
Arthroscopic Tenotomy of the Long Head of the Biceps Tendon and Section of the Anterior Joint Capsule Produce Moderate Osteoarthritic Changes in an Experimental Sheep Model

 ,
,  ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
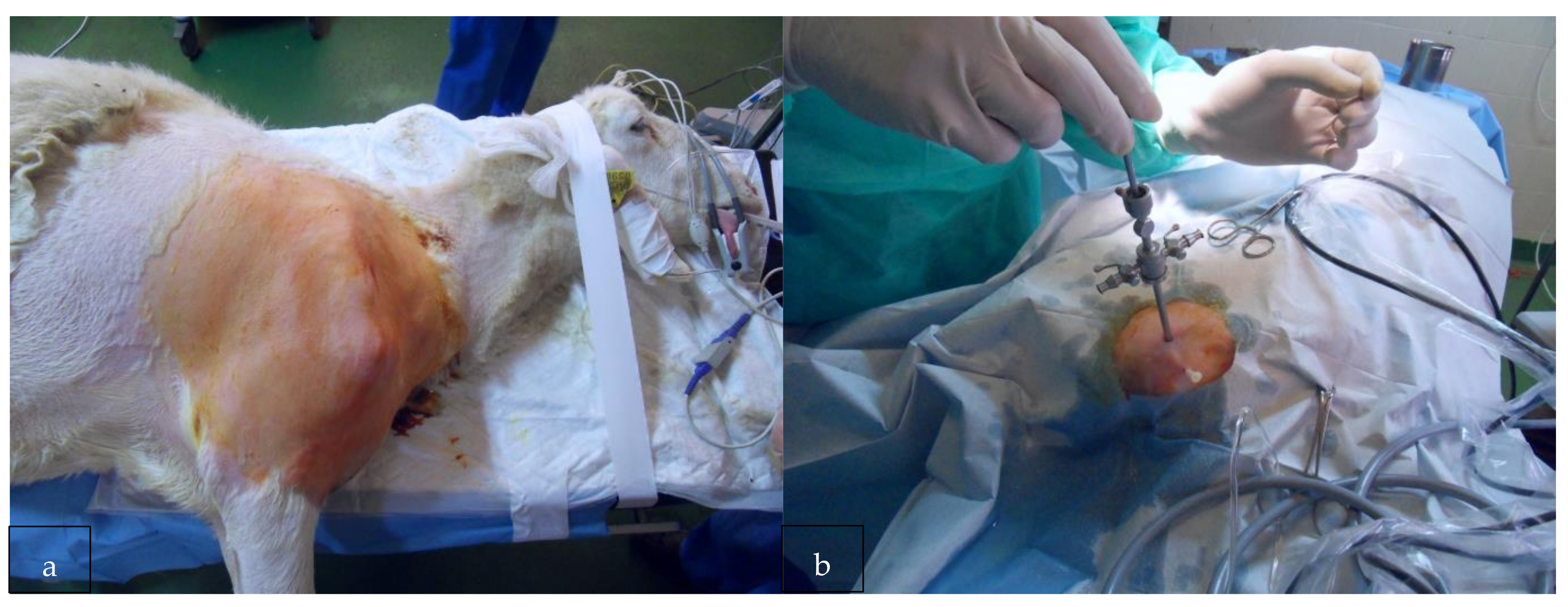
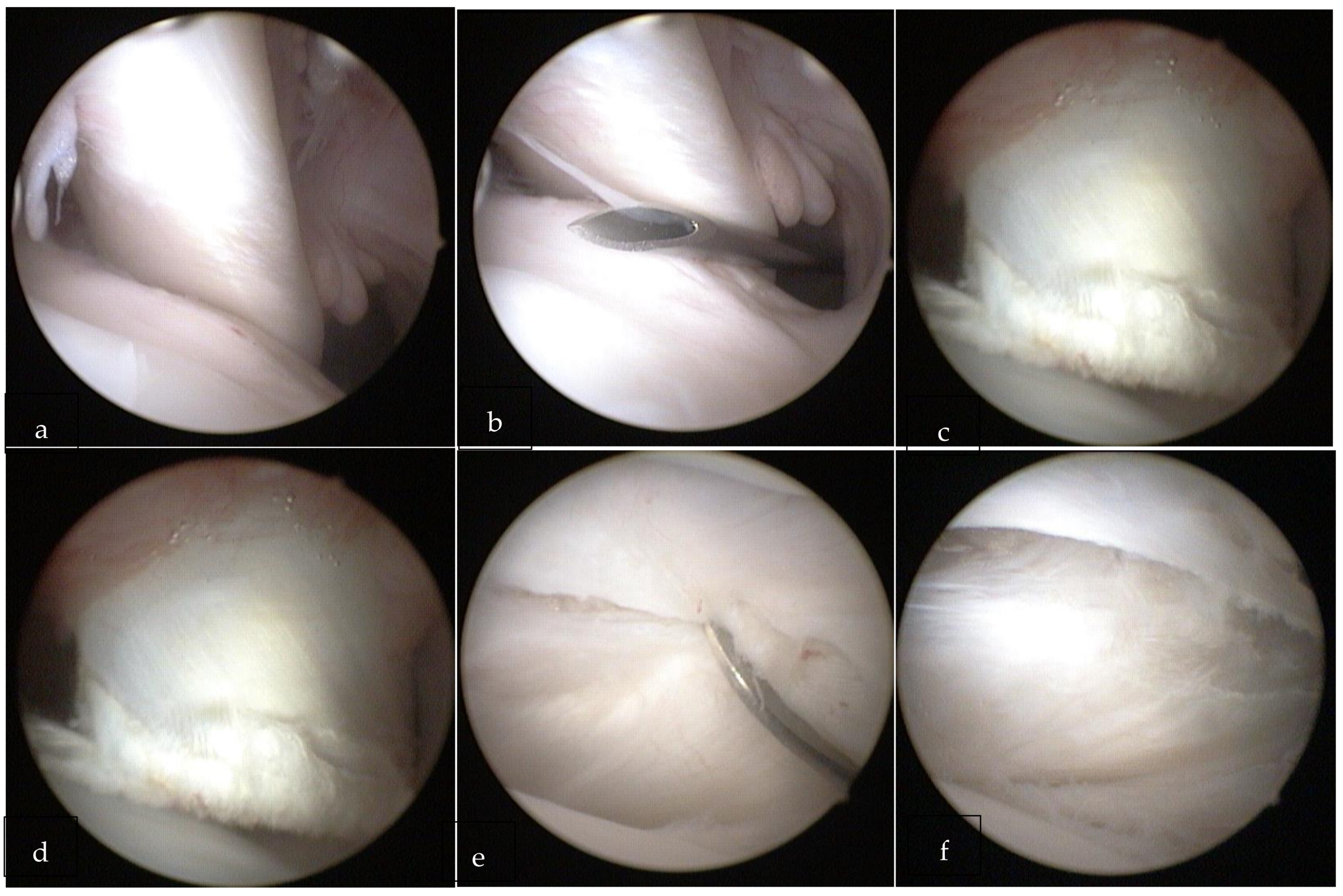
2.2. Surgical Procedure
2.3. Imaging
2.4. Shoulder Arthritis According to the Histopathologic Scoring System
2.5. Statistical Analysis
3. Results
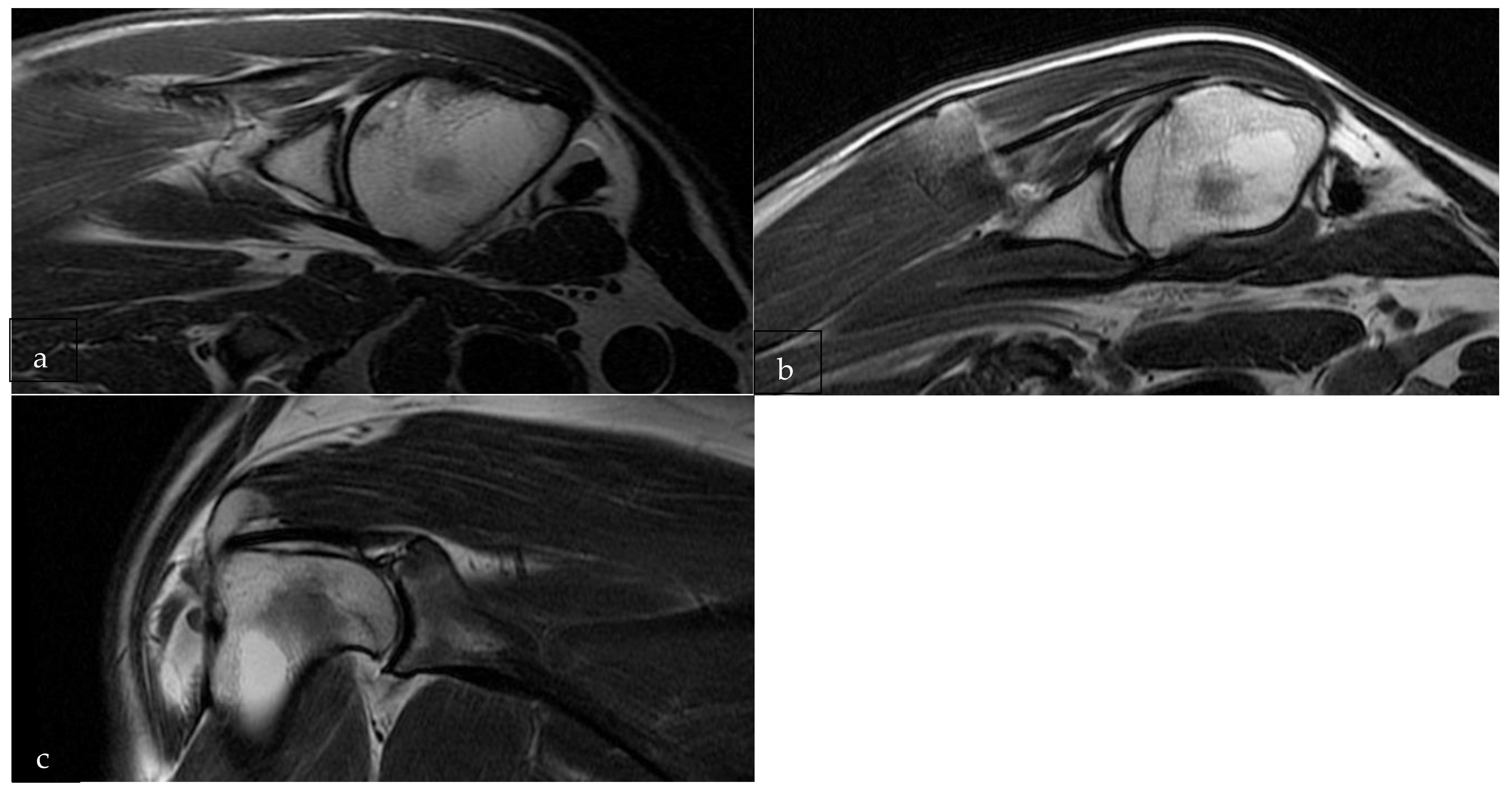
3.1. Pre-Operative MRI Evaluation
3.2. Post-Operative MRI Evaluation
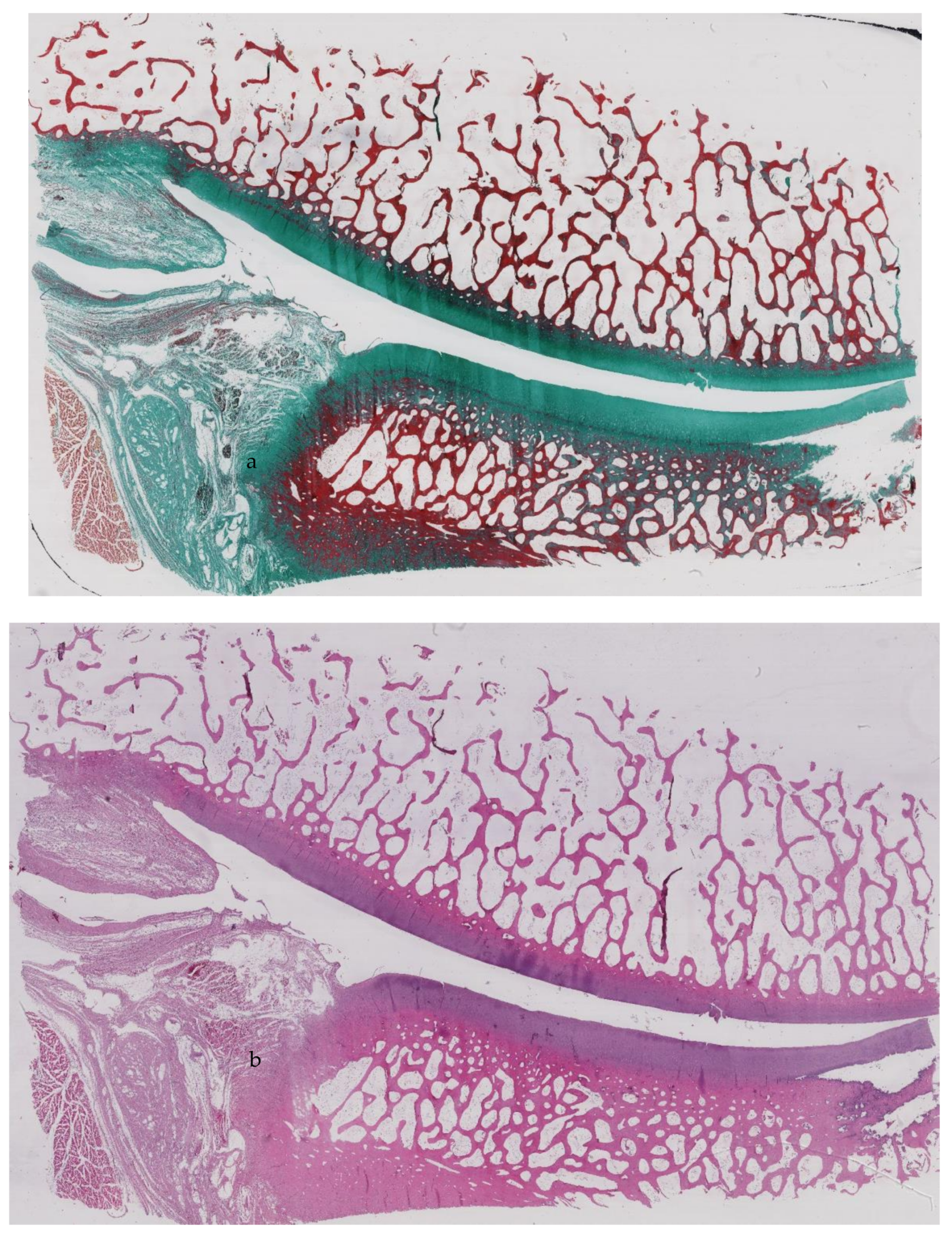
3.3. Histological Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
Abbreviations
| AC | Articular cartilage |
| ACL | anterior cruciate ligament |
| AIG | anterior-inferior glenoid |
| AIH | anterior-inferior humerus |
| ASG | anterior-superior glenoid |
| ASH | anterior-superior humerus |
| BML | bone marrow lesions |
| CSA | cartilage surface area |
| CTL | cervical, thoracic, lumbar |
| EDTA | Ethylenediaminetetraacetic acid |
| GH | glenohumeral |
| ICRS | International Cartilage Regeneration and Joint Preservation Society |
| MRI | Magnetic Resonance Imaging |
| MSAS | Murine Shoulder Arthritis Score |
| OA | Osteoarthritis |
| OARSI | Osteoarthritis Research Society International |
| OSAS | Ovine Shoulder Arthritis Score |
| PIG | posterior-inferior glenoid |
| PIH | posterior-inferior humerus |
| PSG | posterior-superior glenoid |
| PSH | posterior-superior humerus |
| SD | standard deviation |
| sMOASS | Sheep MRI Osteoarthritis Shoulder Score |
References
- Forriol, F.; Longo, U.G.; Hernández-Vaquero, D.; Monllau, J.C.; Montserrat, F.; Valentí, J.R.; Vaquero, J.; Maffulli, N.; Denaro, V. The effects of previous meniscus and anterior cruciate ligament injuries in patients with total knee arthroplasty. Ortop. Traumatol. Rehabil. 2010, 12, 50–57. [Google Scholar]
