
The COVID-19 Pandemic in Spain: Experiences of Midwives on the Healthcare Frontline

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Context of the Study
2.3. Selection and Characteristics of Participants
- Hospital midwives who continued to provide care in delivery rooms during these months;
- Midwives who provide care at home births;
- Primary care midwives who continued to provide care throughout these months;
- Hospital midwives at centers where the delivery rooms were closed and who were transferred to care for COVID-19 patients;
- Midwives in hospital or primary care sectors who contracted COVID-19 while carrying out their work;
- Hospital or primary care midwives who were pregnant or who became pregnant at the start of the pandemic.
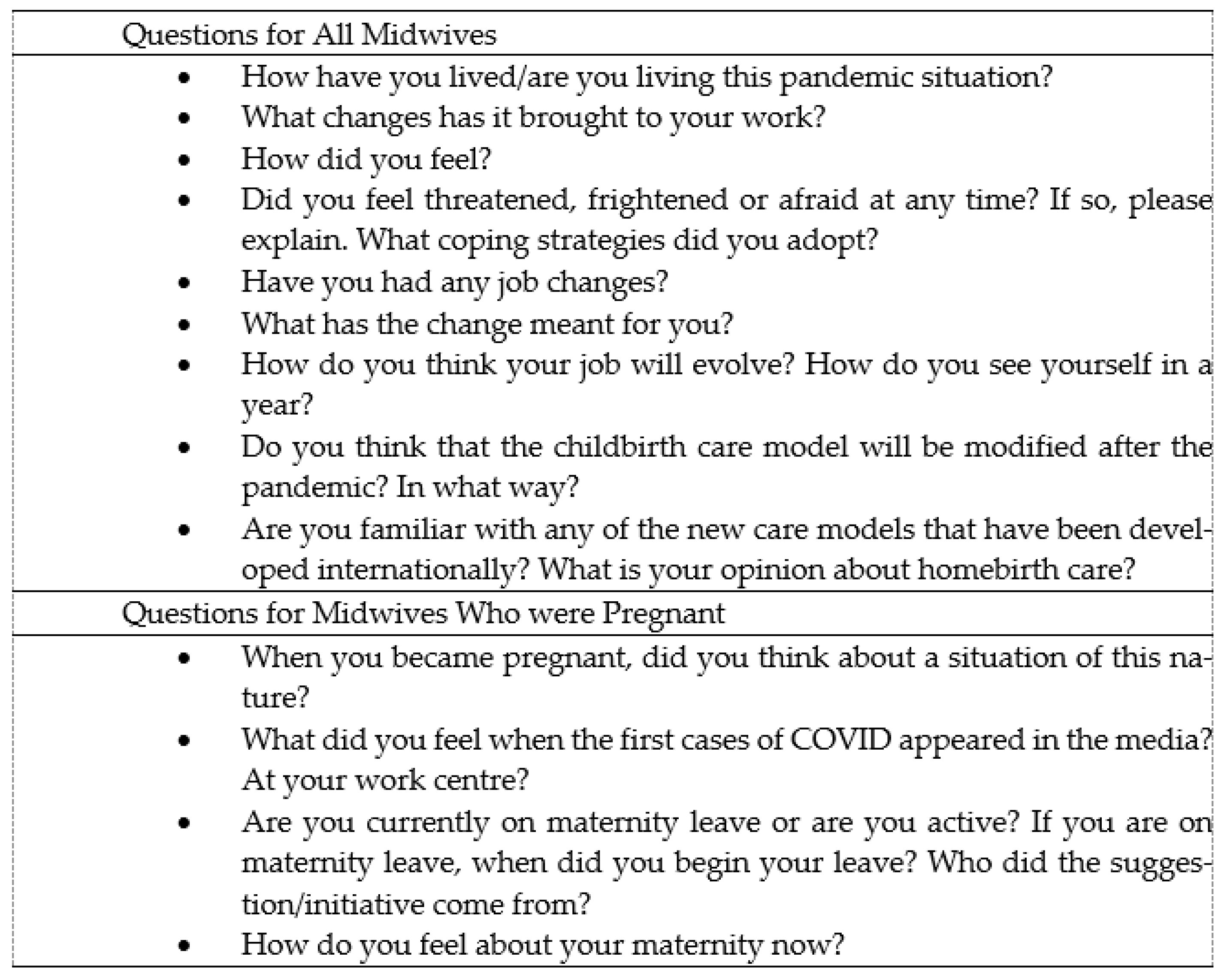
2.4. Technique Used to Gather the Information
2.5. Ethical Aspects
2.6. Criteria for Methodological Rigor
2.7. Data Analysis
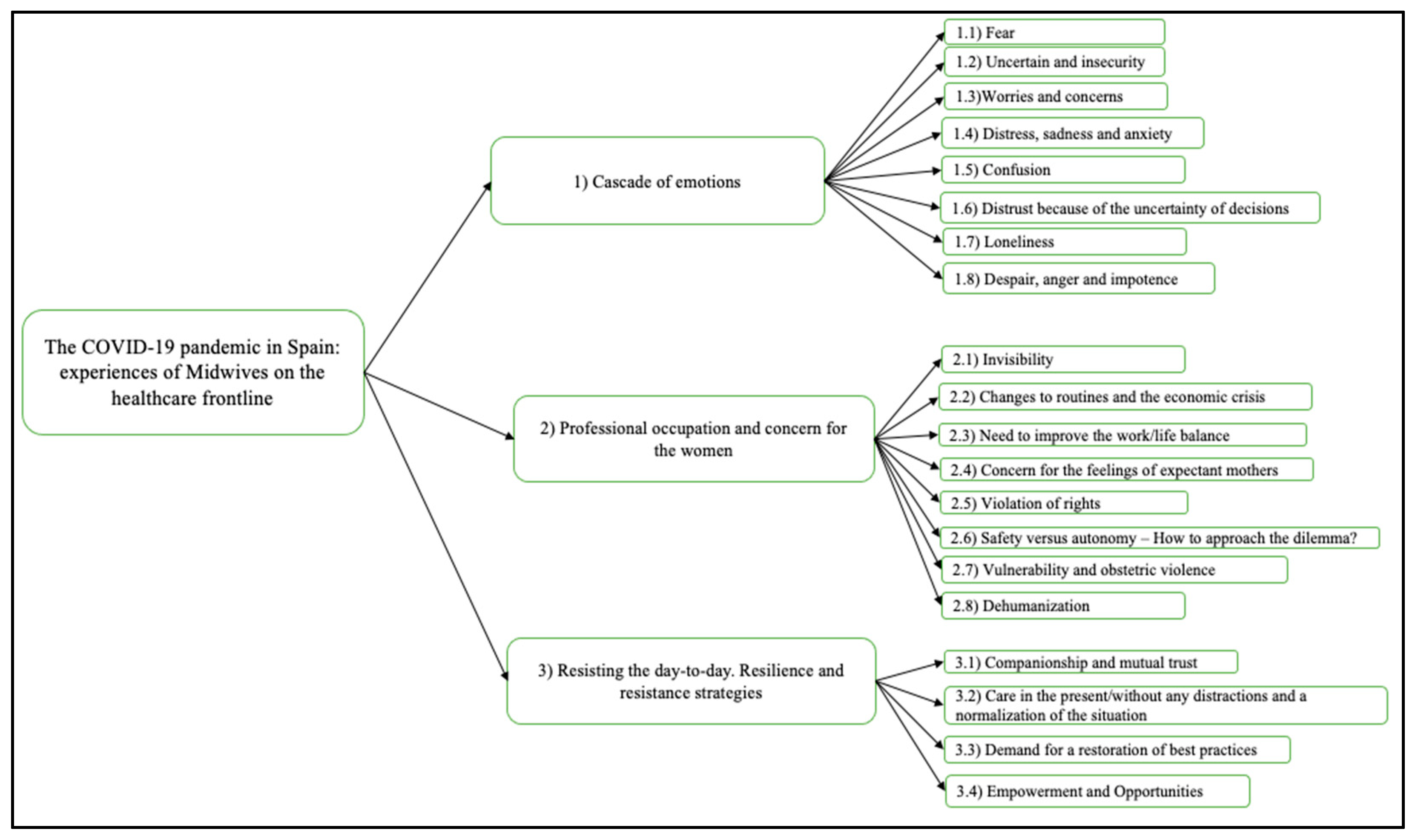
3. Results
3.1. Cascade of Emotions
3.1.1. Fear
“Well, at the beginning I was a bit scared, like everyone I guess, I sort of freaked out when the state of alarm was declared nationwide, it was a bit shocking. I’d never been in a situation like that in my whole life and it was a bit shocking especially because of the fear of becoming infected”.(Aurora)
“Of course, we were scared at first, because we hadn’t worked as nurses for a long time...”.(Alice)
3.1.2. Uncertainty and Insecurity
“Everyone was a bit lost at the time, didn’t know what to think, even when we knew what was going on in China or Italy, in my opinion nobody could have imagined... It felt like we were immersed in a virtual reality”.(Nancy)
“[...] because it’s a whole new situation and you’re aware that there won’t be any equipment available...”.(Alice)
“[...] then for a while there was nobody in charge, leading the whole process, it seemed that we were being isolated, and then the thing with the PPE (Personal Protection Equipment), it was not clear what we were supposed to do or when and how we had to wear it [...]”.(Elisa)
“[...] we had the feeling that we were drifting because nobody was directly responsible for coordinating our response”.(Jennifer)
“Other nurses were transferred to another floor. Obviously, some of us had not worked in a hospital floor unit for many years, taking care of the patient’s hygiene with the nursing assistants, with... You know, usually we don’t take care of the patient’s hygiene in the delivery room. We clean the mother, but they are self-sufficient... And then, of course, all of a sudden, you have much older patients. And obviously you gotta deal with their nappies, well... it’s a huge change of role, the way you take care of the patient, it’s a totally different patient”.(Aurora)
“[...] it’s true that as things were getting better, we had more equipment, more PPE, we were calmer, right? You feel safer doing your job”.(Elisa)
“Besides this, I looked up some things on the Internet and I also searched for articles about the pandemic in China but there wasn’t too much information about the consequences that infection could cause during pregnancy. It was initially thought that infection did not pose a threat for pregnant women but with the passing of time, we started to see that some studies associated it with a higher risk of preeclampsia and a greater risk of other pathologies, and since my pregnancy had been diagnosed as high risk, well I got even more scared”.(Aurora)
3.1.3. Worries and Concerns
“Maybe it’s true that my healthcare practices are a bit unorthodox in this sense. I don’t completely trust studies that undermine what’s going on and underplay the risks, maybe I feel a bit insecure in this regard”.(Nancy)
