
Analysis of Physiological Response during Cardiopulmonary Resuscitation with Personal Protective Equipment: A Randomized Crossover Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- CPR test without PPE (CPR_control): carried out with the usual clothing of each rescuer.
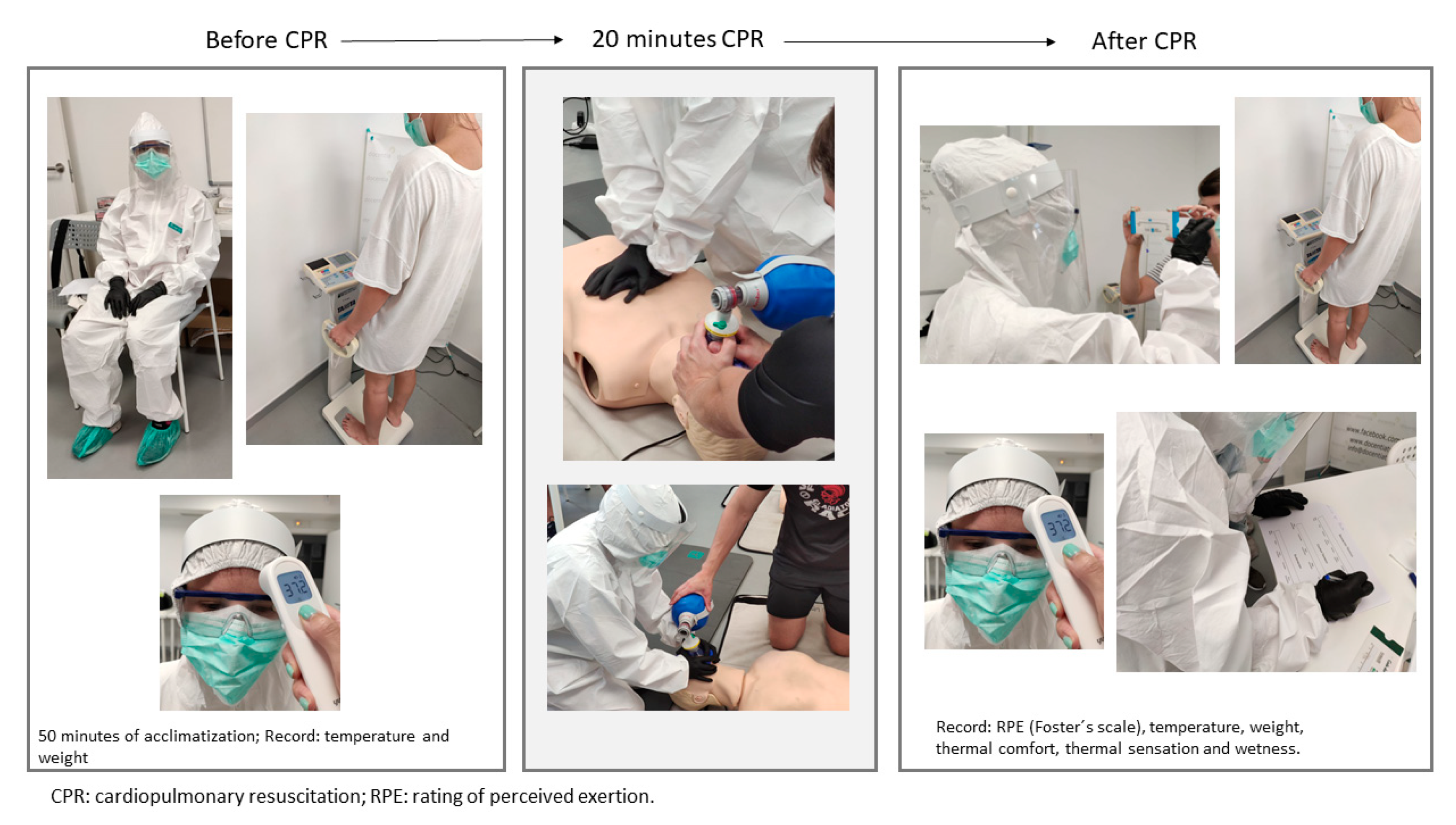
- CPR test with PPE (CPR_PPE): the personal protective equipment consisted of a protective coverall, face shield, goggles, surgical mask, KN95 mask, nitrile gloves and boot swabs (Figure 2).
