
Association between Residence Location and Pre-Hospital Delay in Patients with Heart Failure


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Sample
2.2. Procedure
2.3. Measurement
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
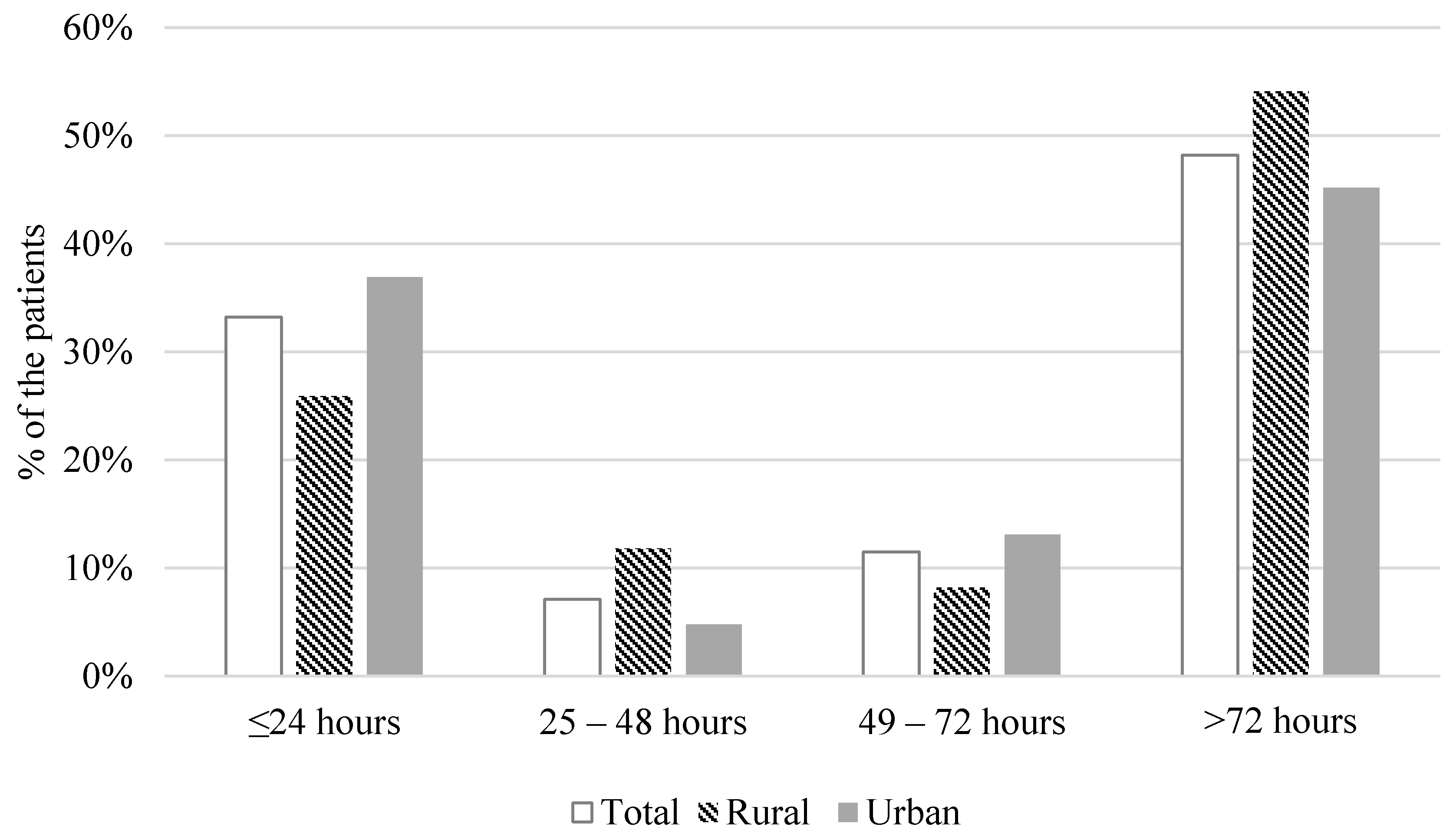
3.2. Duration of Pre-Hospital Delay
3.3. Symptom Experience before Seeking Medical Care
3.4. Interpretation and Response to Worsening of Symptoms by Patients
3.5. Factors Associated with a Pre-Hospital Delay
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allen, L.A.; Gheorghiade, M.; Reid, K.J.; Dunlay, S.M.; Chan, P.S.; Hauptman, P.J.; Zannad, F.; Konstam, M.A.; Spertus, J.A. Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Lesyuk, W.; Kriza, C.; Kolominsky-Rabas, P. Cost-of-illness studies in heart failure: A systematic review 2004–2016. BMC Cardiovasc. Disord. 2018, 18, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham, P.N.; Xiao, H.; Sarayani, A.; Chen, M.; Brown, J.D. Risk Factors Associated With 7- Versus 30-Day Readmission Among Patients with Heart Failure Using the Nationwide Readmission Database. Med. Care 2019, 57, 1–7. [Google Scholar] [CrossRef]
- Darling, C.; Saczynski, J.S.; McManus, D.D.; Lessard, D.; Spencer, F.A.; Goldberg, R.J. Delayed hospital presentation in acute decompensated heart failure: Clinical and patient reported factors. Heart Lung 2013, 42, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, R.; Sullivan, A.; Hales, S.; Gillies, G.; Burke, R.; Tofler, G. Symptom patterns, duration and responses in newly diagnosed patients with heart failure. Int. J. Nurs. Pract. 2012, 18, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Okada, A.; Tsuchihashi-Makaya, M.; Kang, J.; Aoki, Y.; Fukawa, M.; Matsuoka, S. Symptom Perception, Evaluation, Response to Symptom, and Delayed Care Seeking in Patients with Acute Heart Failure: An Observational Study. J. Cardiovasc. Nurs. 2019, 34, 36–43. [Google Scholar] [CrossRef]
- Sethares, K.A.; Sosa, M.E.; Fisher, P.; Riegel, B. Factors Associated with Delay in Seeking Care for Acute Decompensated Heart Failure. J. Cardiovasc. Nurs. 2014, 29, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.R.; Lee, K.S.; Dekker, R.D.; Welsh, J.D.; Song, E.K.; Abshire, D.A.; Lennie, T.A.; Moser, D.K. Prehospital Delay, Precipitants of Admission, and Length of Stay in Patients with Exacerbation of Heart Failure. Am. J. Crit. Care 2016, 26, 62–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphreys, J.S.; Solarsh, G. Populations at special health risk: Rural populations. In International Encyclopedia of Public Health; Heggenhougen, H.K.(Kris), Ed.; Academic Press: Oxford, UK, 2008; pp. 242–253. [Google Scholar] [CrossRef]