“Because of the uncertainty, because I don’t know what the situation will be like in a year, I find myself struggling to cope with my family life and keep working at the usual rhythm, because I like to give my best at work, and having to slow everything down takes its toll, because I’m a very active person, but I think I’m managing, trying to keep calm. Now I’m just in survival mode”.(Bárbara)
3.1.4. Distress, Sadness and Anxiety
“[...] you’re working there coping with the anxiety of not knowing if you’re properly equipped, of not knowing if you’re dealing with infected people... perhaps you’ll take the virus home with you, and then you realize that the people in charge are also sick at home, the situation was a bit...”.(Jennifer)
“And then the anxiety of having to administer an amount of antibiotics you’re not used to dealing with, of using medicines that you have not known even how to dilute for a long time and giving them to elderly patients who are not only suffering from COVID but who also have their base pathologies, many medicines you don’t know how to manage”.(Aurora)
“I felt weaker with a constant need to cry, I was helpless with a feeling that the situation we were going through was chaotic because we didn’t know the extent to which our unconscious and memory would be affected, the after-effects, the “post-traumatic stress” so to speak”.(Jennifer)
3.1.5. Confusion
“It’s an illness where doctors don’t even see you, where they check on you from the door, they show fear when using their stethoscopes on you, everyone is really scared. I think the first few weeks, when everyone was a bit lost, were mostly defined by a sensation of pervading fear, of confusion, as experienced by the workers (we are not really in touch with the doctors) but especially by the nurses, supporting staff such as the cleaning personnel and the nurses... a lot of confusion, fear, they were totally baffled by a situation they had never encountered before”.(Nancy)
“It was totally like being in a movie. Society, the pervading fear, gathering at the balcony every day at eight o’clock to clap for the health workers, everything was a bit... weird”.(Aurora)
3.1.6. Distrust Because of the Uncertainty of Decisions
“They tried treatments that were, well, a bit experimental, to see how people responded to them. You’re scared because doctors you’ve always trusted to cure you, well, you feel like a guinea pig, that they were trying things on you to see how you respond to the treatment”.(Nancy)
“I don’t feel calmed yet, and if my parents do manage to come to Catalonia, which I’m not sure they’ll be able to, because on the one hand the authorities are telling us that we have to keep two meters apart from each other, right? But on the other hand, the planes are crammed with people, they don’t even leave an empty seat between passengers. Well, it seems that certain things are allowed and others... I don’t understand what all this means, but I will only allow my parents to come to see me, I won’t be meeting any friends for a long time, a year maybe, I don’t know, when the situation is a much more under control”.(Bárbara)
“And this, on an internal basis, has brought us a lot of trouble and misunderstandings, because many of our colleagues in gynecology were convinced that it was us, the midwives, who were behind all this, and the truth is that it had nothing to do with us, the women organized themselves and created a network to make it loud and clear that “we don’t want to be part of this””.(Antonia)
“It seemed impossible, even some heads of service had their doubts... we were not sure if it was necessary to cancel so many appointments. And they told us that it was, “yes, everything must be cancelled””.(Nancy)