- Weinstein, D.M.; Bucchieri, J.S.; Pollock, R.G.; Flatow, E.L.; Bigliani, L.U. Arthroscopic debridement of the shoulder for osteoarthritis. Arthrosc. J. Arthrosc. Relat. Surg. 2000, 16, 471–476. [Google Scholar] [CrossRef]
- Longo, U.G.; Petrillo, S.; Rizzello, G.; Candela, V.; Denaro, V. Deltoid muscle tropism does not influence the outcome of arthroscopic rotator cuff repair. Musculoskelet. Surg. 2016, 100, 193–198. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Longo, U.G.; Madry, H.; Marchettini, P.; Marmotti, A.; Van Assche, D.; Zanon, G.; Peretti, G. Non-surgical treatments for the management of early osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Fumo, C.; Rizzello, G.; Khan, W.S.; Maffulli, N.; Denaro, V. Osteoarthritis: New Insights in Animal Models. Open Orthop. J. 2012, 6, 558–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschi, F.; Longo, G.U.; Ruzzini, L.; Rizzello, G.; Maffulli, N.; Denaro, V. The Roman Bridge: A “double pulley–suture bridges” technique for rotator cuff repair. BMC Musculoskelet. Disord. 2007, 8, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Manzano, G.; Kim, H.T.; Feeley, B.T. A rat model of massive rotator cuff tears. J. Orthop. Res. 2010, 29, 588–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longo, U.G.; Forriol, F.; Campi, S.; Maffulli, N.; Denaro, V. Animal Models for Translational Research on Shoulder Pathologies. Sports Med. Arthrosc. Rev. 2011, 19, 184–193. [Google Scholar] [CrossRef]
- Reuther, K.E.; Sarver, J.J.; Schultz, S.M.; Lee, C.S.; Sehgal, C.M.; Glaser, D.L.; Soslowsky, L.J. Glenoid cartilage mechanical properties decrease after rotator cuff tears in a rat model. J. Orthop. Res. 2012, 30, 1435–1439. [Google Scholar] [CrossRef] [Green Version]
- Kramer, E.J.; Bodendorfer, B.M.; Laron, D.; Wong, J.; Kim, H.T.; Liu, X.; Feeley, B.T. Evaluation of cartilage degeneration in a rat model of rotator cuff tear arthropathy. J. Shoulder Elb. Surg. 2013, 22, 1702–1709. [Google Scholar] [CrossRef] [Green Version]