- Gamble, J.M.; Eurich, D.T.; Ezekowitz, J.A.; Kaul, P.; Quan, H.; McAlister, F.A. Patterns of care and outcomes differ for urban versus rural patients with newly diagnosed heart failure, even in a universal healthcare system. Circ. Heart Fail. 2011, 4, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Munoz, M.A.; Garcia, R.; Navas, E.; Duran, J.; Del Val-Garcia, J.L.; Verdu-Rotellar, J.M. Relationship between the place of living and mortality in patients with advanced heart failure. BMC Fam. Pract. 2020, 21, 145. [Google Scholar] [CrossRef]
- Teng, T.H.; Katzenellenbogen, J.M.; Hung, J.; Knuiman, M.; Sanfilippo, F.M.; Geelhoed, E.; Hobbs, M.; Thompson, S.C. Rural-urban differentials in 30-day and 1-year mortality following first-ever heart failure hospitalisation in Western Australia: A population-based study using data linkage. BMJ Open 2014, 4, e004724. [Google Scholar] [CrossRef]
- Kim, H. Interlinking open government data in Korea using administrative district knowledge graph. J. Inf. Sci. Theory Pract. 2018, 6, 18–30. [Google Scholar]
- Lee, K.S.; Moser, D.K. Heart failure symptom measures: Critical review. Eur. J. Cardiovasc. Nurs. 2013, 12, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Reeder, K.M.; Ercole, P.M.; Peek, G.M.; Smith, C.E. Symptom Perceptions and Self-care Behaviors in Patients Who Self-manage Heart Failure. J. Cardiovasc. Nurs. 2015, 30, E1–E7. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Lee, K.S.; Oh, S. An Integrative Review of the Symptom Perception Process in Heart Failure. J. Cardiovasc. Nurs. 2020. [Google Scholar] [CrossRef]
- Friedman, M.M.; Quinn, J.R. Heart Failure Patients’ Time, Symptoms, and Actions Before a Hospital Admission. J. Cardiovasc. Nurs. 2008, 23, 506–512. [Google Scholar] [CrossRef]
- Clark, A.M.; Freydberg, C.N.; McAlister, F.A.; Tsuyuki, R.T.; Armstrong, P.W.; Strain, L.A. Patient and informal caregivers’ knowledge of heart failure: Necessary but insufficient for effective self-care. Eur. J. Heart Fail. 2009, 11, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.; Hart, L.G.; Goodman, D.C. Geographic access to health care for rural Medicare beneficiaries. J. Rural Health 2006, 22, 140–146. [Google Scholar] [CrossRef]