“[...] Seeing that we were getting sick, not sure how we became infected, not sure if we were properly equipped, because otherwise nothing made sense, you felt fine, but the folks at home were getting sick”.(Jennifer)
3.1.7. Loneliness
“[...] I lived with my husband and he had to go and stay in a hotel room, he had to stay there for a month and a half. If we add to that the fact that I couldn’t see my gynecologist, because all the visits were performed over the phone, that my family was also away ... It required fortitude, personal strength, writing a diary where I could share my emotions was a great help to me”.(Barbara)
“At that moment, the situation required us to act as nurses, midwives, to provide the best care to the people who needed us the most, but, of course, I have also spoken with some of the women... We cannot make the same mistakes again and... I think that I must do something for our women patients, who also had to go through this alone”.(Alice)
3.1.8. Despair, Anger and Impotence
“Hopelessness and rage, because of the uncertainty of not knowing exactly what was going on or of not having...”.(Bárbara)
“[...] COVID has had a great impact on my life, because I work in the health sector, my ex-husband convinced my daughter not to come to my home because I was working at the hospital, and so I spent three months without seeing my daughter”.(Antonia)
“[…] And I think that’s shame it was not allowed, the personals who are in the front line have to be endowed with the greatest team, it makes me very angry”.(Bárbara)
3.2. Professional Occupation and Concern for the Women
3.2.1. Invisibility
“[...] but we felt a bit as if we’d been forgotten, you know? Because the crisis committee would meet on a daily basis and these meetings were reported, you know? I had access to those briefs via the trade union’s WhatsApp group, and well, the delivery room was not even mentioned”.(Antonia)
“A very uncommon situation, because in all those meetings between the hospital management and the department heads, we didn’t take any precautions, we did not respect the safety distance or wear any masks...”.(Nancy)
3.2.2. Changes to Routines and the Economic Crisis
“I think that many workers will be made redundant and will have to take more than one job or come up with a plan if their partner is on a temporary layoff, and you don’t have the expected income. Then, I think that we’ll see a rise in work mobility”.(Aurora)
“[...] And considering our job in primary healthcare, I also think that we’ll resort more to virtual tools, more phone calls, more online group learning, things like that will start to be implemented. As for birth assistance, I don’t think that will change much, the emergency services will be pretty much the same too, as I see it. Had I been working during the pandemic instead of being on a maternity leave, I would been relocated, because the hospital where I worked closed and became an ICU unit”.(Aurora)
“What is more, we also had to deal with the centralization of birth care... the private sector services were transferred to public hospitals, and so we had to deal with more patients, midwives had to face an increasing workload”.(Antonia)
“At our hospital birth-care services were transferred. First, they asked the midwives if they wanted to go, but afterwards, they told us that we had to go, that is, we were not forced to go, but it was clearly a command, you have to go, or they need you there, and...”.(Alice)
