
Influence of Psychological Distress in Patients with Hypoallergenic Total Knee Arthroplasty. Treatment Algorithm for Patients with Metal Allergy and Knee Osteoarthritis




Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Patients
2.3. Covers Variables and Data Collection
2.4. Questionnaires
2.5. Statistical Analysis
3. Results
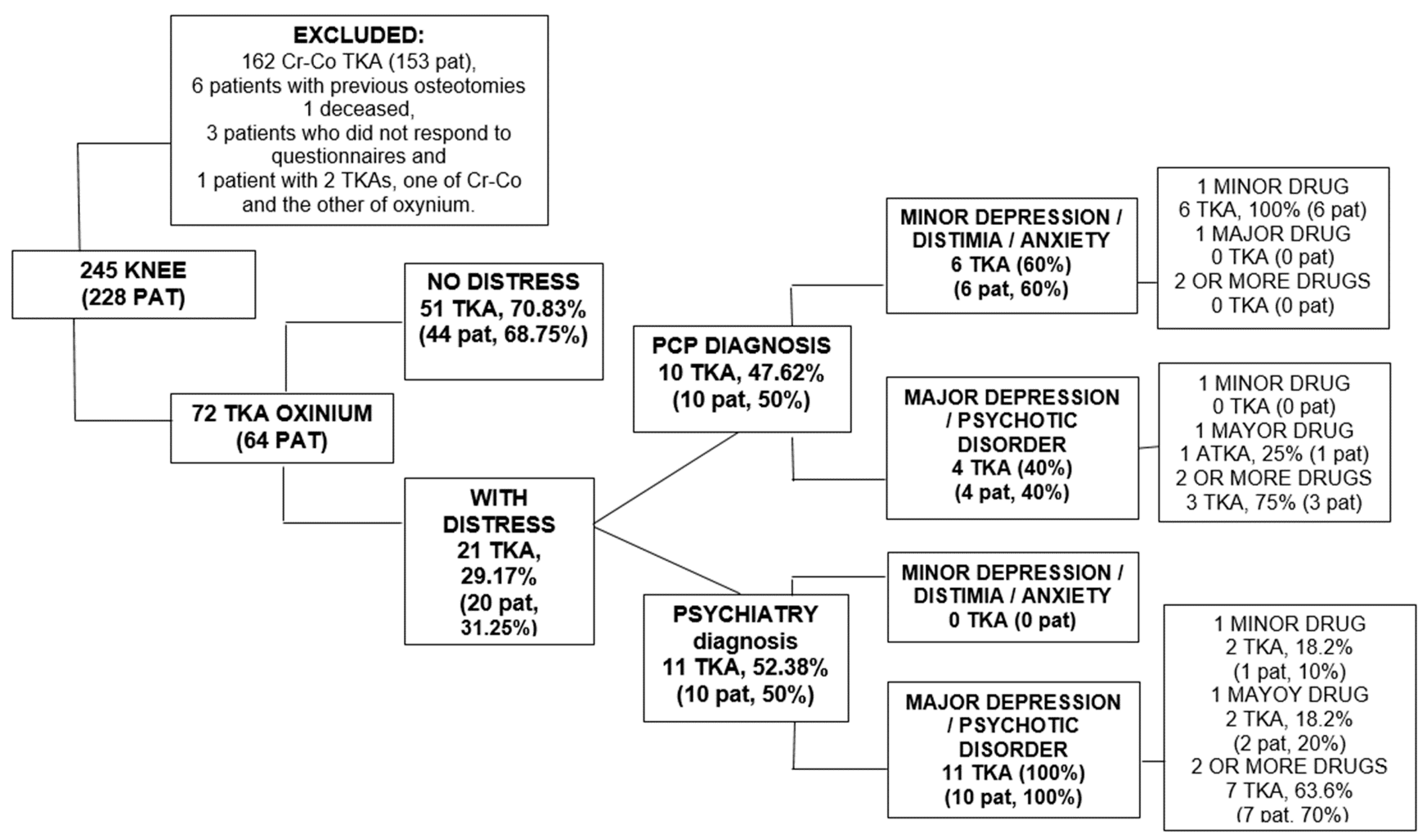
3.1. Cohort
3.2. Psychological Distress in Patients with Hypoallergenic TKA
3.3. Results of the Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TKA | total knee arthroplasty |
| OA | osteoarthritis |
| MA | metal allergy |
| N | nickel |
| Cr-Co | chromium–cobalt |
| MSH | Metal skin hypersensitivity |
| PD | psychological distress |
| Pre-PD | preoperative Psychological Distress |
| BMI | body mass index |
| SPT | skin patch test |
| PS TKA | posterior-stabilized |
| WOMAC | Western Ontario McMaster Universities Osteoarthritis Index |
| SF-12 | questionnaire Short Form 12 questionnaire |
| Euro-Qol-5D L-VAS | The EQ-5D-5L questionnaire essentially consists of two pages: the EQ-5D descriptive system and the EQ visual analogue scale (EQ VAS). |
| PCP | primary care physician |
| PHQ-15 | questionnaires Patient Health Questionnaire Spanish version |
| SD | standard deviation |
References
- Benz, T.; Angst, F.; Lehmann, S.; Aeschlimann, A. Association of the sense of coherence with physical and psychosocial health in the rehabilitation of osteoarthritis of the hip and knee: A prospective cohort study. BMC Musculoskelet. Disord. 2013, 14, 159. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Prieto, D.; Gil-González, S.; Pelfort, X.; Leal-Blanquet, J.; Puig-Verdié, L.; Hinarejos, P. Influence of Depression on Total Knee Arthroplasty Outcomes. J. Arthroplast. 2014, 29, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Cuevas-Castillejos, H.; Cuevas-Castillejos, J.E. Alergia e hipersensibilidad: Conceptos básicos para el pediatra. Rev. Mex. Pediatr. 2012, 79, 192–200. [Google Scholar]
- Ibarra, B.; García-García, J.; Azuara, G.; Vázquez-Lasa, B.; Ortega, M.A.; Asúnsolo, Á.; San Román, J.; Buján, J.; García-Honduvilla, N.; De la Torre, B. Polylactic-co-glycolic acid microspheres added to fixative cements and its role on bone infected architecture. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 2517–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feeley, B.T. Management of osteoarthritis of the knee in the active patient. J. Am. Acad. Orthop. Surg. 2010, 18, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Azuara, G.; García-García, J.; Ibarra, B.; Parra-Ruiz, F.J.; Asúnsolo, A.; Ortega, M.A.; Vázquez-Lasa, B.; Buján, J.; San Román, J.; de la Torre, B. Experimental study of the application of a new bone cement loaded with broad spectrum antibiotics for the treatment of bone infection. Rev. Esp. Cir. Ortop. Traumatol. 2019, 63, 95–103. [Google Scholar] [CrossRef]
- Moskowitz, R. Osteoarthritis: Diagnosis and Medical and Surgical Management, 3rd ed.; Saunders: Philadelphia, PA, USA, 2001. [Google Scholar]
