
COVID-19 Changed the Incidence and the Pattern of Pediatric Traumas: A Single-Centre Study in a Pediatric Emergency Department


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Time Interval between Trauma and Presentation to the Emergency Department
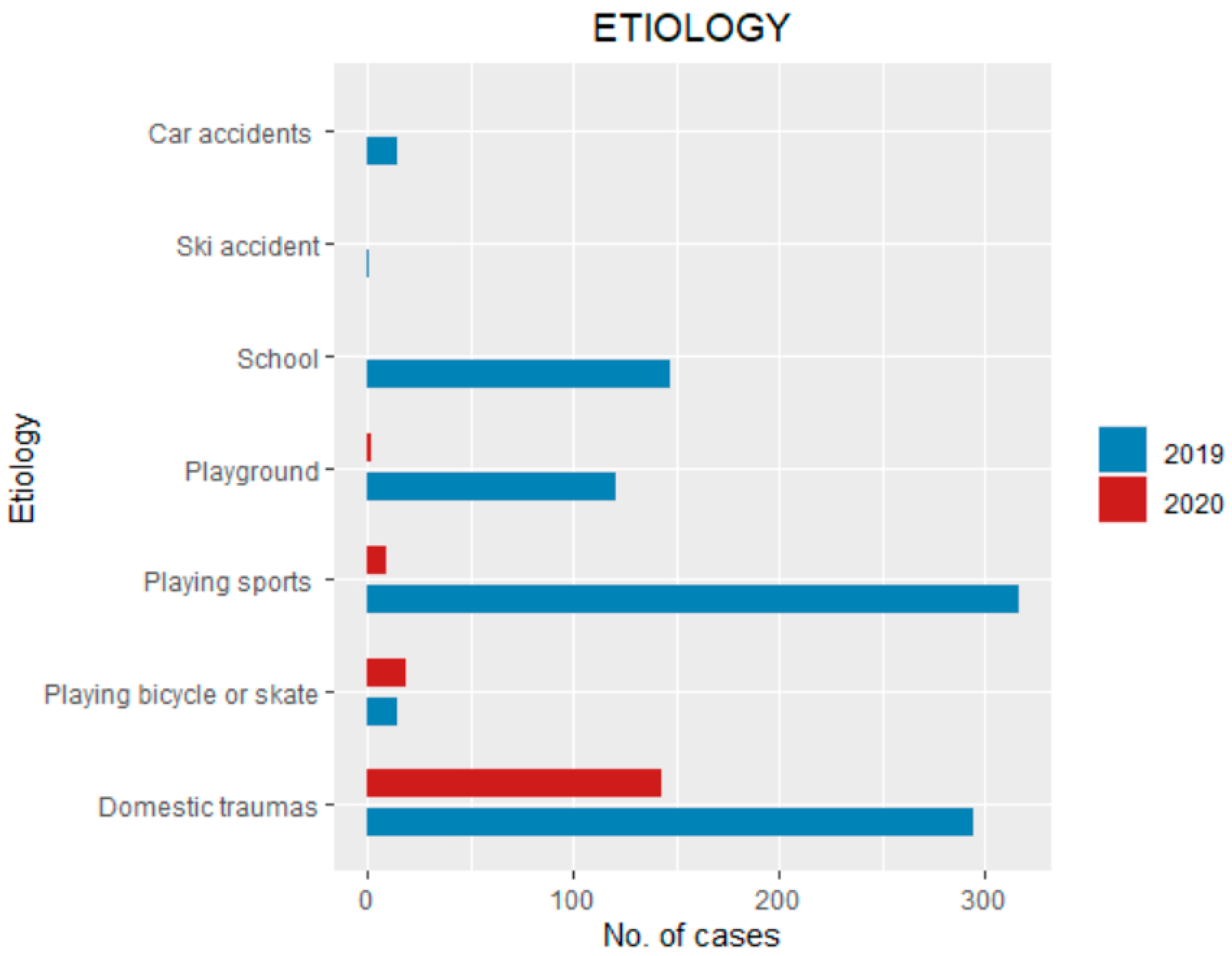
3.3. Etiology of the Trauma
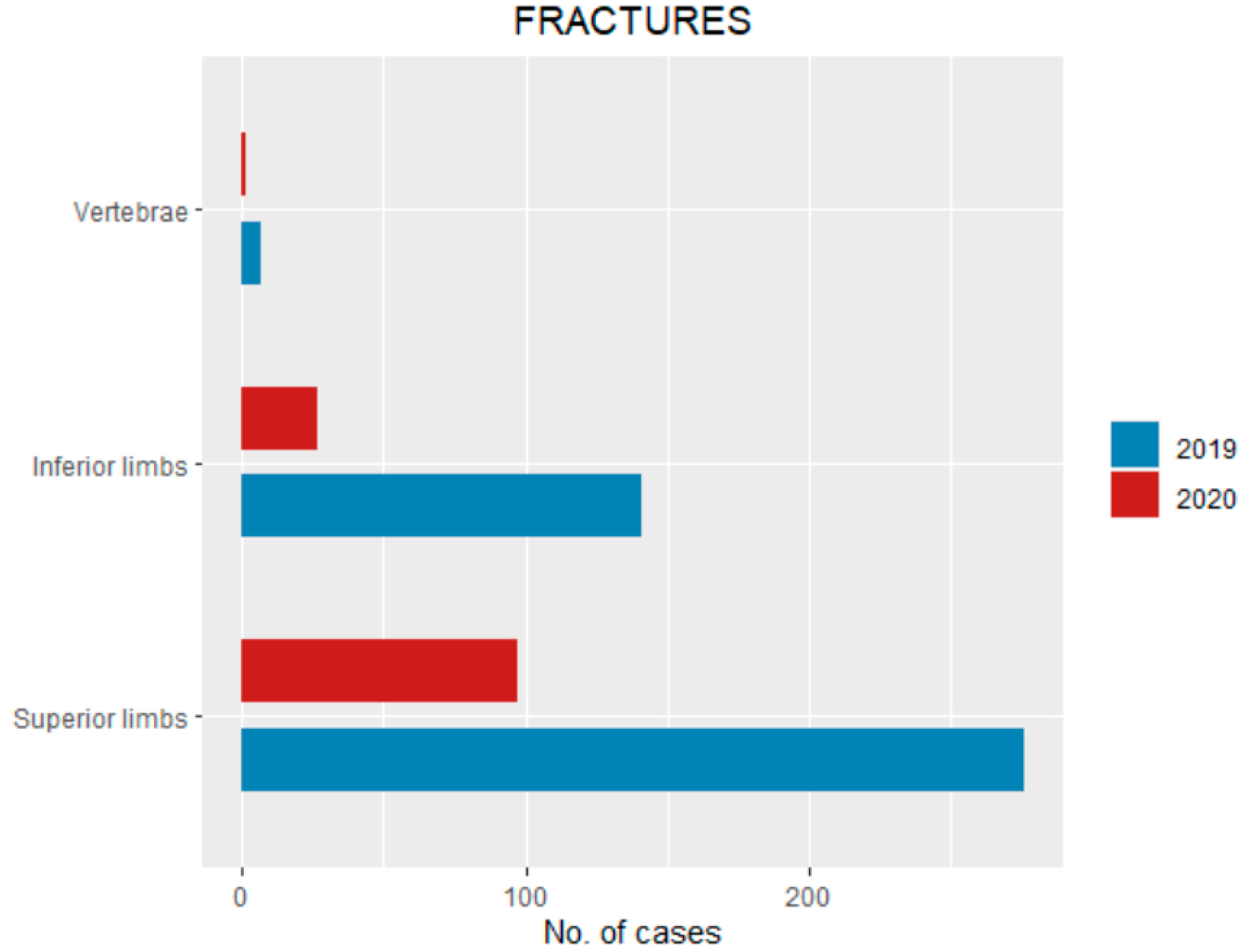
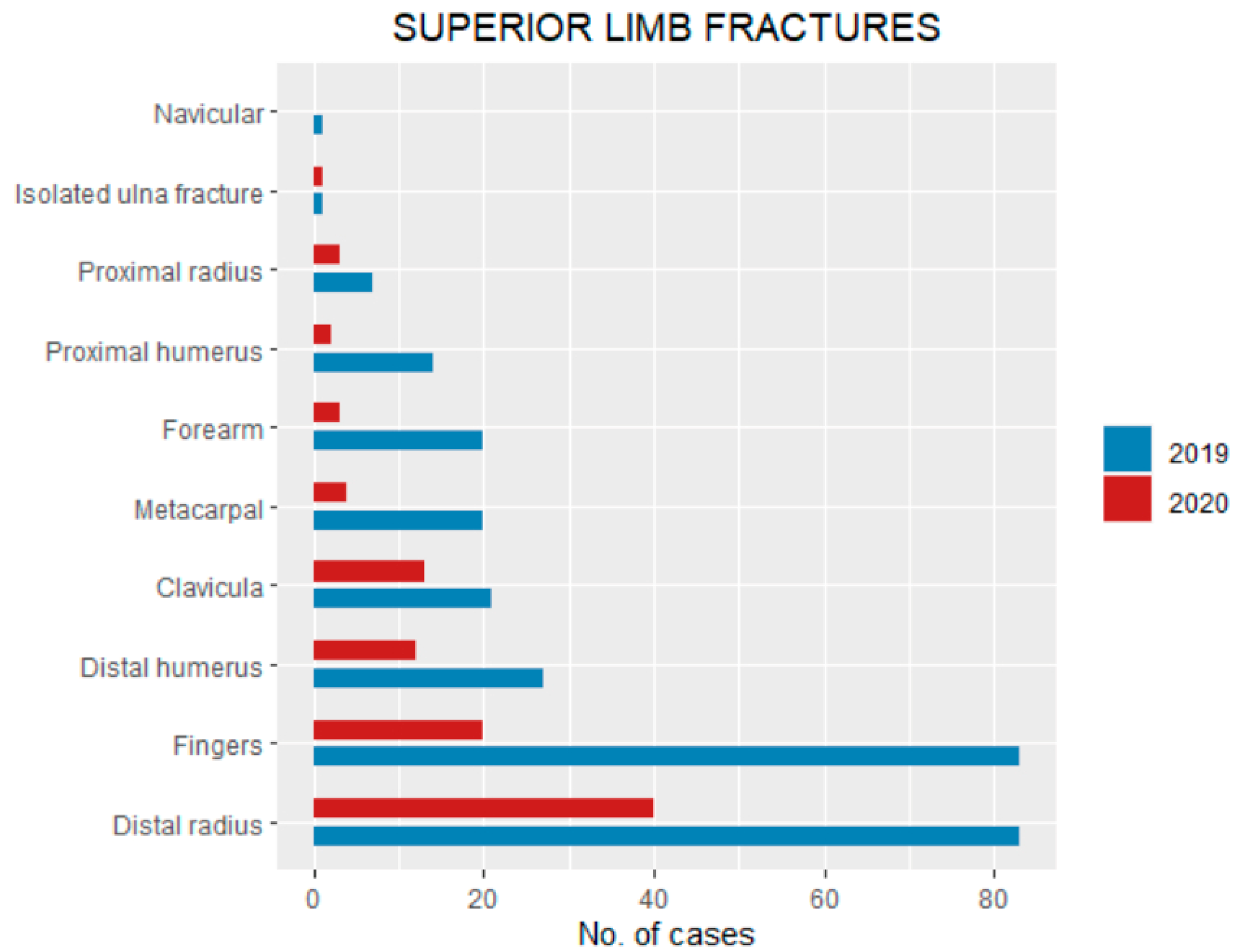
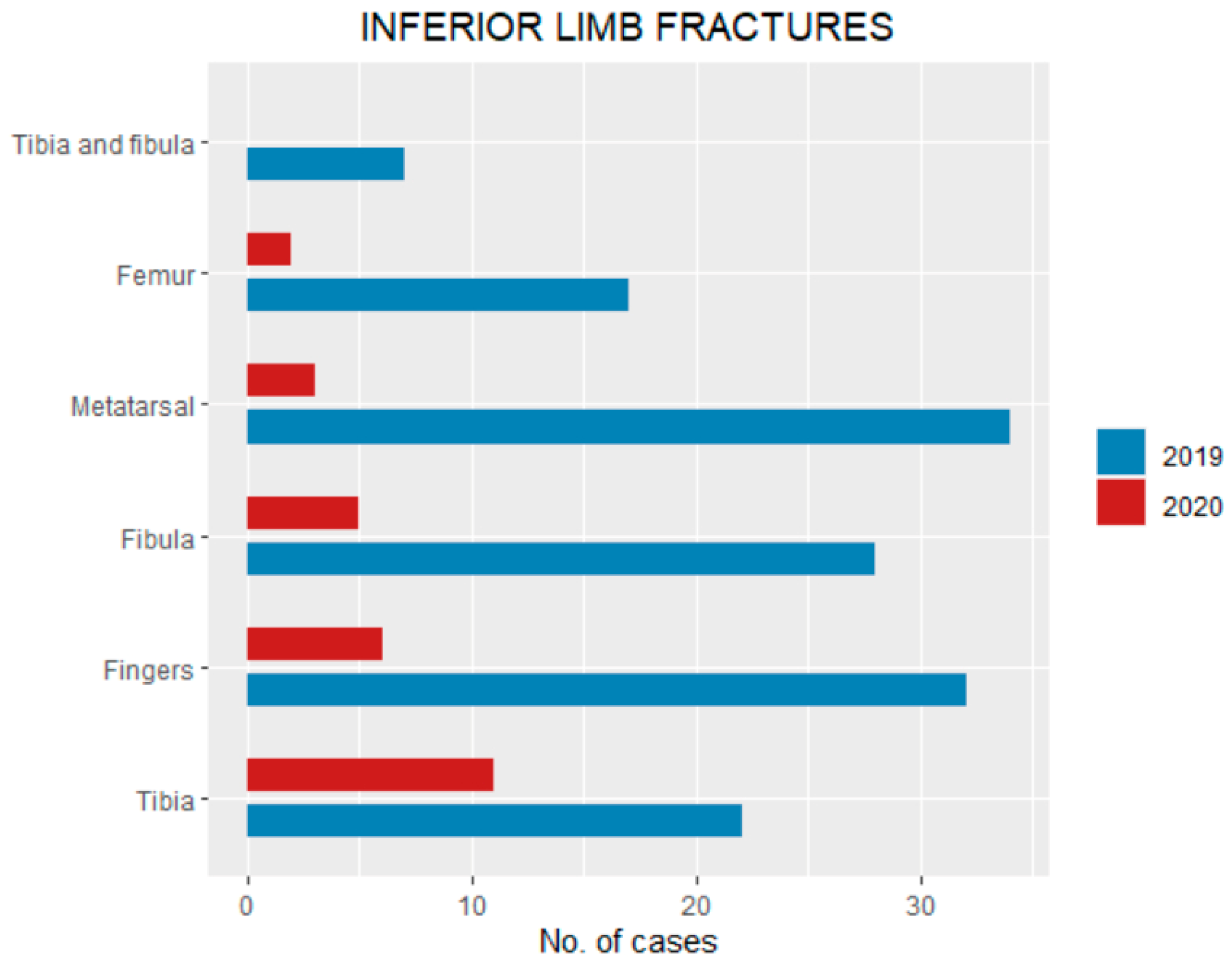
3.4. Fracture Pattern
3.5. Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pelletier, J.H.; Rakkar, J.; Au, A.K.; Fuhrman, D.; Clark, R.S.B.; Horvat, C.M. Trends in US Pediatric Hospital Admissions in 2020 Compared With the Decade Before the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2037227. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Shen, X.; Shao, J.; Ze, R.; Rai, S.; Hong, P.; Tang, X. How to Manage Pediatric Orthopaedic Patients: Strategies to Provide Safer Care During the COVID-19 Outbreak in Wuhan, People’s Republic of China. J. Bone Jt. Surg. Am. 2020, 102, e86. [Google Scholar] [CrossRef]
- Moreland, A.; Herlihy, C.; Tynan, M.A.; Sunshine, G.; McCord, R.F.; Hilton, C.; Poovey, J.; Werner, A.K.; Jones, C.D.; Fulmer, E.B.; et al. Timing of State and Territorial COVID-19 Stay-at-Home Orders and Changes in Population Movement-United States, March 1–May 31, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- VoPham, T.; Weaver, M.D.; Hart, J.E.; Ton, M.; White, E.; Newcomb, P.A. Effect of Social Distancing on COVID-19 Incidence and Mortality in the US. medRxiv 2020. [Google Scholar] [CrossRef]
