
Moderate-To-Vigorous Intensity Physical Activity and Sedentary Behaviour across Childhood and Adolescence, and Their Combined Relationship with Obesity Risk: A Multi-Trajectory Analysis

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Settings
2.3. Physical Activity Assessment
2.4. Anthropometric Proxies for Body Fatness and Body Fatness Measures
2.5. Study Size
2.6. Statistical Methods
3. Results
3.1. Characteristics of Study Participants
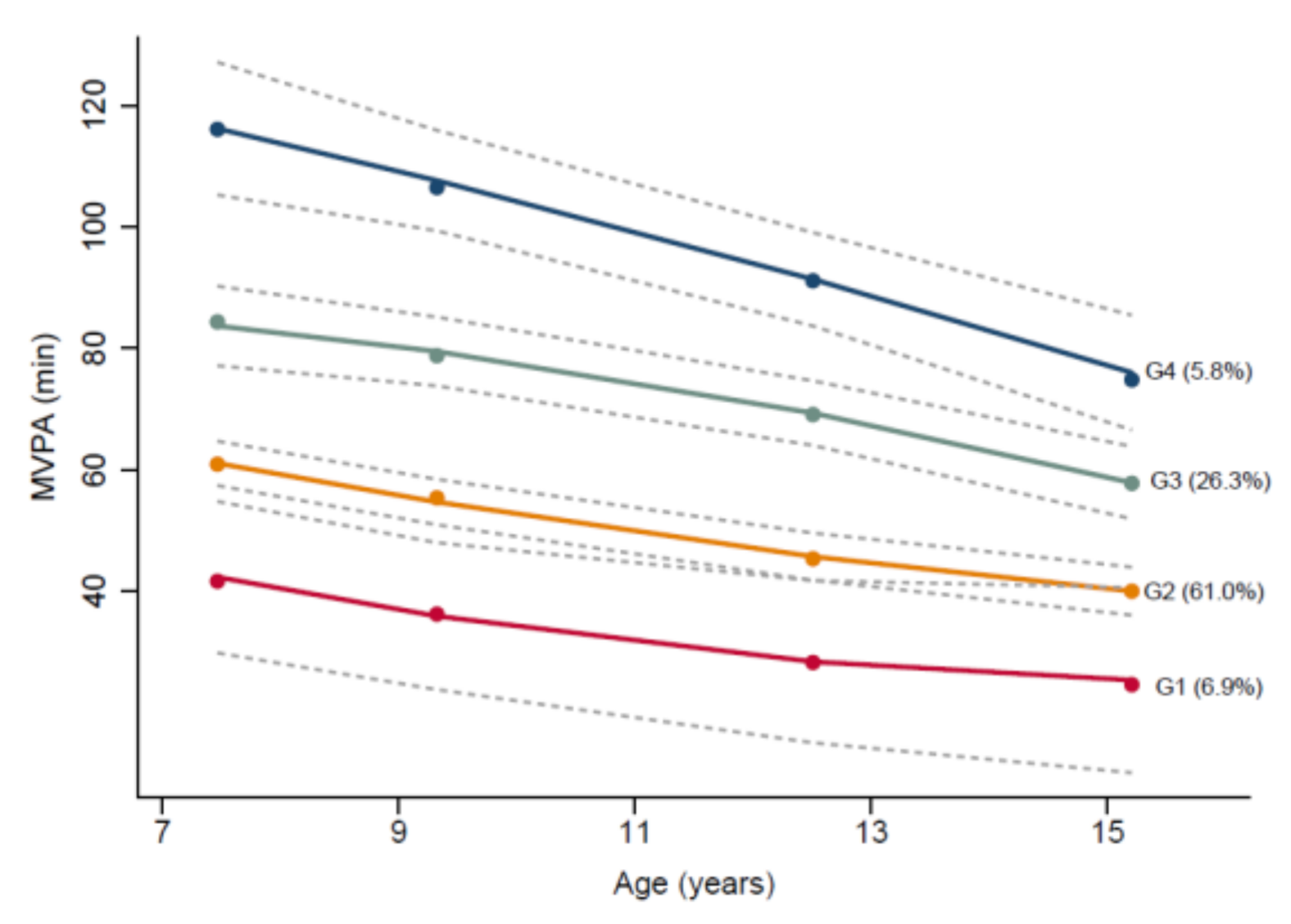
