
Intergenerational Transmission of Child Feeding Practices




Abstract
:1. Introduction
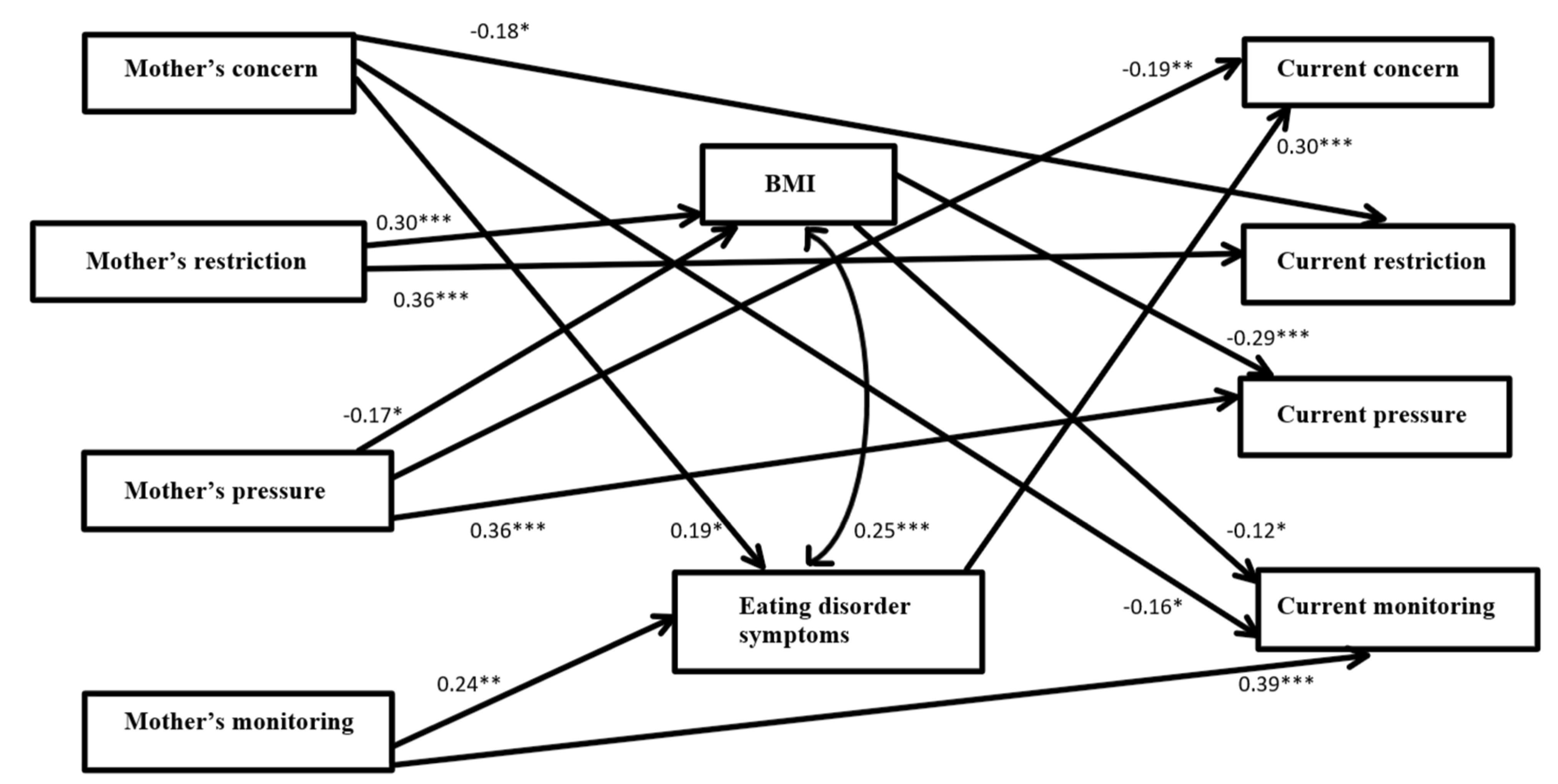
- There will be a positive and significant association between retrospectively recalled maternal CFP and current CFP, after controlling for BMI.