- Turner, A.S. Experiences with sheep as an animal model for shoulder surgery: Strengths and shortcomings. J. Shoulder Elb. Surg. 2007, 16, S158–S163. [Google Scholar] [CrossRef]
- Garcia, D.; Longo, U.G.; Vaquero, J.; Forriol, F.; Loppini, M.; Khan, W.S.; Denaro, V. Amniotic membrane transplant for articular cartilage repair: An experimental study in sheep. Curr Stem Cell Res Ther 2015, 10, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Kozono, N.; Okada, T.; Takeuchi, N.; Hamai, S.; Higaki, H.; Shimoto, T.; Ikebe, S.; Gondo, H.; Nakanishi, Y.; Senju, T.; et al. Dynamic kinematics of the glenohumeral joint in shoulders with rotator cuff tears. J. Orthop. Surg. Res. 2018, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- Frank, R.M.; Cotter, E.J.; Strauss, E.; Jazrawi, L.M.; Romeo, A.A. Management of Biceps Tendon Pathology. J. Am. Acad. Orthop. Surg. 2018, 26, e77–e89. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Reuther, K.E.; Tucker, J.J.; Sarver, J.J.; Yannascoli, S.M.; Caro, A.C.; Voleti, P.B.; Rooney, S.; Glaser, D.L.; Soslowsky, L.J. Biceps Detachment Decreases Joint Damage in a Rotator Cuff Tear Rat Model. Clin. Orthop. Relat. Res. 2014, 472, 2404–2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longo, U.G.; Loppini, M.; Marineo, G.; Khan, W.S.; Maffulli, N.; Denaro, V. Tendinopathy of the Tendon of the Long Head of the Biceps. Sports Med. Arthrosc. Rev. 2011, 19, 321–332. [Google Scholar] [CrossRef]
- Longo, U.G.; Garau, G.; Denaro, V.; Maffulli, N. Surgical management of tendinopathy of biceps femoris tendon in athletes. Disabil. Rehabil. 2008, 30, 1602–1607. [Google Scholar] [CrossRef]
- Del Buono, A.; Oliva, F.; Longo, U.G.; Rodeo, S.A.; Orchard, J.; Denaro, V.; Maffulli, N. Metalloproteases and rotator cuff disease. J. Shoulder Elb. Surg. 2012, 21, 200–208. [Google Scholar] [CrossRef]
- Ahrens, P.M.; Boileau, P. The long head of biceps and associated tendinopathy. J. Bone Jt. Surg. Br. Vol. 2007, 89, 1001–1009. [Google Scholar] [CrossRef] [Green Version]
