
A Qualitative Evaluation of Young People’s, Parents’ and Carers’ Experiences of a National and Specialist CAMHS Dialectical Behaviour Therapy Outpatient Service


Abstract
:1. Introduction
1.1. Dialectical Behaviour Therapy (DBT)
1.2. DBT for Adolescent Populations
- To evaluate the acceptability of the treatment programme;
- To explore service users’ retrospective expectations of DBT;
- To investigate perceived benefits of the treatment programme, and specifically whether certain treatment components were experienced more favourably and beneficially to service users (e.g., individual therapy, skills groups, and phone support);
- To explore suggestions for improvements and modifications of the treatment programme;
- To explore service user’s experience of using DBT skills to manage their difficulties and investigate the type of skills used outside of therapy; and
- To evaluate service users’ reflections on their symptomatology, problems, and achievements having completed the treatment programme.
2. Materials and Methods
3. Results
3.1. Demographics & Descriptive Statistics
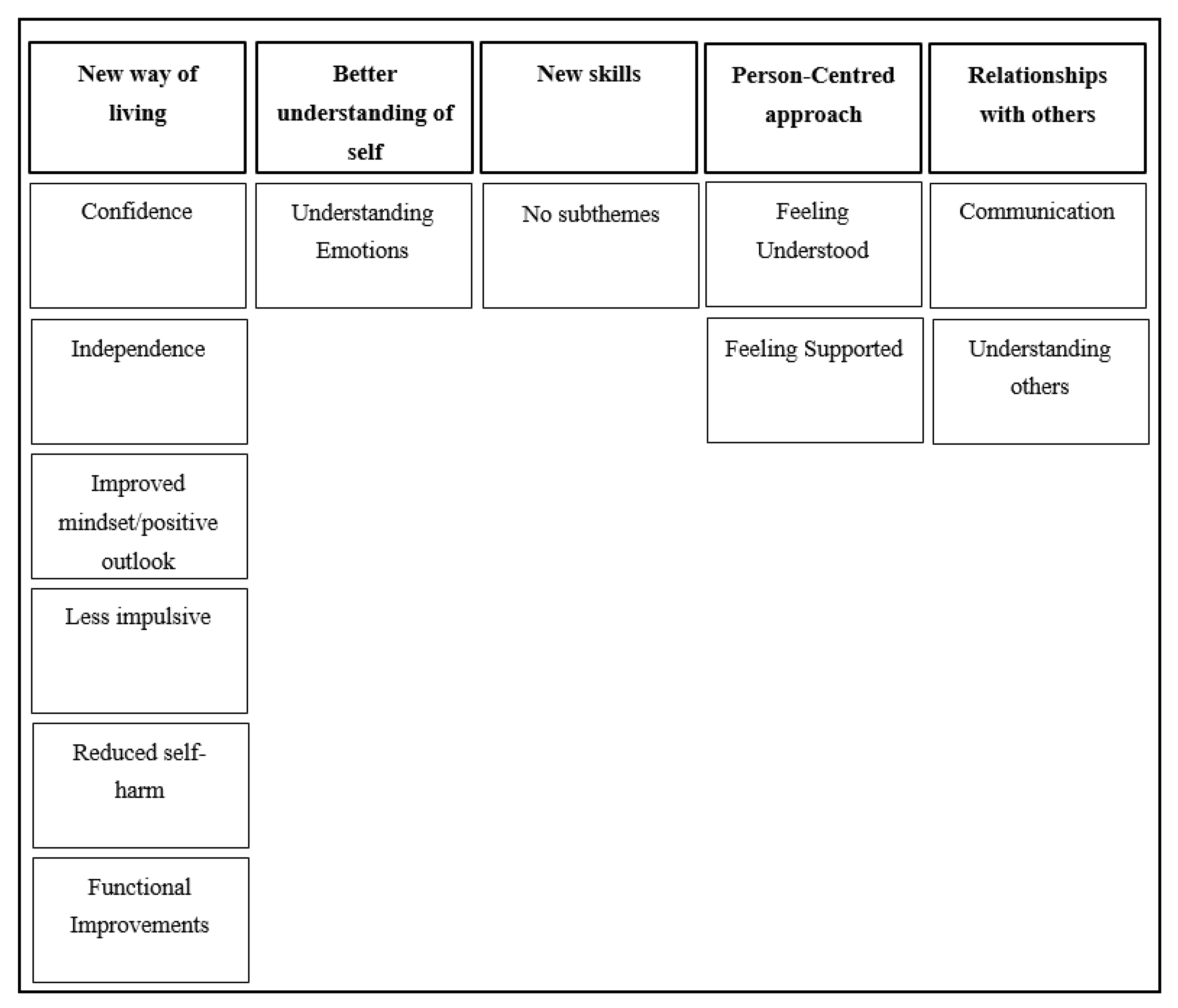
3.2. Theme 1: New Way of Living
P2: I don’t think I maybe have like a quality of life that everyone would think is amazing. But for someone that like is blatant and I’ve got certain difficulties, I think for someone like me, like, wow, my life is so much, so much better.