3.2. Group-Based Trajectories of Time Spent in MVPA and Sedentary Behaviour Considered Separately
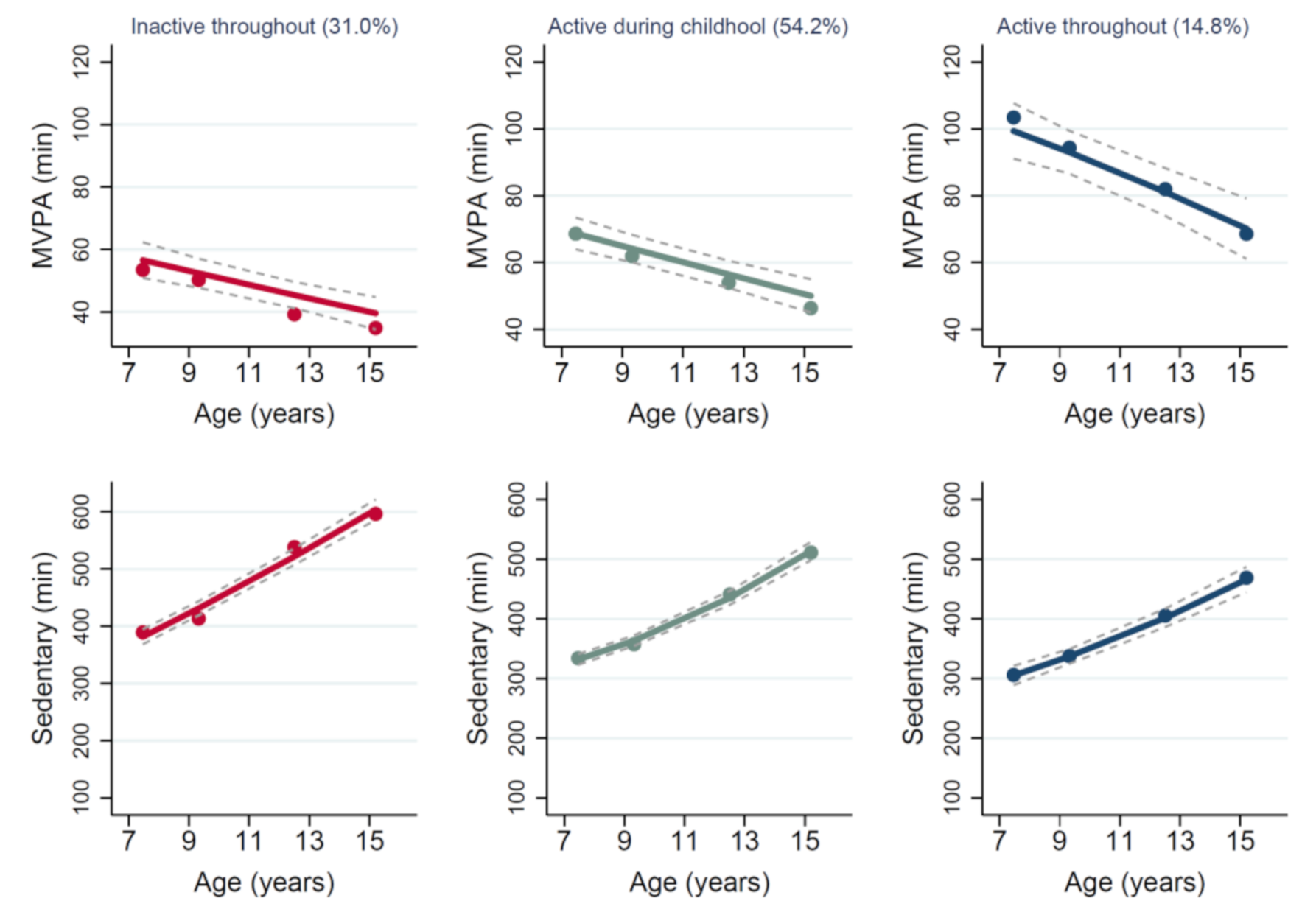
3.3. Multiple Trajectory of Time Spent in MVPA and Sedentary Behaviour Simultaneously
3.4. Association of Sex with Individual and Multiple Group Trajectories
3.5. Associations between Individual Group Trajectories and Multiple Group Trajectories and Adiposity at Age 15 Years
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Obesity and Overweight. World Health Organization, 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 November 2020).