- Zabrzyński, J.; Huri, G.; Gryckiewicz, S.; Çetik, R.M.; Szwedowski, D.; Łapaj, Ł.; Gagat, M.; Paczesny, Ł. Biceps Tenodesis versus Tenotomy with Fast Rehabilitation Protocol—A Functional Perspective in Chronic Tendinopathy. J. Clin. Med. 2020, 9, 3938. [Google Scholar] [CrossRef]
- Little, C.; Smith, M.; Cake, M.; Read, R.; Murphy, M.; Barry, F. The OARSI histopathology initiative—Recommendations for histological assessments of osteoarthritis in sheep and goats. Osteoarthr. Cartil. 2010, 18, S80–S92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forriol, F.; Longo, U.G.; Alvarez, E.; Campi, S.; Ripalda-Cemborain, P.; Rabitti, C.; Maffulli, N.; Denaro, V. Scanty integration of osteochondral allografts cryopreserved at low temperatures with dimethyl sulfoxide. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Moya-Angeler, J.; Gonzalez-Nieto, J.; Monforte, J.S.; Altonaga, J.R.; Vaquero, J.; Forriol, F. Surgical induced models of joint degeneration in the ovine stifle: Magnetic resonance imaging and histological assessment. Knee 2016, 23, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Zingman, A.; Li, H.; Sundem, L.; Dehority, B.; Geary, M.; Fussel, T.; Mooney, R.; Zuscik, M.; Elfar, J. Shoulder arthritis secondary to rotator cuff tear: A reproducible murine model and histopathologic scoring system. J. Orthop. Res. 2017, 35, 506–514. [Google Scholar] [CrossRef] [Green Version]
- Zabrzyński, J.; Paczesny, Ł.; Zabrzyńska, A.; Grzanka, D.; Łapaj, Ł. Sonography in the instability of the long head of the biceps tendon confronted with histopathologic and arthroscopic findings. Folia Morphol. 2018, 77, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Zabrzyński, J.; Gagat, M.; Paczesny, Ł.; Łapaj, Ł.; Grzanka, D. Electron microscope study of the advanced tendinopathy process of the long head of the biceps brachii tendon treated arthroscopically. Folia Morphol. 2018, 77, 371–377. [Google Scholar] [CrossRef] [Green Version]