- Zee-Cheng, J.; McCluskey, C.K.; Klein, M.J.; Scanlon, M.C.; Rotta, A.T.; Shein, S.L.; Pineda, J.A.; Remy, K.E.; Carroll, C.L. Changes in Pediatric Intensive Care Unit Utilization and Clinical Trends during the Coronavirus Pandemic. Chest 2021. [Google Scholar] [CrossRef] [PubMed]
- Heiber, M.; Lou, W.Y.W. Effect of the SARS Outbreak on Visits to a Community Hospital Emergency Department. CJEM 2006, 8, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Khang, Y.H.; Lim, H.K. Impact of the 2015 Middle East Respiratory Syndrome Outbreak on Emergency Care Utilization and Mortality in South Korea. Yonsei Med. J. 2019, 60, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Randelli, P.S.; Compagnoni, R. Management of Orthopaedic and Traumatology Patients during the Coronavirus Disease (COVID-19) Pandemic in Northern Italy. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 1683–1689. [Google Scholar] [CrossRef] [Green Version]
- Gilmartin, S.; Barrett, M.; Bennett, M.; Begley, C.; Chroinin, C.N.; O’Toole, P.; Blackburn, C. The Effect of National Public Health Measures on the Characteristics of Trauma Presentations to a Busy Paediatric Emergency Service in Ireland: A Longitudinal Observational Study. Ir. J. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Isba, R.; Edge, R.; Jenner, R.; Broughton, E.; Francis, N.; Butler, J. Where Have All the Children Gone? Decreases in Paediatric Emergency Department Attendances at the Start of the COVID-19 Pandemic of 2020. Arch. Dis. Child. 2020, 105, 704. [Google Scholar] [CrossRef]