- There will be positive and significant associations between parents’ current DE, current CFP and retrospectively recalled maternal CFP, after controlling for BMI.
- Parents’ current DE and BMI will mediate the association between their current CFP and their retrospectively recalled maternal CFP.
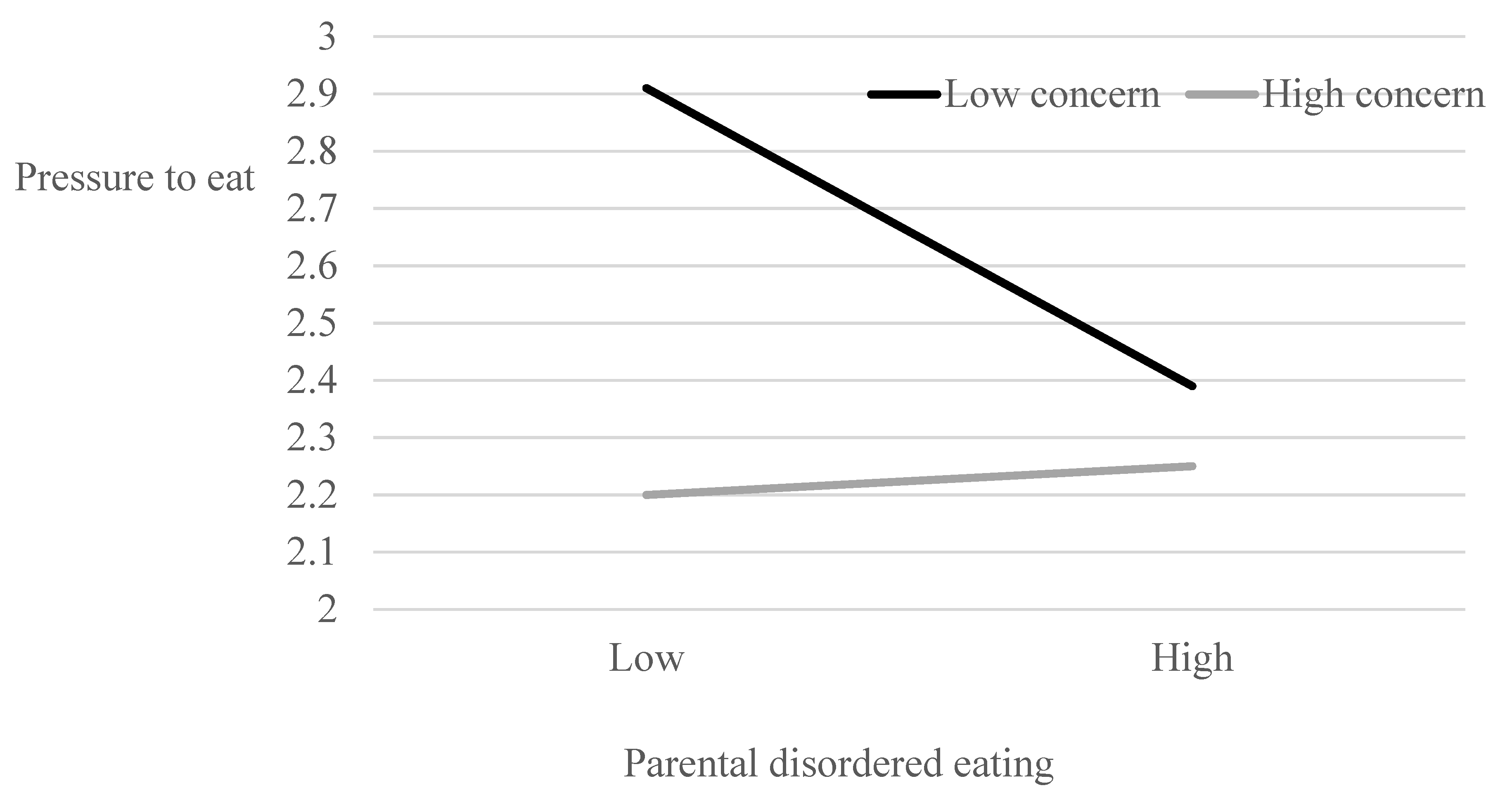
- Parents’ current DE will moderate the association between their current concern about their child’s weight and both pressure for him/her to eat and restriction of his/her caloric intake.