- Verdejo, H.E.; Ferreccio, C.; Castro, P.F. Heart Failure in Rural Communities. Heart Fail. Clin. 2015, 11, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.J.; Kim, E.J. The effects of accessibility to medical facilities and public transportation on perceived health of urban and rural elderly: Using generalized ordered logic model. J. Korean Reg. Dev. Assoc. 2015, 27, 65–88. [Google Scholar]


{kind=link}
| Characteristic | Total | Rural Residents (n = 85) | Urban Residents (n = 168) | p-Value | |
|---|---|---|---|---|---|
| Mean (SD) or Frequency (%) | |||||
| Age (years) | 71.5 (12.7) | 74 (11.1) | 70 (13.3) | 0.018 | |
| Gender | Male | 117 (46.2%) | 39 (45.9%) | 78 (46.4%) | 0.934 |
| Female | 136 (53.8%) | 46 (54.1%) | 90 (53.6%) | ||
| Body mass index (kg/m2) | 23.9 (4.1) | 23.1 (4.0) | 24.4 (4.1) | 0.021 | |
| Education level | ≥High school graduate | 72 (28.5%) | 16 (18.8%) | 56 (33.3%) | 0.016 |
| Marital status | Single/widowed/divorced | 50 (19.8%) | 20 (23.5%) | 30 (17.9%) | 0.285 |
| Married | 203 (80.2%) | 65 (76.5%) | 138 (82.1%) | ||
| Charlson comorbidity index | 2.8 (1.7) | 2.6 (1.5) | 3.0 (1.8) | 0.086 | |
| Left ventricular ejection fraction | <40 | 129 (51.0%) | 46 (54.1%) | 83 (49.4%) | 0.479 |
| ≥40 | 124 (49.0%) | 39 (45.9%) | 8 (50.6%) | ||
| Etiology of heart failure | Ischemic | 90 (35.6%) | |||
| Non-ischemic | 163 (64.4%) | ||||
| Years since HF diagnosis | 2.8 (3.4) | 3.3 (3.9) | 2.5 (3.1) | 0.072 | |
| NT-pro BNP (n = 214) | 7266.5 (8625.7) | 6361.3 (7435.2) | 7744.9 (9182.1) | 0.265 | |
| NYHA functional class on admission | II | 55 (21.7%) | 12 (14.1%) | 43 (25.6%) | 0.037 |
| III/IV | 198 (78.3%) | 73 (85.9%) | 125 (74.4%) | ||
| Prior admission due to HF exacerbation within 3 months | 36 (14.2%) | 11 (12.9%) | 25 (14.9%) | 0.677 | |
| Number of medications | 6.9 (3.1) | 6.6 (2.7) | 7.2 (3.3) | 0.117 | |
| ACEi/ARB | 184 (72.7%) | 62 (74.7%) | 122 (74.4%) | 0.958 | |
| Beta blockers | 211 (83.4%) | 70 (84.3%) | 141 (86.0%) | 0.730 | |
| Diuretics | 225 (88.9%) | 75 (90.4%) | 150 (91.5%) | 0.774 | |
| Admission route | Emergency room | 174 (68.8%) | 58 (68.2%) | 116 (69.0%) | 0.895 |
| Clinic | 79 (31.2%) | 27 (31.8%) | 52 (31.0%) | 0.895 | |
| Admission vital sign | Systolic blood pressure | 138.6 (31.7) | 132.8 (29.5) | 141.6 (32.5) | 0.038 |
| Diastolic blood pressure | 81.0 (17.4) | 80.1 (16.8) | 81.4 (17.8) | 0.585 | |
| Heart rate | 97.1 (24.2) | 91.8 (21.7) | 99.7 (25.0) | 0.014 | |
| Respiration | 24.6 (6.0) | 24.6 (5.9) | 24.7 (6.0) | 0.877 | |
| Saturation | 95.0 (5.4) | 95.1 (6.2) | 95.0 (5.0) | 0.879 | |
| Time interval from onset to the admission (hours) 1 | 379.8 (1125.6) | 410.2 (930.7) | 364.5 (1214.7) | 0.114 | |