“Nurses in general and midwives in particular do their job by the patients’ side, and in the case of pregnant women, midwives stay with them every step of the way, an assistance and accompaniment that in this case must be done via phone call”.(Nancy)
“Telephone visits or video calls, cancelled visits, no childbirth preparation classes, no pap smears, nothing. They only saw pregnant women. They have continued to act as midwives, but the management of resources has changed due to the need to schedule home visits instead having pregnant women come to the hospital... PCRs have also been performed on their birth partners”.(Sara)
3.2.3. Need to Improve the Work/Life Balance
“That’s what I think sometimes that our society has its shortcomings, especially when it comes to creating support networks and resources, so that they help us balance our work and family life, until the kids are three years old”.(Aurora)
“My husband and I are alone here... My mother-in-law wants to come from Colombia to live here and help me with the child, but I don’t know if they will let her come... My parents don’t live here either, I’m not sure it’s safe to leave the baby at the nursery... I will have to find someone to take care of the child at home, but these days it’s not easy”.(Bárbara)
“This is my greatest fear now, I’m worried about who will take of the baby, but there aren’t too many options, because you think “Well, I could leave him at the nursery”, but they don’t know what to tell you either. Of course, it’s not so easy to find a reliable person you can trust to take care of the baby. And leaving him at the nursery is also a risk, because the children also get sick there. If the baby has a fever, they’ll call me and say to me: “Hey, come pick him up”. And what can I do then? And this not just my problem, but... This is what I’m most concerned about now and what keeps me awake at night”.(Aurora)
3.2.4. Concern for the Feelings of Expectant Mothers
“Pregnant women were afraid of us when we visited them at home”.(Maria)
“And then the virus spread, and of course some people who showed symptoms got worse, their condition got more serious and they had to be admitted to the intensive care unit and eventually died, there were people who were admitted to the ICU, there were women who only went to the hospital when their condition was really serious, but others came and were terrified, well, they didn’t know if they were supposed to come... and, well, of course, we’re an emergency service, a very specific emergency service that does not exclude the possibility of our patients being infected with the virus. Many patients were admitted to the hospital in a critical condition as a result of COVID. Everything was a bit chaotic, especially during the first weeks”.(Antonia)
3.2.5. Violation of Rights
“Yes, that was already happening, and all these studies that were being published of how it could affect pregnant women in the 40th week of gestation. But now... the way you tell these women that labor must be induced, the information given to them by their gynecologists, and how their choice is limited, informed decision making... So yes, I believe that the right to choose has not prevailed somehow in these circumstances”.(Elisa)
“In the past you did what the doctor told you to do without even blinking, regardless of the patient’s opinion; now for a time we’ve been working hard to develop a healthcare paradigm where it is the patient who makes her own decisions and who can choose, has the right to know what’s going on with her health at all times, can ask to see her clinical record and can make her own decisions. For what I’ve seen, when facing uncertain situations, we tend to go a bit backwards and bring back the old biomedical and patronizing healthcare practices”.(Nancy)