2. Method
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Birch, L.L.; Fisher, J.O. Mothers’ child-feeding practices influence daughters’ eating and weight. Am. J. Clin. Nutr. 2000, 71, 1054–1061. [Google Scholar] [CrossRef]
- Handford, C.M.; Rapee, R.M.; Fardouly, J. The influence of maternal modeling on body image concerns and eating disturbances in preadolescent girls. Behav. Res. Ther. 2018, 100, 17–23. [Google Scholar] [CrossRef]
- Ogden, J.; Reynolds, R.; Smith, A. Expanding the concept of parental control: A role for overt and covert control in children’s snacking behaviour? Appetite 2006, 47, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Rhee, K. Childhood overweight and the relationship between parent behaviors, parenting style, and family functioning. ANNALS Am. Acad. Polit. Soc. Sci. 2008, 615, 11–37. [Google Scholar] [CrossRef]
- Keller, K.L.; Pietrobelli, A.; Johnson, S.L.; Faith, M.S. Maternal restriction of children’s eating and encouragements to eat as the ‘non-shared environment’: A pilot study using the child feeding questionnaire. Int. J. Obes. 2006, 30, 1670–1675. [Google Scholar] [CrossRef] [Green Version]
- Carruth, B.R.; Skinner, J.; Houck, K.; Moran, J., III; Coletta, F.; Ott, D. The phenomenon of “picky eater”: A behavioral marker in eating patterns of toddlers. J. Am. Coll. Nutr. 1998, 17, 180–186. [Google Scholar] [CrossRef]
- Farrow, C.V.; Galloway, A.T.; Fraser, K. Sibling eating behaviours and differential child feeding practices reported by parents. Appetite 2009, 52, 307–312. [Google Scholar] [CrossRef] [Green Version]
- Zohar, A.H.; Lev-Ari, L.; Bachner-Melman, R. Child and Maternal Correlates of Picky Eating in Young Children. Psychology 2019, 10, 1249–1261. [Google Scholar] [CrossRef] [Green Version]
- Lev-Ari, L.; Zohar, A.H. Nothing gained: An explorative study of the long-term effects of perceived maternal feeding practices on women’s and men’s adult BMI, body image dissatisfaction, and disordered eating. Int. J. Psych. 2013, 48, 1201–1211. [Google Scholar] [CrossRef]
- Batsell, W.R.; Brown, A.S., Jr.; Ansfield, M.E.; Paschall, G.Y. “You will eat all of that!”: A retrospective analysis of forced consumption episodes. Appetite 2002, 38, 211–219. [Google Scholar] [CrossRef]
- Galloway, A.T.; Fiorito, L.M.; Francis, L.A.; Birch, L.L. ‘Finish your soup’: Counterproductive effects of pressuring children to eat on intake and affect. Appetite 2006, 46, 318–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, S.W.; Chamberlin, L.A.; Van Schaick, K.B.; Sherman, S.N.; Whitaker, R.C. Maternal feeding strategies, child eating behaviors, and child BMI in low-income African-American preschoolers. Obesity 2006, 14, 2026–2033. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo-Mendez, J.; Power, T.G.; Fisher, J.O.; O’Connor, T.M.; Hughes, S.O. Child weight status and accuracy of perceived child weight status as predictors of Latina mothers’ feeding practices and styles. Appetite 2019, 142, 104387. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.C.; Sussner, K.M.; Greaney, M.L.; Peterson, K.E. Latina mothers’ beliefs and practices related to weight status, feeding, and the development of child overweight. Public Health Nurs. 2011, 28, 107–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francis, L.A.; Hofer, S.M.; Birch, L.L. Predictors of maternal child-feeding style: Maternal and child characteristics. Appetite 2001, 37, 231–243. [Google Scholar] [CrossRef]
