
The Effects of Dietary Education Interventions on Individuals with Type 2 Diabetes: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
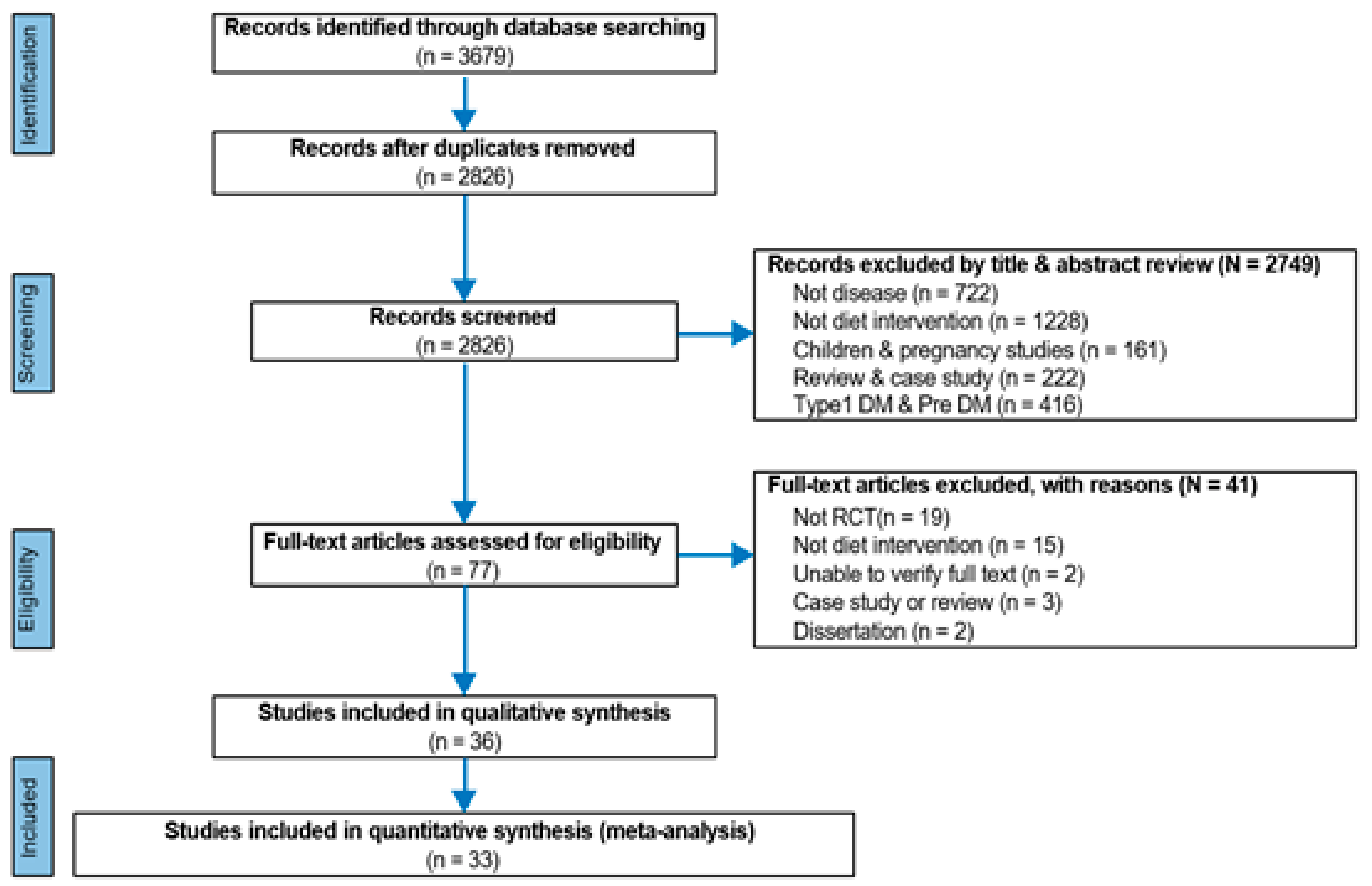
2.2. Study Selection
2.3. Inclusion and Exclusion Criteria
2.4. Data Synthesis and Analysis
3. Results
3.1. Characteristics of Studies Selected for the Systematic Literature Review
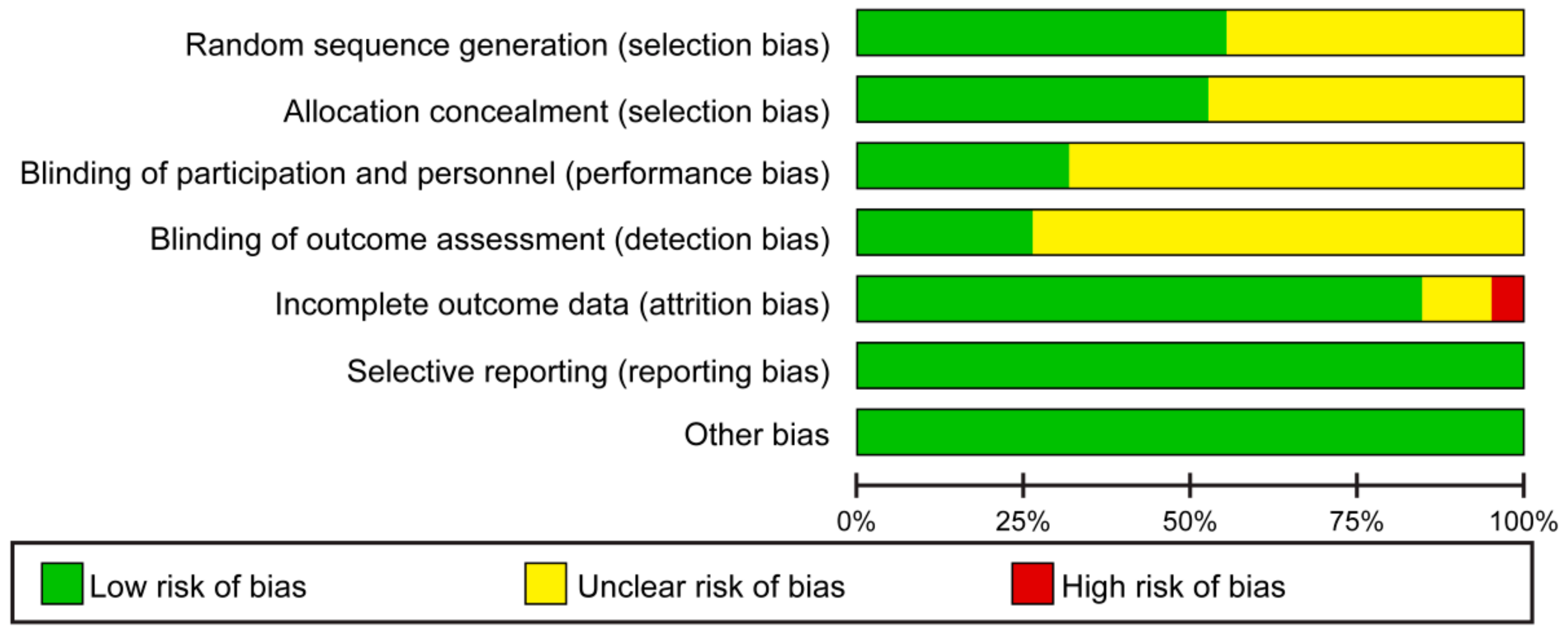
3.2. Literature Quality Assessment
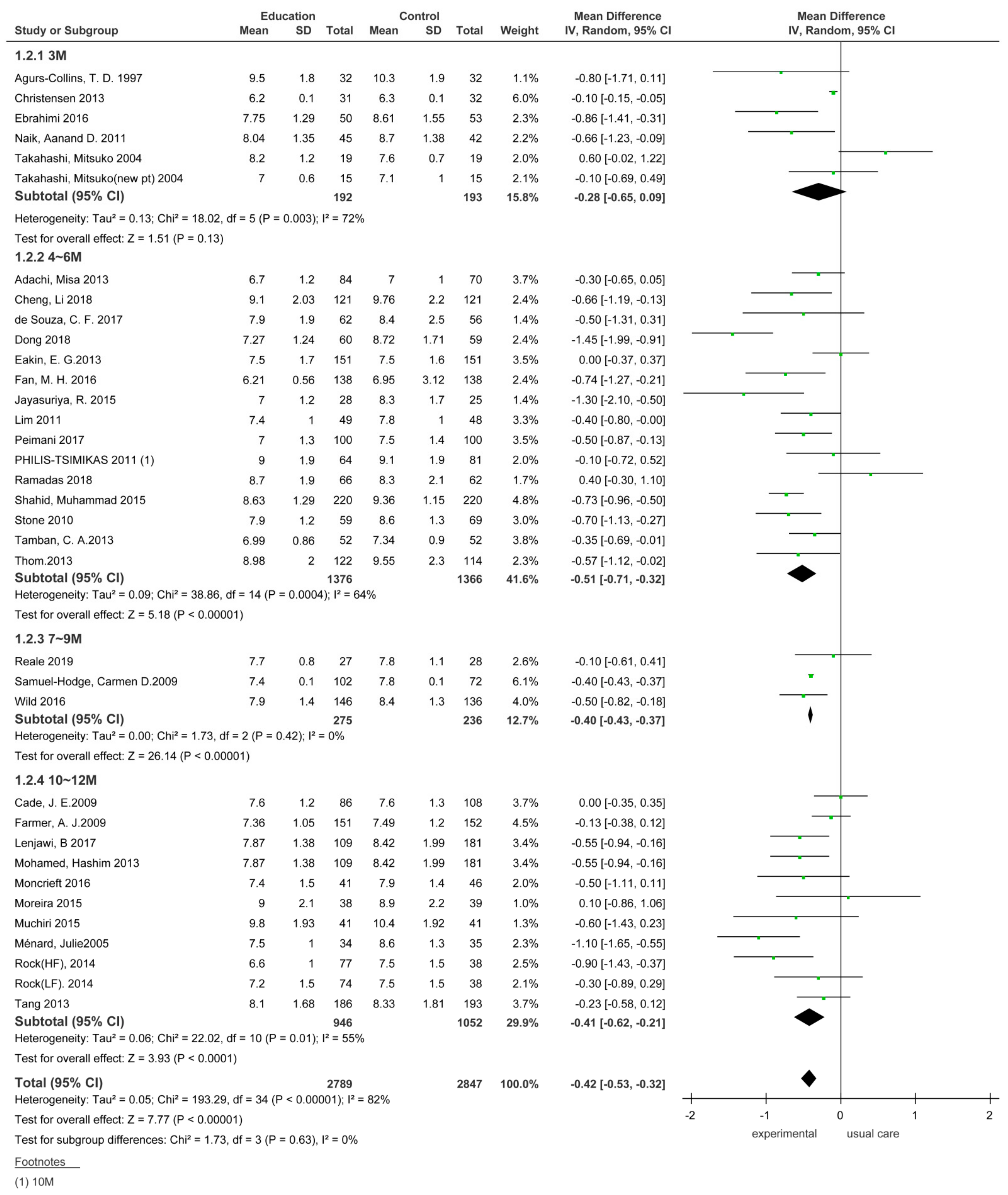
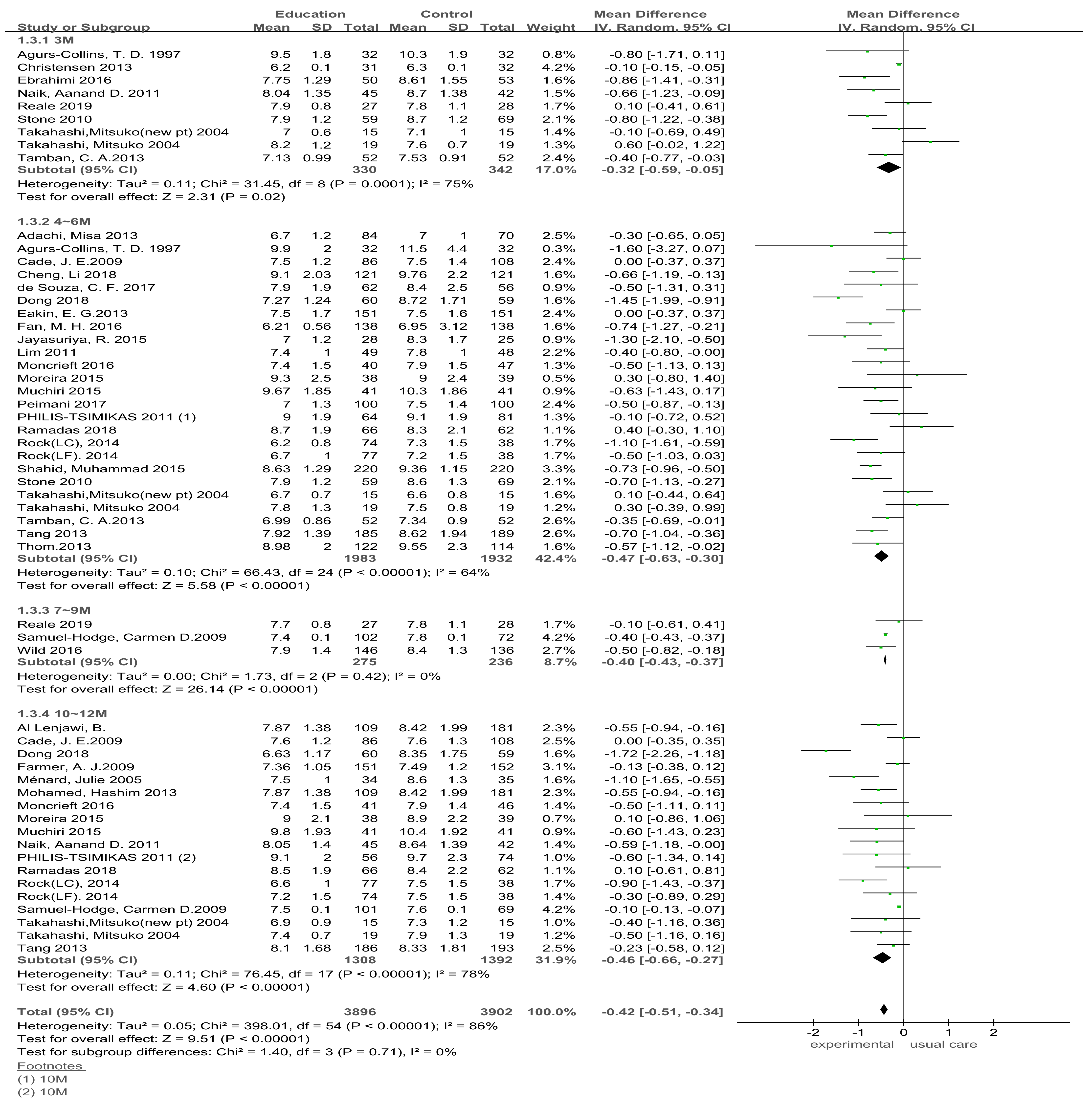
3.3. Effects of Dietary Education Interventions on HbA1cin Type 2 Diabetes Patients
3.3.1. Comparison of the HbA1C Effect Size According to the Duration of Dietary Education Interventions in Type 2 Diabetes Patients
HbA1C Effect Size at the Endpoints of Dietary Education Interventions
HbA1c Effect Size in Dietary Education Interventions Assessed at Different Follow-up Time-Points
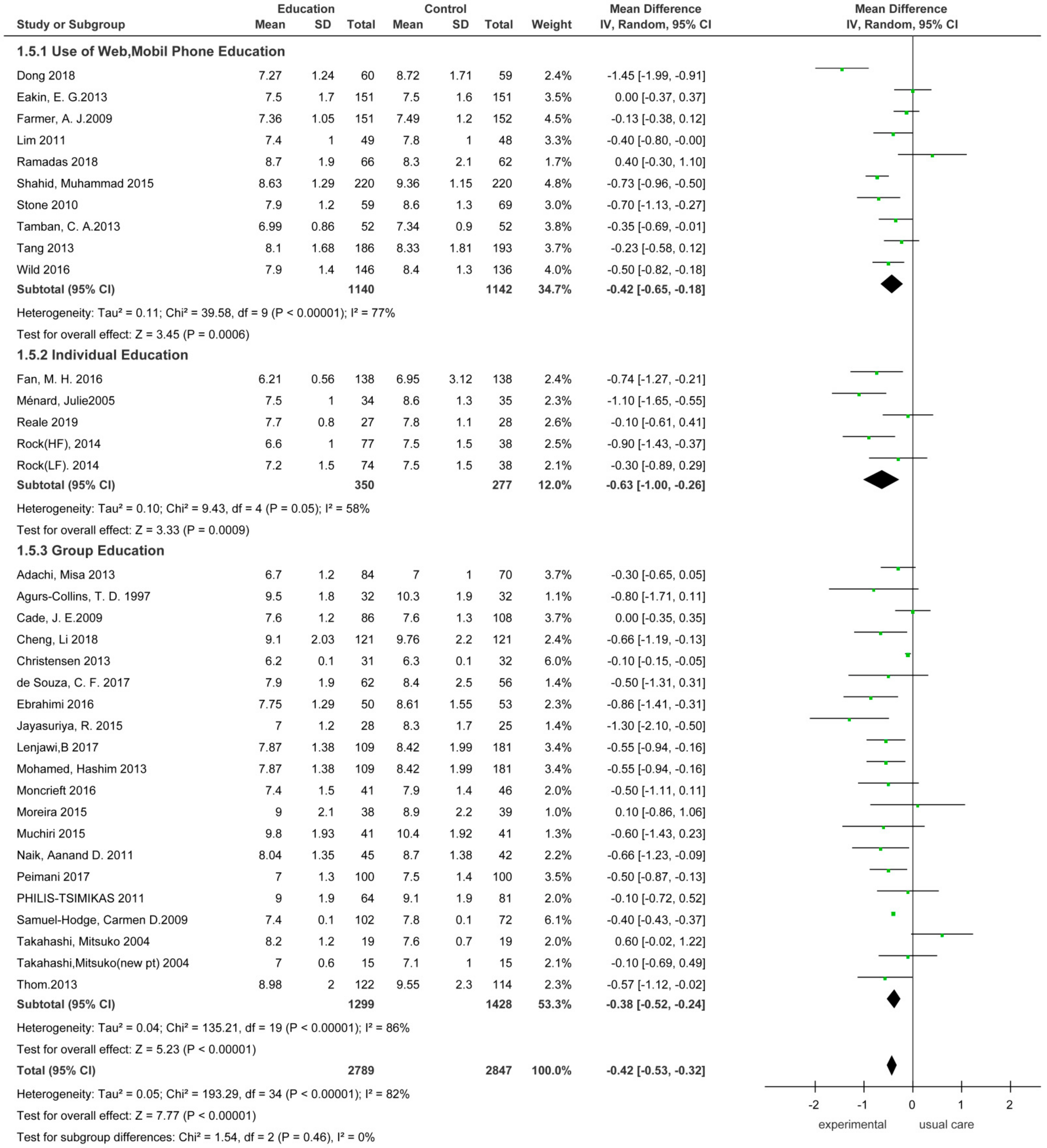
3.3.2. Comparison of the Effect Size of HbA1C According to Dietary Education Intervention Methods
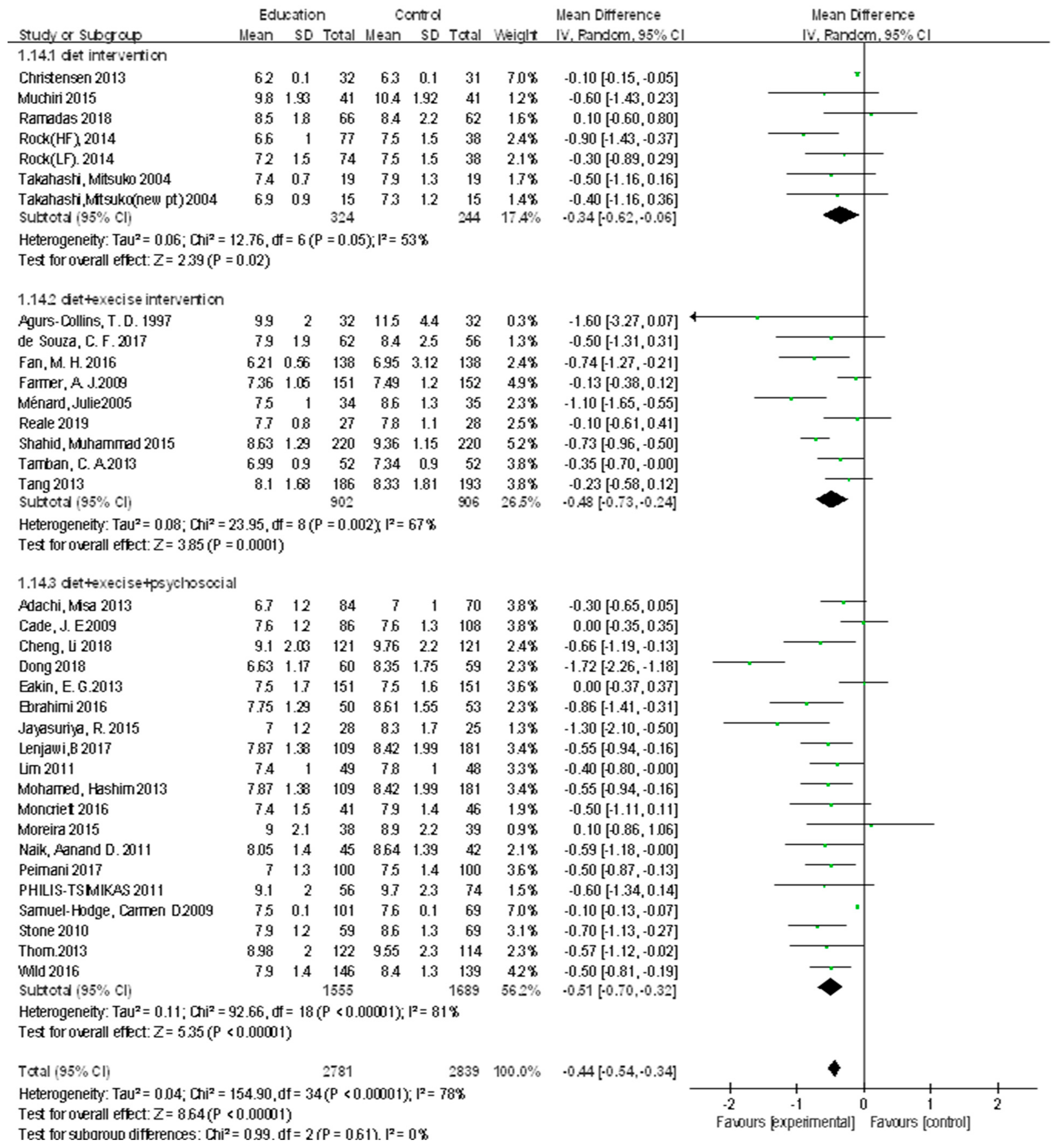
3.3.3. Comparison of the Effect Size of HbA1C According to Dietary Education Contents
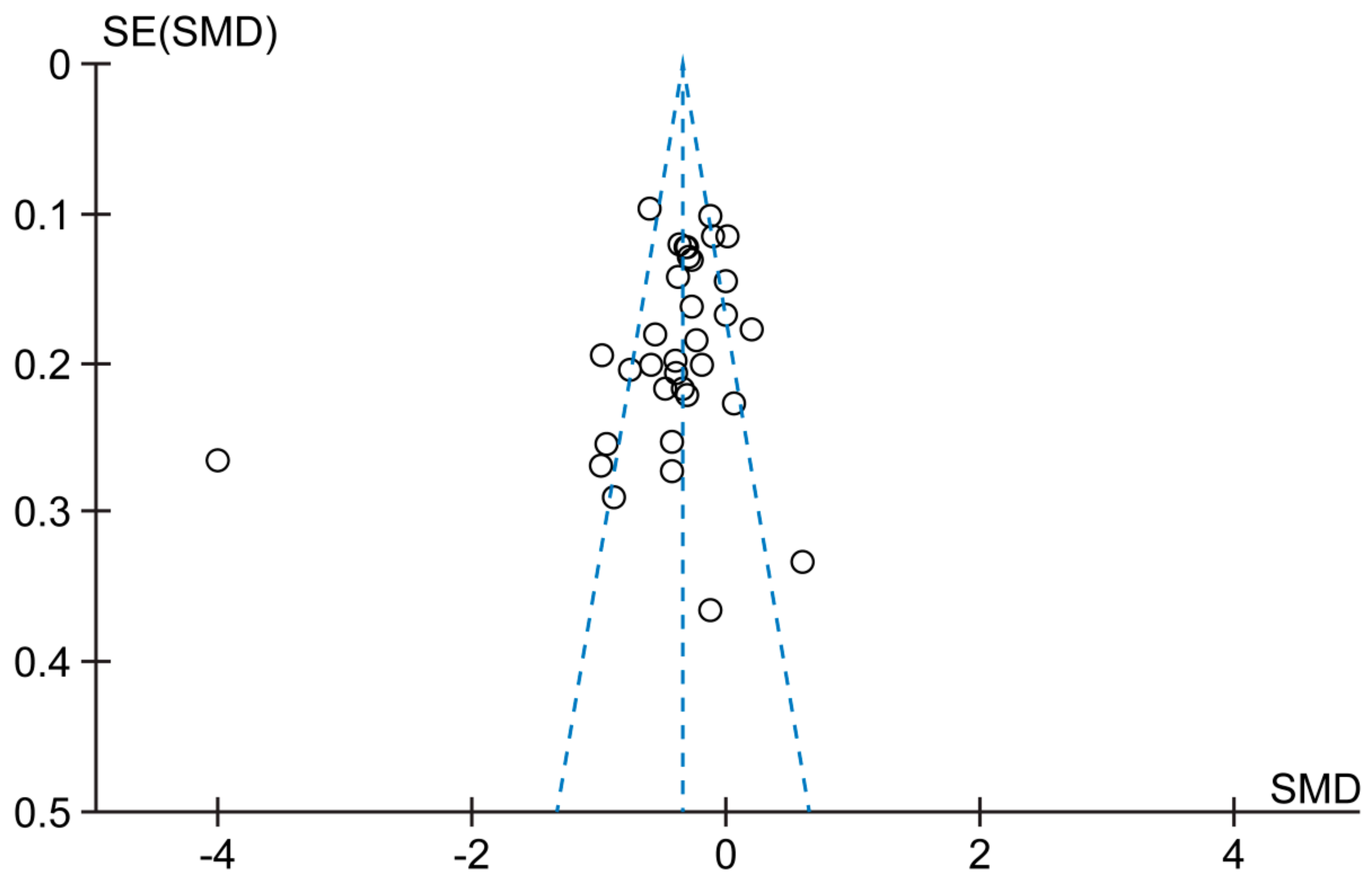
3.4. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atlas, D. International Diabetes Federation, IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- Kim, M.K.; Ko, S.H.; Kim, B.Y.; Kang, E.S.; Noh, J.; Kim, S.K.; Park, S.O.; Hur, K.Y.; Chon, S.; Moon, M.K.; et al. 2019 Clinical Practice Guidelines for Type 2 Diabetes Mellitus in Korea. Diabetes Metab. J. 2019, 43, 398–406. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.; et al. Type 2 diabetes mellitus. Nat. Rev. Dis. Prim. 2015, 1, 15019. [Google Scholar] [CrossRef]
- Silva, F.M.; Kramer, C.K.; De Almeida, J.C.; Steemburgo, T.; Gross, J.L.; Azevedo, M.J. Fiber intake and glycemic control in patients with type 2 diabetes mellitus: A systematic review with meta-analysis of randomized controlled trials. Nutr. Rev. 2013, 71, 790–801. [Google Scholar] [CrossRef]
- Yang, S.H.; Chung, H.-K.; Lee, S.-M. Effects of Activity-Based Personalized Nutrition Education on Dietary Behaviors and Blood Parameters in Middle-Aged and Older Type 2 Diabetes Korean Outpatients. Clin. Nutr. Res. 2016, 5, 237–248. [Google Scholar] [CrossRef] [Green Version]
- Nathan, D.M.; Barrett-Connor, E.; Crandall, J.; Edelstein, S.L.; Goldberg, R.; Horton, E.S.; Knowler, W.; Mather, K.J.; Orchard, T.; Pi-Sunyer, X.; et al. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: The Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015, 3, 866–875. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Qin, S.; Huang, L.; Tang, Y.; Ren, H.; Hu, H. Efficacy and safety of Rhizoma curcumea longae with respect to improving the glucose metabolism of patients at risk for cardiovascular disease: A meta-analysis of randomised controlled trials. J. Hum. Nutr. Diet. 2019, 32, 591–606. [Google Scholar] [CrossRef]
- Hou, C.; Carter, B.; Hewitt, J.; Francisa, T.; Mayor, S. Do Mobile Phone Applications Improve Glycemic Control (HbA1c) in the Self-management of Diabetes? A Systematic Review, Meta-analysis, and GRADE of 14 Randomized Trials. Diabetes Care 2016, 39, 2089–2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.E.; Kim, E.; Kim, G. The effects of diabetes management programs using mobile app: A systematic review and a me-ta-analysis. J. Korea Contents Assoc. 2015, 15, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Snorgaard, O.; Poulsen, G.M.; Andersen, H.K.; Astrup, A. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2017, 5, e000354. [Google Scholar] [CrossRef]