3.2.6. Safety versus Autonomy—How to Approach the Dilemma?
“I’m in favor of letting women give birth how and where they feel more secure. If a woman gives birth at home, provided that hers is a low-risk pregnancy and that she had made the necessary arrangements with qualified professionals, and also that both she and her partner have tested negative for COVID, I don’t see why there should be any problem with her giving birth at home... but now...”.(Bárbara)
“We’re a group of four midwives that help to deliver babies at home in low-risk pregnancies; during the pandemic we have not been able to do our job because, well, we also work at the hospital and we thought that it might add just another risk factor... We decided we would not take any chances. But we’ve seen an increasing demand for home births, and we’ve transferred these requests to other colleagues who were willing to do it. Many of them have been assisting far more births than usual, and even had to decline in some cases due to the rising demand, but... for us it’s been like this, working at the hospital, it didn’t seem convenient to have us assisting births at home”.(Antonia)
3.2.7. Vulnerability and Obstetric Violence
“All visits were cancelled even for women with high-risk pregnancies”.(Sara)
“We had to work with plastic bags on. We didn’t have protection equipment, even coats were scarce”.(Jane)
“They didn’t give us the first coats and FP2 masks until we were three weeks into the pandemic, that is, until then we didn’t wear any masks as we were supposed to, I was scared”.(Antonia)
“I believe that many births have been delayed and many unnecessary inductions carried out, as many pregnant women have not delivered their babies spontaneously, their births were induced. It was a very stressful situation”.(Antonia)
3.2.8. Dehumanization
“Well, psychologically speaking, I don’t think I can do it, I suffered from anxiety a few years ago, I’ve been better since, but it’s a lot of pressure to take on, I don’t know, maybe I’ll give it a try, but I don’t think so, it’s taken too much of a toll on me to see people all alone, and there was nothing you could do, and they died alone, and, psychologically, I cannot bear it”.(Alice)
“Well, maybe, precisely due to that fear, I didn’t show the empathy the situation required”.(Elisa)
“Screens and protective equipment (with all the effort it had taken just to allow the midwife to be by the women’s side throughout the process...)”.(Jane)
3.3. Resilience and Resistance Strategies
3.3.1. Companionship and Mutual Trust
“Yes, and it was an opportunity to develop teamwork. We had a problem and we had to create circuits; there were three of us on our first watch and we had some time to spare, so we decided to go to the operating theatre and ask: “How are you doing it? How are you dressing up? How do you take your PPE off?”. We created our own circuit and with everybody’s help we generated this whole network of protocols and procedures that were required to do our job optimally”.(Jennifer)
“Personally, I faced the whole situation with a complete trust in the health system, in its professionals, in our capacity to make it through...”.(Nancy)
“As I’d been working closely with my colleagues from the emergency services for many years, we’ve always had a close relationship, and well, now, with all this COVID thing, it got even closer... Because I had so many questions for them, I wanted to know”.(Antonia)
3.3.2. Care in the Present/without any Distractions and a Normalization of the Situation
“Inside the hospital you had to remain focused every step of the way. This is what comes through the door, this is what I’ve got to do, and so this is what I’m doing. Trying to forget about everything else, that helped me a lot. Step by step, this is what I’ve got between my hands, and so this is what I have to figure out. And then, once I got home, I shut the world out, no news, no television”.(Jennifer)
“I think so, the first few days, I was a bit nervous before going to work, but then you get used to it little by little, and then your days off help you to relax and relieve the fatigue and tension”.(Elisa)
3.3.3. Demand for a Restoration of Best Practices
