
Differential Kinetics of Cycle Threshold Values during Admission by Symptoms among Patients with Mild COVID-19: A Prospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design
2.3. Participants
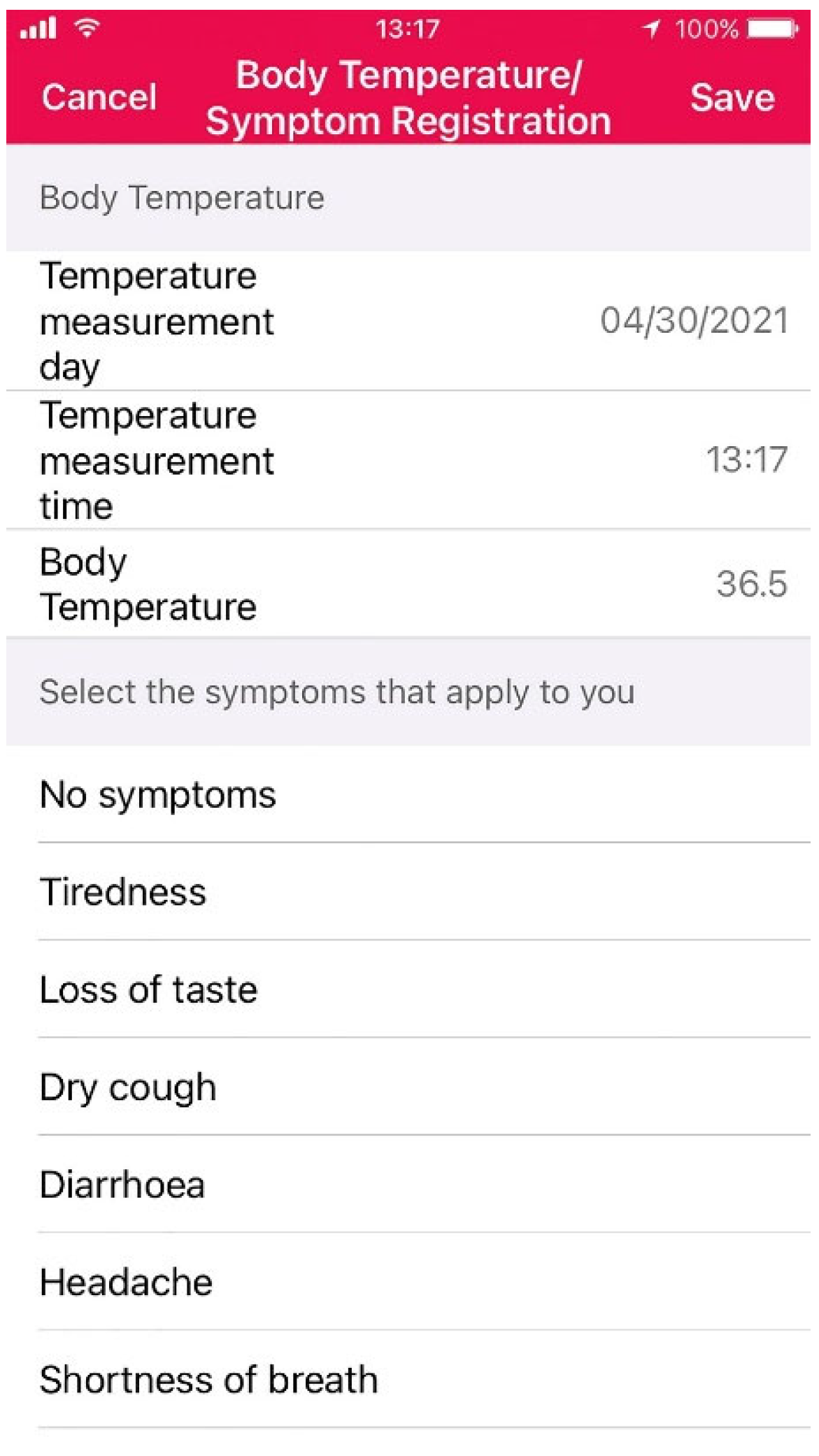
2.4. MySOS
2.5. Cycle threshold (Ct) Values of Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) Test
2.6. University of Pennsylvania Smell Identification Test (UPSIT)
2.7. Data Monitoring during Admission
2.8. Post-Discharge Questionnaire Survey
2.9. Statistics
3. Results
3.1. Patients’ Characteristics Stratified by Three Groups: Asymptomatic Patients, Febrile Patients, and Afebrile Patients with any Other Symptoms
3.2. Characteristics of Three Patients Who Deteriorated after Admission and Were Referred to the Hospital
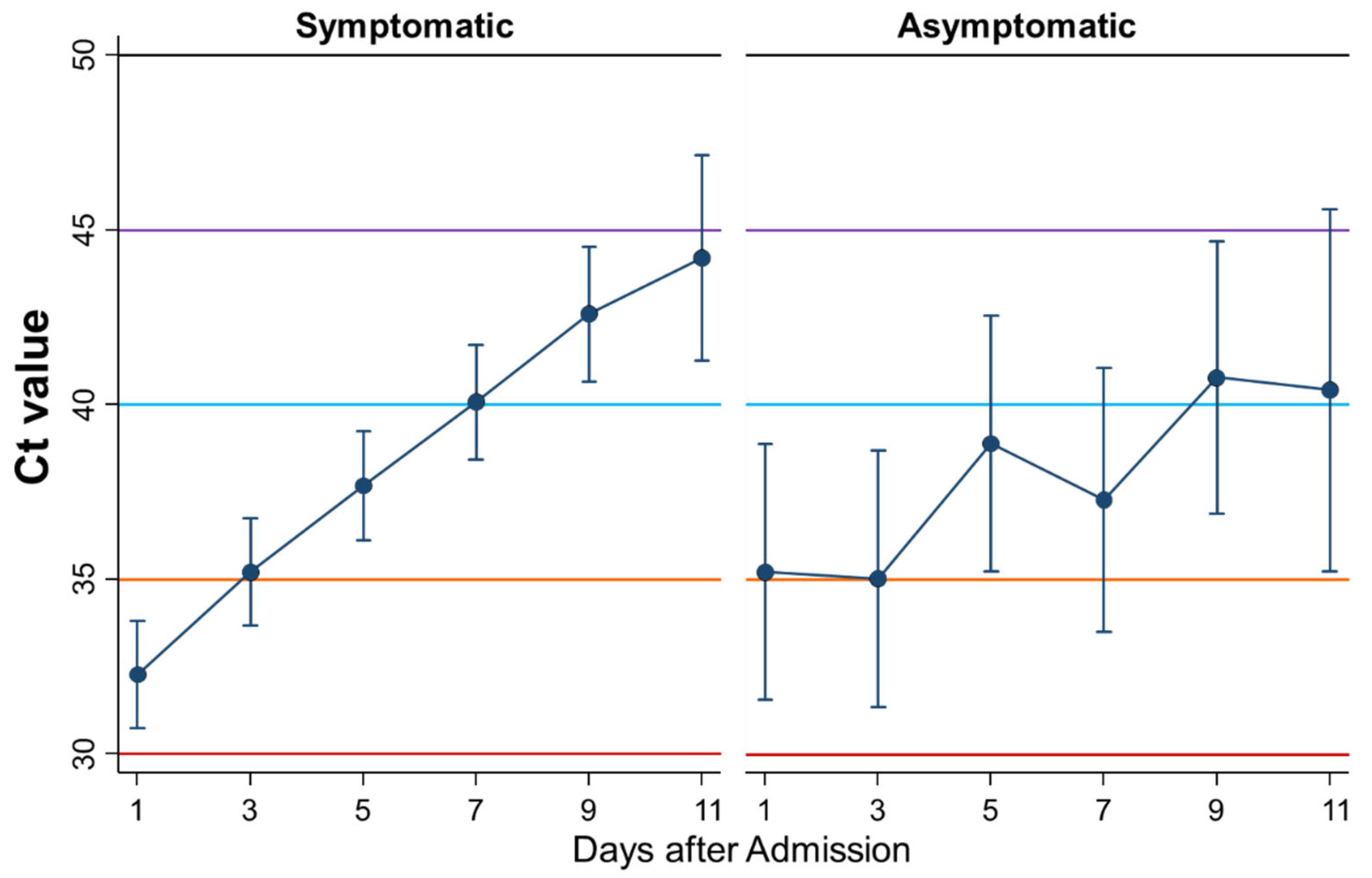
3.3. Differential Kinetics of Ct Values between Symptomatic and Asymptomatic Patients
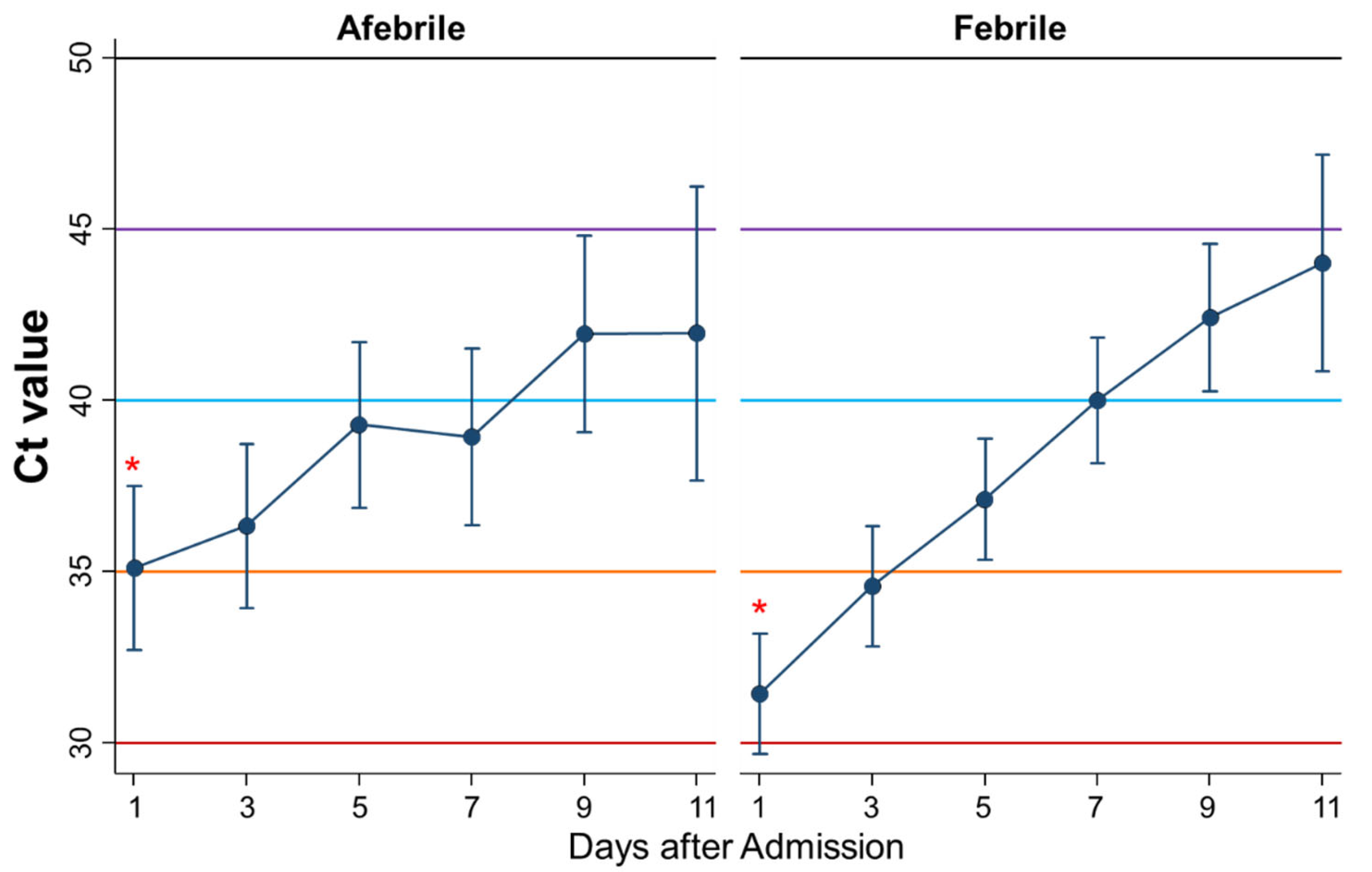
3.4. Differential Kinetics of Ct Values between Afebrile and Febrile Patients
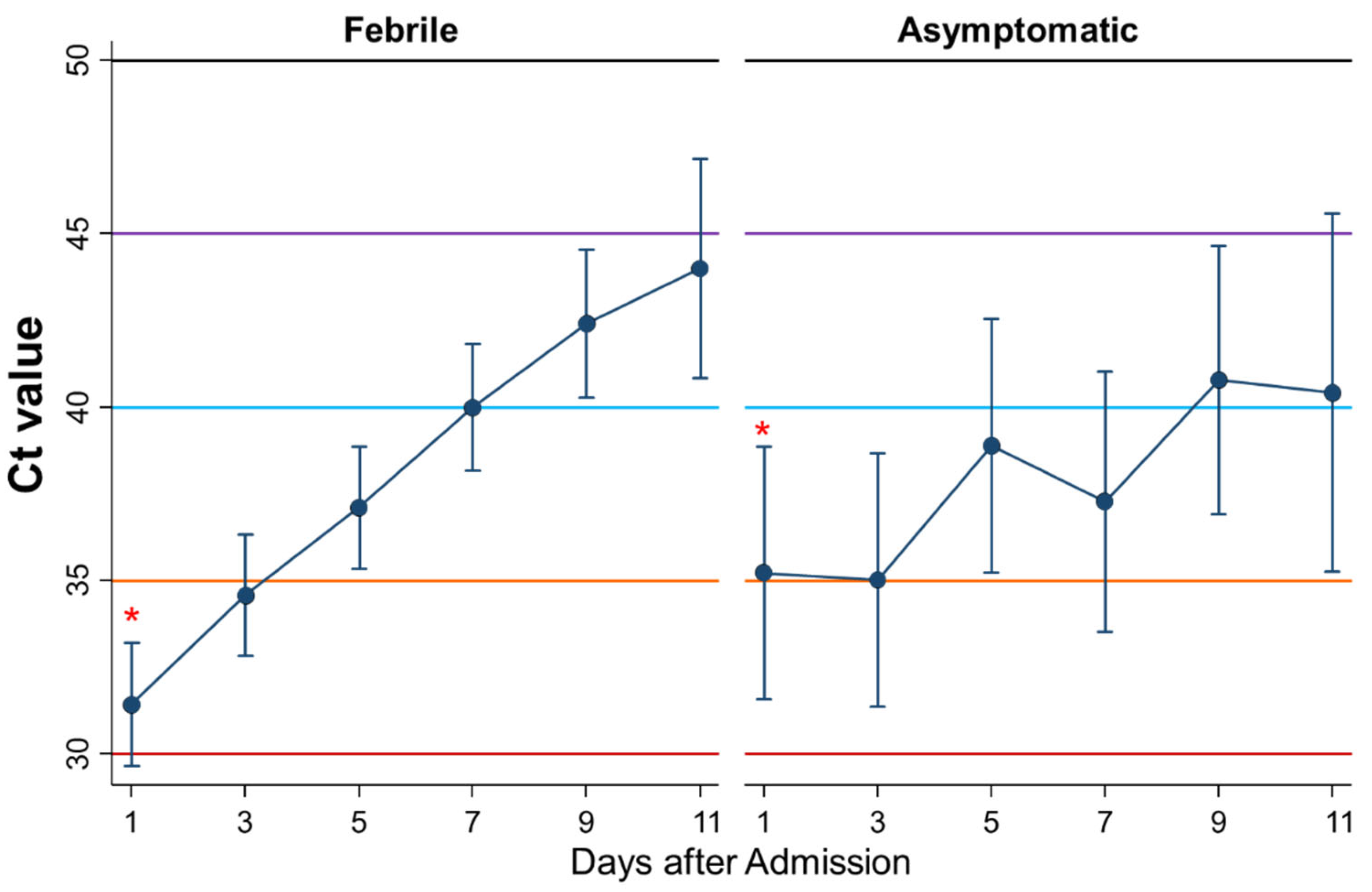
3.5. Differential Kinetics of Ct Values between Febrile Patients and Asymptomatic Patients
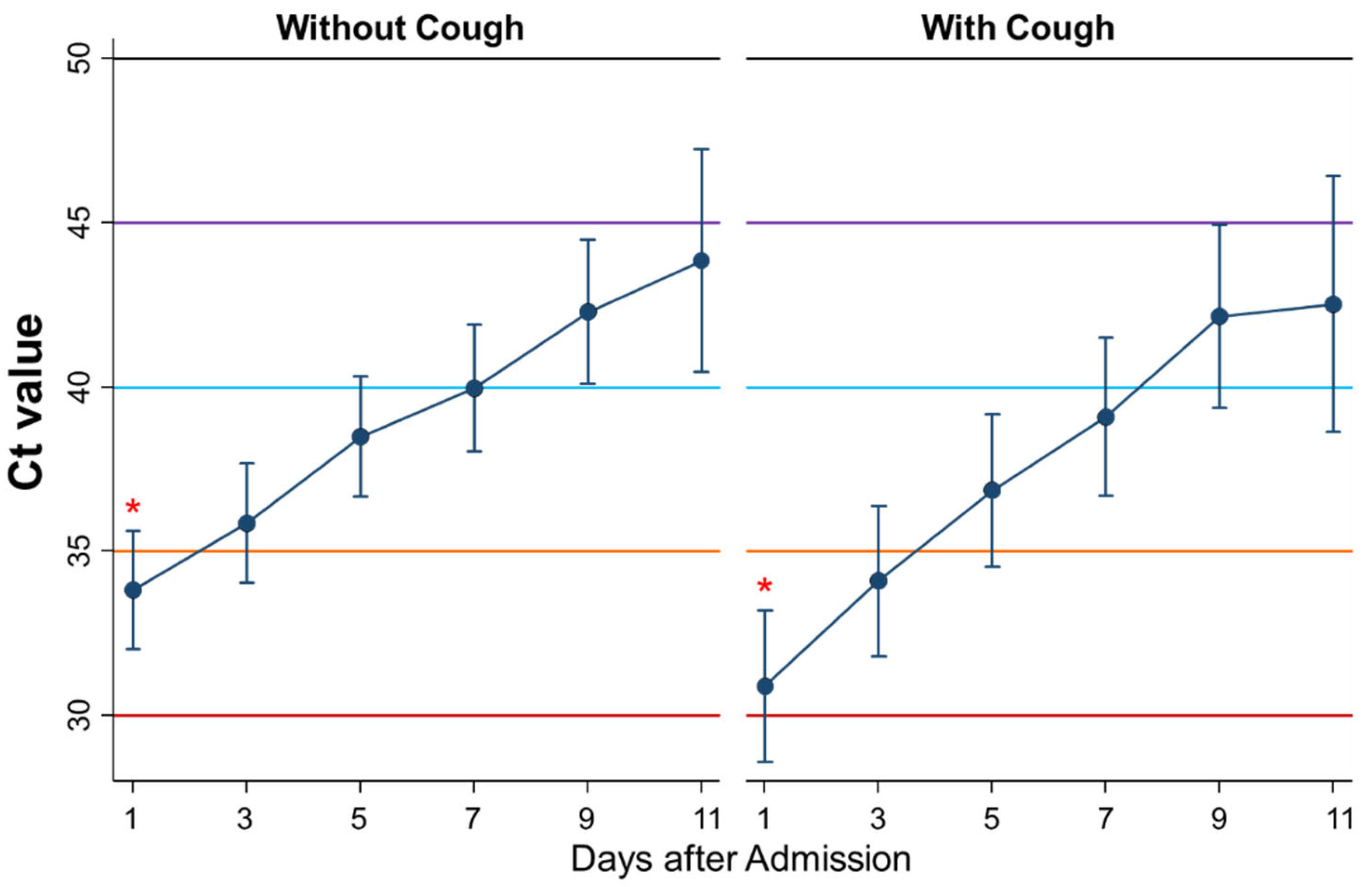
3.6. Differential Kinetics of Ct Values between Patients without and with Cough
3.7. Differential Kinetics of Ct Values between Patients without and with Dysosmia/Dysgeusia
3.8. Differential Kinetics of Ct Values between Patients without and with Headache
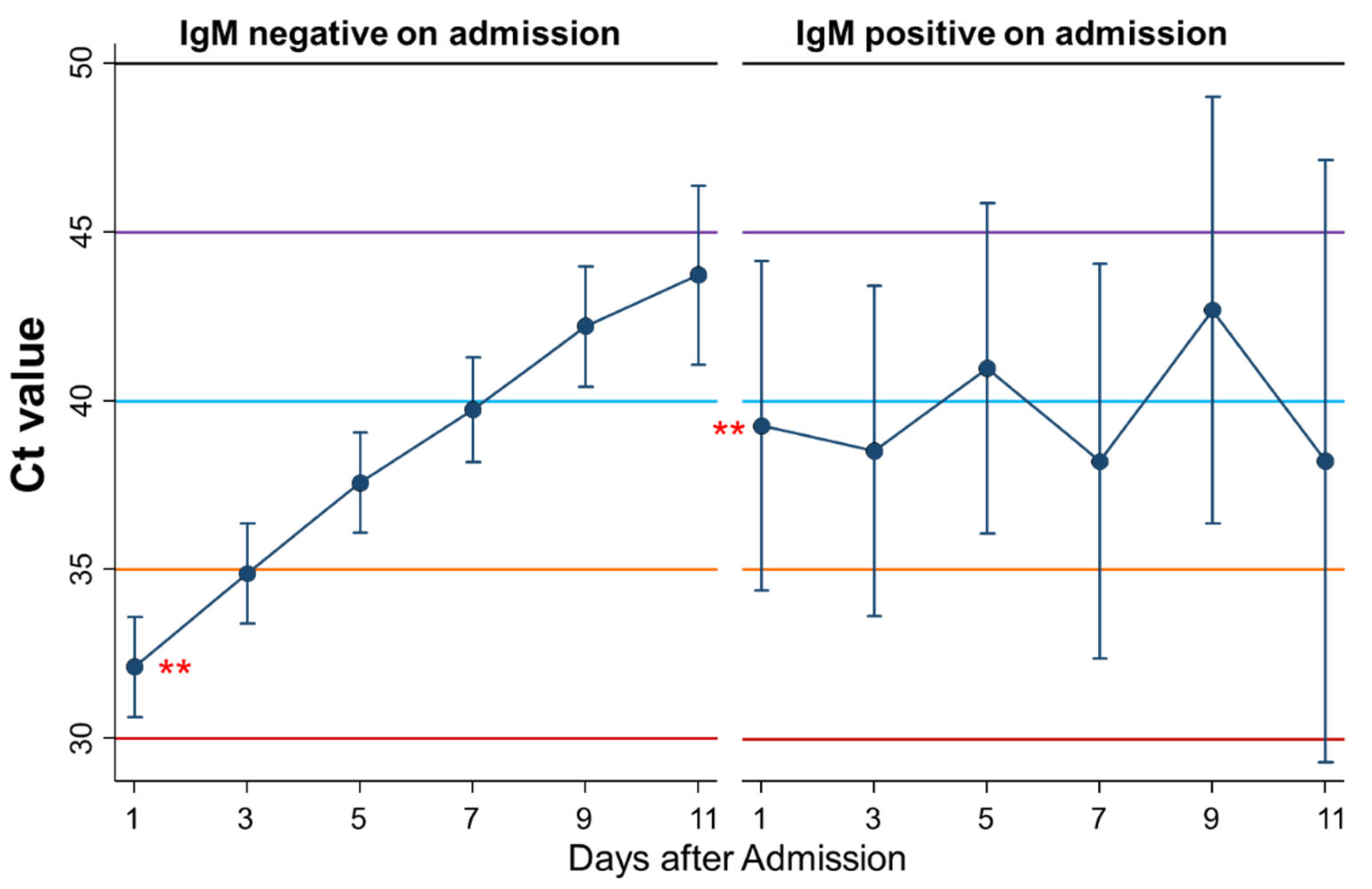