- Webber, L.; Hill, C.; Cooke, L.; Carnell, S.; Wardle, J. Associations between child weight and maternal feeding styles are mediated by maternal perceptions and concerns. Eur. J. Clin. Nutr. 2010, 64, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Kaur, H.; Li, C.; Nazir, N.; Choi, W.S.; Resnicow, K.; Birch, L.L.; Ahluwalia, J.S. Confirmatory factor analysis of the child-feeding questionnaire among parents of adolescents. Appetite 2006, 47, 36–45. [Google Scholar] [CrossRef]
- Branen, L.; Fletcher, J. Comparison of college students’ current eating habits and recollections of their childhood food practices. J. Nutr. Educ. 1999, 31, 304–310. [Google Scholar] [CrossRef]
- Galloway, A.T.; Farrow, C.V.; Martz, D.M. Retrospective reports of child feeding practices, current eating behaviors, and BMI in college students. Obesity 2010, 18, 1330–1335. [Google Scholar] [CrossRef]
- McPhie, S.; Skouteris, H.; Daniels, L.; Jansen, E. Maternal correlates of maternal child feeding practices: A systematic review. Matern. Child Nutr. 2014, 10, 18–43. [Google Scholar] [CrossRef] [Green Version]
- Haycraft, E.L.; Blissett, J.M. Maternal and paternal controlling feeding practices: Reliability and relationships with BMI. Obesity 2008, 16, 1552–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blissett, J.; Haycraft, E. Parental eating disorder symptoms and observations of mealtime interactions with children. J. Psychosom. Res. 2011, 70, 368–371. [Google Scholar] [CrossRef] [Green Version]
- Sadeh-Sharvit, S.; Levy-Shiff, R.; Feldman, T.; Ram, A.; Gur, E.; Zubery, E.; Steiner, E.; Latzer, Y.; Lock, J.D. Child feeding perceptions among mothers with eating disorders. Appetite 2015, 95, 67–73. [Google Scholar] [CrossRef]
- Lev-Ari, L.; Zohar, A.H. The psychometric properties of the retrospective child feeding questionnaire in Hebrew. Appetite 2013, 65, 14–19. [Google Scholar] [CrossRef]
- Camcı, N.; Bas, M.; Buyukkaragoz, A.H. The psychometric properties of the Child Feeding Questionnaire (CFQ) in Turkey. Appetite 2014, 78, 49–54. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef]
- Apter, A.; Yanko, Y. Anorexia Nervosa in Subpopulations in Israel. (Unpublished Manuscript). Tel Aviv University: Tel Aviv, Israel, 1989. [Google Scholar]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commic. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Bentler, P.M.; Bonett, D.G. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. Sociol Methods Res 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Roberts, L.T.; Carbonneau, N.; Goodman, L.C.; Musher-Eizenman, D.R. Retrospective reports of childhood feeding in mother-daughter dyads. Appetite 1993, 149, 104613. [Google Scholar] [CrossRef]
- Zohar, A.H.; Lev-Ari, L.; Bachner-Melman, R. Two to tango? The dance of maternal feeding practices and child eating behavior. Int. J. Environ. Res. Public Health 2021, 18, 1650. [Google Scholar] [CrossRef]