“... I think that with all this situation, with the pandemic, we’ve gone a bit backwards in terms of our healthcare models and treatment practices”.(Nancy)
“I think that in-person visits will be back”.(Sara)
3.3.4. Empowerment and Opportunities
“... and then the renewed strength, you felt very strong because you’d been there, helping people who needed you, and well, when everything was “over” I felt really empowered”.(Alice)
“A group of women got together to vindicate their rights, lodge a complaint to show their disagreement with the fact that birth partners were not allowed into the delivery room”.(Antonia)
“…... I believe that hospitals should be as separated as possible from maternity services”.(Aurora)
“In my opinion, it would be ideal if we could create some low-risk units, run by midwives, or promote home births within the public health system for low-risk pregnancies; we must try to reduce the patient’s stay at the hospital as much as we can. We must encourage them to come only when they’re actually in labor and then check them out of the hospital as quickly as possible”.(Elisa)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levine, M.S.; Lowe, N.K. Measuring Nurse Attitudes about Childbirth: Revision and Pilot Testing of the Nurse Attitudes and Beliefs Questionnaire. J. Nurs. Meas. 2015, 23, 287–301. [Google Scholar] [CrossRef]
- Adams, E.D.; Sauls, D.J. Development of the Intrapartum Nurses’ Beliefs Related to Birth Practice Scale. J. Nurs. Meas. 2014, 22, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Sadeghzadeh, N.; Amiri-Farahani, L.; Haghani, S.; Hasanpoor-Azghady, S.B. Iranian midwives’ attitudes and beliefs toward physiological childbirth: A cross-sectional study. BMC Pregnancy Childbirth 2019, 19, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de Sanidad. Dirección General de Salud Pública, Calidad e Innovación. Centro de Coordinación de Alertas y Emergencias Sanitarias. Enfermedad por Nuevo Coronavirus. Información Inicial de Alerta en China; Ministerio de Sanidad: Madrid, Spain, 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Informacion_inicial_alerta.pdf (accessed on 28 May 2021).
- Ministerio de Sanidad. Ministerio de Derechos Sociales y Agenda. Ministerio de Consumo. Sanidad/ Profesionales/Salud Pública/Centro de Coordinación de Alertas y Emergencias Sanitarias/Alertas en Salud Pública de actualidad/Enfermedad por Nuevo Coronavirus, COVID-19; Ministerio de Sanidad: Madrid, Spain, 2021. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/situacionActual.htm (accessed on 28 May 2021).
- Ministerio de Sanidad. Documento Técnico. Manejo de La Mujer Embarazada y el Recién Nacido con COVID-19; Ministerio de Sanidad: Madrid, Spain, 2020; pp. 1–26. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Documento_manejo_embarazo_recien_nacido.pdf (accessed on 28 May 2021).
- López, M.; Gonce, A.; Meler, E.; Plaza, A.; Hernández, S.; Martínez-Portilla, R.J.; Cobo, T.; García, F.; Gómez-Roig, M.D.; Gratacós, E.; et al. Coronavirus Disease 2019 in Pregnancy: A Clinical Management Protocol and Considerations for Practice. Fetal Diagn. Ther. 2020, 47, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Trapani-Júnior, A.; Rassi-Vanhoni, L.; Koettker-Silveira, S.; Marcolin, A.C. Childbirth, Puerperium and Abortion Care Protocol during the COVID-19 Pandemic. Rev. Bras. Ginecol. Obstet. 2020, 42, 349–355. [Google Scholar] [CrossRef]
- Davis-Floyd, R.; Gutschow, K.; Schwartz, D.A. Pregnancy, Birth and the COVID-19 Pandemic in the United States. Med. Anthropol. 2020, 39, 413–427. [Google Scholar] [CrossRef] [PubMed]
- Costa-Abos, S.; Behaghel, M. Parir en casa en tiempos de Coronavirus. Musas. Rev. Investig. Mujer Salud Soc. 2020, 5, 4–22. [Google Scholar] [CrossRef]
- International Confederation of Midwives. Protecting Midwives to Sustain Care for Women, Newborns and Their Families in the COVID-19 Pandemic; International Confederation of Midwives: The Hague, The Netherlands, 2020; Available online: https://www.internationalmidwives.org/icm-news/joint-call-to-action-protecting-midwives-to-sustain-care-for-women,-newborns-their-families-in-the-covid-19-pandemic.html (accessed on 28 May 2021).