3.9. Differential Kinetics of Ct Values between Patients Negative and Positive for IgM on Admission
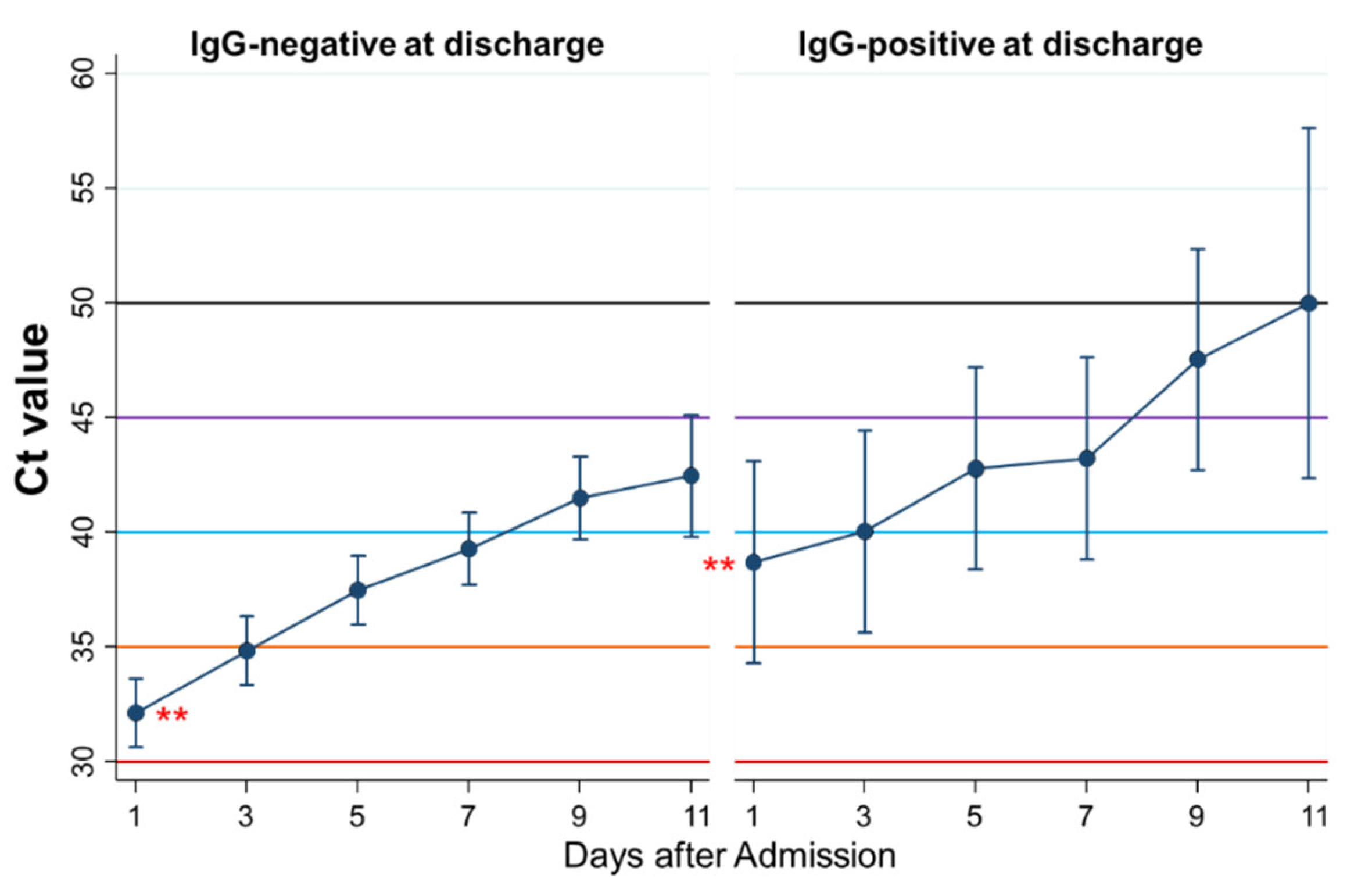
3.10. Differential Kinetics of Ct Values between Patients Negative and Positive for IgG at Discharge
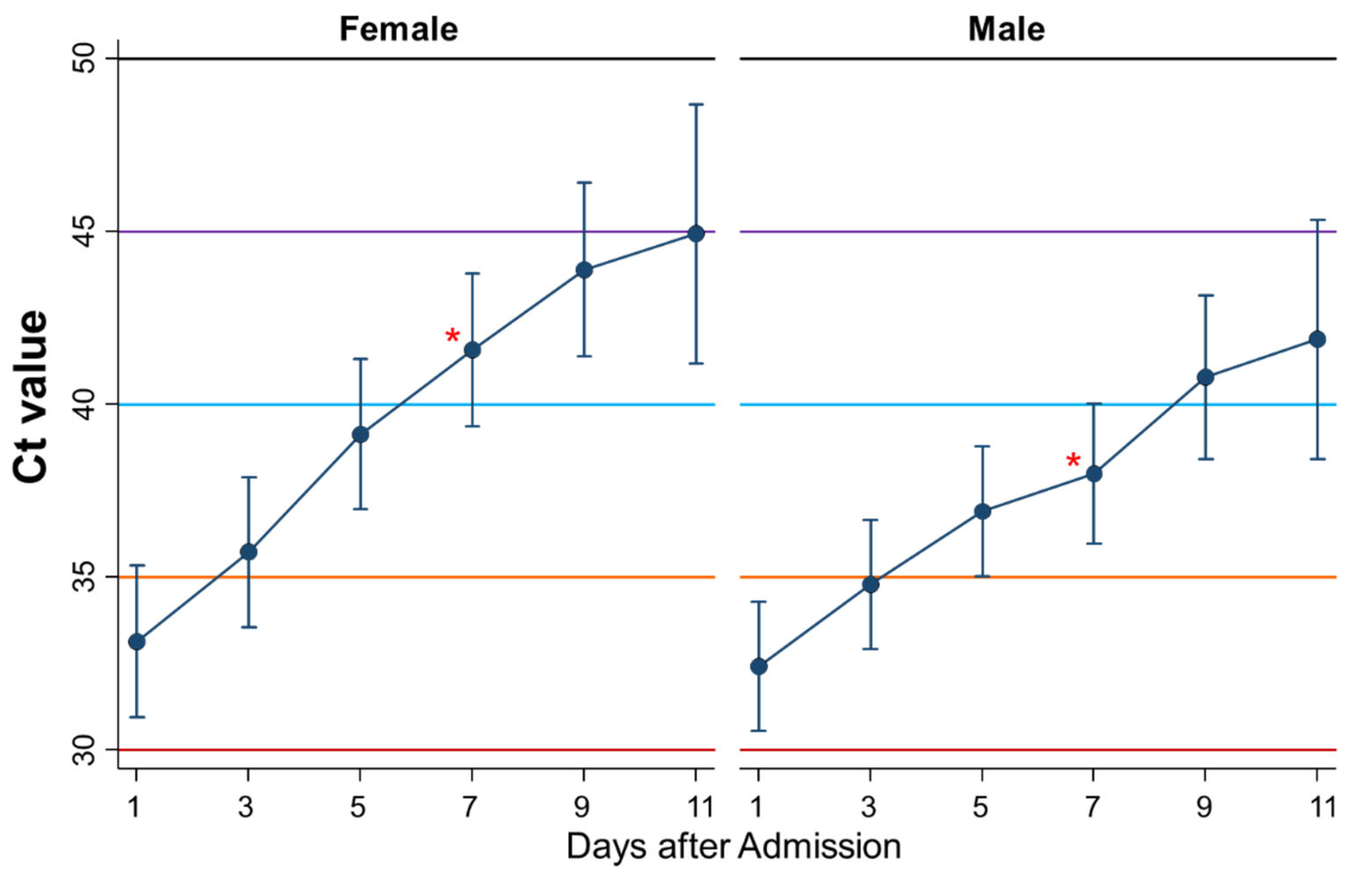
3.11. Differential Kinetics of Ct Values between Women and Men
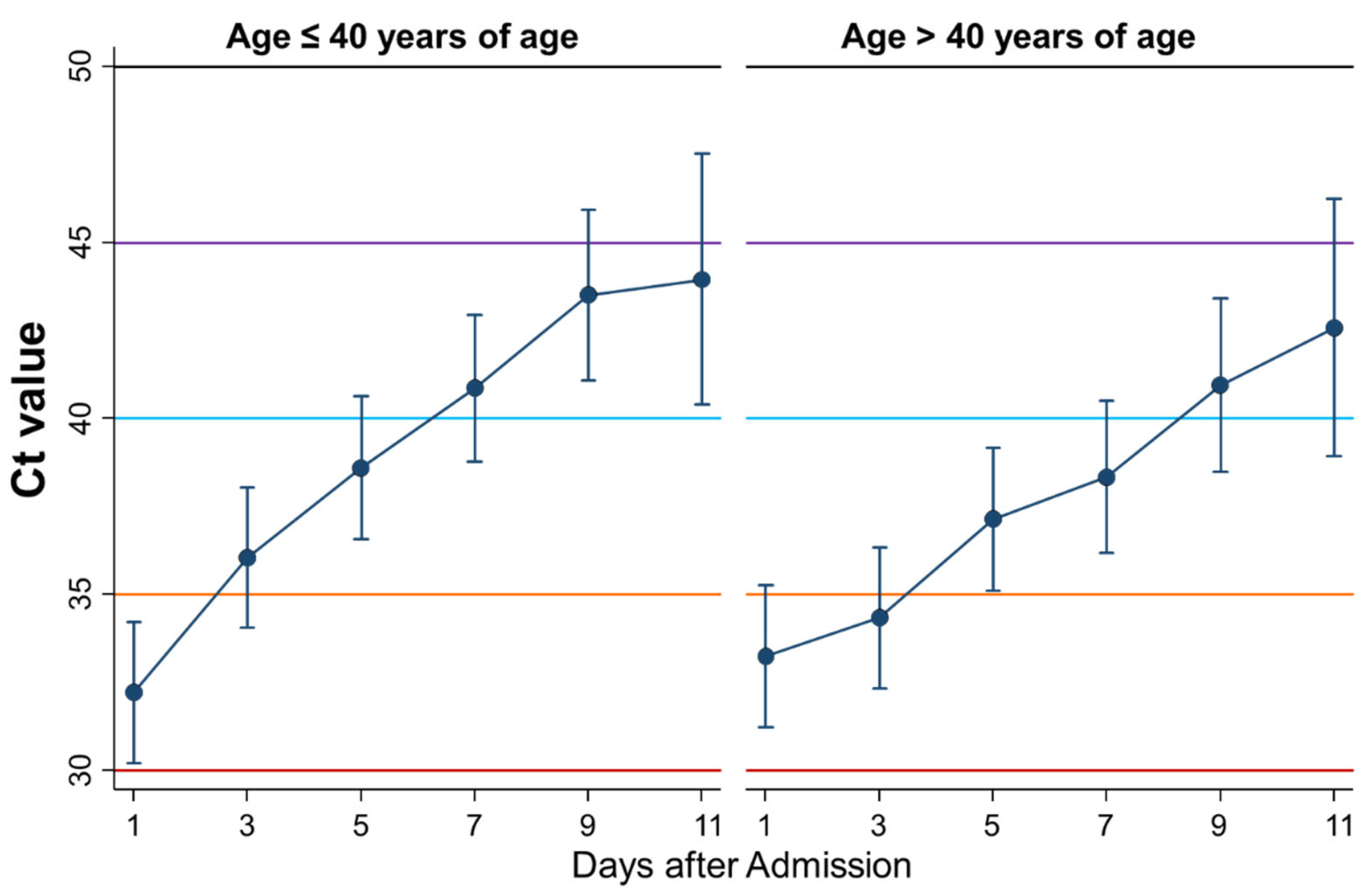
3.12. Differential Kinetics of Ct Values between Younger and Older Than Forty Years
3.13. Persistent Symptoms in Patients after Acute COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of Coronavirus Disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M.; Butler, J.C. SARS-CoV-2 transmission from people without COVID-19 symptoms. JAMA Netw. Open 2021, 4, e2035057. [Google Scholar] [CrossRef]
- Wei, W.E.; Li, Z.; Chiew, C.J.; Yong., S.E.; Toh, M.P.; Lee, V.J. Presymptomatic transmission of SARS-CoV-2—Singapore, January 23–March 16, 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 411–415. [Google Scholar] [CrossRef] [Green Version]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an asymptomatic contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byambasuren, O.; Cardona, M.; Bell, K.; Clark, J.; McLaws, M.; Glasziou, P. Estimating the extent of asymptomatic COVID-19 and its potential for community transmission: Systematic review and meta-analysis. Off. J. Assoc. Med. Microbiol. Infect. Dis. Can. 2020, 5, 223–234. [Google Scholar] [CrossRef]