- Kwon, S.; Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Levy, S.M. Active lifestyle in childhood and adolescence prevents obesity development in young adulthood. Obesity 2015, 23, 2462–2469. [Google Scholar] [CrossRef] [PubMed]
- Pirgon, Ö.; Aslan, N. The Role of Urbanization in Childhood Obesity. J. Clin. Res. Pediatr. Endocrinol. 2015, 7, 163–167. [Google Scholar] [CrossRef]
- Freedson, P.; Pober, D.; Janz, K.F. Calibration of Accelerometer Output for Children. Med. Sci. Sports Exerc. 2005, 37, S523–S530. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, B.; Williams, J.; Rakovac, I.; Wickramasinghe, K.; Hennis, A.; Shin, H.-R.; Farmer, M.; Weber, M.; Berdzuli, N.; Borges, C.; et al. Life course approach to prevention and control of non-communicable diseases. BMJ 2019, 364, l257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagin, D.S. Analyzing developmental trajectories: A semiparametric, group-based approach. Psychol. Methods 1999, 4, 139–157. [Google Scholar] [CrossRef]
- Pate, R.R.; Schenkelberg, M.A.; Dowda, M.; McIver, K.L. Group-based physical activity trajectories in children transitioning from elementary to high school. BMC Public Heal. 2019, 19, 323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Gilmore, J.M.E.; Torner, J.C.; Levy, S.M. Objectively measured physical activity trajectories predict adolescent bone strength: Iowa Bone Development Study. Br. J. Sports Med. 2014, 48, 1032–1036. [Google Scholar] [CrossRef]
- Kwon, S.; Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Levy, S.M. Developmental Trajectories of Physical Activity, Sports, and Television Viewing During Childhood to Young Adulthood. JAMA Pediatr. 2015, 169, 666–672. [Google Scholar] [CrossRef]
- Howie, E.K.; McVeigh, J.A.; Smith, A.J.; Straker, L. Organized Sport Trajectories from Childhood to Adolescence and Health Associations. Med. Sci. Sports Exerc. 2016, 48, 1331–1339. [Google Scholar] [CrossRef]
- Farooq, M.A.; Parkinson, K.N.; Adamson, A.J.; Pearce, M.S.; Reilly, J.K.; Hughes, A.R.; Janssen, X.; Basterfield, L.; Reilly, J.J. Timing of the decline in physical activity in childhood and adolescence: Gateshead Millennium Cohort Study. Br. J. Sports Med. 2018, 52, 1002–1006. [Google Scholar] [CrossRef] [Green Version]
- Lounassalo, I.; Salin, K.; Kankaanpää, A.; Hirvensalo, M.; Palomäki, S.; Tolvanen, A.; Yang, X.; Tammelin, T.H. Distinct trajectories of physical activity and related factors during the life course in the general population: A systematic review. BMC Public Heal. 2019, 19, 271. [Google Scholar] [CrossRef] [Green Version]
- Nagin, D.S.; Odgers, C.L. Group-Based Trajectory Modeling in Clinical Research. Annu. Rev. Clin. Psychol. 2010, 6, 109–138. [Google Scholar] [CrossRef] [Green Version]
- Nagin, D.S.; Jones, B.L.; Passos, V.L.; E Tremblay, R. Group-based multi-trajectory modeling. Stat. Methods Med Res. 2016, 27, 2015–2023. [Google Scholar] [CrossRef]
- Kwon, S.; Janz, K.F.; Burns, T.L.; Levy, S.M. Effects of Adiposity on Physical Activity in Childhood. Med. Sci. Sports Exerc. 2011, 43, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, C.; Reilly, J.J.; Huang, W. Longitudinal changes in objectively measured sedentary behaviour and their relationship with adiposity in children and adolescents: Systematic review and evidence appraisal. Obes. Rev. 2014, 15, 791–803. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Nagin, D.S. Group-Based Trajectory Modeling: An Overview. Annals of Nutrition and Metabolism. Ann. Nutr. Metab. 2014, 65, 205–210. [Google Scholar] [CrossRef]