- Shaban, R.Z.; Nahidi, S.; Sotomayor-Castillo, C.; Li, C.; Gilroy, N.; O’Sullivan, M.V.; Sorrell, T.; White, E.; Hackett, K.; Bag, S. SARS-CoV-2 infection and COVID-19: The lived experience and perceptions of patients in isolation and care in an Australian healthcare setting. Am. J. Infect. Control 2020, 48, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Nioi, M.; Napoli, P.E.; Lobina, J.; Fossarello, M.; D’Aloja, E. COVID-19 and Italian healthcare workers from the initial sacrifice to the mRNA vaccine: Pandemic chrono-history, epidemiological data, ethical dilemmas, and future challenges. Front. Public Health 2021, 8, 591900. [Google Scholar] [CrossRef]
- Bender, W.R.; Srinivas, S.; Coutifaris, P.; Acker, A.; Hirshberg, A. The psychological experience of obstetric patients and health care workers after implementation of Universal SARS-CoV-2 testing. Am. J. Perinatol. 2020, 37, 1271–1279. [Google Scholar] [CrossRef]
- Galehdar, N.; Kamran, A.; Toulabi, T.; Heydari, H. Exploring nurses’ experiences of psychological distress during care of patients with COVID-19: A qualitative study. BMC Psychiatry 2020, 20, 489–498. [Google Scholar] [CrossRef]
- González-Timoneda, A.; Hernández, V.H.; Moya, S.P.; Blazquez, R.A. Experiences and attitudes of midwives during the birth of a pregnant woman with COVID-19 infection: A qualitative study. Women Birth 2020, 20, 30379–30386. [Google Scholar] [CrossRef]
- Denzin, N.; Lincoln, Y. El Campo de La Investigación Cualitativa. Manual de Investigación Cualitativa; Gedisa: Barcelona, Spain, 2012; Volume 1. [Google Scholar]
- Fuster, D.E. Investigación Cualitativa: Método Fenomenológico Hermenéutico. Propóstos Represent. 2019, 7, 201–229. [Google Scholar] [CrossRef] [Green Version]
- Erausquin, C.; Sulle, A.; García-Labandal, L. La vivencia como unidad de análisis de la conciencia: Sentidos y significados en trayectorias de profesionalización de psicólogos y profesores en comunidades de práctica. Anu. Investig. 2016, 23, 97–104. Available online: https://www.redalyc.org/pdf/3691/369152696009.pdf (accessed on 27 May 2021).
- Escuriet-Peiró, R.; Goberna-Tricas, J.; Pueyo-Sanchez, M.J.; Garriga-Comas, N.; Úbeda-Bonet, I.; Caja-López, C.; Ortún-Rubio, V. Impact of maternity care policy in Catalonia: A retrospective cross-sectional study of service delivery in public and private hospitals. BMC Pregnancy Childbirth 2015, 15, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conselleria Serveis I Salut Illes Balears. (iB Salut). Available online: https://www.caib.es/seucaib/es/organigrama/273 (accessed on 9 June 2021).
- Ministerio de Sanidad. Secretaria General de Sanidad. Centro de Coordinación de Alertas y Emergencias Sanitarias. ESPAÑA, (2021). Actualización nº 90. Enfermedad por el Coronavirus (COVID-19). Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_90_COVID-19.pdf (accessed on 9 June 2021).
- Trindade, V. Entrevistando en investigación cualitativa y los imprevistos en el trabajo de campo: De la entrevista semiestructurada. In Técnicas y Estrategias en la Investigación Cualitativa; Schettini, P., Cortazzo, I.C., Eds.; Universidad Nacional de la Plata: La Plata, Argentina, 2012; pp. 18–32. [Google Scholar]
- Briscoe, L.; Lavender, T.; McGowan, L. A concept analysis of women’s vulnerability during pregnancy, birth and the postnatal period. J. Adv. Nurs. 2016, 72, 2330–2345. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Calderón, C. Criterios de calidad en la investigación cualitativa en salud (ICS): Apuntes para un debate necesario. Rev. Española Salud Pública 2002, 76, 473–482. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-57272002000500009 (accessed on 27 May 2021). [CrossRef] [Green Version]
- Taylor, S.J.; Bogdan, R. Introducción a Los Métodos Cualitativos de Investigación. La Búsqueda de Significados; Paidos: Barcelona, Spain, 1994. [Google Scholar]
- Shorey, S.; Chan, V. Lessons from past epidemics and pandemics and a way forward for pregnant women, midwives and nurses during COVID-19 and beyond: A meta-synthesis. Midwifery 2020, 90, 102821. [Google Scholar] [CrossRef]
- Aksoy, Y.E.; Koçak, V. Psychological effects of nurses and midwives due to COVID-19 outbreak: The case of Turkey. Arch. Psychiatr. Nurs. 2020, 34, 427–433. [Google Scholar] [CrossRef]
- Bar-Zeev, S.; Breen-Kamkong, C.; Hoope-Bender, P.T.; Sahbani, S.; Abdullah, M. UNFPA supporting midwives at the heart of the COVID-19 response. Women Birth 2021, 34, 4–6. [Google Scholar] [CrossRef]
- Estevan-Reina, L.; Rodríguez-Sánchez, R.M.; Romero-González, B.; Rodríguez-López, A.; Romo-Sola, M. Doble presencia: Un riesgo psicosocial que evidencia la desigualdad entre hombres y mujeres en la conciliación de la vida familiar y laboral. ReiDoCrea 2014, 3, 172–179. [Google Scholar] [CrossRef]
- Cronie, D.; Perdok, H.; Verhoeven, C.; Jans, S.; Hermus, M.; de Vries, R.; Rijnders, M. Are midwives in the Netherlands satisfied with their jobs? A systematic examinations of satisfaction levels among hospital and primary-care midwives in the Netherlands. BMC Health Serv. Res. 2019, 19, 832–841. [Google Scholar] [CrossRef]
- Baumann, S.; Gaucher, L.; Bourgueil, Y.; Saint-Lary, O.; Gautier, S.; Rousseau, A. Adaptation of independent midwives to the COVID-19 pandemic: A national descriptive survey. Midwifery 2021, 94, 102918. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.; Yuri, T.; Pereira, A.C. Dificultades y temores de las enfermeras que enfrentan la pandemia de COVID-19 en Brasil. Humanid. Méd. 2020, 20, 312–333. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1727-81202020000200312 (accessed on 26 May 2021).