- Singanayagam, A.; Patel, M.; Charlett, A.; Lopez Bernal, J.; Saliba, V.; Ellis, J.; Ladhani, S.; Zambon, M.; Gopal, R. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Euro Surveill. 2020, 25, 2001483. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Lee, S.; Kim, T.; Lee, E.; Lee, C.; Kim, H.; Rhee, H.; Park, S.Y.; Son, H.J.; Yu, S.; Park, J.W.; et al. Clinical course and molecular viral shedding among asymptomatic and symptomatic patients with SARS-CoV-2 infection in a community treatment center in the Republic of Korea. JAMA Intern. Med. 2020, 180, 1447–1452. [Google Scholar] [CrossRef] [PubMed]
- Dahdouh, E.; Lázaro-Perona, F.; Romero-Gómez, M.P.; Mingorance, J.; García-Rodriguez, J. Ct values from SARS-CoV-2 diagnostic PCR assays should not be used as direct estimates of viral load. J. Infect. 2021, 82, 414–451. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.C.; Cui, C.; Shin, K.R.; Bae, J.Y.; Kweon, O.J.; Lee, M.K.; Choi, S.H.; Jung, S.Y.; Park, M.S.; Chung, J.W. Duration of culturable SARS-CoV-2 in hospitalized patients with Covid-19. N. Engl. J. Med. 2021, 384, 671–673. [Google Scholar] [CrossRef] [PubMed]
- Tabata, S.; Imai, K.; Kawano, S.; Ikeda, M.; Kodama, T.; Miyoshi, K.; Obinata, H.; Mimura, S.; Kodera, T.; Kitagaki, M.; et al. Clinical characteristics of COVID-19 in 104 people with SARS-CoV-2 infection on the Diamond Princess cruise ship: A retrospective analysis. Lancet Infect. Dis. 2020, 20, 1043–1050. [Google Scholar] [CrossRef]