- Zabrzyński, J.; Paczesny, Ł.; Łapaj, Ł.; Grzanka, D.; Szukalski, J. Process of neovascularisation compared with pain intensity in tendinopathy of the long head of the biceps brachii tendon associated with concomitant shoulder disorders, after arthroscopic treatment. Microscopic evaluation supported by immunohistochemical. Folia Morphol. 2018, 77, 378–385. [Google Scholar] [CrossRef] [Green Version]
- van der Kraan, P. Factors that influence outcome in experimental osteoarthritis. Osteoarthr. Cartil. 2017, 25, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.; Clarke, E.; Little, C. Considerations for the design and execution of protocols for animal research and treatment to improve reproducibility and standardization: DEPART well-prepared and ARRIVE safely. Osteoarthr. Cartil. 2017, 25, 354–363. [Google Scholar] [CrossRef] [Green Version]
- Walch, G.; Edwards, T.B.; Boulahia, A.; Nové-Josserand, L.; Neyton, L.; Szabo, I. Arthroscopic tenotomy of the long head of the biceps in the treatment of rotator cuff tears: Clinical and radiographic results of 307 cases. J. Shoulder Elb. Surg. 2005, 14, 238–246. [Google Scholar] [CrossRef]
- Kelly, A.M.; Drakos, M.C.; Fealy, S.; Taylor, S.A.; O’Brien, S.J. Arthroscopic Release of the Long Head of the Biceps Tendon. Am. J. Sports Med. 2005, 33, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Mathewson, M.A.; Kwan, A.; Eng, C.M.; Lieber, R.; Ward, S.R. Comparison of rotator cuff muscle architecture among humans and selected vertebrate species. J. Exp. Biol. 2014, 217, 261–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonnabend, D.H.; Young, A.A. Comparative anatomy of the rotator cuff. J. Bone Jt. Surg. Br. Vol. 2009, 91, 1632–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffulli, N.; Longo, U.G.; Maffulli, G.D.; Rabitti, C.; Khanna, A.; Denaro, V. Marked pathological changes proximal and distal to the site of rupture in acute Achilles tendon ruptures. Knee Surg. Sports Traumatol. Arthrosc. 