2.2. Participants
2.3. Context
Retraining in Skills
2.4. Experimental Procedure and Materials
2.4.1. Physiological Adjustment
2.4.2. Cardiopulmonary Resuscitation (CPR) Test
2.5. Variables
2.5.1. CPR
- 1.
- Chest compression quality
- Compressions reaching the target depth: the target depth was considered to be between 5 and 6 cm [20].
- Compressions with a proper re-expansion: those in which the manikin’s chest returned to the starting position before performing the next compression [20].
- Compressions with a proper rate: the recommended rate was followed, that is, between 100 and 120 compressions per minute [20], recorded as a percentage.
- Compressions with a proper hand position: those in which the hands were placed on the lower half of the thorax [20].
- 2.
- Ventilation quality
- Ventilations with adequate volume: those with a volume between 500 and 600 mL [20].
- Insufficient volume ventilation: those with a volume less than 500 mL.
- Excessive volume ventilation: if the record was greater than 600 mL.
2.5.2. Physiological Variables
- 1.
- Maximum percentage of heart rate during CRP (%HRmax).
- 2.
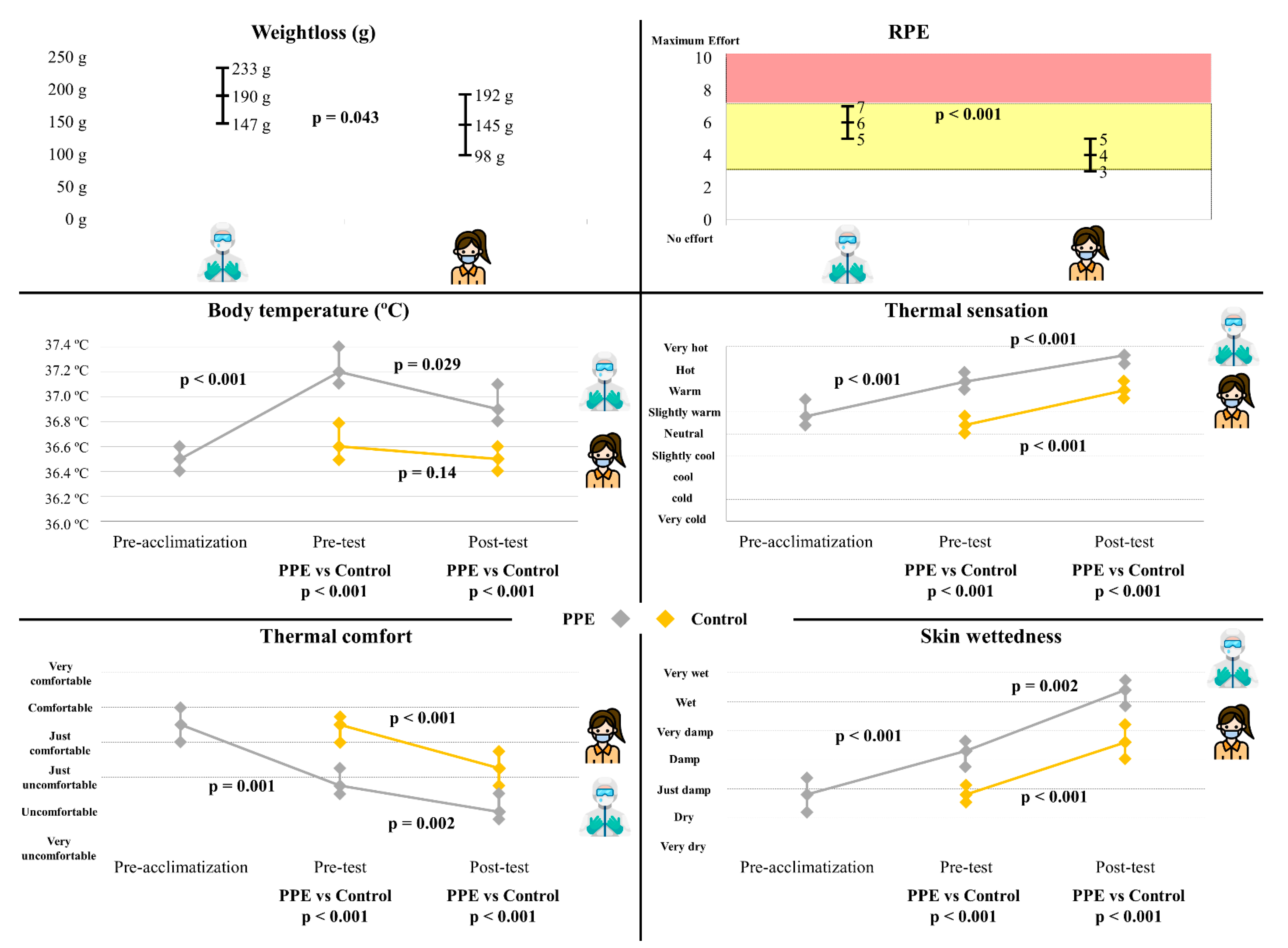
- Loss of body fluid (LBF).
