab. 2014, 306, E635–E647. [Google Scholar] [CrossRef] [Green Version]
- Friedman, M.I.; Appel, S. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men: A secondary analysis of energy expenditure and physical activity. PLoS ONE 2019, 14, e0222971. [Google Scholar] [CrossRef] [Green Version]
- Veldhorst, M.A.B.; Westerterp-Plantenga, M.S.; Westerterp, K.R. Gluconeogenesis and energy expenditure after a high-protein, carbohydrate-free diet. Am. J. Clin. Nutr. 2009, 90, 519–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartorius, K.; Sartorius, B.E.; Madiba, P.T.; Stefan, C. Does high-carbohydrate intake lead to increased risk of obesity? A systematic review and meta-analysis. BMJ Open. 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Carbone, J.W.; Pasiakos, S.M. Dietary Protein and Muscle Mass: Translating Science to Application and Health Benefit. Nutrients 2019, 11, 1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martens, E.A.; Gonnissen, H.K.; Gatta-Cherifi, B.; Janssens, P.L.; Westerterp-Plantenga, M.S. Maintenance of energy expenditure on high-protein vs. high-carbohydrate diets at a constant body weight may prevent a positive energy balance. Clin. Nutr. Edinb. Scotl. 2015, 34, 968–975. [Google Scholar] [CrossRef]
- Westerterp-Plantenga, M.S. Protein intake and energy balance. Regul. Pept. 2008, 149, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Riccardi, G.; Giacco, R.; Rivellese, A.A. Dietary fat, insulin sensitivity and the metabolic syndrome. Clin. Nutr. Edinb. Scotl. 2004, 23, 447–456. [Google Scholar] [CrossRef]
- Beulen, Y.; Martínez-González, M.A.; van de Rest, O.; Salas-Salvadó, J.; Sorlí, J.V.; Gómez-Gracia, E.; Fiol, M.; Estruch, R.; Santos-Lozano, J.M.; Schröder, H.; et al. Quality of Dietary Fat Intake and Body Weight and Obesity in a Mediterranean Population: Secondary Analyses within the PREDIMED Trial. Nutrients 2018, 10, 2011. [Google Scholar] [CrossRef] [Green Version]
- Hooper, L.; Abdelhamid, A.; Bunn, D.; Brown, T.; Summerbell, C.D.; Skeaff, C.M. Effects of total fat intake on body weight. Cochrane Database Syst. Rev. 2015, 8, CD011834. [Google Scholar] [CrossRef] [Green Version]
- Othman, F.; Mohamad Nor, N.S.; Appannah, G.; Zaki, N.A.M.; Ambak, R.; Omar, A.; Fazliana, M.; Salleh, R.; Yusof, B.N.M.; Muksan, N.; et al. Prediction of body fat loss in relation to change in nutrient intake among housewives participating in the MyBFF@home study. BMC Women Health 2018, 18, 102. [Google Scholar] [CrossRef]
- Comparative Analysis of Serum Levels of Total Carbohydrates and Protein Linked Carbohydrates in Normal and Diabetic Individuals. Available online: https://web.a.ebscohost.com/abstract?direct=true&profile=ehost&scope=site&authtype=crawler&jrnl=0973709X&AN=136644015&h=TGKOG5cIqTzHt69YiGuXs3e%2fVsyLZpPT9vM2HMIunwHhM%2beAGOuE4I%2fQCbBlkfz%2bQWhJDVSJm00XxXkB7WVahA%3d%3d&crl=c&resultNs=AdminWebAuth&resultLocal=ErrCrlNotAuth&crlhashurl=login.aspx%3fdirect%3dtrue%26profile%3dehost%26scope%3dsite%26authtype%3dcrawler%26jrnl%3d0973709X%26AN%3d136644015 (accessed on 15 April 2021).