- Christey, G.; Amey, J.; Campbell, A.; Smith, A. Variation in Volumes and Characteristics of Trauma Patients Admitted to a Level One Trauma Centre during National Level 4 Lockdown for COVID-19 in New Zealand. N. Z. Med. J. 2020, 133, 81–88. [Google Scholar] [PubMed]
- Sokoloff, W.C.; Krief, W.I.; Giusto, K.A.; Mohaimin, T.; Murphy-Hockett, C.; Rocker, J.; Williamson, K.A. Pediatric Emergency Department Utilization during the COVID-19 Pandemic in New York City. Am. J. Emerg. Med. 2021, 45, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Sanford, E.L.; Zagory, J.; Blackwell, J.-M.; Szmuk, P.; Ryan, M.; Ambardekar, A. Changes in Pediatric Trauma during COVID-19 Stay-at-Home Epoch at a Tertiary Pediatric Hospital. J. Pediatr. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nuñez, J.H.; Sallent, A.; Lakhani, K.; Guerra-Farfan, E.; Vidal, N.; Ekhtiari, S.; Minguell, J. Impact of the COVID-19 Pandemic on an Emergency Traumatology Service: Experience at a Tertiary Trauma Centre in Spain. Injury 2020, 51, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.J.; Clement, N.D.; Farrow, L.; MacLullich, A.M.J.; Dall, G.F.; Scott, C.E.H.; Jenkins, P.J.; White, T.O.; Duckworth, A.D. IMPACT-Scot Study Group IMPACT-Scot Report on COVID-19 and Hip Fractures. Bone Jt. J. 2020, 102, 1219–1228. [Google Scholar] [CrossRef]
- Pichard, R.; Kopel, L.; Lejeune, Q.; Masmoudi, R.; Masmejean, E.H. Impact of the COronaVIrus Disease 2019 Lockdown on Hand and Upper Limb Emergencies: Experience of a Referred University Trauma Hand Centre in Paris, France. Int. Orthop. 2020, 44, 1497–1501. [Google Scholar] [CrossRef]