- 3.
- Body temperature.
- 4.
- Ratings of perceived exertion (RPE).
- 5.
- Thermal comfort, thermal sensation and sweating.
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sprague, R.M.; Ladd, M.; Ashurst, J.V. EMS Resuscitation During Contamination While Wearing PPE. Available online: http://www.ncbi.nlm.nih.gov/books/NBK534092/ (accessed on 25 May 2021).
- Sahu, A.K.; Suresh, S.; Mathew, R.; Aggarwal, P.; Nayer, J. Impact of personal protective equipment on the effectiveness of chest compression—A systematic review and meta-analysis. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Malhotra, N.; Gupta, N.; Ish, S.; Ish, P. COVID-19 in intensive care. Some necessary steps for health care workers. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef]
- Nolan, J.P.; Monsieurs, K.G.; Bossaert, L.; Böttiger, B.W.; Greif, R.; Lott, C.; Madar, J.; Olasveengen, T.M.; Roehr, C.C.; Semeraro, F.; et al. European Resuscitation Council COVID-19 guidelines executive summary. Resuscitation 2020, 153, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Edelson, D.P.; Sasson, C.; Chan, P.S.; Atkins, D.L.; Aziz, K.; Becker, L.B.; Berg, R.A.; Bradley, S.M.; Brooks, S.C.; Cheng, A.; et al. Interim Guidance for Basic and Advanced Life Support in Adults, Children, and Neonates With Suspected or Confirmed COVID-19: From the Emergency Cardiovascular Care Committee and Get With The Guidelines-Resuscitation Adult and Pediatric Task Forces of the American Heart Association. Circulation 2020, 141, e933–e943. [Google Scholar] [PubMed] [Green Version]
- Tabah, A.; Ramanan, M.; Laupland, K.B.; Buetti, N.; Cortegiani, A.; Mellinghoff, J.; Morris, A.C.; Camporota, L.; Zappella, N.; Elhadi, M.; et al. Personal protective equipment and intensive care unit healthcare worker safety in the COVID-19 era (PPE-SAFE): An international survey. J. Crit. Care 2020, 59, 70–75. [Google Scholar] [CrossRef]
- Monsieurs, K.G.; Nolan, J.P.; Bossaert, L.L.; Greif, R.; Maconochie, I.K.; Nikolaou, N.I.; Perkins, G.D.; Soar, J.; Truhlář, A.; Wyllie, J.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 1. Executive summary. Resuscitation 2015, 95, 1–80. [Google Scholar] [CrossRef]
- Truhlář, A.; Deakin, C.D.; Soar, J.; Khalifa, G.E.A.; Alfonzo, A.; Bierens, J.J.L.M.; Brattebø, G.; Brugger, H.; Dunning, J.; Hunyadi-Antičević, S.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. Resuscitation 2015, 95, 148–201. [Google Scholar] [CrossRef]
- Carballo-Fazanes, A.; Barcala-Furelos, R.; Eiroa-Bermúdez, J.; Fernández-Méndez, M.; Abelairas-Gómez, C.; Martínez-Isasi, S.; Murciano, M.; Fernández-Méndez, F.; Rodríguez-Núñez, A. Physiological demands of quality cardiopulmonary resuscitation performed at simulated 3250 meters high. A pilot study. Am. J. Emerg. Med. 2020, 38, 2580–2585. [Google Scholar] [CrossRef] [PubMed]
- Barcala-Furelos, R.; Fernández-Méndez, M.; Cano-Noguera, F.; Otero-Agra, M.; Morán-Navarro, R.; Martínez-Isasi, S. Measuring the physiological impact of extreme heat on lifeguards during cardiopulmonary resuscitation. Randomized simulation study. Am. J. Emerg. Med. 2020, 38, 2019–2027. [Google Scholar] [CrossRef]
- Martin-Conty, J.L.; Martin-Rodríguez, F.; Criado-Álvarez, J.J.; Romo Barrientos, C.; Maestre-Miquel, C.; Viñuela, A.; Polonio-López, B.; Durantez-Fernández, C.; Marcos-Tejedor, F.; Mohedano-Moriano, A. Do Rescuers’ Physiological Responses and Anxiety Influence Quality Resuscitation under Extreme Temperatures? Int. J. Environ. Res. Public Health 2020, 17, 4241. [Google Scholar] [CrossRef]