- Razaz, J.M.; Rahmani, J.; Varkaneh, H.K.; Thompson, J.; Clark, C.; Abdulazeem, H. The health effects of medical nutrition therapy by dietitians in patients with diabetes: A systematic review and meta-analysis. Prim. Care Diabetes 2019, 13, 399–408. [Google Scholar] [CrossRef]
- Wei, N.; Zheng, H.; Nathan, D.M. Empirically Establishing Blood Glucose Targets to Achieve HbA 1c Goals. Diabetes Care 2014, 37, 1048–1051. [Google Scholar] [CrossRef] [Green Version]
- Clarke, P.M.; Gray, A.M.; Briggs, A.; Farmer, A.J.; Fenn, P.; Stevens, R.J.; Matthews, D.R.; Stratton, I.; Holman, R.R.; on behalf of the UK Prospective Diabetes Study (UKPDS) Group. A model to estimate the lifetime health outcomes of patients with Type 2 diabetes: The United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004, 47, 1747–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adachi, M.; Yamaoka, K.; Watanabe, M.; Nishikawa, M.; Kobayashi, I.; Hida, E.; Tango, T. Effects of lifestyle education program for type 2 diabetes patients in clinics: A cluster randomized controlled trial. BMC Public Health 2013, 13, 467. [Google Scholar] [CrossRef] [Green Version]
- Agurs-Collins, T.D.; Kumanyika, S.K.; Have, T.R.T.; Adams-Campbell, L.L. A Randomized Controlled Trial of Weight Reduction and Exercise for Diabetes Management in Older African-American Subjects. Diabetes Care 1997, 20, 1503–1511. [Google Scholar] [CrossRef]
- Cade, J.E.; Kirk, S.; Nelson, P.; Hollins, L.; Deakin, T.; Greenwood, D.C.; Harvey, E.L. Can peer educators influence healthy eating in people with diabetes? Results of a randomized controlled trial. Diabet. Med. 2009, 26, 1048–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, L.; Sit, J.W.; Choi, K.-C.; Chair, S.-Y.; Li, X.; Wu, Y.; Long, J.; Tao, M. Effectiveness of a patient-centred, empowerment-based intervention programme among patients with poorly controlled type 2 diabetes: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 79, 43–51. [Google Scholar] [CrossRef]
- Christensen, A.S.; Viggers, L.; Hasselström, K.; Gregersen, S. Effect of fruit restriction on glycemic control in patients with type 2 diabetes—A randomized trial. Nutr. J. 2013, 12, 29. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Wang, P.; Dai, Z.; Liu, K.; Jin, Y.; Li, A.; Wang, S.; Zheng, J. Increased self-care activities and glycemic control rate in relation to health education via Wechat among diabetes patients: A randomized clinical trial. Medicine 2018, 97, e13632. [Google Scholar] [CrossRef] [PubMed]
- Eakin, E.G.; Reeves, M.M.; Winkler, E.; Healy, G.; Dunstan, D.; Owen, N.; Marshal, A.M.; Wilkie, K.C. Six-Month Outcomes from Living Well with Diabetes: A Randomized Trial of a Telephone-Delivered Weight Loss and Physical Activity Intervention to Improve Glycemic Control. Ann. Behav. Med. 2013, 46, 193–203. [Google Scholar] [CrossRef]
- Ebrahimi, H.; Sadeghi, M.; Amanpour, F.; Vahedi, H. Evaluation of empowerment model on indicators of metabolic control in patients with type 2 diabetes, a randomized clinical trial study. Prim. Care Diabetes 2016, 10, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Amendezo, E.; Timothy, D.W.; Karamuka, V.; Robinson, B.; Kavabushi, P.; Ntirenganya, C.; Uwiragiye, J.; Mukantagwabira, D.; Bisimwa, J.; Marie, H.U.; et al. Effects of a lifestyle education program on glycemic control among patients with diabetes at Kigali University Hospital, Rwanda: A randomized controlled trial. Diabetes Res. Clin. Pr. 2017, 126, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.-H.; Huang, B.-T.; Tang, Y.-C.; Han, X.-H.; Dong, W.-W.; Wang, L.-X. Effect of individualized diabetes education for type 2 diabetes mellitus: A single-center randomized clinical trial. Afr. Health Sci. 2017, 16, 1157–1162. [Google Scholar] [CrossRef] [Green Version]