3.2.1. Subtheme 1A: Confidence
P6: It was more because like I was not very well, so I kind of, I knew that I seem a lot happier now and that…I definitely seem more confident sometimes…
3.2.2. Subtheme 1B: Independence
P1: And then I think I’m a lot more self-sufficient and before I was too anxious to go out by myself or like do things by myself. And now I’m a lot more willing to do that.
3.2.3. Subtheme 1C: Improved Mindset/Positive Outlook
P15: I’m less negative about the world, in general, about myself and about others, less judgemental, less comparing, but obviously I still feel like I still do it [judge/compare] ’cause I don’t even notice when I do it half the time. But as soon as I catch myself it’s an opportunity to learn...
P14: I can be in a difficult situation and at first be distressed but then think about ways I can help improve it, using like the skills that I’ve been taught, and maybe not just improve the situation but maybe improve my mindset on it instead.
3.2.4. Subtheme 1D: Less Impulsive
P14: I’m not as impulsive as I used to be. I don’t act straight away in the moment, most of the time. I can calm myself down and think how I can improve the situation in a healthier way.
3.2.5. Subtheme 1E: Reduced Self-Harm
P14: Like [before DBT] I got given a few skills to help with self-harm and things like that but there was no kind of reinforcement in it, it wasn’t…seen as such in a negative way. Like if I’d hurt myself, she’d just be like: ‘Oh, okay, what can you do better next time? Let’s carry on.’ Whereas in DBT you’ve got the whole chain thing that you have to do and it’s kind of seen more as a negative thing which in a way I think has helped with me stopping because it’s kind of been reinforced that it’s not a good thing to do compared to before, where it was seen as kind of a little bit normal.
P11: I rarely self-harm. I haven’t had a suicidal incident in a long time. I haven’t been in hospital for a very long time.
3.2.6. Subtheme 1F: Functional Improvements
P9: They may have seen like a boost in motivation, considering I was out of school for a very long time probably like almost two years. And then, I’ve successfully integrated from being in hospital to going back to mainstream school.
3.3. Theme 2: Better Understanding of Self
Interviewer: What do these skills and techniques kind of do for you? How do they help you?
P10: …they help me to identify what emotion I’m feeling…or where in my body it’s feeling…for example if I’m getting really anxious I’ll get lots of like pain in my stomach or I’ll feel like my chest is really heavy...So instead of like stressing about that I’ll be like thinking “oh, I’m feeling this because of this”, or if I’m feeling really like dissociated or just not connected at all, the grounding techniques really help me to get back.
P15: I feel like I thought I knew things before…but I feel like I have a better understanding, like a more broad understanding of just things…that help me.
Interviewer: So, is it like a more broad understanding of you or like how to manage…
P15: Yeah, just how my mind works, like my thoughts and emotions, like I don’t feel like I’m just a slave to my thoughts and I just react…I’m able now to regain control over that to benefit myself.
Subtheme 2A: Understanding of Emotions
P18: I’m much more aware of my thoughts and of like where they’re coming from, and whether they are rational or not. I therefore find it easier to control my behaviour…I find it easier to regulate emotions.