- Kasper, M.R.; Geibe, J.R.; Sears, C.L.; Riegodedios, A.J.; Luse, T.; Von Thun, A.M.; McGinnis, M.B.; Olson, N.; Houskamp, D.; Fenequito, R.; et al. An outbreak of Covid-19 on an aircraft carrier. N. Engl. J. Med. 2020, 383, 2417–2426. [Google Scholar] [CrossRef] [PubMed]
- MySOS. Available online: https://www.allm.net/en/mysos-en/ (accessed on 19 May 2021).
- Team. Available online: https://www.allm.net/en/team-en/ (accessed on 19 May 2021).
- Le Bert, N.; Clapham, H.E.; Tan, A.T.; Chia, W.N.; Tham, C.Y.L.; Lim, J.M.; Kunasegaran, K.; Tan, L.W.L.; Dutertre, C.A.; Shankar, N.; et al. Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection. J. Exp. Med. 2021, 218, e20202617. [Google Scholar] [CrossRef] [PubMed]
- Carsetti, R.; Zaffina, S.; Piano Mortari, E.; Terreri, S.; Corrente, F.; Capponi, C.; Palomba, P.; Mirabella, M.; Cascioli, S.; Palange, P.; et al. Different innate and adaptive immune responses to SARS-CoV-2 infection of asymptomatic, mild, and severe cases. Front. Immunol 2020, 11, 610300. [Google Scholar] [CrossRef]
- Spinato, G.; Fabbris, C.; Polesel, J.; Cazzador, D.; Borsetto, D.; Hopkins, C.; Boscolo-Rizzo, P. Alterations in smell or taste in mildly symptomatic outpatients with SARS-CoV-2 infection. JAMA 2020, 323, 2089–2090. [Google Scholar] [CrossRef] [Green Version]