| Median: 72 (IQR: 17.25–240.00) | Median: 96 (IQR 24.0–324.0) | Median: 72 (IQR 11.25–240.0) | |||
| Total | Rural Residents | Urban Residents | p-Value | |
|---|---|---|---|---|
| Mean (SD) or Frequency (%) | ||||
| Symptom experience | ||||
| Total number of symptoms experienced before the admission | 2.6 (1.6) | 2.6 (1.6) | 2.7 (1.7) | 0.807 |
| Shortness of breath | 218 (86.2%) | 74 (87.1%) | 144 (85.7%) | 0.770 |
| Shortness of breath with activity | 68 (26.9%) | 27 (31.8%) | 41 (24.4%) | 0.212 |
| Lower extremity swelling | 45 (17.8%) | 8 (9.4%) | 37 (22.0%) | 0.013 |
| Coughing | 42 (16.6%) | 9 (10.6%) | 33 (19.6%) | 0.068 |
| Chest pain | 40 (15.8%) | 13 (15.3%) | 27 (16.1%) | 0.873 |
| Shortness of breath when lying flat | 37 (14.6%) | 10 (11.8%) | 27 (16.1%) | 0.360 |
| Poor appetite | 19 (7.5%) | 8 (9.4%) | 11 (6.5%) | 0.414 |
| Difficulty in sleeping | 16 (6.3%) | 6 (7.1%) | 10 (6.0%) | 0.733 |
| Palpitations | 14 (5.5%) | 5 (5.9%) | 9 (5.4%) | 0.863 |
| Weight gain | 13 (5.1%) | 2 (2.4%) | 11 (6.5%) | 0.229 |
| Dizziness | 11 (4.3%) | 6 (7.1%) | 5 (3.0%) | 0.133 |
| Abdominal bloating | 3 (1.2%) | 0 (0.0%) | 3 (1.8%) | 0.553 |
| Fatigue | 3 (1.2%) | 2 (2.4%) | 1 (0.6%) | 0.262 |
| Nausea and vomiting | 3 (1.2%) | 0 (0.0%) | 3 (1.2%) | 0.049 |
| Worrying | 1 (0.4%) | 1 (1.2%) | 0 (0.0%) | 0.336 |
| Feeling sad or depressed | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | N/A |
| Difficulty in concentrating or forgetfulness | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | N/A |
| Precipitating factors of symptoms identified by patients | N/A | |||
| Unable to identify | 171 (67.6%) | 60 (70.6%) | 111 (66.1%) | |
| Exacerbation of comorbid conditions | 67 (26.5%) | 18 (21.2%) | 49 (29.2%) | |
| Non-adherence to medication | 12 (4.7%) | 5 (5.9%) | 7 (4.2%) | |
| Psychological stress | 2 (0.8%) | 1 (1.2%) | 1 (0.6%) | |
| Loss of clinic appointment | 1 (0.4%) | 1 (1.2%) | 0 (0%) | |
| Actions taken to decrease symptoms before the hospitalization 1 | N/A | |||
| Doing nothing | 128 (50.6%) | 42 (49.4%) | 86 (51.2%) | |
| Went to clinic other than cardiology clinic | 62 (24.5%) | 25 (29.4%) | 37 (22.0%) | |
| Call to family | 69 (27.3%) | 23 (27.1%) | 46 (27.4%) | |
| Call to the doctor | 24 (9.5%) | 9 (10.6%) | 15 (8.9%) | |
| Took unrelated medication or actions irrelevant to HF | 5 (2.0%) | 1 (1.2%) | 4 (2.4%) | |
| Took an extra diuretic | 1 (0.4%) | 0 | 1 (0.6%) | |
| Variables | Unstandardized Coefficients | Standardized Coefficients | p-Value | 95% Confidence Interval |