- Abelairas-Gómez, C.; Barcala-Furelos, R.; Szarpak, L.; García-García, Ó.; Paz-Domínguez, Á.; López-García, S.; Rodríguez-Núñez, A. The effect of strength training on quality of prolonged basic cardiopulmonary resuscitation. Kardiol. Pol. 2017, 75, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Barcala-Furelos, R.; Abelairas-Gomez, C.; Romo-Perez, V.; Palacios-Aguilar, J. Effect of physical fatigue on the quality CPR—A water rescue study of lifeguards: Physical fatigue and quality CPR in a water rescue. Am. J. Emerg. Med. 2013, 31, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Loibner, M.; Hagauer, S.; Schwantzer, G.; Berghold, A.; Zatloukal, K. Limiting factors for wearing personal protective equipment (PPE) in a health care environment evaluated in a randomised study. PLoS ONE 2019, 14, e0210775. [Google Scholar] [CrossRef] [PubMed]
- Malysz, M.; Dabrowski, M.; Böttiger, B.W.; Smereka, J.; Kulak, K.; Szarpak, A.; Jaguszewski, M.; Filipiak, K.J.; Ladny, J.R.; Ruetzler, K.; et al. Resuscitation of the patient with suspected/confirmed COVID-19 when wearing personal protective equipment: A randomized multicenter crossover simulation trial. Cardiol. J. 2020, 27, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Kim, C.H.; Shin, S.D.; Haam, S. Influence of personal protective equipment on the performance of life-saving interventions by emergency medical service personnel. Simulation 2016, 92, 893–898. [Google Scholar] [CrossRef] [Green Version]
- Donoghue, A.J.; Kou, M.; Good, G.L.; Eiger, C.; Nash, M.; Henretig, F.M.; Stacks, H.; Kochman, A.; Debski, J.; Chen, J.-Y.; et al. Impact of Personal Protective Equipment on Pediatric Cardiopulmonary Resuscitation Performance: A Controlled Trial. Pediatr. Emerg. Care 2020, 36, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Barcala-Furelos, R.; Abelairas-Gómez, C.; Alonso-Calvete, A.; Cano-Noguera, F.; Carballo-Fazanes, A.; Martínez-Isasi, S.; Rodríguez-Núñez, A. Safe On-Boat Resuscitation by Lifeguards in COVID-19 Era: A Pilot Study Comparing Three Sets of Personal Protective Equipment. Prehosp. Disaster Med. 2021, 36, 163–169. [Google Scholar] [CrossRef]
- Song, W.; Liu, Y.; Ouyang, Y.; Chen, W.; Li, M.; Xianyu, S.; Yi, S. Recommendations on cardiopulmonary resuscitation strategy and procedure for novel coronavirus pneumonia. Resuscitation 2020, 152, 52–55. [Google Scholar] [CrossRef]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castrén, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Gräsner, J.-T.; Wenzel, V.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, C.; Iwami, T.; Murakami, Y.; Kitamura, T.; Okamoto, Y.; Marukawa, S.; Sakamoto, T.; Kawamura, T. Effectiveness of simplified 15-min refresher BLS training program: A randomized controlled trial. Resuscitation 2015, 90, 56–60. [Google Scholar] [CrossRef] [Green Version]
- Adelborg, K.; Bjørnshave, K.; Mortensen, M.B.; Espeseth, E.; Wolff, A.; Løfgren, B. A randomised crossover comparison of mouth-to-face-shield ventilation and mouth-to-pocket-mask ventilation by surf lifeguards in a manikin. Anaesthesia 2014, 69, 712–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barcala-Furelos, R.; Abelairas-Gomez, C.; Palacios-Aguilar, J.; Rey, E.; Costas-Veiga, J.; Lopez-Garcia, S.; Rodriguez-Nunez, A. Can surf-lifeguards perform a quality cardiopulmonary resuscitation sailing on a lifeboat? A quasi-experimental study. Emerg. Med. J. EMJ 2017, 34, 370–375. [Google Scholar] [CrossRef]
- Fungueiriño-Suárez, R.; Barcala-Furelos, R.; González-Fermoso, M.; Martínez-Isasi, S.; Fernández-Méndez, F.; González-Salvado, V.; Navarro-Patón, R.; Rodríguez-Núñez, A. Coastal Fishermen as Lifesavers While Sailing at High Speed: A Crossover Study. BioMed. Res. Int. 2018, 2018, 2747046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karvonen, M. The effects of training on heart rate: A longitudinal study. Ann. Med. Exp. Biol. Fenn. 1957, 35, 307–315. [Google Scholar] [PubMed]