- Farmer, A.J.; Wade, A.N.; French, D.; Simon, J.; Yudkin, P.; Gray, A.; Craven, A.; Goyder, L.; Holman, R.R.; Mant, D.; et al. Blood glucose self-monitoring in type 2 diabetes: A randomised controlled trial. Health Technol. Assess. 2009, 13, 1–50. [Google Scholar] [CrossRef] [Green Version]
- Jayasuriya, R.; Pinidiyapathirage, M.; Jayawardena, R.; Kasturiratne, A.; De Zoysa, P.; Godamunne, P.; Gamage, S.; Wickremasinghe, A. Translational research for Diabetes Self-Management in Sri Lanka: A randomized controlled trial. Prim. Care Diabetes 2015, 9, 338–345. [Google Scholar] [CrossRef]
- Lim, S.; Kang, S.M.; Shin, H.; Lee, H.J.; Yoon, J.W.; Yu, S.H.; Kim, S.-Y.; Yoo, S.Y.; Jung, H.S.; Park, K.S.; et al. Improved Glycemic Control without Hypoglycemia in Elderly Diabetic Patients Using the Ubiquitous Healthcare Service, a New Medical Information System. Diabetes Care 2011, 34, 308–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Lenjawi, B.; Mohamed, H.; Amuna, P.; Zotor, F.; Ziki, M.D.A. Nurse-led theory-based educational intervention improves glycemic and metabolic parameters in South Asian patients with type II diabetes: A randomized controlled trial. Diabetol. Int. 2016, 8, 95–103. [Google Scholar] [CrossRef]
- Ménard, J.; Payette, H.; Baillargeon, J.-P.; Maheux, P.; Lepage, S.; Tessier, D.; Ardilouze, J.-L. Efficacy of intensive multitherapy for patients with type 2 diabetes mellitus: A randomized controlled trial. Can. Med. Assoc. J. 2005, 173, 1457–1466. [Google Scholar] [CrossRef] [Green Version]
- Mohamed, H.; Al-Lenjawi, B.; Amuna, P.; Zotor, F.; Elmahdi, H. Culturally sensitive patient-centred educational programme for self-management of type 2 diabetes: A randomized controlled trial. Prim. Care Diabetes 2013, 7, 199–206. [Google Scholar] [CrossRef]
- Muchiri, J.W.; Gericke, G.J.; Rheeder, P. Effect of a nutrition education programme on clinical status and dietary behaviours of adults with type 2 diabetes in a resource-limited setting in South Africa: A randomised controlled trial. Public Health Nutr. 2015, 19, 142–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreira, R.C.; Mantovani, M.D.F.; Soriano, J.V. Nursing Case Management and Glycemic Control among Brazilians with Type 2 Diabetes: Pragmatic Clinical Trial. Nurs. Res. 2015, 64, 272–281. [Google Scholar] [CrossRef]
- Moncrieft, A.E.; Llabre, M.M.; McCalla, J.R.; Gutt, M.; Mendez, A.J.; Gellman, M.D.; Goldberg, R.B.; Schneiderman, N. Effects of a Multicomponent Life-Style Intervention on Weight, Glycemic Control, Depressive Symptoms, and Renal Function in Low-Income, Minority Patients with Type 2 Diabetes: Results of the Community Approach to Lifestyle Modification for Diabetes Randomized Controlled Trial. Psychosom. Med. 2016, 78, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.D.; Palmer, N.; Petersen, N.J.; Street, R.L.; Rao, R.; Suarez-Almazor, M.; Haidet, P. Comparative Effectiveness of Goal Setting in Diabetes Mellitus Group Clinics: Randomized clinical trial. Arch. Intern. Med. 2011, 171, 453–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peimani, M.; Monjazebi, F.; Ghodssi-Ghassemabadi, R.; Nasli-Esfahani, E. A peer support intervention in improving glycemic control in patients with type 2 diabetes. Patient Educ. Couns. 2018, 101, 460–466. [Google Scholar] [CrossRef]
- Philis-Tsimikas, A.; Fortmann, A.; Lleva-Ocana, L.; Walker, C.; Gallo, L.C. Peer-Led Diabetes Education Programs in High-Risk Mexican Americans Improve Glycemic Control Compared with Standard Approaches: A Project Dulce promotora randomized trial. Diabetes Care 2011, 34, 1926–1931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramadas, A.; Chan, C.K.Y.; Oldenburg, B.; Hussein, Z.; Quek, K.F. Randomised-controlled trial of a web-based dietary intervention for patients with type 2 diabetes: Changes in health cognitions and glycemic control. BMC Public Health 2018, 18, 1–13. [Google Scholar] [CrossRef]