- Baxter, I.; Hancock, G.; Clark, M.; Hampton, M.; Fishlock, A.; Widnall, J.; Flowers, M.; Evans, O. Paediatric Orthopaedics in Lockdown: A Study on the Effect of the SARS-Cov-2 Pandemic on Acute Paediatric Orthopaedics and Trauma. Bone Jt. Open 2020, 1, 424–430. [Google Scholar] [CrossRef]
- Bram, J.T.; Johnson, M.A.; Magee, L.C.; Mehta, N.N.; Fazal, F.Z.; Baldwin, K.D.; Riley, J.; Shah, A.S. Where Have All the Fractures Gone? The Epidemiology of Pediatric Fractures During the COVID-19 Pandemic. J. Pediatr. Orthop. 2020, 40, 373–379. [Google Scholar] [CrossRef]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed Access or Provision of Care in Italy Resulting from Fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Zhu, Y.; Chen, W.; Xin, X.; Yin, Y.; Hu, J.; Lv, H.; Li, W.; Deng, X.; Zhu, C.; Zhu, J.; et al. Epidemiologic Characteristics of Traumatic Fractures in Elderly Patients during the Outbreak of Coronavirus Disease 2019 in China. Int. Orthop. 2020, 1–6. [Google Scholar] [CrossRef]
- Gumina, S.; Proietti, R.; Villani, C.; Carbone, S.; Candela, V. The Impact of COVID-19 on Shoulder and Elbow Trauma in a Skeletally Immature Population: An Italian Survey. JSES Int. 2020. [Google Scholar] [CrossRef]
- Amer, K.M.; Congiusta, D.V.; Suri, P.; Choudhry, A.; Otero, K.; Adams, M. Clavicle Fractures: Associated Trauma and Morbidity. J. Clin. Orthop. Trauma 2021, 13, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Tolone, S.; Gambardella, C.; Brusciano, L.; Del Genio, G.; Lucido, F.S.; Docimo, L. Telephonic