- Parvizi, J.; Gehrke, T. International consensus on periprosthetic joint infection: Let cumulative wisdom be a guide. J. Bone Jt. Surg. Am. Vol. 2014, 96, 441–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogel, M.; Riediger, C.; Krippl, M.; Frommer, J.; Lohmann, C.; Illiger, S. Negative affect, type D personality, quality of life, and dysfunctional outcomes of total knee arthroplasty. Pain Res. Manag. 2019, 2019, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granchi, D.; Cenni, E.; Tigani, D.; Trisolino, G.; Baldini, N.; Giunti, A. Sensitivity to implant materials in patients with total knee arthroplasties. Biomaterials 2008, 29, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Post, Z.D.; Orozco, F.R.; Ong, A.C. Metal sensitivity after TKA presenting with systemic dermatitis and hair loss. Orthopedics 2013, 36, e525. [Google Scholar] [CrossRef] [Green Version]
- Bircher, A.; Friederich, N.F.; Seelig, W.; Scherer, K. Allergic complications from orthopaedic joint implants: The role of delayed hypersensitivity to benzoyl peroxide in bone-cement. Contact Dermat. 2012, 66, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.; Merritt, K.; Jacobs, J.J. Metal sensitivity in patients with orthopaedic implants. J. Bone Jt. Surg. Am. Vol. 2001, 83, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Willert, H.G.; Buchhorn, G.H.; Fayyazi, A.; Flury, R.; Windler, M.; Köster, G.; Lohmann, C.H. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints. A clinical and histomorphological study. J. Bone Jt. Surg. Am. Vol. 2005, 87, 28–36. [Google Scholar] [CrossRef]
- Innocenti, M.; Carulli, C.; Matassi, F.; Carossino, A.M.; Brandi, M.L.; Civinini, R. Total knee arthroplasty in patients with hypersensitivity to metals. Int. Orthop. 2014, 38, 329–333. [Google Scholar] [CrossRef] [Green Version]
- Lützner, J.; Hartmann, A.; Dinnebier, G.; Spornraft-Ragaller, P.; Hamann, C.; Kirschner, S. Metal hypersensitivity and metal ion levels in patients with coated or uncoated total knee arthroplasty: A randomised controlled study. Int. Orthop. 2013, 37, 1925–1931. [Google Scholar] [CrossRef] [Green Version]
- Peña, P.; Ortega, M.A.; Buján, J.; De la Torre, B. Decrease of Quality of Life, Functional Assessment and Associated Psychological Distress in Patients with Hypoallergenic Total Knee Arthroplasty. J. Clin. Med. 2020, 9, 3270. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Dong, J.Y. Patient’s personality predicts recovery after total knee arthroplasty: A retrospective study. J. Orthop. Sci. 2014, 19, 263–269. [Google Scholar] [CrossRef]
- Utrillas-Compaired, A.; De La Torre-Escuredo, B.J.; Tebar-Martínez, A.J.; Barco Ángel, A.-D. Does preoperative psychologic distress influence pain, function, and quality of life after TKA? Clin. Orthop. Relat. Res. 2014, 472, 2457–2465. [Google Scholar] [CrossRef] [Green Version]