- Gold, J.M.; Vander Weg, M.W. Investigating the relationship between parental weight stigma and feeding practices. Appetite 2020, 149, 104635. [Google Scholar] [CrossRef]
- Webb, H.J.; Haycraft, E. Parental body dissatisfaction and controlling child feeding practices: A prospective study of Australian parent-child dyads. Eat. Beh. 2019, 32, 1–6. [Google Scholar] [CrossRef]
- Gregory, J.E.; Paxton, S.J.; Brozovic, A.M. Pressure to eat and restriction are associated with child eating behaviours and maternal concern about child weight, but not child body mass index, in 2-to 4-year-old children. Appetite 2010, 54, 550–556. [Google Scholar] [CrossRef]
- Jansen, P.W.; de Barse, L.M.; Jaddoe, V.W.; Verhulst, F.C.; Franco, O.H.; Tiemeier, H. Bi-directional associations between child fussy eating and parents’ pressure to eat: Who influences whom? Physiol. Behav. 2017, 176, 101–106. [Google Scholar] [CrossRef]
- Ellis, J.M.; Schenk, R.R.; Galloway, A.T.; Zickgraf, H.F.; Webb, R.M.; Martz, D.M. A multidimensional approach to understanding the potential risk factors and covariates of adult picky eating. Appetite 2018, 125, 1–9. [Google Scholar] [CrossRef]
- Williams, N.A.; Dev, D.A.; Hankey, M.; Blitch, K. Role of food preoccupation and current dieting in the associations of parental feeding practices to emotional eating in young adults: A moderated mediation study. Appetite 2017, 111, 195–202. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Current Retrospective | Concern | Restriction | Pressure | Monitoring | Mean (SD) |
|---|---|---|---|---|---|
| Concern | 0.19 ** | 0.09 | −0.08 | 0.09 | 1.93 (1.12) |
| Restriction | 0.13 * | 0.29 *** | 0.05 | 0.17 * | 2.06 (0.77) |
| Pressure | −0.11 | 0.22 ** | 0.37 *** | 0.13 * | 2.70 (1.06) |
| Monitoring | 0.12 | 0.10 | −0.07 | 0.28 *** | 2.32 (1.13) |
| Mean (SD) | 2.00 (1.00) | 2.58 (0.73) | 2.49 (0.99) | 3.52 (0.89) |
| EAT-26 | |
|---|---|
| Current (CFQ) | |
| Concern | 0.38 *** |
| Restriction | 0.16 * |
| Pressure | −0.17 * |
| Monitoring | 0.16 * |
| Retrospective (RCFQ) | |
| Concern | 0.37 *** |
| Restriction | 0.24 *** |
| Pressure | 0.07 |
| Monitoring | 0.33 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lev-Ari, L.; Zohar, A.H.; Bachner-Melman, R.; Totah Hanhart, A. Intergenerational Transmission of Child Feeding Practices. Int. J. Environ. Res. Public Health 2021, 18, 8183. https://doi.org/10.3390/ijerph18158183
Lev-Ari L, Zohar AH, Bachner-Melman R, Totah Hanhart A. Intergenerational Transmission of Child Feeding Practices. International Journal of Environmental Research and Public Health. 2021; 18(15):8183. https://doi.org/10.3390/ijerph18158183
Chicago/Turabian StyleLev-Ari, Lilac, Ada H. Zohar, Rachel Bachner-Melman, and Auriane Totah Hanhart. 2021. "Intergenerational Transmission of Child Feeding Practices" International Journal of Environmental Research and Public Health 18, no. 15: 8183. https://doi.org/10.3390/ijerph18158183
APA StyleLev-Ari, L., Zohar, A. H., Bachner-Melman, R., & Totah Hanhart, A. (2021). Intergenerational Transmission of Child Feeding Practices. International Journal of Environmental Research and Public Health, 18(15), 8183. https://doi.org/10.3390/ijerph18158183