Triage before Surgical Ward Admission and Telemedicine during COVID-19 Outbreak in Italy. Effective and Easy Procedures to Reduce in-Hospital Positivity. Int. J. Surg. 2020, 78, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Sherman, W.F.; Khadra, H.S.; Kale, N.N.; Wu, V.J.; Gladden, P.B.; Lee, O.C. How Did the Number and Type of Injuries in Patients Presenting to a Regional Level I Trauma Center Change During the COVID-19 Pandemic with a Stay-at-Home Order? Clin. Orthop. Relat. Res. 2021, 479, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Qasim, Z.; Sjoholm, L.O.; Volgraf, J.; Sailes, S.; Nance, M.L.; Perks, D.H.; Grewal, H.; Meyer, L.K.; Walker, J.; Koenig, G.J.; et al. Trauma Center Activity and Surge Response during the Early Phase of the COVID-19 Pandemic-the Philadelphia Story. J. Trauma Acute Care Surg. 2020, 89, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, M.R.; Grigorian, A.; Inaba, K.; Kuza, C.M.; Kim, D.; Dolich, M.; Lekawa, M.; Nahmias, J. A Dual Pandemic: The Influence of Coronavirus Disease 2019 on Trends and Types of Firearm Violence in California, Ohio, and the United States. J. Surg. Res. 2021, 263, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Ghafil, C.; Matsushima, K.; Ding, L.; Henry, R.; Inaba, K. Trends in Trauma Admissions During the COVID-19 Pandemic in Los Angeles County, California. JAMA Netw. Open 2021, 4, e211320. [Google Scholar] [CrossRef]
- Sidpra, J.; Abomeli, D.; Hameed, B.; Baker, J.; Mankad, K. Rise in the Incidence of Abusive Head Trauma during the COVID-19 Pandemic. Arch. Dis. Child. 2021, 106, e14. [Google Scholar] [CrossRef]