- Rock, C.L.; Flatt, S.W.; Pakiz, B.; Taylor, K.S.; Leone, A.F.; Brelje, K.; Heath, D.D.; Quintana, E.L.; Sherwood, N.E. Weight Loss, Glycemic Control, and Cardiovascular Disease Risk Factors in Response to Differential Diet Composition in a Weight Loss Program in Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2014, 37, 1573–1580. [Google Scholar] [CrossRef] [Green Version]
- Reale, R.; Tumminia, A.; Romeo, L.; La Spina, N.; Baratta, R.; Padova, G.; Tomaselli, L.; Frittitta, L. Short-term efficacy of high intensity group and individual education in patients with type 2 diabetes: A randomized single-center trial. J. Endocrinol. Investig. 2018, 42, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Samuel-Hodge, C.D.; Keyserling, T.C.; Park, S.; Johnston, L.F.; Gizlice, Z.; Bangdiwala, S.I. A Randomized Trial of a Church-Based Diabetes Self-management Program for African Americans with Type 2 Diabetes. Diabetes Educ. 2009, 35, 439–454. [Google Scholar] [CrossRef]
- Shahid, M.; Mahar, S.A.; Shaikh, S.; Shaikh, Z.U. Mobile phone intervention to improve diabetes care in rural areas of Pakistan: A randomized controlled trial. J. Coll. Physicians Surg. Pak. 2015, 25, 166–171. [Google Scholar]
- De Souza, C.F.; Dalzochio, M.B.; Zucatti, A.T.N.; De Nale, R.; De Almeida, M.T.; Gross, J.L.; Leitao, C. Efficacy of an education course delivered to community health workers in diabetes control: A randomized clinical trial. Endocrine 2017, 57, 280–286. [Google Scholar] [CrossRef]
- Spencer, M.S.; Rosland, A.-M.; Kieffer, E.C.; Sinco, B.R.; Valerio, M.; Palmisano, G.; Anderson, M.; Guzman, J.R.; Heisler, M. Effectiveness of a Community Health Worker Intervention among African American and Latino Adults with Type 2 Diabetes: A Randomized Controlled Trial. Am. J. Public Health 2011, 101, 2253–2260. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.A.; Rao, R.H.; Sevick, M.A.; Cheng, C.; Hough, L.J.; MacPherson, D.S.; Franko, C.M.; Anglin, R.A.; Obrosky, D.S.; Derubertis, F.R. Active Care Management Supported by Home Telemonitoring in Veterans with Type 2 Diabetes: The DiaTel randomized controlled trial. Diabetes Care 2009, 33, 478–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, M.; Araki, A.; Ito, H. Development of a new method for simple dietary education is elderly individuals with diabetes mellitus. Nippon. Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2002, 39, 527–532. [Google Scholar] [CrossRef]
- Tamban, C.; Isip-Tan, I.T.; Jimeno, C. Use of Short Message Services (SMS) for the Management of Type 2 Diabetes Mellitus: A Randomized Controlled Trial. J. ASEAN Fed. Endocr. Soc. 2013, 28, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Tang, P.C.; Overhage, J.; Chan, A.S.; Brown, N.L.; Aghighi, B.; Entwistle, M.P.; Hui, S.L.; Hyde, S.M.; Klieman, L.H.; Mitchell, C.J.; et al. Online disease management of diabetes: Engaging and Motivating Patients Online with Enhanced Resources-Diabetes (EMPOWER-D), a randomized controlled trial. J. Am. Med Inform. Assoc. 2013, 20, 526–534. [Google Scholar] [CrossRef] [Green Version]
- Thom, D.H.; Ghorob, A.; Hessler, D.; De Vore, D.; Chen, E.; Bodenheimer, T.A. Impact of Peer Health Coaching on Glycemic Control in Low-Income Patients with Diabetes: A Randomized Controlled Trial. Ann. Fam. Med. 2013, 11, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varney, J.E.; Weiland, T.; Inder, W.; Jelinek, G.A. Effect of hospital-based telephone coaching on glycaemic control and adherence to management guidelines in type 2 diabetes, a randomised controlled trial. Intern. Med. J. 2014, 44, 890–897. [Google Scholar] [CrossRef]