P1: I think it gave you a chance to really explore your feelings on why you felt this way and I think it was different to a lot of things I’ve done in the past...It’s more specific and you look into your traumas more in depth. And look at them as reasons for emotional responses and I thought that was really useful and it gives you insight into why you react in certain ways so you can then control the way you react.
3.4. Theme 3: New Skills
P2: …felt like I was just a slave to my emotions and now having those skills and having like everything I learned in group…I actually feel like I have a functioning life now.
3.5. Theme 4: Person-Centred Approach
P10: …like other therapies that I’ve had, they’re all quite broad, so the therapies will be exactly the same for every individual while like I feel like DBT can be very specified for that person even though it’s the same DBT…so I think that’s why it’s very beneficial.
3.5.1. Subtheme 4A: Feeling Understood
P3: I found group quite helpful because…it makes you feel like you’re not alone. There are other people actually there and know how you feel.
P3: That staff need to understand they need to…just they can’t assume things…just ask your patient or client…you may have assumptions but don’t tell them until like the reason they done something has come out and just like ‘well, this is what I thought, but I’m glad you kind of told me it wasn’t that’. That’s how I think it should come.
3.5.2. Subtheme 4B: Feeling Supported
P16: I think the support. Like you have to have a good therapist, you have to have a good care co-ordinator, you have to have a good team, to use the skills. And when I was ever stuck on a skill or I didn’t know like what to do or I was just distressed, they would help me get myself out of that…
P14: …there are some times when I have got frustrated because of phone coaching. And maybe that’s kind of down to my thought process instead of actually DBT. I don’t know, but when I’m looking for kind of reassurance on something and I get told to use skills…I know it’s phone coaching for skills but it’s a bit invalidating sometimes?
3.6. Theme 5: Relationships with Others
P3: One of my relationships has improved and that’s with my mum…I think it was more that [the therapist] kind of explained a couple of things to my mum that I don’t think she understood before.
3.6.1. Subtheme 5A: Communication
P18: …definitely my behaviour towards relationships because before I would never be able to say sorry. I would just literally go at people, and say whatever I wanted to say. Now, I realise I have to say sorry.