- Rougereau, G.; Guedj, R.; Irtan, S.; Qassemyar, Q.; Vialle, R.; Langlais, T. Emergency Department Visits for Pediatric Traumatic Injuries during General Confinement: A Single-Center Study in an Urban Setting. Arch. Pediatr. 2021. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2019 | 2020 | ||
|---|---|---|---|
| Traumas | 909 | 173 | p < 0.001 |
| M/F | 512/397 | 102/71 | p > 0.05 |
| Age | 9.1 ± 4.04 (0–18) | 8.3 ± 5.8 (0–16) | p < 0.05 |
| Fractures | 424 | 125 | p < 0.001 |
| Sprain/Blunt Traumas | 448 | 36 | p < 0.001 |
| Pulled Elbow | 34 | 12 | p > 0.05 |
| Dislocations | 5 | 0 | p > 0.05 |
| Hospitalized | 19 | 10 | p < 0.001 |
| Outpatient | 890 | 163 | p > 0.05 |
| Surgery | 16 | 9 | p < 0.001 |
| Fracture Involved | Bones Involved | 2019 | 2020 | |
|---|---|---|---|---|
| Superior limbs | 276 | 97 | p < 0.05 | |
| Distal radius | 83 | 40 | p < 0.05 | |
| Fingers | 83 | 20 | p > 0.05 | |
| Clavicula | 21 | 13 | p > 0.05 | |
| Distal humerus | 27 | 12 | p > 0.05 | |
| Metacarpal | 20 | 4 | p > 0.05 | |
| Forearm | 20 | 3 | p > 0.05 | |
| Proximal radius | 7 | 3 | p > 0.05 | |
| Proximal humerus | 10 | 1 | p > 0.05 | |
| Isolated ulna fracture | 4 | 1 | p > 0.05 | |
| Navicular | 1 | 0 | p > 0.05 | |
| Inferior limbs | 141 | 27 | p < 0.05 | |
| Tibia | 22 | 11 | p < 0.05 | |
| Fingers | 32 | 6 | p > 0.05 | |
| Fibula | 28 | 5 | p > 0.05 | |
| Metatarsal | 34 | 3 | p > 0.05 | |
| Femur | 18 | 2 | p > 0.05 | |
| Tibia and fibula | 7 | 0 | p > 0.05 | |