- Xydakis, M.S.; Dehgani-Mobaraki, P.; Holbrook, E.H.; Geisthoff, U.W.; Bauer, C.; Hautefort, C.; Herman, P.; Manley, G.T.; Lyon, D.M.; Hopkins, C. Smell and taste dysfunction in patients with COVID-19. Lancet Infect. Dis. 2020, 20, 1015–1016. [Google Scholar] [CrossRef]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Scully, E.P.; Haverfield, J.; Ursin, R.L.; Tannenbaum, C.; Klein, S.L. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef]
- Rao, S.N.; Manissero, D.; Steele, V.R.; Pareja, J. A Systematic review of the clinical utility of cycle threshold values in the context of COVID-19. Infect. Dis. Ther. 2020, 9, 573–586. [Google Scholar] [CrossRef] [PubMed]
- Ade, C.; Pum, J.; Abele, I.; Raggub, L.; Bockmühl, D.; Zöllner, B. Analysis of cycle threshold values in SARS-CoV-2-PCR in a long-term study. J. Clin. Virol. 2021, 138, 104791. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.; Yip, C.C.; To, K.K.; Tang, T.H.; Wong, S.C.; Leung, K.H.; Fung, A.Y.; Ng, A.C.; Zou, Z.; Tsoi, H.W.; et al. Improved molecular diagnosis of COVID-19 by the novel, highly sensitive and specific COVID-19-RdRp/Hel real-time reverse transcription-PCR assay validated in vitro and with clinical specimens. J. Clin. Microbiol. 2020, 58, e00310-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinnes, J.; Deeks, J.J.; Berhane, S.; Taylor, M.; Adriano, A.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2021, 3, CD013705. [Google Scholar] [CrossRef] [PubMed]
- Moein, S.T.; Hashemian, S.M.; Mansourafshar, B.; Khorram-Tousi, A.; Tabarsi, P.; Doty, R.L. Smell dysfunction: A biomarker for COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 944–950. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Asymptomatic n = 18 | Symptomatic n = 102 | p-Value | |