P18: … [the therapist] could improve in terms of knowing when to stop asking questions. Sometimes [the therapist]…asks the same questions again and again...Or if it’s at a time when I can’t answer for a reason, like I’m really dissociated… [the therapist] still asks the question, like “what do you need?”…again and again. But if I’m not in the place to answer that and I say like ‘I can’t answer this right now’, [the therapist] just keeps asking it for too long, [the therapist] doesn’t know when to stop.
3.6.2. Subtheme 5B: Understanding Others
P18: I feel much more able to…communicate with people in the right way, in terms of like validating them, understanding their needs, and also communicating when I need help.
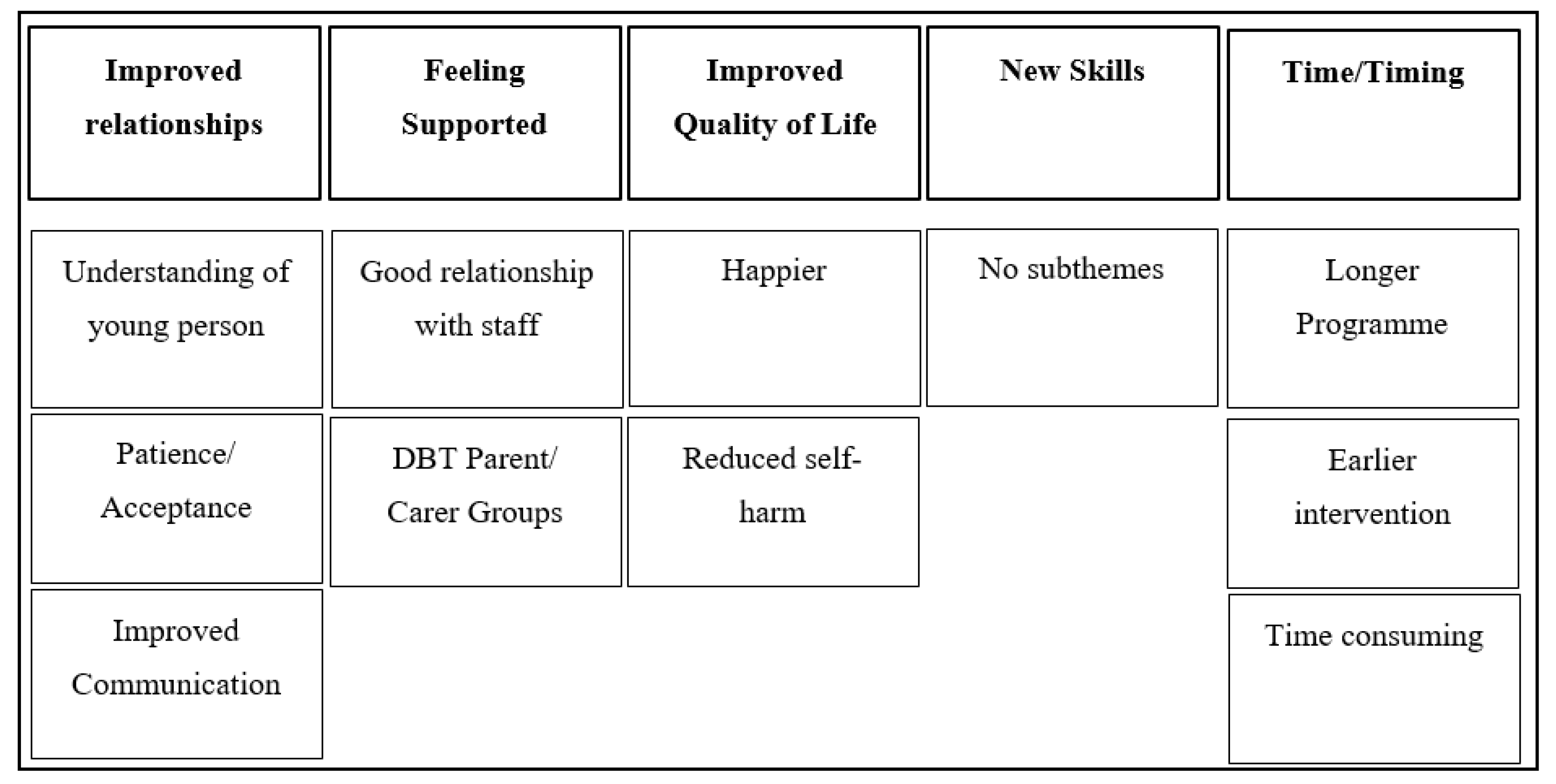
3.7. Theme 1: Improved Relationships
P4: Closer relationship. I think I would say it’s helped with, specially with her dad ’cause they were not as close. I think him coming along and being part of it, too, and learning things has helped him to understand so their relationship [has] improved.
P6: …realising that actually we are human so me and my wife are working as a team...recognising when my wife might need some help and recognising…when I might not be so great at communicating…helping me out in those situations.
3.7.1. Subtheme 1A: Understanding of Young Person
P4: The understanding of why she feels how she feels and like for me coming to…the parent meetings and being, you know, more understanding. And, you know, having the understanding of why they’re doing what they’re doing and why their emotions are up and down. You know, breaking down what is happening and understanding why they’re doing it.
3.7.2. Subtheme 1B: Patience/Acceptance
P16: Yeah, I think it’s just to look at life in a different way…to be more accepting. More accepting of the good and bad as well and just accepting of the situation. This is…what it is, we’re gonna try and make the best of it and, obviously, if it improves, it’s a blast, but at the moment we work with what we’ve got and we’ll have to give it our all and we’ll see, it could be worse. We were at a worse place [before].
3.7.3. Subtheme 1C: Improved Communication
P3: [The young person] is opening up to me a lot and…(inaudible) my other member of staff…[the young person] is very open talking about [the young person’s] emotions and the way [the young person] feels at times when…[the young person] was a bit reluctant in the beginning. But, at the end of the day, I think again the credit goes to [the therapist]. The way, the things have been explained, we have been told how to communicate with [the young person], how to deal with situations. [The young person] has improved in applying DBT skills, regulating emotions and then communicating with the staff has improved more.