- Wild, S.H.; Hanley, J.; Lewis, S.C.; McKnight, J.A.; McCloughan, L.B.; Padfield, P.L.; Parker, R.A.; Paterson, M.; Pinnock, H.; Sheikh, A.; et al. Supported Telemonitoring and Glycemic Control in People with Type 2 Diabetes: The Telescot Diabetes Pragmatic Multicenter Randomized Controlled Trial. PLoS Med. 2016, 13, e1002098. [Google Scholar] [CrossRef]
- Ohkubo, Y.; Kishikawa, H.; Araki, E.; Miyata, T.; Isami, S.; Motoyoshi, S.; Kojima, Y.; Furuyoshi, N.; Shichiri, M. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: A randomized prospective 6-year study. Diabetes Res. Clin. Pr. 1995, 28, 103–117. [Google Scholar] [CrossRef]
- Franz, M.J.; Powers, M.A.; Leontos, C.; Holzmeister, L.A.; Kulkarni, K.; Monk, A.; Wedel, N.; Gradwell, E. The Evidence for Medical Nutrition Therapy for Type 1 and Type 2 Diabetes in Adults. J. Am. Diet. Assoc. 2010, 110, 1852–1889. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition Therapy Recommendations for the Management of Adults with Diabetes. Diabetes Care 2013, 37, S120–S143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Zhang, P.; Wang, J.; Gregg, E.; Yang, W.; Gong, Q.; Li, H.; Li, H.; Jiang, Y.; An, Y.; et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: A 20-year follow-up study. Lancet 2008, 371, 1783–1789. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (yr)/ Country | Intervention Group Intervention Method | Control Group | Age (yr) M ± SD or Median (IQR) | Length of Program | Result | Authors’ Conclusions |
|---|---|---|---|---|---|---|
| * Adachi (2013) Japan [14] | (A) Structured individual-based lifestyle education (SILE) program (n = 84) | (B) Control group (n = 70) | (A) 60.4 ± 11.4 (B) 62.3 ± 10.1 | 6 M | MD −0.30 95% CI [−0.65, 0.05] | The SILE program that was provided in primary care settings for patients with type 2 diabetes resulted in greater improvement in HbA1c levels than usual diabetes care and education. |
| * Agurscollins (1997) USA [15] | (A) Intervention (n = 32) | (B) Control group (n = 32) | (A) 62.4 ± 5.9 (B) 61.0 ± 5.7 | 3 M/6 M | MD −0.80 95% CI [−1.71, 0.11] | The decrease in HbA1c values was generally independent of the relatively modest changes in dietary intake, weight, and activity and may reflect indirect program effects on other aspects of self-care. |
| * Cade (2009) Canada [16] | (A) Peer Expert Patient Program (EPP) (n = 86) | (B) Control group (n = 108) | (A) 65.4 ± 11.6 (B) 66.2 ± 11.5 | 6 M/12 M | MD 0.00 95% CI [−0.35, 0.35] | The EPP approach was not effective in changing measures of diabetes control or diet. |
| * Cheng (2018) China [17] | (A) Empowerment-based self-management program (n = 121) | (B) Control group (n = 121) | (A) 56.13 ± 10.72 (B) 53.91 ± 13.01 | 5 M | MD −0.66 95% CI [−1.19, −0.13] | Findings indicate that the patient-centered, empowerment-based self-management intervention program did not induce a significant HbA1c reduction. |
| * Christensen (2013) Denmark [18] | (A) Low-fruit (n = 31) | (B) High-fruit (n = 32) | (A) 57 ± 12 (B) 59 ± 12 | 3 M | MD −0.10 95% CI [−0.15, −0.05] | HbA1c decreased in both groups with no difference between the groups (difference: 0.19%, 95% CI: −0.23 to 0.62). |
| * Dong (2018) China [19] | (A) Health education using the WeChat platform plus usual care (n = 60) | (B) Control group (n = 59) | NR | 6 M/12 M | MD −1.72 95% CI [−1.99, −0.91] | Health education of diabetic individuals via the WeChat platform in conjunction with conventional diabetes treatment could improve glycemic control and positively influence other aspects of diabetes self-care skills. |
| * Eakin (2013) USA [20] | (A) Telephone counseling (n = 151) | (B) Control group (n = 151) | (A) 57.7 ± 8.1 (B) 58.3 ± 9.0 | 6 M | MD 0.00 95% CI [−0.37, 0.37] | No intervention effect for HbA1c (RR = 0.99, 95% CI: 0.96, 1.01). |