|---|---|---|---|---|
| Febrile n = 78 | Afebrile n = 24 | |||
| Age, y Median (IQR 1) | 37 (24–48) | 43.5 (29–50) | 38.5 (26–47) | 0.72 4 |
| Men, n (%) | 12 (66.7%) | 44 (56.4%) | 13 (54.2%) | 0.68 5 |
| Onset to admission, days Median (IQR 1) | - | 4 (3–5) | 5 (3–6.5) | 0.16 6 |
| Admission to discharge, days Median (IQR 1) | 10 (9–10) | 9 (7–10) | 8 (6–9) | 0.01 4 |
| Onset to discharge, days Median (IQR 1) | - | 12 (12–12) | 12 (12–12) | 0.15 6 |
| Ct value on day 1 Mean (SD 1) | 32.7 (28.5–39.7) | 30.1 (26.9–35.2) | 34.4 (28.4–38.8) | 0.04 7 |
| Minimum Ct value Mean (SD 1) | 30.3 (25.9–35.7) | 29.1 (26.0–31.6) | 31.8 (27.1–36.8) | 0.14 7 |
| Ct value on discharge Mean (SD 1) | 39.0 (35.2–50) | 41.9 (34.7–50) | 47.1 (36.4–50) | 0.76 7 |
| UPSIT for smell test 3 | 0.29 5 | |||
| 0~24% | 5 (27.8%) | 14 (18.0%) | 9 (40.9%) | |
| 25~49% | 2 (11.1%) | 5 (6.4%) | 3 (13.6%) | |
| 50~74% | 1 (5.7%) | 14 (18.0%) | 3 (13.6%) | |
| 75~99% | 3 (16.7%) | 20 (25.6%) | 3 (13.6%) | |
| 100% | 7 (38.9%) | 25 (32.1%) | 4 (18.2%) | |
| SpO2, % 2 Median (IQR 1) | 97 (97–97) | 97 (97–98) | 97 (96–97) | 0.20 4 |
| IgM on admission | 0.37 5 | |||
| - | 15 (83.3%) | 73 (93.6%) | 22 (91.7%) | |
| ± | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| + | 3 (16.7%) | 5 (6.4%) | 2 (8.3%) | |
| IgG on admission | - | |||
| - | 18 (100%) | 78 (100%) | 24 (100%) | |
| ± | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| + | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| IgM at discharge | 0.96 5 | |||
| - | 7 (38.9%) | 25 (32.9%) | 8 (34.8%) | |
| ± | 3 (16.7%) | 19 (25.0%) | 5 (21.7%) | |
| + | 8 (44.4%) | 32 (42.1%) | 10 (43.5%) | |
| IgG at discharge | 0.44 5 | |||
| - | 16 (88.9%) | 63 (82.9%) | 18 (78.3%) | |
| ± | 0 (0.0%) | 7 (9.2%) | 1 (4.4%) | |
| + | 2 (11.1%) | 6 (7.9%) | 4 (17.4%) | |
| Patient | Age (y) Sex | Onset Date Admission Date | Symptoms | Ct Value on Admission | Minimum O2 Saturation | Date of Referral | Reason for Referral |
|---|---|---|---|---|---|---|---|
| 1 | 39 male | 11/11/2020 13/11/2020 | Fever Dysosmia | 28.2 | 93 | 18/11/2020 | hypoxia |
| 2 | 54 male | 18/11/2020 21/11/2020 | Cough | 34.3 | 82 | 23/11/2020 | hypoxia |
| 3 | 58 male | 1/12/2020 6/12/2020 | Fever, Cough, Sore throat | 24.8 | 93 | 18/11/2020 | hypoxia |
| Variable n (%) 1 | Asymptomatic n = 15 | Symptomatic n = 102 | p-Value 2 | |
|---|---|---|---|---|
| Febrile n = 64 | Afebrile n = 17 | |||
| Dysosmia/dysgeusia | 2 (13.3%) | 12 (19.1%) | 4 (23.5%) | 0.76 |
| Difficulty in breath | 1 (6.7%) | 10 (15.9%) | 2 (11.8%) | 0.63 |
| Cough/sputum | 1 (6.7%) | 6 (9.5%) | 5 (29.4%) | 0.07 |
| Fatigue | 0 (0.0%) | 5 (7.9%) | 3 (17.7%) | 0.19 |
| Headache | 0 (0.0%) | 2 (3.2%) | 1 (5.9%) | 0.64 |
| Fever | 0 (0.0%) | 2 (3.2%) | 0 (0.0%) | 0.60 |
| Sleepiness | 1 (6.7%) | 0 (0.0%) | 1 (5.9%) | 0.13 |