- Padilla-Raygoza, N.; Ruiz-Paloalto, M.L.; Díaz-Guerrero, R.; Olvera-Villanueva, G.; Maldonado, A.; del Raygoza-Mendoza, M.P. Correlación de mediciones de temperatura corporal con 3 termómetros: Ótico, cutáneo y digital, en niños mexicanos. Enferm. Clín. 2014, 24, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar] [PubMed]
- Davey, S.; Reilly, M.; Newton, M.; Tipton, M. The Reproducibility and Validity of Visual Analogue Scales (VAS) that Assess Thermal Perceptions in Stable and Dynamic, Asymmetric Environments. In Proceedings of the 12th International Conference on Environmental Ergonomics, Piran, Slovenia, 19–24 August 2007; p. 117. [Google Scholar]
- Filingeri, D.; Fournet, D.; Hodder, S.; Havenith, G. Why wet feels wet? A neurophysiological model of human cutaneous wetness sensitivity. J. Neurophysiol. 2014, 112, 1457–1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Lu, K.-Z.; Yi, B.; Chen, Y. Chest Compression with Personal Protective Equipment During Cardiopulmonary Resuscitation: A Randomized Crossover Simulation Study. Medicine 2016, 95, e3262. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Tu, X.; Zhou, X.; Yu, J.; Luo, S.; Ma, L.; Liu, C.; Zhao, Y.; Jin, X. Wearing a N95 mask increases rescuer’s fatigue and decreases chest compression quality in simulated cardiopulmonary resuscitation. Am. J. Emerg. Med. 2020, 44, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Kienbacher, C.L.; Grafeneder, J.; Tscherny, K.; Krammel, M.; Fuhrmann, V.; Niederer, M.; Neudorfsky, S.; Herbich, K.; Schreiber, W.; Herkner, H.; et al. The use of personal protection equipment does not impair the quality of cardiopulmonary resuscitation: A prospective triple-cross over randomised controlled non-inferiority trial. Resuscitation 2021, 160, 79–83. [Google Scholar] [CrossRef] [PubMed]
- González-Alonso, J.; Coyle, E.F. Efectos fisiológicos de la deshidratación. ¿Por qué los deportistas deben ingerir líquidos durante el ejercicio en el calor? Apunts. Educ. Física Deport. 1998, 4, 46–52. [Google Scholar]
- Scherr, J.; Wolfarth, B.; Christle, J.W.; Pressler, A.; Wagenpfeil, S.; Halle, M. Associations between Borg’s rating of perceived exertion and physiological measures of exercise intensity. Eur. J. Appl. Physiol. 2013, 113, 147–155. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Kenefick, R.W.; Montain, S.J.; Sawka, M.N. Mechanisms of aerobic performance impairment with heat stress and dehydration. J. Appl. Physiol. 2010, 109, 1989–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawka, M.N.; Montain, S.J. Fluid and electrolyte supplementation for exercise heat stress. Am. J. Clin. Nutr. 2000, 72, S564–S572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barcala-Furelos, R.; Szpilman, D.; Palacios-Aguilar, J.; Costas-Veiga, J.; Abelairas-Gomez, C.; Bores-Cerezal, A.; López-García, S.; Rodríguez-Nuñez, A. Assessing the efficacy of rescue equipment in lifeguard resuscitation efforts for drowning. Am. J. Emerg. Med. 2016, 34, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Abelairas-Gómez, C.; Barcala-Furelos, R.; Mecías-Calvo, M.; Rey-Eiras, E.; López-García, S.; Costas-Veiga, J.; Bores-Cerezal, A.; Palacios-Aguilar, J. Prehospital Emergency Medicine at the Beach: What Is the Effect of Fins and Rescue Tubes in Lifesaving and Cardiopulmonary Resuscitation After Rescue? Wilderness Environ. Med. 2017, 28, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Flouris, A.D.; Schlader, Z.J. Human behavioral thermoregulation during exercise in the heat. Scand. J. Med. Sci. Sports 2015, 25, 52–64. [Google Scholar] [CrossRef]