- Pallangyo, E.; Nakate, M.G.; Maina, R.; Fleming, V. The impact of COVID-19 on midwives’ practice in Kenya, Uganda and Tanzania: A reflective account. Midwifery 2020, 89, 102775. [Google Scholar] [CrossRef]
- Liu, J.; Cai, Y.; Xu, C.; Zhou, C.; Wei, W.; Yuan, J.; Wang, L.; Kang, L.; Qu, X. Midwifery and Nursing Strategies to protect against COVID-19 during the third trimester of pregnancy. Midwifery 2021, 92, 102876. [Google Scholar] [CrossRef] [PubMed]
- Homer, C.; Davies-Tuck, M.; Dahlen, H.; Scarf, V. The impact of planning for COVID-19 on private practicing midwives in Australia. Women Birth 2021, 34, e32–e37. [Google Scholar] [CrossRef]
- D’aloja, E.; Finco, G.; Demontis, R.; Napoli, P.E.; Fossarello, M.; Nioi, M. COVID-19 and medical liability: Italy denies the shield to its heroes. EClinicalMedicine 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Nioi, M.; Napoli, P.E.; Finco, G.; Demontis, R.; Fossarello, M.; D’aloja, E. Fear of the COVID-19 and medical liability. Insights from a series of 130 consecutives medico-legal claims evaluated in a single institution during SARS-CoV-2-related pandemic. J. Anesth. Intensive Care Emerg. Pain Med. 2021, 17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Name | Age | Area of Work | COVID-19 | Pregnant |
|---|---|---|---|---|
| Bárbara | 30 | Primary Care | No | Yes |
| Aurora | 32 | Hospital Delivery Room | No | Yes |
| Nancy | 50 | Hospital. Delivery Room Coordinator | Yes. Seriously ill. Admitted Hospital | No |
| Alice | 37 | Transferred to COVID ward | No | No |
| Antonia | 42 | Hospital. Delivery Room and Home-birth care | No | No |
| Elisa | 45 | Hospital. Delivery Room | No | No |
| Jennifer | 44 | Hospital. Delivery Room | No | No |
| Jane | 45 | Hospital. Delivery Room Coordinator | No | No |
| Maria | 29 | Providing home-birth care | Yes. Mildly ill. Did not have to be admitted to hospital | No |
| Sara | 35 | Primary Care | No | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goberna-Tricas, J.; Biurrun-Garrido, A.; Perelló-Iñiguez, C.; Rodríguez-Garrido, P. The COVID-19 Pandemic in Spain: Experiences of Midwives on the Healthcare Frontline. Int. J. Environ. Res. Public Health 2021, 18, 6516. https://doi.org/10.3390/ijerph18126516
Goberna-Tricas J, Biurrun-Garrido A, Perelló-Iñiguez C, Rodríguez-Garrido P. The COVID-19 Pandemic in Spain: Experiences of Midwives on the Healthcare Frontline. International Journal of Environmental Research and Public Health. 2021; 18(12):6516. https://doi.org/10.3390/ijerph18126516
Chicago/Turabian StyleGoberna-Tricas, Josefina, Ainoa Biurrun-Garrido, Carme Perelló-Iñiguez, and Pía Rodríguez-Garrido. 2021. "The COVID-19 Pandemic in Spain: Experiences of Midwives on the Healthcare Frontline" International Journal of Environmental Research and Public Health 18, no. 12: 6516. https://doi.org/10.3390/ijerph18126516
APA StyleGoberna-Tricas, J., Biurrun-Garrido, A., Perelló-Iñiguez, C., & Rodríguez-Garrido, P. (2021). The COVID-19 Pandemic in Spain: Experiences of Midwives on the Healthcare Frontline. International Journal of Environmental Research and Public Health, 18(12), 6516. https://doi.org/10.3390/ijerph18126516