| Chest pain | 0 (0.0%) | 1 (1.6%) | 0 (0.0%) | 0.77 |
| Joint pain | 0 (0.0%) | 1 (1.6%) | 0 (0.0%) | 0.77 |
| Any chronic symptoms, n (%) 2 | 4 (26.7%) | 23 (36.5%) | 7 (41.2%) | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakano, T.; Urashima, M.; Takao, H.; Takeshita, K.; Kobashi, H.; Fujiwara, T. Differential Kinetics of Cycle Threshold Values during Admission by Symptoms among Patients with Mild COVID-19: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 8181. https://doi.org/10.3390/ijerph18158181
Sakano T, Urashima M, Takao H, Takeshita K, Kobashi H, Fujiwara T. Differential Kinetics of Cycle Threshold Values during Admission by Symptoms among Patients with Mild COVID-19: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(15):8181. https://doi.org/10.3390/ijerph18158181
Chicago/Turabian StyleSakano, Teppei, Mitsuyoshi Urashima, Hiroyuki Takao, Kohei Takeshita, Hiroe Kobashi, and Takeo Fujiwara. 2021. "Differential Kinetics of Cycle Threshold Values during Admission by Symptoms among Patients with Mild COVID-19: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 15: 8181. https://doi.org/10.3390/ijerph18158181
APA StyleSakano, T., Urashima, M., Takao, H., Takeshita, K., Kobashi, H., & Fujiwara, T. (2021). Differential Kinetics of Cycle Threshold Values during Admission by Symptoms among Patients with Mild COVID-19: A Prospective Cohort Study. International Journal of Environmental Research and Public Health, 18(15), 8181. https://doi.org/10.3390/ijerph18158181