P4: The last couple of years has been absolutely awful…I’m sure we’re not the first parents that you get a kid who’s self-harming, a kid who wants to kill themselves and you look at each other and you start picking at bones at each other and it drives a big wedge between the two of you…and the communication breaks down between the two of you and, yeah, that’s what DBT is about, communication, and I think it has helped us as well, not just [the young person], I think it’s helped us.
3.8. Theme 2: Feeling Supported
P3: The only advice that I would give the families who were starting…DBT…is that they’re in the most safe hands. And they should engage really well in all of the sessions, with all the professionals and I’m sure they will be looked after very well.
3.8.1. Subtheme 2A: Good Relationship with Staff
P1: …the biggest thing that I thought [the young person] benefitted from was the one-to-one relationship with [the therapist]…with the previous services we had, if it got down to discussing difficult situations, as soon as…the staff started trying to take a more neutral stance, trying to support us a bit as parents, it felt like to [the young person] that she was being picked on or we were ganging up on her. Whereas [the therapist] was able to maintain…the kind of closer relationship with [the young person] throughout and…that really encouraged her, and I think really helped.
3.8.2. Subtheme 2B: DBT Parent/Carer Groups
P5: I think I really needed the parent group at the time…it’s nice to know that you are not the only one dealing with it…it makes such a difference to think that it’s not just you and…it’s normal parents…you just feel like a terrible person sometimes and there’s other people in there that are just nice people. Not all these horrible people that because you think ‘Am I a terrible person?’…they’re just normal parents living their everyday life, having struggled with their children.
3.9. Theme 3: Improved Quality of Life
P2: And we’ve just been doing like normal things, like taking her shopping, that’s been amazing. Where, to start with, we couldn’t leave her in a shop on her own, we had to stay with her, she didn’t feel strong enough to just stand in a shop and you know browse. We had to be like two centimetres away from her.
3.9.1. Subtheme 3A: Happier
P6: …generally that we’re a happier bunch than maybe we were before. So, yeah, there’s a strength as well.
3.9.2. Subtheme 3B: Reduced Self-Harm
P2: …she’s not had any self-harming, any major incidents for quite a while now…things have been a lot calmer at home since she’s not being having to go to A&E.
3.10. Theme 4: New Skills
P5: She knows how to deal with things so much better because of all the strategies she’s learned through the DBT treatment, and when she’s getting stressed with something, she uses these.
P4: Even the…mindfulness and relaxation techniques, I never thought that I’d embrace it and there I am downloading my apps…
3.11. Theme 5: Timing/Time
P5: …not so helpful was probably…phone calls last minute for a meeting and expecting to drop things at the last minute…And I’m a single parent that works and somebody needs to make money and I can’t just drop things…Yeah, and as much as I want to go and be part of the meeting, I can’t just drop things just like that because if I drop things just like that I won’t get paid.
3.11.1. Subtheme 5A: Longer Programme
P2: …it’s only time related, it’s only a year. And I know that it’s expensive, but for [the young person] it would’ve been better for her to go on a little bit longer, to possibly extend it…particularly for [the young person], she’s got a difficult time around [date] next year and it would’ve been beneficial to her to have the extra support in place…we knew it was a year when she started, but that’s still not helpful to her.
3.11.2. Subtheme 5B: Earlier Intervention
P5: …I wish we had this service a good couple of years before. We probably wouldn’t have had all the emotional upheaval that we have had, I think it would have been a lot better. And maybe [the young person] wouldn’t have cut as much as she had done and in the emotional state, she had been in…
3.11.3. Subtheme 5C: Time-Consuming
P1: Obviously, it takes a lot of time, for the best part of a year. I had to get special permission from my employers so that I could take time off…luckily, I’m in a job where I was able to get that permission, but…I didn’t miss a session…and neither did my wife. But I know…that could be a problem. It wasn’t a problem for me in the end, but I had sacrificed a promotion to basically to be able to do this but for me it wasn’t really a decision because you know obviously it’s for [the young person’s] benefit and ours.