| * Ebrahimi (2016) Iran [21] | (A) Empowerment model (n = 50) | (B) Control group (n = 53) | (A) 46.97 ± 5.54 (B) 48.15 ± 6.52 | 3 M | MD −0.86 95% CI [−1.41, −0.31] | Study results indicated the positive effects of applying the empowerment model on the metabolic control indicators. |
| Etienne (2017) Rwanda [22] | (A) Lifestyle education program (n = 115) | (B) Control group (n = 108) | (A) 51.4 ± 10.9 (B) 50.5 ± 11.0 | 12 M | NR | This study demonstrated that a structured lifestyle group education program for people with diabetes is an attractive option in a resource-limited setting, as it showed significant benefits in improved glycemic control over 12 months. |
| * Fan (2016) Australia [23] | (A) Individualized education (n = 138) | (B) Control group (n = 138) | (A)62.94 ± 10.72 (B) 64.89 ± 10.14 | 6 M | MD −0.74 95% CI [−1.27, −0.21] | Individualized diabetes education is more effective than group education in facilitating the control of type 2 diabetes. |
| * Farmer (2009) UK [24] | (A) Intensive self-monitoring blood glucose (n = 151) | (B) Control group (n = 152) | (A) 65.5 ± 9.9 (B) 66.3 ± 10.2 | 12 M | MD −0.13 95% CI [−0.38, 0.12] | Significant improvement in glycemic control compared with usual care monitored by HbA1c levels. |
| * Jayasuriya (2015) Australia [25] | (A) Diabetes Self-Management (DSM) Intervention (n = 28) | (B) Control group (n = 25) | (A) 51.5 ± 7.5 (B) 51.4 ± 7.1 | 6 M | MD −1.30 95% CI [−2.10, −0.50] | There was a significant difference in HbA1c between the groups. |
| * Lim (2011) South of Korea [26] | (A) Based ubiquitous healthcare service (n = 49) | (B) Control Group (n = 48) | (A) 67.2 ± 4.1 (B) 68.1 ± 5.5 | 6 M | MD −0.40 95% CI [−0.80, −0.00] | U-healthcare service achieved better glycemic control with less hypoglycemia than SMBG (self-monitored blood glucose) and routine care and may provide effective and safe diabetes management in elderly diabetic patients. |
| * Lenjawi (2017) Qatar [27] | (A) Nurse-led, group-based diabetes educational program (n = 109) | (B) Control group (n = 181) | (A) 52 ± 8.9 (B) 55 ± 9.7 | 12 M | MD −0.55 95% CI [−0.94, −0.16] | The inclusion of South Asian patients with type II diabetes in a structured, theory-based diabetes educational program that is led by nurses improves glycemic and metabolic parameters after 12 months. |
| * Ménard (2005) Canada [28] | (A) Intensive multi therapy (n = 34, 32) | (B) Control group (n = 35, 29) | (A) 53.7 ± 7.5 (B) 55.9 ± 8.6 | 12 M/18 M | MD −1.10 95% CI [−1.65, −0.55] | Successful in helping patients meet most of the goals set by a national diabetes association. However, 6 months after intensive therapy stopped and patients returned to the control group, the benefits had vanished. |
| * Mohamed (2013) Qatar [29] | (A) Culturally sensitive, structured education program (CSSEP) (n = 109) | (B) Control group (n = 181) | (A) 52 ± 8.9 (B) 55 ± 10.7 | 12 M | MD −0.55 95% CI [−0.94, −0.16] | After 12 months of participation, the intervention was shown to have led to a statistically significant reduction in HbA1C in the CSSEP group. |
| * Muchiri (2015) South Africa [30] | (A) Nutrition education sessions (n = 41) | (B) Control group (n = 41) | (A) 59.4 ± 6.9 (B) 58.2 ± 8.0 | 6 M/12 M | MD −0.6 95% CI [−1.43, 0.23] | Nutrition education was not efficacious on HbA1c. |
| * Moreira (2015) Brazil [31] | (A) Nursing case management (n = 38) | (B) Control group (n = 39) | (A) 50.0 ± 6.5 (B) 50.3 ± 7.6 | 6 M/12 M | MD 0.10 95% CI [−0.86, 1.06] | Both groups showed a statistically significant reduction in HbA1c at 6- and 12-months following baseline. |