- Basterfield, L.; Adamson, A.J.; Frary, J.K.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.J.; for the Gateshead Millennium Study Core Team. Longitudinal Study of Physical Activity and Sedentary Behavior in Children. Pediatrics 2010, 127, e24–e30. [Google Scholar] [CrossRef]
- Basterfield, L.; Pearce, M.S.; Adamson, A.J.; Frary, J.K.; Parkinson, K.N.; Wright, C.M.; Reilly, J.J. Physical Activity, Sedentary Behavior, and Adiposity in English Children. Am. J. Prev. Med. 2012, 42, 445–451. [Google Scholar] [CrossRef]
- King, A.C.; Parkinson, K.N.; Adamson, A.J.; Murray, L.; Besson, H.; Reilly, J.J.; Basterfield, L. Correlates of objectively measured physical activity and sedentary behaviour in English children. Eur. J. Public Heal. 2010, 21, 424–431. [Google Scholar] [CrossRef] [Green Version]
- Pearce, M.S.; Basterfield, L.; Mann, K.; Parkinson, K.N.; Adamson, A.J.; John, J. Reilly on behalf of the Gateshead Millennium Study Core Team Early Predictors of Objectively Measured Physical Activity and Sedentary Behaviour in 8–10 Year Old Children: The Gateshead Millennium Study. PLoS ONE 2012, 7, e37975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basterfield, L.; Adamson, A.J.; Pearce, M.S.; Reilly, J.J. Stability of Habitual Physical Activity and Sedentary Behavior Monitoring by Accelerometry in 6- to 8-Year-Olds. J. Phys. Act. Heal. 2011, 8, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Freeman, J.V.; A Preece, M. Body mass index reference curves for the UK, 1990. Arch. Dis. Child. 1995, 73, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Farooq, A.; Martin, A.; Janssen, X.; Wilson, M.; Gibson, A.; Hughes, A.; Reilly, J.J. Longitudinal changes in moderate-to-vigorous-intensity physical activity in children and adolescents: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e12953. [Google Scholar] [CrossRef] [Green Version]
- Nagin, D. Group-Based Modeling of Development; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Kwon, S.; Lee, J.; Carnethon, M.R. Developmental trajectories of physical activity and television viewing during adolescence among girls: National Growth and Health Cohort Study. BMC Public Heal. 2015, 15, 667. [Google Scholar] [CrossRef] [Green Version]
- Audrain-McGovern, J.; Rodriguez, D.; Tercyak, K.P.; Cuevas, J.; Rodgers, K.; Patterson, F. Identifying and characterizing adolescent smoking trajectories. Cancer Epidemiol. Biomark. Prev. 2004, 13, 2023–2034. [Google Scholar]
- Findlay, L.C.; Garner, R.E.; Kohen, D.E. Children’s Organized Physical Activity Patterns from Childhood into Adolescence. J. Phys. Act. Heal. 2009, 6, 708–715. [Google Scholar] [CrossRef]
- Hanson, S.K.; Munthali, R.J.; Micklesfield, L.K.; Lobelo, F.; Cunningham, S.A.; Hartman, T.J.; Norris, S.A.; Stein, A.D. Longitudinal patterns of physical activity, sedentary behavior and sleep in urban South African adolescents, Birth-To-Twenty Plus cohort. BMC Pediatr. 2019, 19, 241. [Google Scholar] [CrossRef] [Green Version]
- Gallant, F.; Thibault, V.; Hebert, J.; Gunnell, K.E.; Bélanger, M. One size does not fit all: Identifying clusters of physical activity, screen time, and sleep behaviour co-development from childhood to adolescence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–14. [Google Scholar] [CrossRef]