4. Discussion
4.1. Implications
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hawton, K.; Saunders, K.E.; O’Connor, R.C. Self-Harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Ougrin, D.; Tranah, T.; Stahl, D.; Moran, P.; Asarnow, J.R. Therapeutic interventions for suicide attempts and self-harm in adolescents: Systematic review and meta-analysis. J. Am. Acad. Child. Adolesc. Psychiatry 2015, 54, 97–107. [Google Scholar] [CrossRef]
- Hessels, C.J.; Laceulle, O.M.; van Aken, M.A.; Resch, F.; Kaess, M. Differentiating BPD in adolescents with NSSI disorder: The role of adverse childhood experiences and current social relationships. Bord. Personal Disord. Emot. Dysregul. 2018, 5, 20. [Google Scholar] [CrossRef]
- Linehan, M. Cognitive-Behavioral Treatment of Borderline Personality Disorder, 1st ed.; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Crowell, S.E.; Beauchaine, T.P.; Linehan, M.M. A biosocial developmental model of borderline personality: Elaborating and extending Linehan’s theory. Psychol Bull. 2009, 135, 495–510. [Google Scholar] [CrossRef] [Green Version]
- Ruocco, A.C.; Amirthavasagam, S.; Choi-Kain, L.W.; McMain, S.F. Neural correlates of negative emotionality in borderline personality disorder: An activation-likelihood-estimation meta-analysis. Biol. Psychiatry. 2013, 73, 153–160. [Google Scholar] [CrossRef]
- Ruocco, A.C. The neuropsychology of borderline personality disorder: A meta-analysis and review. Psychiatry Res. 2005, 137, 191–202. [Google Scholar] [CrossRef]
- Guilé, J.M.; Boissel, L.; Alaux-Cantin, S.; de La Rivière, S.G. Borderline personality disorder in adolescents: Prevalence, diagnosis, and treatment strategies. Adolesc Health Med. Ther. 2018, 9, 199–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chanen, A.M.; Jackson, H.J.; McGorry, P.D.; Allot, K.A.; Clarkson, V.; Yuen, H.P. Two-Year stability of personality disorder in older adolescent outpatients. J. Pers Disord. 2004, 18, 526–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenfield, B.; Henry, M.; Weiss, M.; Tse, S.M.; Guile, J.M.; Dougherty, G.; Zhang, X.; Fombonne, E.; Lis, E.; Lapalme-Remis, S.; et al. Previously suicidal adolescents: Predictors of six-month outcome. J. Can. Acad Child. Adolesc Psychiatry 2008, 17, 197–201. [Google Scholar] [PubMed]
- National Collaboration Centre for Mental Health. Borderline Personality Disorder: Treatment and Management, 1st ed.; British Psychological Society: Leicester, UK, 2009; p. 346. [Google Scholar]
- National Institute for Health and Care Excellence. Borderline Personality Disorder: Treatment and Management; NICE Guideline No. CG78; NICE: London, UK, 2009. [Google Scholar]
- Kaess, M.; Brunner, R.; Chanen, A. Borderline personality disorder in adolescence. Pediatrics 2014, 134, 782–793. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.clinical-partners.co.uk/child-adolescents/a-z-of-issues/support-for-personality-disorders-in-children (accessed on 6 August 2020).