| * Moncrieft (2016) USA [32] | (A) Lifestyle intervention (n = 55, 40, 41) | (B) Control group (n = 51, 47, 46) | (A) 54.8 ± 8.27 (B) 54.8 ± 6.34 | 6 M/12 M | MD −0.50 95% CI [−1.11, 0.11] | Multicomponent behavioral interventions targeting weight loss and depressive symptoms as well as diet and physical activity are efficacious in the management of Type 2 diabetes. |
| * Naik (2011) USA [33] | (A) Empowering Patients in Care (EPIC) (n = 45) | (B) Control group (n = 42) | (A) 63.82 ± 7.9 (B) 63.45 ± 7.8 | 3 M/12 M | MD −0.66 95% CI [−1.23, −0.09] | Primary care-based DM group clinics that include structured goal-setting approaches to self-management can significantly improve HbA1c levels after intervention and maintain improvements for 1 year. |
| * Peimani (2017) Iran [34] | (A) Peer support intervention (n = 100) | (B) Control group (n = 100) | (A) 59.0 ± 11.3 (B) 58.8 ± 11.7 | 6 M | MD −0.50 95% CI [−0.87, −0.13] | Peer support activities can be successfully applied in diabetes self-management, especially in areas with a shortage of professionals and economic resources. |
| * Philistsimkas (2011) USA [35] | (A) Trained peer education (n = 104) | (B) Control group (n = 103) | (A) 52.2 ± 9.6 (B) 49.2 ± 11.8 | 4 M/10 M | MD 0.00 95% CI [−0.62, 0.62] | The Project Dulce model of culturally sensitive, peer-led education, demonstrates improvement in glucose and metabolic control and suggests that this low-cost approach to self-management education for high-risk diabetic populations is effective. |
| * Ramadas (2018) Malaysia [36] | (A) Web-based dietary (n = 66) | (B) Control group (n = 62) | (A) 49.6 ± 10.7 (B) 51.5 ± 10.3 | 6 M/12 M | MD 0.40 95% CI [−0.30,1.10] | Aided by improvements in knowledge and attitudes. |
| * Rock (2014) USA [37] | (A) Low fat (n = 74) (B) High fat (n = 77) | (C) Control group (n = 76) | (A) 55.5 ± 9.2 (B) 57.3 ± 8.6 (C) 56.8 ± 9.3 | 6 M/12 M | LF MD −0.30 95% CI [−0.89, 0.29] HF MD −0.90 95% CI [−1.43, −0.37] | The weight loss program resulted in greater weight loss and improved glycemic control in type 2 diabetes patients. |
| * Reale (2019) Italy [38] | (A) Individual education (IE) (n = 27) | (B) Control group (n = 28) | (A) 59.4 ± 9.1 (B) 61.5 ± 8.2 | 3 M/8 M | MD −0.10 95% CI [−0.61, 0.41] | Our trial provides preliminary data regarding the efficacy of structured group and individual education on achieving better neurometabolic control without drug therapy reinforcement and with positive effects on patients’ attitudes and treatment satisfaction. |
| * Samuelhodge (2009) USA [39] | (A) Church-based diabetes self- management (n = 102/101) | (B) Control group (n = 72/69) | (A) 57.0 ± 0.9 (B) 61.3 ± 1.3 | 8 M/12 M | MD −0.40 95% CI [−0.43, −0.37] | At 12 months, the difference between groups was not significant. The church-based intervention was well received by participants and improved short-term metabolic control. |
| * Shahid (2015) Pakistan [40] | (A) Mobile phone intervention (n = 220) | (B) Control group (n = 220) | (A) 48.95 ± 8.83 (B) 49.21 ± 7.92 | 4 M | MD −0.73 95% CI [−0.96, −0.50] | Helpful in lowering HbA1c levels in the intervention group through direct communication with the diabetic patients. |
| * Souza (2017) Brazil [41] | (A) Community health worker educational program (n = 62) | (B) Control group (n = 56) | (A) 62.6 ± 11.2 (B) 58.9 ± 11.5 | 4 M | MD −0.50 95% CI [−1.31, 0.31] | A significant decrease in HbA1c was observed during patients’ follow-up, but it was similar in the intervention and control groups. |
| Spencer (2011) USA [42] | (A) Community health worker intervention (n = 56) | (B) Control group (n = 57) | NR | 6 M | NR | This study contributes to the growing evidence for the effectiveness of community health workers and their role in multi-disciplinary teams engaged in culturally appropriate health care delivery. |