- Campbell, S.D.I.; Brosnan, B.J.; Chu, A.K.Y.; Skeaff, C.M.; Rehrer, N.J.; Perry, T.L.; Peddie, M.C. Sedentary Behavior and Body Weight and Composition in Adults: A Systematic Review and Meta-analysis of Prospective Studies. Sports Med. 2018, 48, 585–595. [Google Scholar] [CrossRef]
- Guo, C.; Zhou, Q.; Zhang, D.; Qin, P.; Li, Q.; Tian, G.; Liu, D.; Chen, X.; Liu, L.; Liu, F.; et al. Association of total sedentary behaviour and television viewing with risk of overweight/obesity, type 2 diabetes and hypertension: A dose–response meta-analysis. Diabetes Obes. Metab. 2020, 22, 79–90. [Google Scholar] [CrossRef]
- Blackburn, N.E.; Wilson, J.; McMullan, I.I.; Caserotti, P.; Giné-Garriga, M.; Wirth, K.; Coll-Planas, L.; Alias, S.B.; Roqué, M.; Deidda, M.; et al. The effectiveness and complexity of interventions targeting sedentary behaviour across the lifespan: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Bäck, M.; Rees, J.M.B.; Mason, A.M.; Burgess, S. Body mass index and body composition in relation to 14 cardiovascular conditions in UK Biobank: A Mendelian randomization study. Eur. Hear. J. 2020, 41, 221–226. [Google Scholar] [CrossRef]
- Oh, M.; Zhang, D.; Whitaker, K.M.; Letuchy, E.M.; Janz, K.F.; Levy, S.M. Moderate-to-vigorous intensity physical activity trajectories during adolescence and young adulthood predict adiposity in young adulthood: The Iowa Bone Development Study. J. Behav. Med. 2021, 44, 231–240. [Google Scholar] [CrossRef]
- Prince, S.A.; Reed, J.; McFetridge, C.; Tremblay, M.S.; Reid, R.D. Correlates of sedentary behaviour in adults: A systematic review. Obes. Rev. 2017, 18, 915–935. [Google Scholar] [CrossRef]
- Sport England. Active Lives Children and Young People Survey Coronavirus (Covid-19) Report UK: Sport England. 2020. Available online: https://www.sportengland.org/know-your-audience/data/active-lives (accessed on 1 November 2020).
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–11. [Google Scholar] [CrossRef]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID -19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2021, 16. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|
| Age 7 n = 279 | Age 9 n = 277 | Age 12 n = 246 | Age 15 n = 173 | Age 7 n = 283 | Age 9 n = 287 | Age 12 n = 260 | Age 15 n = 155 | |
| Anthropometry | ||||||||
| Body mass index z-score * | 0.4 ± 0.1 | 0.6 ± 0.1 a | 0.7 ± 0.1 a,b,d | 0.6 ± 0.1 ‡ | 0.4 ± 0.1 | 0.6 ± 0.1 a | 0.7 ± 0.1 a,b | 0.8 ± 0.1 a,b |
| Fat mass index | 4.1 ± 0.1 | 4.7 ± 0.1 a | 5.2 ± 0.2 a,b,‡ | 5.1 ± 0.3 a,‡ | 4.0 ± 0.1 | 5.0 ± 0.1 a | 5.9 ± 0.2 a,b | 8.4 ± 0.2 a,b,c |
| Obesity ** (%) | 9.7% | 13.4% a | 13.8% | 13.3% | 8.8% | 8.4% | 12.7% a,b | 14.8% a,b |
| Accelerometer | ||||||||
| MVPA (min/day) | 75.2 ± 1.4 ‡,b,c,d | 70.0 ± 1.3 ‡,c,d | 60.1 ± 1.5 ‡,d | 51.0 ± 1.5 ‡ | 63.1 ± 1.4 b,c,d | 56.3 ± 1.3 c,d | 46.7 ± 1.4 d | 40.6 ± 1.4 |
| Sedentary behaviour (min/day) | 338.3 ± 4.3 ‡ | 364.5 ± 3.9 a,‡ | 447.5 ± 6.0 a,b,‡ | 518.7 ± 6.8 a,b,c | 352.5 ± 4.3 | 378.3 ± 3.8 a | 480.5 ± 5.7 a,b | 536.1 ± 6.4 a,b,c |
| Univariate Group-Based Trajectories for Moderate–Vigorous-Intensity Physical Activity (MVPA) | |||||
|---|---|---|---|---|---|
| Group 1 The Lowest MVPA throughout (n = 15) | Group 2 High MVPA but Declining (n = 94) | Group 3 Low MVPA and Declining (n = 221) | Group 4 High MVPA (n = 26) | p-Value | |