- Bopp, M.J.; Houston, D.K.; Lenchik, L.; Easter, L.; Kritchevsky, S.B.; Nicklas, B.J. Lean Mass Loss Is Associated with Low Protein Intake during Dietary-Induced Weight Loss in Postmenopausal Women. J. Am. Diet. Assoc. 2008, 108, 1216–1220. [Google Scholar] [CrossRef] [Green Version]
- Nabuco, H.C.; Tomeleri, C.M.; Sugihara Junior, P.; dos Reis Fernandes, R.; Cavalcante, E.F.; Antunes, M.; Burini, R.C.; Venturini, D.; Barbosa, D.S.; Silva, A.M.; et al. Lower protein and higher carbohydrate intake are related with altering metabolic syndrome components in elderly women: A cross-sectional study. Exp. Gerontol. 2018, 103, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Koga, N.; Ogura, J.; Yoshida, F.; Hattori, K.; Hori, H.; Aizawa, E.; Ishida, I.; Kunugi, H. Altered polyunsaturated fatty acid levels in relation to proinflammatory cytokines, fatty acid desaturase genotype, and diet in bipolar disorder. Transl. Psychiatry 2019, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Telle-Hansen, V.H.; Christensen, J.J.; Ulven, S.M.; Holven, K.B. Does dietary fat affect inflammatory markers in overweight and obese individuals?—A review of randomized controlled trials from 2010 to 2016. Genes Nutr. 2017, 12. [Google Scholar] [CrossRef]
- Hendy, G.N.; Canaff, L. Calcium-sensing receptor, proinflammatory cytokines and calcium homeostasis. Semin. Cell Dev. Biol. 2016, 49, 37–43. [Google Scholar] [CrossRef]
- Moslehi, N.; Vafa, M.; Rahimi-Foroushani, A.; Golestan, B. Effects of oral magnesium supplementation on inflammatory markers in middle-aged overweight women. J. Res. Med. Sci Off. J. Isfahan Univ. Med. Sci. 2012, 17, 607–614. [Google Scholar]
- Ghishan, F.K.; Kiela, P.R. Vitamins and minerals in IBD. Gastroenterol. Clin. N. Am. 2017, 46, 797–808. [Google Scholar] [CrossRef]
- Yin, K.; Agrawal, D.K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar] [CrossRef] [Green Version]
- Pecora, F.; Persico, F.; Argentiero, A.; Neglia, C.; Esposito, S. The Role of Micronutrients in Support of the Immune Response against Viral Infections. Nutrients 2020, 12, 3198. [Google Scholar] [CrossRef]
- Zavala, G.; Long, K.Z.; García, O.P.; del Carmen Caamaño, M.; Aguilar, T.; Salgado, L.M.; Rosado, J.L. Specific micronutrient concentrations are associated with inflammatory cytokines in a rural population of Mexican women with a high prevalence of obesity. Br. J. Nutr. 2013, 109, 686–694. [Google Scholar] [CrossRef] [Green Version]
- El-Zayat, S.R.; Sibaii, H.; Mannaa, F.A. Micronutrients and many important factors that affect the physiological functions of toll-like receptors. Bull. Natl. Res. Cent. 2019, 43, 123. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Macronutrient | Median (Min to Max) | % of the Median Energy Need |
|---|---|---|
| Carbohydrates (g/day) | 906.1 (709.3 to 1143.9 kcal) | 54.06 (42.32 to 68.25 kcal) |
| Fats (g/day) | 688.2 (530.1 to 855.6 kcal) | 41.06 (31.62 to 51.05%) |
| Macronutrient | Median (Min to Max) | CV, % | |
|---|---|---|---|
| Carbohydrates (g/day) | 207.6 (100 to 393 ) | 29.37 | |
| Sugars (g/day) | 42.32 (10.5 to 110.9) | 40.74 | |
| Fibers (g/day) | 25.51 (10.24 to 110.9) | 30.41 | |
| Proteins (g/day) | 79.2 (28.2 to 227.9) | 36.63 | |
| Fats (g/day) | 72.53 (16.55 to 164.3) | 39.80 | |
| Saturated fats (g/day) | 735.4 (4.03 to 3966) | 12.94 | |