| * Stone (2010) USA [43] | (A) Active care management with home telemonitoring (ACM + HT) (n = 59) | (B) Monthly care coordination telephone call (CC) (n = 69) | NR | 3 M/6 M | MD −0.70 95% CI [−1.13, −0.27] | Compared with the CC group, the ACM + HT group demonstrated significantly greater reductions in A1C by 3 and 6 months. |
| * Takahashi (2004) Japan [44] | (A)Simple new education group (n = 15) (C) Long pt. simple education (n = 19) | (B) Conventional education group (n = 15) (D) Long patient conventional education group (n = 19) | New Pt (A) 67.4 ± 8.0 (B) 67.1 ± 8.0 Long Pt (A) 74.4 ± 6.0 (B) 74.2 ± 5.3 | 3 M/6 M/12 M | New MD −0.10 95% CI [−0.69,0.49] Long MD 0.60 95% CI [−0.02, 1.22] | Simple dietary education is useful and effective for elderly diabetic patients on their first visit in a similar fashion to conventional dietary education. Because of the small effects of both types of education on glucose control in long-term patients, more psychosocial support may be necessary. |
| * Tamban (2013) Philippine [45] | (A) Short message services (SMS) (n = 52) | (B) Control group (n = 52) | (A) 48.0 ± 8.1 (B) 51.0 ± 6.2 | 3 M/6 M | MD −0.35 95% CI [−0.69, −0.01] | The use of SMS as an adjunct to the standard of DM care improved a significant reduction in HbA1c levels after 3 and 6 months. |
| * Tang (2012) USA [46] | (A) Online with enhanced resources for diabetes (n = 186) | (B) Control group (n = 193) | (A) 54 ± 10.7 (B) 53 ± 10.2.2 | 6 M/12 M | MD −0.23 95% CI [−0.58,0.12] | Intervention patients achieved greater decreases in A1C at 6 months than control patients, but the differences were not sustained at 12 months. More intervention group patients than control patients achieved improvement in A1C (>0.5% decrease). |
| * Thom (2013) USA [47] | (A) Peer Health coaching (n = 122) | (B) Control group (n = 114) | (A) 56.3 ± 10.3 (B) 54.1 ± 10.4 | 6 M | MD −0.57 95% CI [−1.12, −0.02] | Peer health coaching significantly improved diabetes control in this group of low-income primary care patients. |
| Varney (2014) Australia [48] | (A) Telephone coaching (n = 47) | (B) Control group (n = 47) | (A) 59 (56–62) (B) 64 (61–66) | 6 M/12 M | NR | Significant interaction effects were observed between group and time at 6 months, demonstrating improvement in HbA1C, fasting glucose, diastolic blood pressure, and physical activity. The intervention’s effect on these parameters was not sustained at 12 months. |
| * Wild (2016) England [49] | (A) Tele monitoring (n = 146) | (B) Control group (n = 139) | (A) 60.5 ± 9.8 (B) 61.4 ± 9. | 9 M | MD −0.50 95% CI [−0.81, −0.19] | Supported telemonitoring resulted in clinically important improvements in the control of glycemia in patients with type 2 diabetes in family practice. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Hur, M.-H. The Effects of Dietary Education Interventions on Individuals with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8439. https://doi.org/10.3390/ijerph18168439
Kim J, Hur M-H. The Effects of Dietary Education Interventions on Individuals with Type 2 Diabetes: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(16):8439. https://doi.org/10.3390/ijerph18168439
Chicago/Turabian StyleKim, Juri, and Myung-Haeng Hur. 2021. "The Effects of Dietary Education Interventions on Individuals with Type 2 Diabetes: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 16: 8439. https://doi.org/10.3390/ijerph18168439
APA StyleKim, J., & Hur, M. -H. (2021). The Effects of Dietary Education Interventions on Individuals with Type 2 Diabetes: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(16), 8439. https://doi.org/10.3390/ijerph18168439