2010, 19, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Mainil-Varlet, P.; Aigner, T.; Brittberg, M.; Bullough, P.; Hollander, A.; Hunziker, E.; Kandel, R.; Nehrer, S.; Pritzker, K.; Roberts, S.; et al. Histological assessment of cartilage repair: A report by the Histology Endpoint Committee of the International Cartilage Repair Society (ICRS). J. Bone Jt. Surg. Am. Vol. 2003, 85, 45–57. [Google Scholar] [CrossRef]
- Lorenz, J.; Grässel, S. Experimental Osteoarthritis Models in Mice. Methods Mol. Biol. 2014, 1194, 401–419. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Muendermann, A. The role of ambulatory mechanics in the initiation and progression of knee osteoarthritis. Curr. Opin. Rheumatol. 2006, 18, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.E.; Reuther, K.E.; Sarver, J.J.; Lee, C.S.; Thomas, S.J.; Glaser, D.L.; Soslowsky, L.J. Restoration of anterior-posterior rotator cuff force balance improves shoulder function in a rat model of chronic massive tears. J. Orthop. Res. 2011, 29, 1028–1033. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Points | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Sphericity of articular portion of humeral head | 100% spherical | 80% spherical | 50% spherical | Mostlyflattened/pitted |
| Glenoid bony erosion | 0 | <20% | >20%, <50% | >50% |
| Cellularity | Obvious hypocellular layer superficial to tidemark | Reactive cellular layer superficial to tidemark | Scant layer superficial to tidemark | Tidemark difficult to distinguish/ inconsistent |
| Subchondral bone morphology | Well trabeculated subchondral bone without bone marrow close to osteochondral junction | Scant bone marrow approaching osteochondral junction | <50% of subchondral bone infiltrated by marrow space | >50% of subchondral bone infiltrated by marrow space |
| Alcian blue staining | Intense blue staining deep to tidemark | Two separate areas of intense blue staining: one deep to tidemark and one superficial | One thin area of deep blue staining with tidemark unclear | Disorganized |