- Papakostidou, I.; Dailiana, Z.; Papapolychroniou, T.; Liaropoulos, L.; Zintzaras, E.; Karachalios, T.; Malizos, K.N. Factors affecting the quality of life after total knee arthroplasties: A prospective study. BMC Musculoskelet. Disord. 2012, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bourne, R.B. Measuring tools for functional outcomes in total knee arthroplasty. Clin. Orthop. Relat. Res. 2008, 466, 2634–2638. [Google Scholar] [CrossRef] [Green Version]
- Lavernia, C.J.; Villa, J.M.; Iacobelli, D.A. What is the role of mental health in primary total knee arthroplasty? Clin. Orthop. Relat. Res. 2015, 473, 159–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolfson, O.; Eresian, C.K.; Franklin, P.; Bohm, E.; Lübbeke, A.; Denissen, G.; Dunn, J.; Chenok, K.E.; Dunbar, M.; Overgaard, S.; et al. Patient-reported outcome measures in arthroplasty registries report of the patient-reported outcome measures working group of the inter- national society of arthroplasty registries part, I. overview and rationale for patient-reported outcome measures. Acta Orthop. 2016, 87, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz Ortiz, J. Value and quantification of quality of life in medicine. Med. Clin. 1991, 96, 66–69. [Google Scholar]
- Goh, G.S.; Liow, M.H.; Bin Abd Razak, H.R.; Tay, D.K.; Lo, N.N.; Yeo, S.J. Patient-reported outcomes, quality of life, and satisfaction rates in young patients aged 50 years or younger after total knee arthroplasty. J. Arthroplast. 2017, 32, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Faschingbauer, M.; Renner, L.; Boettner, F. Allergy in total knee replacement. does it exist?: Review article. HSS J. 2017, 13, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Benson, T.; Williams, D.H.; Potts, H.W. Performance of EQ-5D, howRu and Oxford hip & knee scores in assessing the outcome of hip and knee replacements. BMC Health Serv. Res. 2016, 16, 512–519. [Google Scholar]
- Conner-Spady, B.L.; Marshall, D.A.; Bohm, E.; Dunbar, M.J.; Loucks, L.; Al Khudairy, A.; Noseworthy, T.W. Reliability and validity of the EQ-5D-5L compared to the EQ-5D-3L in patients with osteoarthritis referred for hip and knee replacement. Qual. Life Res. 2015, 24, 1775–1784. [Google Scholar] [CrossRef]
- Mell, S.P.; Wimmer, M.A.; Lundberg, H.J. Sensitivity of total knee replacement wear to variability in motion and load input: A parametric finite element analysis study. J. Orthop. Res. 2020, 38, 1538–1549. [Google Scholar] [CrossRef]
- Gallo, J.; Goodman, S.B.; Konttinen, Y.T.; Wimmer, M.A.; Holinka, M. Osteolysis around total knee arthroplasty: A review of pathogenetic mechanisms. Acta Biomater. 2013, 9, 8046–8058. [Google Scholar] [CrossRef] [Green Version]
- Namba, R.S.; Cafri, G.; Khatod, M.; Inacio, M.C.; Brox, T.W.; Paxton, E.W. Risk factors for total knee arthroplasty aseptic revision. J. Arthroplast. 2013, 28, 122. [Google Scholar] [CrossRef]
- Bravo, D.; Wagner, E.R.; Larson, D.R.; Davis, M.P.; Pagnano, M.W.; Sierra, R.J. No Increased Risk of Knee Arthroplasty Failure in Patients with Positive Skin Patch Testing for Metal Hypersensitivity: A Matched Cohort Study. J. Arthroplast. 2016, 31, 1717–1721. [Google Scholar] [CrossRef] [PubMed]