- Chanen, A.; Sharp, C.; Hoffman, P. Global Alliance for Prevention and Early Intervention for Borderline Personality Disorder. Prevention and early intervention for borderline personality disorder: A novel public health priority. World Psychiatry 2017, 16, 215–216. [Google Scholar] [CrossRef]
- McCauley, E.; Berk, M.S.; Asarnow, J.R.; Adrian, M.; Cohen, J.; Korslund, K.; Avina, C.; Hughes, J.; Harned, M.; Gallop, R.; et al. Efficacy of dialectical behavior therapy for adolescents at high risk for suicide a randomized clinical trial. JAMA Psychiatry 2018, 75, 777–785. [Google Scholar] [CrossRef] [Green Version]
- Mehlum, L.; Tørmoen, A.J.; Ramberg, M.; Haga, E.; Diep, L.M.; Laberg, S.; Larsson, B.S.; Stanley, B.H.; Miller, A.L.; Sund, A.M.; et al. Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: A randomized trial. J. Am. Acad. Child. Adolesc. Psychiatry 2014, 53, 1082–1091. [Google Scholar] [CrossRef] [Green Version]
- Santamarina-Perez, P.; Mendez, I.; Singh, M.K.; Berk, M.; Picado, M.; Font, E.; Moreno, E.; Martinez, E.; Morer, A.; Borràs, R.; et al. Adapted dialectical behavior therapy for adolescents with a high risk of suicide in a community clinic: A pragmatic randomized controlled trial. Suicide Life Threat Behav. 2020, 50, 652–667. [Google Scholar] [CrossRef] [PubMed]
- James, A.C.; Taylor, A.; Winmill, L.; Alfoadari, K. A preliminary community study of dialectical behaviour therapy (DBT) with adolescent females demonstrating persistent, deliberate self-harm (DSH). Child. Adolesc. Ment. Health 2008, 13, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, C.; Joyce, M.; Flynn, D.; Corcoran, P. Dialectical behaviour therapy for adolescents: A comparison of 16-week and 24-week programmes delivered in a public community setting. Child. Adolesc. Ment. Health 2019, 24, 266–273. [Google Scholar] [CrossRef]
- Lakeman, R.; Emeleus, M.; Davies, S.; Anderson, S. A pragmatic evaluation of a high fidelity dialectical behaviour therapy programme for youth with borderline personality disorder. Adv. Ment. Health 2020, 1–11. [Google Scholar] [CrossRef]
- Rathus, J.; Campbell, B.; Miller, A.; Smith, H. Treatment acceptability study of walking the middle path, a new DBT skills module for adolescents and their families. Am. J. Psychother. 2015, 69, 163–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.L.; Rathus, J.H.; Linehan, M.M. Dialectical Behavior Therapy with Suicidal Adolescents, 1st ed.; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Rathus, J.H.; Miller, A.L. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life-Threat. Behav. 2002, 32, 146–157. [Google Scholar] [CrossRef]
- Zanarini, M. McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD), 1st ed.; Jones and Bartlett Learning, LLC: Burlington, MA, USA, 2008. [Google Scholar]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Pardo, E.S.; Rivas, A.F.; Barnier, P.O.; Mirabent, M.B.; Lizeaga, I.K.; Cosgaya, A.D.; Alcántara, A.C.; González, E.V.; Aguirre, B.; Torres, M.A.G. A qualitative research of adolescents with behavioral problems about their experience in a dialectical behavior therapy skills training group. BMC Psychiatry 2020, 20, 245. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.; Crawford, T.N.; Johnson, J.G.; Kasen, S. The children in the community study of developmental course of personality disorder. J. Pers. Disord. 2005, 19, 466–486. [Google Scholar] [CrossRef] [PubMed]
- Daley, S.E.; Burge, D.; Hammen, C. Borderline personality disorder symptoms as predictors of 4-year romantic relationship dysfunction in young women: Addressing issues of specificity. J. Abnorm. Psych. 2000, 10, 451. [Google Scholar] [CrossRef]
- Chanen, A.M.; McCutcheon, L.K.; Jovev, M.; Jackson, H.J.; McGorry, P.D. Prevention and early intervention for borderline personality disorder. Med. J. Aus. 2007, 187, S18–S21. [Google Scholar] [CrossRef]
- Haga, E.; Aas, E.; Grøholt, B.; Tørmoen, A.J.; Mehlum, L. Cost-Effectiveness of dialectical behaviour therapy vs. enhanced usual care in the treatment of adolescents with self-harm. Child. Adolesc. Psychiatry Ment. Health 2018, 12, 22. [Google Scholar] [CrossRef] [Green Version]