| Monounsaturated fats (g/day) | 9.44 (0.70 to 42.5) | 73.76 | |
| Polyunsaturated fats (g/day) | 4.03 (0.73 to 31.01) | 93.85 | |
| Trans fats (g/day) | 0.08 (0 to 110.9) | 134.72 | |
| Cholesterol (g/day) | 237.2 (14 to 818.8) | 60.14 | |
| Macronutrient | Median (Min to Max) | CV, % | |
|---|---|---|---|
| Iron (mg/day) | 15.2 (5.68 to 26.27) | 32.52 | |
| Calcium (mg/day) | 14.06 (90.9 to 3530) | 50.69 | |
| Magnesium (mg/day) | 140.1 (56.7 to 313.1) | 43.53 | |
| Phosphorus (mg/day) | 641.1 (141.7 to 2094) | 48.59 | |
| Potassium (mg/day) | 1713 (6936.3 to 3766) | 38.79 | |
| Sodium (mg/day) | 2868 (672.3 to 4493) | 31.72 | |
| Zinc (mg/day) | 8.25 (0.195 to 240.7) | 109.67 | |
| Selenium (mg/day) | 8.60 (0 to 78.6) | 109.66 | |
| Vitamin | A (µg/day) | 677.2 (83.52 to 29,171) | 207.14 |
| C (mg/day) | 28.87 (0.6 to 12.24) | 86.37 | |
| B12 (µg/day) | 1.21 (0 to 12.24) | 105.69 | |
| B1 (mg/day) | 0.93 (0.149 to 1.96) | 46.71 | |
| B6 (mg/day) | 0.98 (0.33 to 3.00) | 49.96 | |
| K (µg/day) | 16.95 (0 to 489.5) | 183 | |
| E (mg/day) | 1.22 (0.118 to 8.07) | 94.65 | |
| Folic Acid (µg/day) | 7.2 (0 to 386.6) | 212.44 | |
| Macronutrient Intakes (Median, Min to Max) | Laboratory Parameters (Median, Min to Max) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IL-6 (pg/mL) (1.41, 0.05 to 5.98) | IL-8 (pg/mL) (7.09, 0.72 to 38.9) | Cholesterol (mg/dL) (144.7, 91.33 to 245.3) | Triglycerides mg/dL) (49.46, 25.67 to 152.4) | Total Proteins (g/L) (69.13, 59.71 to 76.41) | ||||||
| p | r | p | r | p | r | p | r | p | r | |
| Energy intake (kcal/day): 1854, 773.4 to 3606 | 0.446 | −0.074 | 0.560 | 0.056 | 0.822 | 108 | 0.749 | 0.031 | 0.0327 | 0.205 |
| Carbohydrate intake (g/day): 207.6, 100.3 to 393 | 0.114 | −0.152 | 0.066 | 0.177 | 0.400 | 0.081 | 0.787 | −0.026 | 0.006 | −0.262 |
| Fat intake (g/day): 72.53, 16.55 to 164.3 | 0.598 | 0.051 | 0.802 | 0.024 | 0.472 | −0.069 | 0.633 | 0.046 | 0.1617 | −0.135 |
| Protein intake (g/day): 79.2, 28.2 to 227.9 | 0.847 | 0.018 | 0.862 | −0.016 | 0.252 | −0.111 | 0.333 | −0.093 | 0.066 | −0.177 |
| Cholesterol (mg/day): 237.2, 14 to 818.8 | 0.179 | 0.130 | 0.321 | −0.096 | 0.046 | 0.635 | 0.034 | 0.161 | 0.889 | −0.0135 |
| Saturated fat (g/day): 735.4, 4.03 to 3966 | 0.330 | −0.094 | 0.918 | −0.010 | 0.881 | −0.014 | 0.069 | −0.175 | 0.196 | −0.125 |
| Monounsaturated fats(g/day): 9.44, 0.70 to 42.5 | 0.179 | −0.130 | 0.466 | −0.070 | 0.191 | −0.126 | 0.144 | 0.141 | 0.017 | −0.227 |
| Polyunsaturated fats (g/day): 4.03, 0.73 to 31.01 | 0.004 | −0.271 | 0.613 | −0.049 | 0.884 | −0.014 | 0.468 | 0.070 | 0.028 | −0.215 |
| Trans fats (g/day): 0.08, 0 to 110.9 | 0.294 | −0.101 | 0.202 | −0.123 | 0.002 | 0.223 | 0.045 | 0.192 | 0.002 | −0.286 |
| Sugar (g/day): 42.32, 10.5 to 110.9 | 0.018 | 0.226 | 0.720 | 0.034 | 0.949 | −0.006 | 0.048 | 0.190 | 0.449 | −0.073 |
| Fibers (g/day): 25.51, 10.24 to 110.9 | 0.000 | −0.330 | 0.300 | 0.100 | 0.9009 | 0.012 | 0.039 | −0.198 | 0.001 | −0.297 |
| Micronutrient Intakes (Median, Min to Max) | Laboratory Parameters (Median, Min to Max) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IL-6 (pg/mL) (1.41, 0.05 to 5.98) | IL-8 (pg/mL) (7.09, 0.72 to 38.9) | Cholesterol (mg/dL) (144.7, 91.33 to 245.3) | Triglycerides mg/dL) (49.46, 25.67 to 152.4) | Total Proteins (g/L) (69.13, 59.71 to 76.41) | ||||||
| p | r | p | r | p | r | p | r | p | r | |