- Thakur, R.R.; Ast, M.P.; McGraw, M.; Bostrom, M.P.; Rodriguez, J.A.; Parks, M.L. Severe persistent synovitis after cobalt- chromium total knee arthroplasty requiring revision. Orthopedics 2013, 36, e520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schalock, P.C.; Crawford, G.; Nedorost, S.; Scheinman, P.L.; Atwater, A.R.; Mowad, C.; Brod, B.; Ehrlich, A.; Watsky, K.L.; Sasseville, D.; et al. Patch Testing for Evaluation of Hypersensitivity to Implanted Metal Devices: A Perspective From the American Contact Dermatitis Society. Dermatitis 2016, 27, 241–247. [Google Scholar] [CrossRef]
- Ziemssen, T.; Kerrn, S. Psychoneuro-immunology-cross-talk between the immune and nervous systems. J. Neurol. 2007, 254 (Suppl. S2), 8–11. [Google Scholar] [CrossRef]
- Priyadarshini, S.; Aich, P. Effects of psychological stress on innate Immunity and metabolism in humans: A systematic Analysis. PLoS ONE 2012, 7, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.; Dai, X.; Li, L.; Chen, Z.; Cui, H.; Lv, S. Patellar resurfacing versus nonresurfacing in total knee arthroplasty: An updated meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2021, 16, 83. [Google Scholar] [CrossRef] [PubMed]
- Grassi, A.; Compagnoni, R.; Ferrua, P.; Zaffagnini, S.; Berruto, M.; Samuelsson, K.; Svantesson, E.; Randelli, P. Patellar resurfacing versus patellar retention in primary total knee arthroplasty: A systematic review of overlapping meta-analyses. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3206–3218. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Psychological Distress Psychiatric History |
|---|
| 0: no diagnosis of psychiatric pathology |
| 1: diagnosis by family doctor |
| 2: diagnosis by the Psychiatry Service |
| Type Psychiatric Pathology |
| 0: no pathology |
| 1: minor depression or dysthymia or anxiety |
| 2: major depression or psychotic disorder |
| No. and type of drugs administered to the patient |
| 0: no medication |
| 1: take a minor drug |
| 2: take a major drug |
| 3: take two or more drugs |
| Final score |
| 1: 3 points, mild psychiatric pathology |
| 2: 4–5 points, moderate psychiatric pathology |
| 3: 6–7 points, severe psychiatric pathology |
| TKA Hypoallergenic n = 72 | |
|---|---|
| Average age (years) | 72.30 ± 6.03 |
| Women, n (%) | 70 (92.1) |
| BMI (kg/m2) | 32.12 ± 5.08 |
| Weight, n (%) | |
| Normo-weight | 3 (3.9) |
| Overweight | 24 (31.6) |
| Obesity | 49 (64.5) |
| Time after intervention (months) | 27.49 ±8.666 |
| Patellar component, n (%) | 11 (18) |
| Laterality | |
| Right | 36 (50) |
| Left | 23 (38.9) |
| Both | 8 (11.1) |
| Psychiatric history, n (%) | 21 (29.17) |
| Associated complications, n (%) | 12 (15.8) |
| WOMAC | |
| Total | 28.37 ± 20.66 |
| Pain | 5.27 ± 5.29 |
| Rigidity | 1.41 ± 2.10 |
| Difficulty | 22.34 ± 14.62 |
| SF-12 | |
| Physical | 27.28 ± 10.58 |
| Mental | 44.86 ± 11.37 |
| EuroQoL-5D | |
| Index | 0.65 ± 0.32 |
| VAS | 53.86 ± 34.94 |
| Psychological Distress Score | ||||
|---|---|---|---|---|
| Psychological Distress | 3 Points, Mild | 4–5 Points, Moderate | 6–7 Points, Severe | Total |