| Pannus present | No | — | — | Yes |
| Sheep n° | ICC (95% CI 0.95–0.99) |
|---|---|
| 1 | 0.80934561 |
| 2 | 0.97668054 |
| 3 | 0.87859618 |
| 4 | 0.92000267 |
| 5 | 0.90783898 |
| 6 | 0.94328601 |
| 7 | 0.94706078 |
| 8 | 0.97789721 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; Forriol, F.; Candela, V.; Tecce, S.M.; De Salvatore, S.; Altonaga, J.R.; Wallace, A.L.; Denaro, V. Arthroscopic Tenotomy of the Long Head of the Biceps Tendon and Section of the Anterior Joint Capsule Produce Moderate Osteoarthritic Changes in an Experimental Sheep Model. Int. J. Environ. Res. Public Health 2021, 18, 7471. https://doi.org/10.3390/ijerph18147471
Longo UG, Forriol F, Candela V, Tecce SM, De Salvatore S, Altonaga JR, Wallace AL, Denaro V. Arthroscopic Tenotomy of the Long Head of the Biceps Tendon and Section of the Anterior Joint Capsule Produce Moderate Osteoarthritic Changes in an Experimental Sheep Model. International Journal of Environmental Research and Public Health. 2021; 18(14):7471. https://doi.org/10.3390/ijerph18147471
Chicago/Turabian StyleLongo, Umile Giuseppe, Francisco Forriol, Vincenzo Candela, Salvatore Maria Tecce, Sergio De Salvatore, Jose R. Altonaga, Andrew L. Wallace, and Vincenzo Denaro. 2021. "Arthroscopic Tenotomy of the Long Head of the Biceps Tendon and Section of the Anterior Joint Capsule Produce Moderate Osteoarthritic Changes in an Experimental Sheep Model" International Journal of Environmental Research and Public Health 18, no. 14: 7471. https://doi.org/10.3390/ijerph18147471
APA StyleLongo, U. G., Forriol, F., Candela, V., Tecce, S. M., De Salvatore, S., Altonaga, J. R., Wallace, A. L., & Denaro, V. (2021). Arthroscopic Tenotomy of the Long Head of the Biceps Tendon and Section of the Anterior Joint Capsule Produce Moderate Osteoarthritic Changes in an Experimental Sheep Model. International Journal of Environmental Research and Public Health, 18(14), 7471. https://doi.org/10.3390/ijerph18147471