| Iron (mg/day): 15.2, 5.68 to 26.27 | 0.179 | −0.130 | 0.213 | 0.120 | 0.838 | 0.019 | 0.062 | 0.179 | 0.154 | −0.137 |
| Calcium (mg/day): 14.06, 90.9 to 3530 | 0.285 | −0.103 | 0.038 | −0.199 | 0.092 | −0.162 | 0.482 | 0.068 | 0.0001 | −0.356 |
| Magnesium (mg/day): 140.1, 56.7 to 313.1 | 0.047 | −0.191 | 0.521 | 0.062 | 0.167 | −0.133 | 0.192 | 0.126 | 0.040 | −0.197 |
| Phosphorus (mg/day): 641.1, 141.7 to 2094 | 0.335 | −0.093 | 0.861 | −0.017 | 0.163 | −0.135 | 0.173 | 0.131 | 0.015 | −0.232 |
| Potassium (mg/day): 1713, 6936.3 to 3766 | 0.259 | −0.109 | 0.395 | 0.082 | 0.018 | −0.226 | 0.386 | 0.084 | 0.030 | −0.208 |
| Sodium (mg/day): 2868, 672.3 to 4493 | 0.384 | −0.084 | 0.854 | 0.017 | 0.604 | 0.050 | 0.890 | −0.013 | 0.0001 | −0.366 |
| Zinc (mg/day): 8.25, 0.195 to 240.7 | 0.582 | 0.053 | 0.067 | 0.176 | 0.5625 | −0.056 | 0.005 | 0.265 | 0.493 | −0.066 |
| Selenium (mg/day): 8.60, 0 to 78.6 | 0.358 | 0.089 | 0.250 | 0.111 | 0.286 | −0.103 | 0.371 | 0.086 | 0.158 | −0.136 |
| Vitamin A (µg/day): 677.2, 83.52 to 29,171 | 0.048 | −0.19 | 0.984 | 0.001 | 0.012 | −0.239 | 0.498 | 0.065 | 0.025 | −0.215 |
| Vitamin C (mg/day): 28.87, 0.6 to 12.24 | 0.018 | −0.227 | 0.489 | 0.067 | 0.959 | 0.004 | 0.491 | −0.066 | 0.051 | −0.187 |
| Vitamin B12 (µg/day): 1.21, 0 to 12.24 | 0.345 | 0.091 | 0.478 | 0.068 | 0.033 | −0.205 | 0.021 | 0.221 | 0.536 | −0.060 |
| Vitamin B1 (mg/day): 0.93, 0.149 to 1.96 | 0.006 | −0.260 | 0.056 | −0.184 | 0.1844 | −0.128 | 0.1647 | 0.134 | 0.002 | −0.293 |
| Vitamin B6 (mg/day): 0.98, 0.33 to 3.00 | 0.091 | −0.163 | 0.195 | 0.125 | 0.301 | −0.100 | 0.787 | 0.026 | 0.031 | −0.206 |
| Vitamin K (µg/day): 16.95, 0 to 489.5 | 0.0001 | −0.404 | 0.134 | −0.145 | 0.001 | −0.303 | 0.2214 | 0.118 | 0.006 | −0.261 |
| Vitamin E (mg/day): 1.22, 0.118 to 8.07 | 0.002 | −0.293 | 0.812 | 0.023 | 0.014 | −0.234 | 0.1861 | 0.128 | 0.0001 | −0.339 |
| Folic Acid (µg/day): 7.2, 0 to 386.6 | 0.037 | −0.200 | 0.359 | 0.088 | 0.574 | −0.054 | 0.152 | −0.138 | 0.066 | −0.177 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin-Hadmaș, R.M.; Martin, Ș.A.; Romonți, A.; Mărginean, C.O. The Effect of Dietary Intake and Nutritional Status on Anthropometric Development and Systemic Inflammation: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 5635. https://doi.org/10.3390/ijerph18115635
Martin-Hadmaș RM, Martin ȘA, Romonți A, Mărginean CO. The Effect of Dietary Intake and Nutritional Status on Anthropometric Development and Systemic Inflammation: An Observational Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5635. https://doi.org/10.3390/ijerph18115635
Chicago/Turabian StyleMartin-Hadmaș, Roxana Maria, Ștefan Adrian Martin, Adela Romonți, and Cristina Oana Mărginean. 2021. "The Effect of Dietary Intake and Nutritional Status on Anthropometric Development and Systemic Inflammation: An Observational Study" International Journal of Environmental Research and Public Health 18, no. 11: 5635. https://doi.org/10.3390/ijerph18115635
APA StyleMartin-Hadmaș, R. M., Martin, Ș. A., Romonți, A., & Mărginean, C. O. (2021). The Effect of Dietary Intake and Nutritional Status on Anthropometric Development and Systemic Inflammation: An Observational Study. International Journal of Environmental Research and Public Health, 18(11), 5635. https://doi.org/10.3390/ijerph18115635