| Vertebrae | 7 | 1 | p > 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruzzini, L.; De Salvatore, S.; Lamberti, D.; Maglione, P.; Piergentili, I.; Crea, F.; Ossella, C.; Costici, P.F. COVID-19 Changed the Incidence and the Pattern of Pediatric Traumas: A Single-Centre Study in a Pediatric Emergency Department. Int. J. Environ. Res. Public Health 2021, 18, 6573. https://doi.org/10.3390/ijerph18126573
Ruzzini L, De Salvatore S, Lamberti D, Maglione P, Piergentili I, Crea F, Ossella C, Costici PF. COVID-19 Changed the Incidence and the Pattern of Pediatric Traumas: A Single-Centre Study in a Pediatric Emergency Department. International Journal of Environmental Research and Public Health. 2021; 18(12):6573. https://doi.org/10.3390/ijerph18126573
Chicago/Turabian StyleRuzzini, Laura, Sergio De Salvatore, Daniela Lamberti, Pierluigi Maglione, Ilaria Piergentili, Francesca Crea, Chiara Ossella, and Pier Francesco Costici. 2021. "COVID-19 Changed the Incidence and the Pattern of Pediatric Traumas: A Single-Centre Study in a Pediatric Emergency Department" International Journal of Environmental Research and Public Health 18, no. 12: 6573. https://doi.org/10.3390/ijerph18126573
APA StyleRuzzini, L., De Salvatore, S., Lamberti, D., Maglione, P., Piergentili, I., Crea, F., Ossella, C., & Costici, P. F. (2021). COVID-19 Changed the Incidence and the Pattern of Pediatric Traumas: A Single-Centre Study in a Pediatric Emergency Department. International Journal of Environmental Research and Public Health, 18(12), 6573. https://doi.org/10.3390/ijerph18126573