- Havenith, G.; Fogarty, A.; Bartlett, R.; Smith, C.J.; Ventenat, V. Male and female upper body sweat distribution during running measured with technical absorbents. Eur. J. Appl. Physiol. 2008, 104, 245–255. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 20 | CPR with PPE | CPR Control | |||
|---|---|---|---|---|---|
| Mean (SD) | CI | Mean (SD) | CI | ||
| Compressions | |||||
| Overall quality of compressions, in percentage terms | 81 (14) | 75–88 | 81 (13) | 75–87 | p = 0.82 |
| Total number of compressions | 868 (50) | 844–891 | 867 (48) | 845–890 | p = 1.00 |
| Percentage of compressions that reach the correct depth | 62 (32) | 47–77 | 61 (32) | 46–76 | p = 0.74 |
| Percentage of compressions with correct reexpansion | 89 (19) | 81–98 | 88 (19) | 78–97 | p = 0.52 |
| Percentage of compressions with correct rhythm | 75 (31) | 61–90 | 77 (28) | 64–90 | p = 1.00 |
| Percentage of compressions with correct hand position | 99 (2) | 98–100 | 100 (1) | 99–100 | p = 0.96 |
| Ventilations | |||||
| Active phase of CPR (compressions and ventilations) | |||||
| Total number of ventilations | 58 (4) | 56–59 | 57 (4) | 55–59 | p = 0.48 |
| Percentage of ventilations with insufficient volume | 38 (39) | 20–57 | 36 (39) | 18–55 | p = 0.62 |
| Percentage of ventilations with correct volume | 40 (34) | 25–56 | 40 (36) | 23–56 | p = 0.85 |
| Percentage of ventilations with excessive volume | 21 (35) | 5–38 | 24 (39) | 6–42 | p = 0.75 |
| CPR support phase (attaching the mask) | |||||
| Total number of ventilations | 52 (2) | 51–53 | 52 (2) | 50–53 | p = 0.86 |
| Percentage of ventilations with effective air intake | 99 (1) | 98–100 | 99 (2) | 98–100 | p = 0.79 |
| Overall quality of CPR, in percentage terms | 61 (19) | 52–70 | 61 (20) | 51–68 | p = 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Méndez, M.; Otero-Agra, M.; Fernández-Méndez, F.; Martínez-Isasi, S.; Santos-Folgar, M.; Barcala-Furelos, R.; Rodríguez-Núñez, A. Analysis of Physiological Response during Cardiopulmonary Resuscitation with Personal Protective Equipment: A Randomized Crossover Study. Int. J. Environ. Res. Public Health 2021, 18, 7093. https://doi.org/10.3390/ijerph18137093
Fernández-Méndez M, Otero-Agra M, Fernández-Méndez F, Martínez-Isasi S, Santos-Folgar M, Barcala-Furelos R, Rodríguez-Núñez A. Analysis of Physiological Response during Cardiopulmonary Resuscitation with Personal Protective Equipment: A Randomized Crossover Study. International Journal of Environmental Research and Public Health. 2021; 18(13):7093. https://doi.org/10.3390/ijerph18137093
Chicago/Turabian StyleFernández-Méndez, María, Martín Otero-Agra, Felipe Fernández-Méndez, Santiago Martínez-Isasi, Myriam Santos-Folgar, Roberto Barcala-Furelos, and Antonio Rodríguez-Núñez. 2021. "Analysis of Physiological Response during Cardiopulmonary Resuscitation with Personal Protective Equipment: A Randomized Crossover Study" International Journal of Environmental Research and Public Health 18, no. 13: 7093. https://doi.org/10.3390/ijerph18137093
APA StyleFernández-Méndez, M., Otero-Agra, M., Fernández-Méndez, F., Martínez-Isasi, S., Santos-Folgar, M., Barcala-Furelos, R., & Rodríguez-Núñez, A. (2021). Analysis of Physiological Response during Cardiopulmonary Resuscitation with Personal Protective Equipment: A Randomized Crossover Study. International Journal of Environmental Research and Public Health, 18(13), 7093. https://doi.org/10.3390/ijerph18137093