- Robertson, A.; Alford, C.; Wallis, A.; Miskovic-Wheatley, J. Using a brief family based DBT adjunct with standard FBT in the treatment of Anorexia Nervosa. J. Eat. Disord. 2015, 3, O39. [Google Scholar] [CrossRef] [Green Version]
- Nelson-Gray, R.O.; Keane, S.P.; Hurst, R.M.; Mitchell, J.T.; Warburton, J.B.; Chok, J.T.; Cobb, A.R. A modified DBT skills training program for oppositional defiant adolescents: Promising preliminary findings. Behav. Res. Ther. 2006, 44, 1811–1820. [Google Scholar] [CrossRef]
- Lew, M.; Matta, C.; Tripp-Tebo, C.; Watts, D. Dialectical behavior therapy (DBT) for individuals with intellectual disabilities: A program description. Ment. Health Asp. Dev. Disabil. 2006, 9, 1. [Google Scholar]
- Grant, B.F.; Chou, S.P.; Goldstein, R.B.; Huang, B.; Stinson, F.S.; Saha, T.D.; Smith, S.M.; Dawson, D.A.; Pulay, A.J.; Pickering, R.P.; et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: Results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2008, 69, 533–545. [Google Scholar] [CrossRef]
- Sansone, R.A.; Sansone, L.A. Gender patterns in borderline personality disorder. Innov. Clin. Neurosci. 2011, 8, 16–20. [Google Scholar] [PubMed]
- Goodman, M.; Patil, U.; Steffel, L.; Avedon, J.; Sasso, S.; Triebwasser, J.; Stanley, B. Treatment utilization by gender in patients with borderline personality disorder. J. Psychiatr. Pract. 2010, 16, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Swales, M.; Hibbs, R.A.; Bryning, L.; Hastings, R.P. Health related quality of life for young people receiving dialectical behaviour therapy (DBT): A routine outcome-monitoring pilot. SpringerPlus 2016, 5, 1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Service Health Research Authority. Available online: https://www.hra.nhs.uk/planning-and-improving-research/policies-standards-legislation/uk-policy-framework-health-social-care-research/uk-policy-framework-health-and-social-care-research/ (accessed on 28 April 2021).



{kind=link}
{kind=link}
| Factor | Total Sample (Percentage) | |
|---|---|---|
| Gender Identity | 18 (100%) | |
| Female | 16 (88.9%) | |
| Non-Binary | 2 (11.1%) | |
| Sex Assigned at Birth * | Female | 18 (100%) |
| Sex Assigned at Birth Same or Different | Same | 16 (88.9%) |
| Different | 2 (11.1%) | |
| Sexual Orientation | Heterosexual | 8 (44.4%) |
| Bisexual | 2 (11.1%) | |
| Gay or Lesbian | 1 (5.6%) | |
| Demisexual | 1 (5.6%) | |
| Queer | 1 (5.6%) | |
| Pansexual | 1 (5.6%) | |
| Asexual | 1 (5.6%) | |
| Prefer not to say | 2 (11.1%) | |
| Unknown | 1 (5.6%) | |
| Ethnicity | White (White British, White Other) | 11 (61.1%) |
| Black African, Caribbean, or Black British | 1 (5.6%) | |
| Mixed or Multiple Ethnic Groups | 4 (22.2%) | |
| Other White/Mixed European | 1 (5.6%) | |
| Other Ethnic Group (Hispanic) | 1 (5.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratnaweera, N.; Hunt, K.; Camp, J. A Qualitative Evaluation of Young People’s, Parents’ and Carers’ Experiences of a National and Specialist CAMHS Dialectical Behaviour Therapy Outpatient Service. Int. J. Environ. Res. Public Health 2021, 18, 5927. https://doi.org/10.3390/ijerph18115927
Ratnaweera N, Hunt K, Camp J. A Qualitative Evaluation of Young People’s, Parents’ and Carers’ Experiences of a National and Specialist CAMHS Dialectical Behaviour Therapy Outpatient Service. International Journal of Environmental Research and Public Health. 2021; 18(11):5927. https://doi.org/10.3390/ijerph18115927
Chicago/Turabian StyleRatnaweera, Namali, Katrina Hunt, and Jake Camp. 2021. "A Qualitative Evaluation of Young People’s, Parents’ and Carers’ Experiences of a National and Specialist CAMHS Dialectical Behaviour Therapy Outpatient Service" International Journal of Environmental Research and Public Health 18, no. 11: 5927. https://doi.org/10.3390/ijerph18115927
APA StyleRatnaweera, N., Hunt, K., & Camp, J. (2021). A Qualitative Evaluation of Young People’s, Parents’ and Carers’ Experiences of a National and Specialist CAMHS Dialectical Behaviour Therapy Outpatient Service. International Journal of Environmental Research and Public Health, 18(11), 5927. https://doi.org/10.3390/ijerph18115927