| Boys | 3 (20.0) | 56 (59.6) | 90 (40.7) | 24 (92.3) | <0.001 |
| Girls | 12 (80.0) | 38 (40.4) | 131 (59.3) | 2 (7.7) | |
| Fat mass (kg) | 22.5 ± 9.0 a | 17.4 ± 12.0 | 18.7 ± 12.0 a | 12.2 ± 6.3 | 0.021 |
| Fat mass index (FMI) | 8.5 ± 3.5 a | 6.2 ± 4.0 | 6.8 ± 4.3 a | 4.3 ± 2.3 | 0.006 |
| BMI Z-score for age | 0.9 ± 1.3 | 0.6 ± 1.1 | 0.6 ± 1.3 | 0.3 ± 1.2 | 0.337 |
| Obesity (BMI SD-score ≥ 2) | 26.7% | 13.8% | 14.0% | 7.7% | 0.415 |
| Univariate Group-Based Trajectories for Sedentary Behaviour | |||||
| Group 1 Low Sedentary Increasing (n = 151) | Group 2 High Sedentary and Increasing (n = 205) | p-Value | |||
| Boys | 83 (55.0) | 90 (43.9) | 0.038 | ||
| Girls | 68 (45.0) | 115 (56.1) | |||
| Fat mass (kg) | 17.4 ± 11.7 | 18.6 ± 11.7 | 0.515 | ||
| Fat mass index (FMI) | 6.3 ± 4.2 | 6.6 ± 4.0 | 0.477 | ||
| BMI Z-score for age | 0.7 ± 1.3 | 0.6 ± 1.2 | 0.336 | ||
| Obesity (BMI SD-score ≥ 2) | 15.9% | 12.7% | 0.389 | ||
| Multi-Trajectory Groups (MVPA and Sedentary Behaviour Combined) | |||||
| Group 1 Inactive throughout (n = 110) | Group 2 Active during Childhood (n = 191) | Group 3 Active throughout (n = 55) | p-Value | ||
| Boys | 40 (36.4) | 91 (47.6) | 42 (76.4) | ||
| Girls | 70 (63.6) | 100 (52.4) | 13 (23.6) | ||
| Fat mass (kg) | 19.5 ± 11.5 | 18.2 ± 12.2 | 14.9 ± 9.7 | 0.060 | |
| Fat mass index (FMI) | 7.0 ± 3.9 b | 6.6 ± 4.3 | 5.3 ± 3.4 | 0.038 | |
| BMI Z-score for age | 0.6 ± 1.3 | 0.7 ± 1.2 | 0.6 ± 1.1 | 0.770 | |
| Obesity (BMI SD-score > 2) | 12.7% | 15.7% | 10.9% | 0.594 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farooq, A.; Basterfield, L.; Adamson, A.J.; Pearce, M.S.; Hughes, A.R.; Janssen, X.; Wilson, M.G.; Reilly, J.J. Moderate-To-Vigorous Intensity Physical Activity and Sedentary Behaviour across Childhood and Adolescence, and Their Combined Relationship with Obesity Risk: A Multi-Trajectory Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7421. https://doi.org/10.3390/ijerph18147421
Farooq A, Basterfield L, Adamson AJ, Pearce MS, Hughes AR, Janssen X, Wilson MG, Reilly JJ. Moderate-To-Vigorous Intensity Physical Activity and Sedentary Behaviour across Childhood and Adolescence, and Their Combined Relationship with Obesity Risk: A Multi-Trajectory Analysis. International Journal of Environmental Research and Public Health. 2021; 18(14):7421. https://doi.org/10.3390/ijerph18147421
Chicago/Turabian StyleFarooq, Abdulaziz, Laura Basterfield, Ashley J. Adamson, Mark S. Pearce, Adrienne R. Hughes, Xanne Janssen, Mathew G. Wilson, and John J. Reilly. 2021. "Moderate-To-Vigorous Intensity Physical Activity and Sedentary Behaviour across Childhood and Adolescence, and Their Combined Relationship with Obesity Risk: A Multi-Trajectory Analysis" International Journal of Environmental Research and Public Health 18, no. 14: 7421. https://doi.org/10.3390/ijerph18147421
APA StyleFarooq, A., Basterfield, L., Adamson, A. J., Pearce, M. S., Hughes, A. R., Janssen, X., Wilson, M. G., & Reilly, J. J. (2021). Moderate-To-Vigorous Intensity Physical Activity and Sedentary Behaviour across Childhood and Adolescence, and Their Combined Relationship with Obesity Risk: A Multi-Trajectory Analysis. International Journal of Environmental Research and Public Health, 18(14), 7421. https://doi.org/10.3390/ijerph18147421