| N patients (knee) (% pat) | 6 (6) [30] | 2 (3) [10] | 12 (12) [60] | 20 (21) [100] |
| PD | TKA Hypoallergenic | |||
|---|---|---|---|---|
| Mean | SD | p | ||
| WOMAC Total | Yes | 41.76 | 23.212 | 0.000 |
| No | 23.25 | 17.229 | ||
| SF Physical | Yes | 25.269 | 10.048 | 0.015 |
| No | 32.804 | 10.058 | ||
| SF Mental | Yes | 37.568 | 12.665 | 0.017 |
| No | 42.527 | 9.819 | ||
| EQ Index | Yes | 0.84 | 0.25 | 0.019 |
| No | 0.71 | 0.28 | ||
| EQ VAS | Yes | 35.14 | 33.600 | 0.013 |
| No | 61.00 | 33.004 | ||
| Diagnosis PD | PD and TKA Hypoallergenic | |||
|---|---|---|---|---|
| Mean | SD | p | ||
| WOMAC Total | PCP | 40.03 | 20.72 | 0.046 |
| Psychiatry | 30.24 | 15.275 | ||
| SF Physical | PCP | 27.875 | 9.781 | 0.039 |
| Psychiatry | 32.432 | 10.984 | ||
| SF Mental | PCP | 40.937 | 10.735 | 0.057 |
| Psychiatry | 38.652 | 9.54 | ||
| EQ Index | PCP | 0.89 | 0.23 | 0.028 |
| Psychiatry | 0.81 | 0.25 | ||
| EQ VAS | PCP | 36.04 | 30.93 | 0.05 |
| Psychiatry | 40.32 | 29.07 | ||
| Type of DS Diagnosis | PD and TKA Hypoallergenic | |||
|---|---|---|---|---|
| Mean | SD | p | ||
| WOMAC Total | Minor depression | 41.32 | 19.793 | 0.039 |
| Major depression | 31.26 | 16.865 | ||
| SF Physical | Minor depression | 26.114 | 9.546 | 0.056 |
| Major depression | 29.984 | 10.433 | ||
| SF Mental | Minor depression | 36.67 | 9.98 | 0.057 |
| Major depression | 40.154 | 9.17 | ||
| EQ Index | Minor depression | 0.88 | 0.26 | 0.04 |
| Major depression | 0.83 | 0.23 | ||
| EQ VAS | Minor depression | 35.64 | 28.76 | 0.048 |
| Major depression | 41.23 | 28.47 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña, P.; Ortega, M.A.; Buján, J.; De la Torre, B. Influence of Psychological Distress in Patients with Hypoallergenic Total Knee Arthroplasty. Treatment Algorithm for Patients with Metal Allergy and Knee Osteoarthritis. Int. J. Environ. Res. Public Health 2021, 18, 5997. https://doi.org/10.3390/ijerph18115997
Peña P, Ortega MA, Buján J, De la Torre B. Influence of Psychological Distress in Patients with Hypoallergenic Total Knee Arthroplasty. Treatment Algorithm for Patients with Metal Allergy and Knee Osteoarthritis. International Journal of Environmental Research and Public Health. 2021; 18(11):5997. https://doi.org/10.3390/ijerph18115997
Chicago/Turabian StylePeña, Pilar, Miguel A. Ortega, Julia Buján, and Basilio De la Torre. 2021. "Influence of Psychological Distress in Patients with Hypoallergenic Total Knee Arthroplasty. Treatment Algorithm for Patients with Metal Allergy and Knee Osteoarthritis" International Journal of Environmental Research and Public Health 18, no. 11: 5997. https://doi.org/10.3390/ijerph18115997
APA StylePeña, P., Ortega, M. A., Buján, J., & De la Torre, B. (2021). Influence of Psychological Distress in Patients with Hypoallergenic Total Knee Arthroplasty. Treatment Algorithm for Patients with Metal Allergy and Knee Osteoarthritis. International Journal of Environmental Research and Public Health, 18(11), 5997. https://doi.org/10.3390/ijerph18115997