|---|---|---|---|---|
| Urban residence (vs. rural residence) | −0.563 | −0.126 | 0.034 | −1.082, −0.043 |
| Age (years) | −0.003 | −0.016 | 0.806 | −0.025, 0.019 |
| Female (vs. male) | 0.120 | 0.028 | 0.635 | −0.377, 0.616 |
| Body mass index (kg/m2) | 0.061 | 0.118 | 0.061 | −0.003, 0.124 |
| ≥High school graduation (vs. <high school education) | 0.283 | 0.061 | 0.343 | −0.304, 0.87 |
| Married (vs. single/divorced/widowed) | −0.576 | −0.109 | 0.059 | −1.176, 0.023 |
| Preserved ejection fraction (vs. reduced rejection fraction) | −0.292 | −0.069 | 0.227 | −0.766, 0.183 |
| NYHA functional class III/IV (vs. II) | 0.289 | 0.057 | 0.348 | −0.317, 0.895 |
| Charlson comorbidity index | −0.088 | −0.072 | 0.232 | −0.232, 0.056 |
| Admission via clinic (vs. emergency department) | 1.286 | 0.283 | 0.000 | 0.755, 1.816 |
| Prior admission experience due to HF exacerbation | −0.326 | −0.054 | 0.346 | −1.007, 0.354 |
| Did nothing to relieve symptoms before seeking care (vs. did something) | 0.771 | 0.183 | 0.002 | 0.294, 1.248 |
| Shortness of breath | 0.388 | 0.064 | 0.283 | −0.322, 1.099 |
| Shortness of breath with activity | 0.387 | 0.082 | 0.178 | −0.178. 0.952 |
| Lower extremity swelling | 0.722 | 0.131 | 0.027 | 0.084, 1.359 |
| Coughing | 0.891 | 0.157 | 0.007 | 0.24, 1.541 |
| Chest pain | −0.778 | −0.135 | 0.023 | −1.450, −0.107 |
| Shortness of breath when lying flat | 0.093 | 0.352 | 0.791 | −0.600, 0.787 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.S.; Lee, H.; Park, J.-H. Association between Residence Location and Pre-Hospital Delay in Patients with Heart Failure. Int. J. Environ. Res. Public Health 2021, 18, 6679. https://doi.org/10.3390/ijerph18126679
Lee KS, Lee H, Park J-H. Association between Residence Location and Pre-Hospital Delay in Patients with Heart Failure. International Journal of Environmental Research and Public Health. 2021; 18(12):6679. https://doi.org/10.3390/ijerph18126679
Chicago/Turabian StyleLee, Kyoung Suk, Hyeongsuk Lee, and Jae-Hyeong Park. 2021. "Association between Residence Location and Pre-Hospital Delay in Patients with Heart Failure" International Journal of Environmental Research and Public Health 18, no. 12: 6679. https://doi.org/10.3390/ijerph18126679
APA StyleLee, K. S., Lee, H., & Park, J. -H. (2021). Association between Residence Location and Pre-Hospital Delay in Patients with Heart Failure. International Journal of Environmental Research and Public Health, 18(12), 6679. https://doi.org/10.3390/ijerph18126679